
Abstract
Objective
We aimed to compare clinical features, outcomes, treatments, and to define the predictive factors of complete renal response (CRR) in patients with proliferative and non-proliferative lupus nephritis (LN).
Methods
Patients with systemic lupus erythematosus (SLE) followed between 2014 and 2020 at Hacettepe University Hospitals and who had a kidney biopsy were the subject of the study. One hundered and sixteen patients’ kidney biopsies reported as LN were evaluated retrospectively. Clinical characteristics and laboratory values at the time of kidney biopsy, histopathological forms of LN, and renal response (complete or partial) were recorded. We analyzed the association between CRR rates during the 2-year follow-up after induction therapy and the predictive factors for CRR.
Results
Of 116 (93 females, 23 males) patients, 95 (81.9%) were in the proliferative group (class III and IV) and 21 (18.1%) were in the non-proliferative group (class II and V). In the proliferative group, the percentage of the patients with elevated basal creatinine levels, median daily proteinuria, anti-double-stranded DNA (dsDNA) positivity, low C3 and C4 levels, the presence of active urinary sediment, and median renal SLE Disease Activity Index (SLEDAI) scores at the time of kidney biopsy were significantly higher than the non-proliferative group. Renal response status during the 2-year follow-up after induction therapy was available for 99 patients. During this time, 70 (70.7%) patients had achieved CRR and time-to-CRR was similar between the proliferative and non-proliferative groups (p = 0.64, log-rank test). The Cox proportional hazards model showed that achievement of CRR was associated with female gender [HR: 2.15 (1.19–3.89 95% CI), p = 0.011], newly diagnosed SLE with renal biopsy [HR: 2.15 (1.26–3.67 95% CI), p = 0.005], hypertension [HR: 0.40 (0.27–0.94 95% CI), p = 0.032], eGFR increase [HR: 1.01 (1.00–1.01 95% CI), p = 0.046], and the presence of active urinary sediment [HR: 0.46 (0.22–0.96 95% CI), p = 0.039].
Conclusions
Achieving CRR was similar in proliferative and non-proliferative LN patients, although certain laboratory parameters differed at the onset. Our results indicated the importance of kidney biopsy in the decision-making of treatment of SLE patients with renal involvement and that the defined factors associated with CRR achievement help to predict good renal response.
Introduction
Lupus nephritis (LN) is a form of glomerulonephritis, which is one of the causes of serious organ involvement in systemic lupus erythematosus (SLE). LN, which occurs in 60–70% of patients with SLE, is a major determinant of morbidity and mortality. 1 Although LN class estimation can be made with available laboratory findings (such as kidney function, serology, and urinary sediment), kidney biopsy is required for the definitive diagnosis and classification of LN. 2 Kidney biopsy demonstrates active, chronic, or mixed types of glomerular injury and accompanying vascular and/or tubulointerstitial lesions. It also helps to identify the causes of non-LN, reported in approximately 5% of SLE patients. 3
The International Society of Nephrology/Renal Pathology Society (ISN/RPS) classification of LN is currently the gold standard for choosing the appropriate therapy; however, individuals from the same LN class could have different responses to the same treatment. This difference has been associated with individual characterization of histopathological lesions.4,5 Proliferative LN (class III and IV/±V) has a more fulminant course, and these patients need more aggressive treatment to achieve remission and prevent kidney damage. 6 Treatment response is evaluated as complete or partial renal response. At the end of the first year, complete renal response rates range from 10 to 58% and partial renal response rates range from 24 to 52%.7–10 Early-onset LN, female gender, absence of renal exacerbation, and anti-SSB antibodies have been reported as positive predictors for complete renal response.7,11
During the follow-up, 27–66% of LN patients experience at least one renal relapse. 12 Despite current treatment options, the rate of progression to end-stage renal disease in LN patients was between 4 and 28%. 13 Elevated basal serum creatinine levels, diffuse proliferative glomerulonephritis, tubular atrophy, low complement levels, and anti-Ro antibodies were reported to be the independent risk factors for ESRD progression. 14
Most of the studies on LN include patients with proliferative forms of the disease. However, clinical, laboratory, and serological follow-up during the course of the disease are also important in terms of renal prognosis in non-proliferative LN patients. 15
The aim of this study was to compare the clinical features and treatment response rates of proliferative and non-proliferative LN patients and to identify the related factors in patients who achieved complete renal response during the 2-year follow-up.
Materials and methods
Study protocol and patients
This retrospective, descriptive study included the patients with LN who were followed in the Rheumatology and Nephrology Departments of Hacettepe University Faculty of Medicine. Patients with SLE between 2014 and 2020 were identified from the hospital's electronic medical records by using the International Classification of Diseases (ICD)-10 code for SLE (M32). Systemic lupus erythematosus diagnosis was confirmed according to the 2012 SLICC (Systemic Lupus International Collaborating Clinics) and/or 2019 EULAR (European League Against Rheumatism)/ACR (American College of Rheumatology) criteria. Among all SLE patients, those who underwent kidney biopsy were screened. One hundred and eighty-eight patients with LN were reviewed, and 49 kidney biopsies performed in different hospitals were excluded. Additionally, 23 kidney biopsies detailed in the results were also excluded from the study for various reasons. The data of the remaining 116 patients with LN whose specimens were evaluated in the Pathology Department of Hacettepe University Hospitals were included in the study. This study was approved by Hacettepe University Ethics Committee (Approval number: GO 2020/07-14).
