
Abstract
Systemic lupus erythematosus (SLE) is an autoimmune disease that most commonly occurs in women of childbearing age. However, cases of SLE with abnormal pregnancy as the initial manifestation, involving the development of diffuse alveolar hemorrhage (DAH), have rarely been reported. Herein, we report the case of a young woman who underwent a cesarean section for fetal distress and growth restriction at 35 + 1 weeks’ gestation. Following discharge, she experienced progressive worsening of anemia and chest tightness, which was later diagnosed as SLE complicated by DAH.
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease that commonly affects young women of childbearing age. Clinical manifestations are diverse, ranging from mild arthritis to diffuse alveolar hemorrhage (DAH). Its main manifestations include dyspnea, cough, fever, bloody sputum, and hemoptysis, which are closely related to the active state of the disease. DAH is a rare and devastating complication of SLE, seen in only 1%–5% of cases; it has a mortality rate of up to 50% despite aggressive treatment. 1
Case report
A 19-year-old woman was hospitalized for 10 days following a cesarean section due to a 2-day history of dizziness and weakness. The patient had a small amount of vaginal bleeding 10 days after delivery and no abdominal pain. One day prior, the patient felt dizzy and weak and was immediately admitted under the diagnosis of “severe anemia; post-cesarean section.” She had a dry cough, no sputum, slight shortness of breath, poor appetite, an inability to lie down at night, and experienced poor sleep. She had normal bowel movements and no nausea, vomiting, chills, fever, nor history of recent sexual intercourse or bathing. Moreover, the patient had no history of rash, arthralgias, hair loss, oral ulcers, or photosensitivity.
Laboratory test results before and after admission.

WB, white blood cell; Hb, hemoglobin; PLT, platelet; FDP, fibrin degradation products; CRP, C-reactive protein.
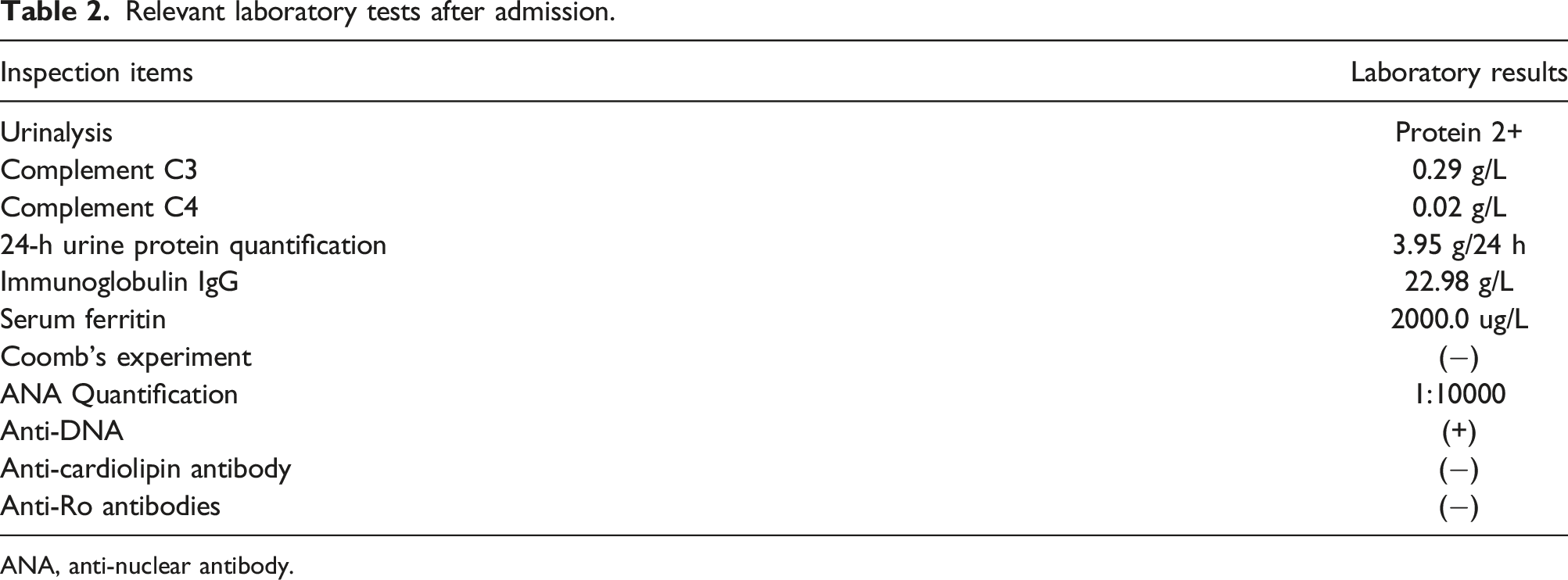
A cardiac ultrasound showed low pericardial effusion, while an abdominal pelvic gynecological ultrasound showed a postpartum uterus with fluid in the uterine cavity and an enlarged spleen with abnormal internal hypovolemia. A computed tomography (CT) scan of the chest showed a diffuse high-density shadow with blurred borders in both lungs (Figure 1). The relevant laboratory tests after admission are shown in Table 2. Computed tomography of the chest. Relevant laboratory tests after admission. ANA, anti-nuclear antibody.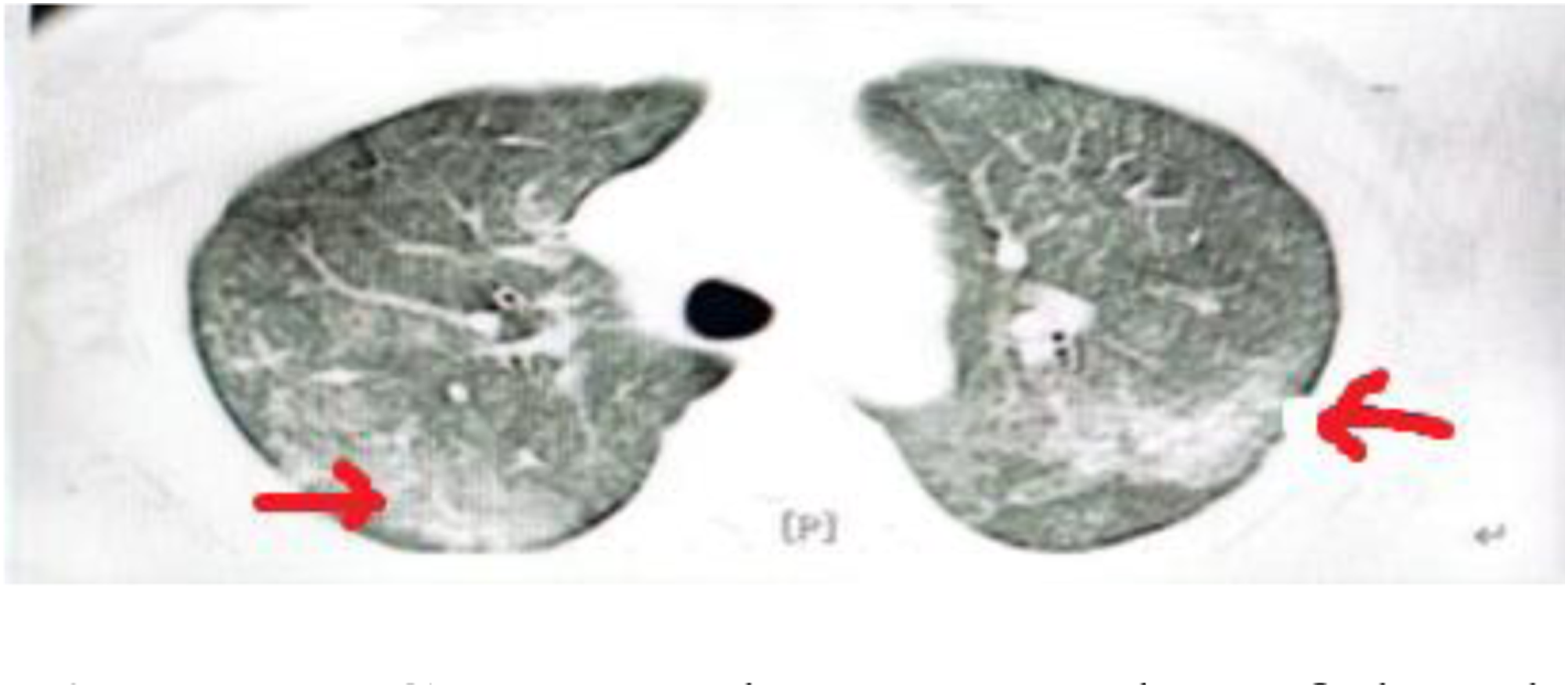
