
Abstract
Objectives
Neuropsychiatric symptoms develop in up to 20% of the patients with Systemic Lupus Erythematosus (SLE). Growing evidence is accruing on the association of SLE with Post-traumatic Stress Disorder (PTSD), but little is known about its contribution on patient-reported outcomes. This study focuses on PTSD prevalence in our SLE cohort and on its impact on quality of life.
Methods
Trauma and Loss Spectrum – Self Reported (TALS-SR) and Lupus Quality of Life (Lupus QoL) questionnaires were administered via web to the patients with SLE in our cohort, along with questions on demographical and disease-related aspects.
Results
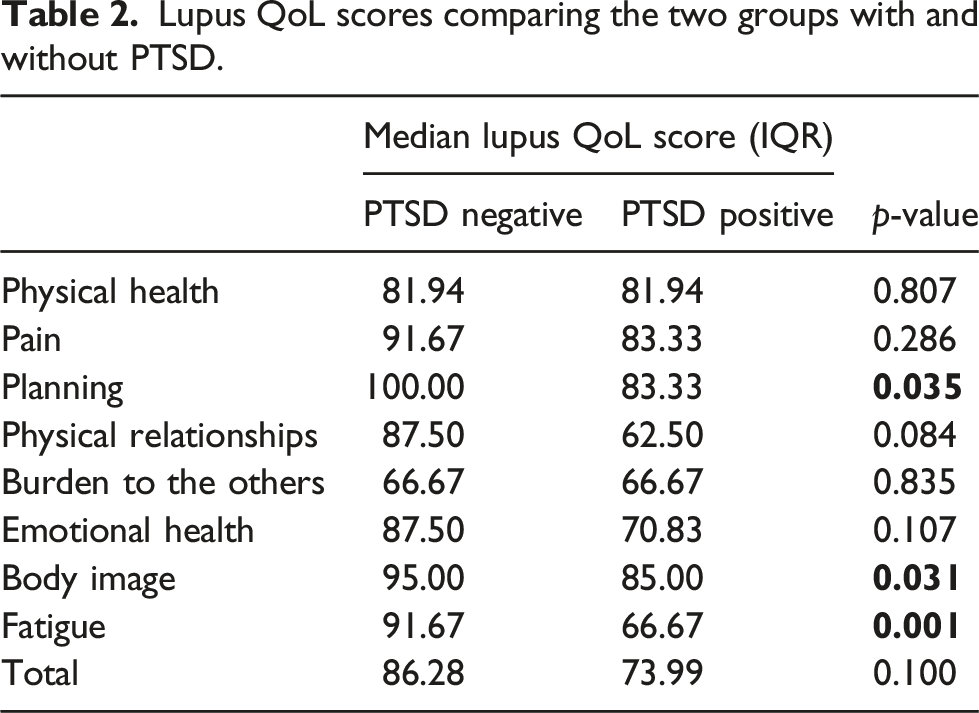