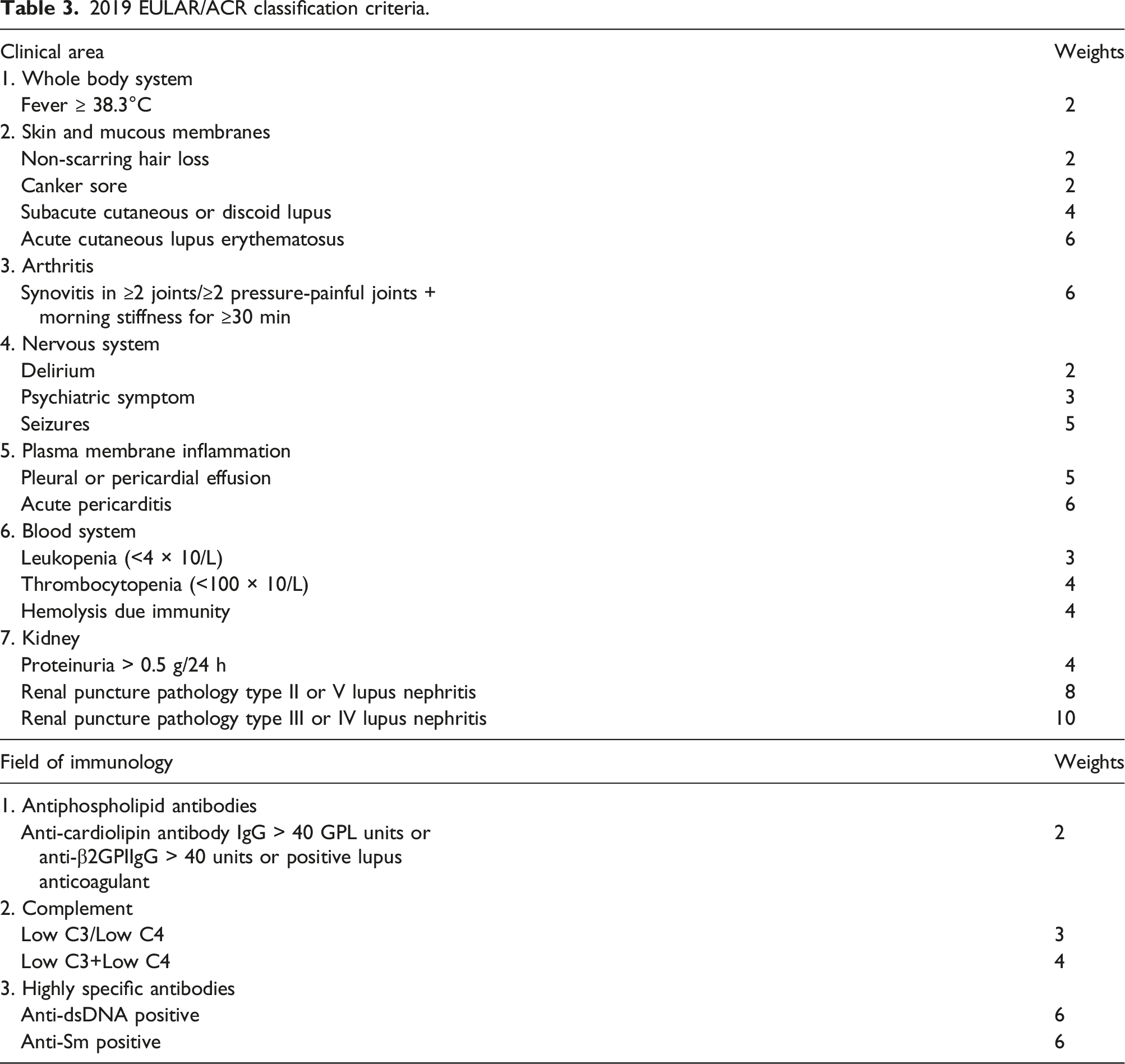
2019 EULAR/ACR classification criteria.
Discussion
SLE is common in women of childbearing age, and pregnancy and childbirth serve as significant factors that can trigger or exacerbate the condition.2,3 Patients may present with pregnancy/delivery-induced SLE, while in some cases lupus crisis is the first symptom. A previous study 4 showed that among 223 mothers with SLE presenting to this hospital during 2013–2017, 68 had SLE with initial-onset in pregnancy/postpartum, while some patients had lupus crisis as their first symptom. Patients with SLE commonly experience renal involvement, and the presence of proteinuria or elevated serum creatinine levels raises suspicion for renal complications. The risk of DAH has been reported to be elevated in patients with lupus nephritis in the presence of acute pulmonary symptoms, new X-ray infiltrates, decreased erythrocyte specific gravity, and even in the absence of hemoptysis. 5 In some cases, alveolar hemorrhage is sufficient to cause anemia; therefore, anemia of unknown origin should exclude DAH. 6 In this case, acute anemia was the first symptom, and lung CT showed diffuse ground glass and solid shadows in both lungs. Hemoptysis had not been seen during the course of the disease. Hence, it is necessary to exclude the possibility of bleeding from the digestive tract, urinary tract, abdominal cavity, and hemolytic anemia. Diffuse pulmonary hemorrhage due to trauma, infectious pneumonia (tuberculosis, bacterial, viral, and fungal), bronchogenic carcinoma, choriocarcinoma, carcinoid tumors, interstitial lung disease, pulmonary hypertension, arteriovenous malformations, pulmonary embolism, congenital heart disease, acute lupus pneumonitis, granulomatous polyangiitis, Goodpasture's syndrome, and drug-induced pulmonary hemorrhage (such as that caused by cocaine, anticoagulants, and antiplatelet agents) should also be excluded. 1 Also in patients with acute anemia, especially in combination with renal involvement and/or decreased complement and/or intestinal infections, we need to rule out hemolytic uremic syndrome (HUS), thrombotic microangiopathy (TMA) possibly.
In summary, this case underscores the possibility of SLE presenting as a lupus crisis, such as DAH. Clinicians should consider the presence of autoantibodies, such as ANAs, detected in the sera of patients with connective tissue diseases like SLE.7,8 It is also necessary to combine the specific diagnostic criteria for SLE (see Table 3 for details) based on the patient’s clinical manifestations and family history, which can lead to early detection, diagnosis, and treatment of SLE. Hormonal changes due to pregnancy are important in triggering or exacerbating SLE, and its development is a risk factor for adverse pregnancy outcomes. 9 Women with SLE have an increased risk of adverse pregnancy outcomes compared to the general population. 10 In cases where a patient experiences an unexplained adverse pregnancy outcome, a multidisciplinary approach combining the opinions of experts from multiple specialties is required, and a timely diagnosis of SLE and aggressive control of the primary disease may prevent the development of DAH.
Footnotes
Acknowledgments
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s note
The manuscript has been read and approved by all authors; the manuscript meets the authorship requirements described earlier in this document.