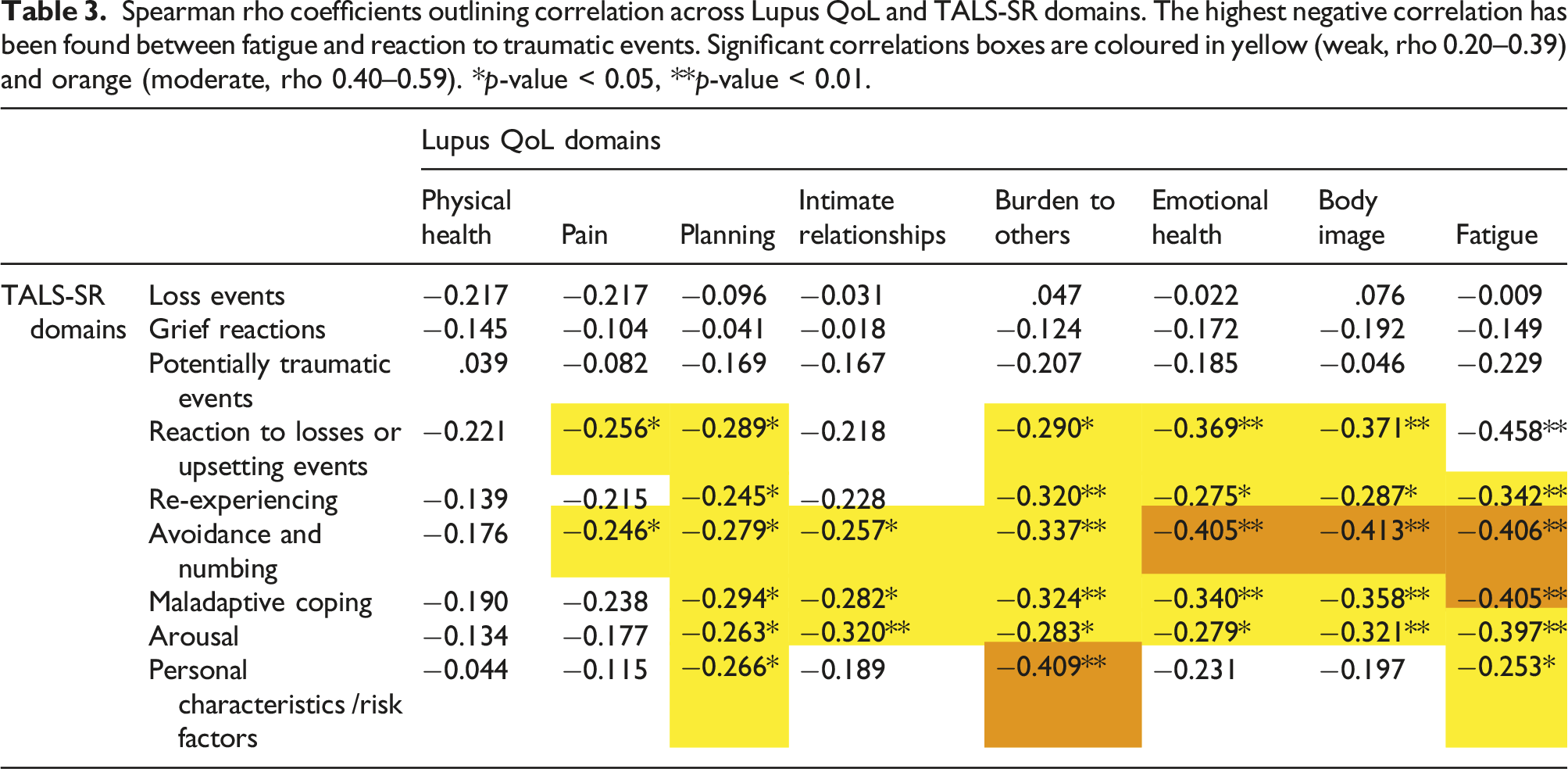
Among 99 patients who completed the questionnaire, fatigue prevalence was 75% and 31% scored TALS-SR test consistently with PTSD. Patients with PTSD achieved lower scores compared to those without PTSD in three Lupus QoL domains: planning (83.3 vs. 100, p = .035), body image (85.0 vs. 95.0, p = .031) and fatigue (66.7 vs. 91.7, p = .001). An inverse correlation was found between TALS-SR domains and Lupus QoL scores, particularly regarding fatigue with reaction to losses or upsetting events (ρ -0.458, p < .001).
Conclusions
PTSD is possibly far more frequent in patients with SLE than in general population and exerts a detrimental influence on quality of life.
Introduction
Post-traumatic stress disorder (PTSD) is a disabling psychiatric condition following traumatic events, such as threatened death, injury or sexual assault or to chronic stressors. 1 It affects 1%–12% of the general population. 2 This condition is often chronic and causes significant functional impairment, 3 in contrast to a simple exaggeration of the normal stress response. According to the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (2013), PTSD is characterized by four symptom clusters: (1) intrusive symptoms or re-experiencing of the traumatic event, (2) avoidance of reminders associated with the traumatic event, (3) hyperarousal and (4) negative alterations in mood and cognitions about oneself and others. 1 Individuals with PTSD have poor subjective overall quality of life. 4 Besides psycho-behavioural symptoms, growing evidence suggests an association between PTSD and somatic morbidity including inflammation and autoimmune diseases.3,5,6
Systemic lupus erythematosus (SLE) is a prototypical autoimmune disease, characterized by multi-organ involvement and it is mediated by humoral and cellular autoimmunity. 7 The pathogenesis of SLE remains incompletely understood, dampening appropriate classification of patients into disease subsets for diagnostic and treatment purposes. Neuropsychiatric SLE (NPSLE), stands as one of the most severe and challenging clinical manifestations of the disease and encompasses a mosaic of neurologic and psychiatric symptoms ranging from mild mood disorders or cognitive dysfunction to psychosis, stroke and epilepsy. 8 A precise definition of NPSLE is still matter of debate and algorithms for attributing neuropsychiatric manifestation to SLE often rely on a key temporal criterion of appearance with respect to SLE onset. 9 In fact, subjects with SLE often display neuropsychiatric comorbidities that can precede by years the disease onset. These manifestations are not part of lupus-related syndromes but may contribute to lupus development in a two-hits model. 10 This might also be the case of PTSD.11,12
In clinical practice, patients often interpret their somatic complaints as disease-related and this can be misleading also for experienced physicians and particularly true for fatigue and widespread pain.13,14 Attributing unspecific symptoms to SLE activity would result in heavier immunosuppression with potential unwanted consequences. Considering the effect of preceding conditions on critical aspects associated with SLE – such as quality of life, fatigue, pain perception and mood changes – would instead improve quality of life in a long-living population with SLE. So far evidence regarding the prevalence and the role of post-traumatic manifestations in SLE patients are still limited and sparse.6,11
The aim of our study was to cross-sectionally investigate the prevalence of post-traumatic stress disorder among our cohort of patients with SLE and to examine its impact on their quality of life.
Methods
A 189-item anonymous questionnaire including demographics, disease features, 9-domain Trauma and Loss Spectrum – Self Reported (TALS-SR) 15 to assess PTSD symptoms and 8-domain Lupus Quality of Life (Lupus QoL) 16 was administered by SurveyMonkey platform (https://it.surveymonkey.com) to our patients.
The questionnaire and data collection strategy were set up to avoid patient-identifiable data collection.
Data acquisition rules through SurveyMonkey were set up in order to disable Internet Protocol address recording. Although redundant due to its anonymity, all patients signed an informed consent of the wider Pan-immuno research protocol on autoimmune diseases phenotyping that included the present study. Pan-immuno protocol is conforming to the Declaration of Helsinki and approved by the Ethics Committee of IRCCS San Raffaele Hospital, Milan, Italy (registry number 22/INT/2018).
Inclusion criteria for the present study were: (a) age ≥ 18 years; (b) a definite diagnosis of SLE according to the 2012 SLICC classification criteria 17 and/or the 2019 ACR/EULAR classification criteria; 18 (c) good comprehension of the Italian language; and (d) an active e-mail account.
Disease-related variables were all self-reported and included age, sex, date of diagnosis, disease extension, symptoms and organ involvement, 0-to-10 numerical global perceived health scale, comorbidities, past and ongoing treatment including prednisone equivalent daily dose.
The frequency of demographics and general clinical features amongst responders to the survey were compared to a representative sample of randomly selected patients 19 belonging to the entire cohort (already enrolled in the Pan-immuno research protocol).
Lupus QoL is a lupus-specific health-related quality of life questionnaire consisting of 34 items grouped in eight domains: physical health, pain, planning, intimate relationships, burden to others, emotional health, body image and fatigue. A score from 0 to 100 is calculated for each domain. 16
TALS-SR is a self-report questionnaire that investigates the lifetime experience of a range of losses and/or potentially traumatic events, as well as symptoms associated with the worst event. The TALS-SR provides a dimensional approach to psychopathology by incorporating information related to subthreshold symptoms and atypical manifestations that might cause serious distress. It includes 116 items grouped into nine domains: Loss events (domain I), Grief reactions (domain II), Potentially traumatic events (Domain III), Reactions to losses or upsetting events (domain IV), Re-experiencing (domain V), Avoidance (domain VI), Maladaptive coping (domain VII), Hyperarousal (domain VIII) and Personal characteristics-risk factors (domain IX).
Item responses are coded dichotomously (yes/no) and domain scores are obtained by summing the positive answers.
The questionnaire was sent in November 2020 and maintained online for one month to ensure patients had enough time to answer.
In line with previous studies,20–23 case definition of PTSD relied on TALS-SR items corresponding to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria for PTSD. 1
Statistical analyses were performed using Microsoft Excel 2013, IBM SPSS Statistics 25, R 4.2.1 and SAS 9.4 softwares. Data are presented as median value and interquartile range (IQR) for non-normal continuous variables, and as absolute number and percentage for frequencies. Kruskal-Wallis (nonparametric) test was employed to assess differences in median values of Lupus QoL items, comparing PTSD cases versus non-PTSD. Spearman’s rank correlation coefficients were used to find correlation of Lupus QoL items and TALS-SR domains. A p-value of <0.05 was considered significant.
Results
The entire cohort of SLE patients on active follow-up at our institution counts 317 patients who fulfil 2012 SLICC classification criteria 17 and/or the 2019 ACR/EULAR classification criteria. 18 Among them, 270 were invited to participate in the survey as they own and e-mail address and agreed to use it for research purposes.
Self-reported disease characteristics (n = 99).
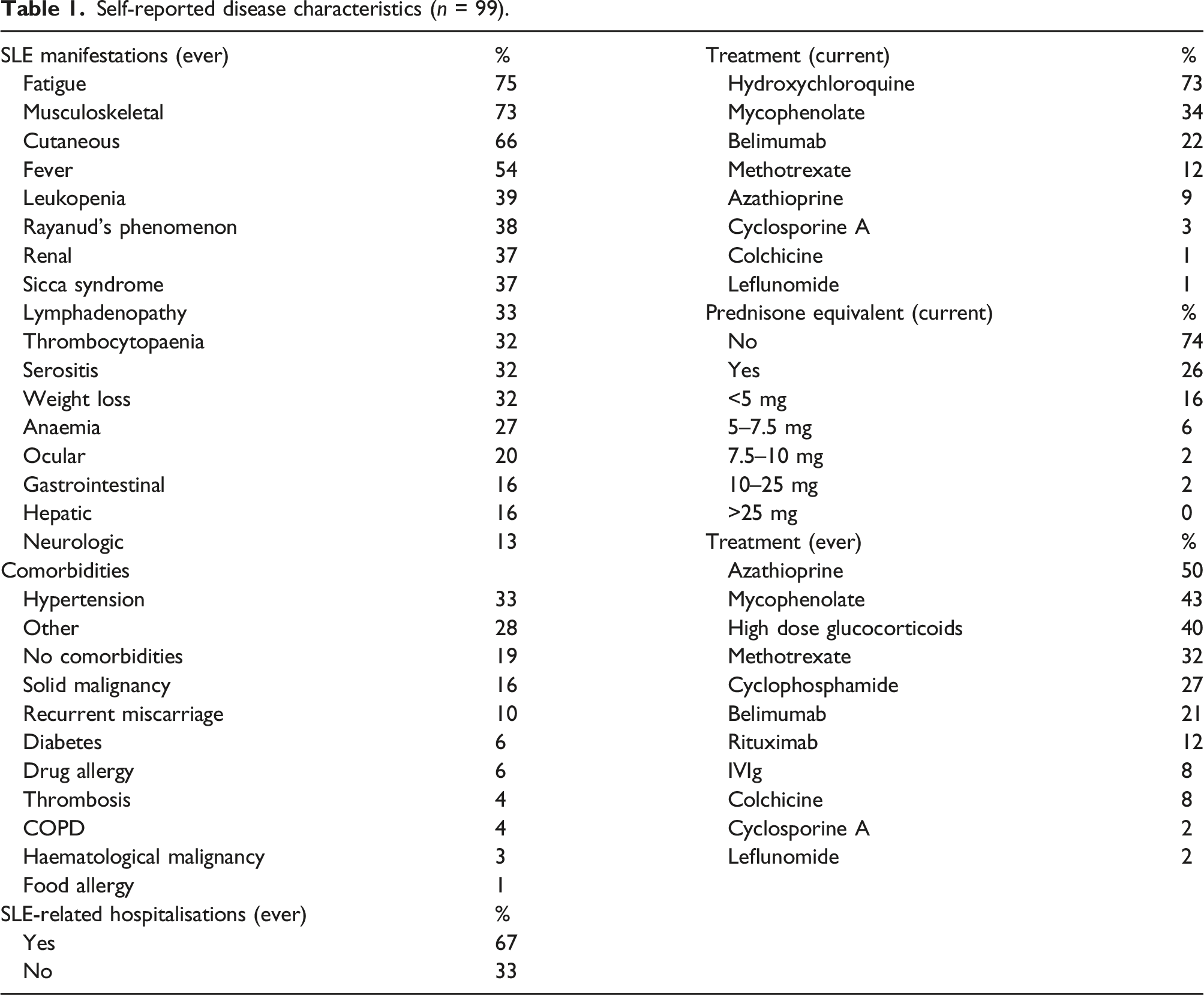
Fifteen percent (15%) of patients declared to have a psychological and/or psychiatric support mainly for depressive symptoms (40%). Details on age groups, family status, education and working life are reported as Supplementary Material (Table S1).
Responders’ sample was tested to be representative of the entire population by comparison of demographics and most objective SLE manifestations (cutaneous, neurological, and renal involvement) with a representative sample of randomly selected patients in order to avoid the bias generated by commitment in responding and self-reporting. Results of the analysis are available in Supplementary Material (Table S2).
Lupus QoL scores comparing the two groups with and without PTSD.
Ninety-three percent (93%) of the patients in our cohort experienced any type of trauma ever in life and for 59% it occurred before SLE diagnosis. Thirty-one patients (31%) scored TALS-SR questionnaire consistently with PTSD. No difference in age at SLE diagnosis or disease severity was found between trauma status groups.
Patients recorded as PTSD cases showed an increased prevalence of self-reported mucocutaneous (81% vs 59% p-value = .034) and musculoskeletal (87% vs 66%, p-value = .030) SLE involvement. No difference was outlined in ongoing and previous treatment, hospitalisation rate, number and severity of SLE manifestations.
Spearman rho coefficients outlining correlation across Lupus QoL and TALS-SR domains. The highest negative correlation has been found between fatigue and reaction to traumatic events. Significant correlations boxes are coloured in yellow (weak, rho 0.20–0.39) and orange (moderate, rho 0.40–0.59). *p-value < 0.05, **p-value < 0.01.
Discussion
In this study, we cross-sectionally analysed PTSD prevalence and its correlation with quality of life in a monocentric cohort of patients with SLE. Our results show that nearly one-third of participants met the DSM-5 criteria for PTSD. This proportion is much higher than the number of patients with a DSM-V diagnosis in the general population. 2 In one of the most comprehensive epidemiological study of mental diseases in Italy, 24 reported lifetime PTSD prevalence was 2.3% (95% CI 1.2%–3.3%), with a slight sex-related difference (1.1% in males, 3.3% in females) which is in line with international literature. 2 This was not a PTSD-restricted study and a diagnostic tool different from TALS-SR was employed to cover all mental symptoms (Composite International Diagnostic Interview). However, such a marked difference with PTSD frequency in our SLE patients couldn’t be explained by methodological heterogeneity only.
To date, this is the first report of PTSD prevalence in a SLE cohort, while a few published studies found an increased odd for incident SLE among patients with previous PTSD diagnosis11,12 or even just traumatic events. 25
When comparing clinical phenotype, patients with SLE and PTSD seem to show a more ‘typical’ pattern, with skin and joint involvement if compared with patients without PTSD. Although it’s hard to explain such a result in depth, it seems not surprising that skin manifestations with their known impact on social life would be tied to reduced psychological wellness. The same can be inferred for arthritis, often leading to chronic pain.
Fatigue is a very prevalent symptom, probably correlated with anxiety and depression rather than with inflammatory activity. 14 It affects three-quarters of the patients in our cohort, a finding which is in line with previous research14,26 and it seems to be associated with some of the specific domains of TALS-SR questionnaire, in particular with reactions to losses or upsetting events (domain IV). This evidence is in line with a previous study on patients with fibromyalgia, which found a significant correlation between symptoms of grief reactions and the VAS fatigue scores. 20 Research conducted in PTSD patients also reported high rates of simultaneous fatigue and PTSD symptoms. 27 Increased neurophysiological reactivity to excessive stress and hypothalamic pituitary axis dysfunctions, characteristic of post-traumatic stress response, may result in pathophysiological alterations in adjustment reactions to stress, disturbances in neurobiological systems and a reduced ability to sustain efforts, leading to a chronic state of fatigability and lack of energy, along with loss of muscle steadiness and chronic pain. 10
This suggests that a therapeutic strategy directed at affective symptoms might be more effective than immunomodulation to treat fatigue in patients with SLE and, at least in those in remission or low disease activity. In day-to-day clinical practice, we also suggest to include a diagnostic psychological interview at baseline, as part of the initial screening workup in all patients diagnosed with SLE. This would prevent physicians from misinterpreting psychological dysfunction as directly SLE-related in patients with distress due to longstanding chronic illness status.
One of the main limitations of our study is self-reporting bias. Patients, in fact, filled the questionnaire defining and interpreting their SLE manifestation and symptoms by their own, leading to unpredictable reliability in clinical assessment. Moreover, the questionnaire was anonymous so we were not able to correlate the results with biological data which would have been intriguing and represents our future research direction. However, this type of correlation wasn’t the main goal of the study and the lack of objective information was acceptable to prioritize anonymity in the very sensitive process of trauma telling.
In addition, fatigue was not assessed by specific validated tools (SF-36, FACIT-FATIGUE) and was patient-reported, since it was not the primary aim of our study. The statistical power is also probably affected by the low–moderate adherence.
The strength of our study is instead being the first analysis of correlation of PTSD with quality of life in an SLE cohort. Anonymous questionnaire could have been also advantageous in capturing answers on sensitive topics.
Conclusion
Our study shows that PTSD is very common in patients with SLE. As it is associated with fatigue and other quality of life dimensions, targeting anxiety and post-traumatic symptoms may be an appropriate treatment strategy. This evidence suggests that a patient-centred therapeutic approach may be far more effective in treating lupus patients than traditional disease-centred medical care. Indeed, research highlights that a multidisciplinary care, with the integration of psychological and psychotherapeutic interventions, along with other non-pharmacological therapies, produce encouraging results in SLE patients’ treatment, not only in reducing psychopathological symptoms and emotional distress but also in alleviating fatigue, pain and functional disability.28–32
Supplemental Material
Supplemental Material - Post-traumatic stress disorder in patients with systemic lupus erythematosus heavily affects quality of life. A cross-sectional web survey-based study
Supplemental Material for Post-traumatic stress disorder in patients with systemic lupus erythematosus heavily affects quality of life. A cross-sectional web survey-based study by Luca Moroni, Martina Mazzetti, Giuseppe Alvise Ramirez, Simone Zuffada, Anna Ciancio, Gabriele Gallina, Nicola Farina, Enrica Bozzolo, Valentina Di Mattei and Lorenzo Dagna in Lupus
Footnotes
Acknowledgements
A special acknowledgement goes to Dr. Naomi Viapiana (Ospedale San Raffaele) for her scientific support in statistical analyses.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.