Data collection
The demographic data involved age at the onset of both SLE and LN, gender, disease duration of SLE, time from the diagnosis of SLE until the kidney biopsy, family history of SLE, and LN follow-up time. Hypertension, diabetes mellitus, and secondary rheumatologic diseases (Sjogren's syndrome and antiphospholipid syndrome) were recorded. In addition, non-renal clinical manifestations of SLE were also noted.
Biopsy results of the patients with LN were obtained from pathology reports evaluated by a nephropathologist according to the ISN/RPS classification. The pathology results other than LN were also noted. Class 3 and class 4 LN were grouped as proliferative LN, while other LN forms were grouped as non-proliferative LN.
The laboratory data recorded at the time of kidney biopsy were as follows: serum creatinine (Cr) and albumin, 24-hour total urine protein, estimated glomerular filtration rate (eGFR, according to CKD-EPI), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), as well as immunologic parameters including complement 3 (C3), complement 4 (C4), anti-dsDNA antibodies, and anti-Smith antibodies. Anti-dsDNA, C3, and C4 values were also classified as positive and negative according to the laboratory upper limit. Antinuclear antibody (ANA) titers analyzed by immunofluorescence method were grouped as ≤1/100, 1/160, 1/320, and ≥1/640. Anti-dsDNA was studied by ELISA method, and serum levels were given quantitatively.
Treatment, renal response, and outcome
The induction therapies (pulse steroid, oral steroid, and immunosuppressive agents) given according to the treating physician’s decision were documented. For renal involvement, renal SLE Disease Activity Index (SLEDAI) was used to assess kidney disease activity. The score consists of the four kidney-related parameters: hematuria, pyuria, proteinuria, and urinary casts. Scores for the renal SLEDAI can range from 0 (inactive renal disease) to a maximum of 16. 16
Response to therapy included complete renal response (CRR), partial renal response (PRR), no response, end-stage renal disease (ESRD), and death. Complete renal response was defined as inactive urinary sediment, proteinuria <0.2 g/day, and normal or stable renal functions (serum creatinine ≤1.2 mg/dL and 25% increase if baseline GFR ≤75 mL/min). Partial response response was defined as inactive urinary sediment, 0.21–2 g/day proteinuria, and normal or stable renal functions (serum creatinine ≤1.2 mg/dL and 25% increase in GFR if baseline GFR ≤75 mL/min).10,17 If relapse developed during the 2-year follow-up period of patients who had a complete/partial renal response, the time of renal relapse was recorded. Renal relapse was indicated by proteinuria (>0.5 g/day after CRR or doubling of proteinuria after PRR) or increase in serum creatinine or decrease in creatinine clearance (serum creatinine ≥30% or decrease in GFR ≥ 10%) and abnormal urinary sediment.12,18 End-stage renal disease was defined as the need for regular dialysis and/or GFR <15 mL/min and/or history of renal transplantation. 10 All patients who died were recorded, including the cause of death.
The renal response and relapse rates of the patients during the 2-year follow-up after LN diagnosis were determined. ESRD, death, and renal transplantation rate were also noted for both during the 2-year follow-up and the last visit.
Statistical analysis
Statistical analysis was performed using the IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, NY, USA). The variables were tested for normality using the visual (histogram and probability plots) and analytic methods (Kolmogorov-Smirnov, skewness, and kurtosis). Continuous data were expressed as median (inter-quartile range, IQR) or mean (standard deviation, SD) and categorical variables were expressed as percentages. Chi-square test was used to compare categorical variables and Mann–Whitney U test/student’s t-test was used to compare continuous variables. Kaplan–Meier test was used for CRR achievement during the 2-year follow-up according to proliferative and non-proliferative LN, and compared with log-rank test. Possible factors identified with univariate analysis (p < 0.20) were entered into the Cox regression analysis to determine independent predictors of CRR achievement during the 2-year follow-up.
Results
The results of 139 kidney biopsies evaluated in the Pathology Department of Hacettepe University Hospitals were as follows: 116 LN, 18 renal pathologies other than LN, 3 biopsies unsuccessful, and 2 biopsies normal (Figure 1). Renal pathologies other than LN were as follows: 6 (4.3%) focal segmental glomerulosclerosis (FSGS), 4 (2.9%) membranous nephropathy, 3 (2.2%) thrombotic microangiopathy, 2 (1.4%) IgM nephropathy, 2 (1.4%) tubulointerstitial nephritis, and 1 (0.7%) proliferative glomerulonephritis with monoclonal IgG deposits. Flowchart of the study patients. ICD: International Classification of Diseases; LN: Lupus nephritis; SLE: Systemic lupus erythematosus. CRR: Compleate renal response, ESRD: End-stage renal disease, NR: No response, PRR: Partial renal response.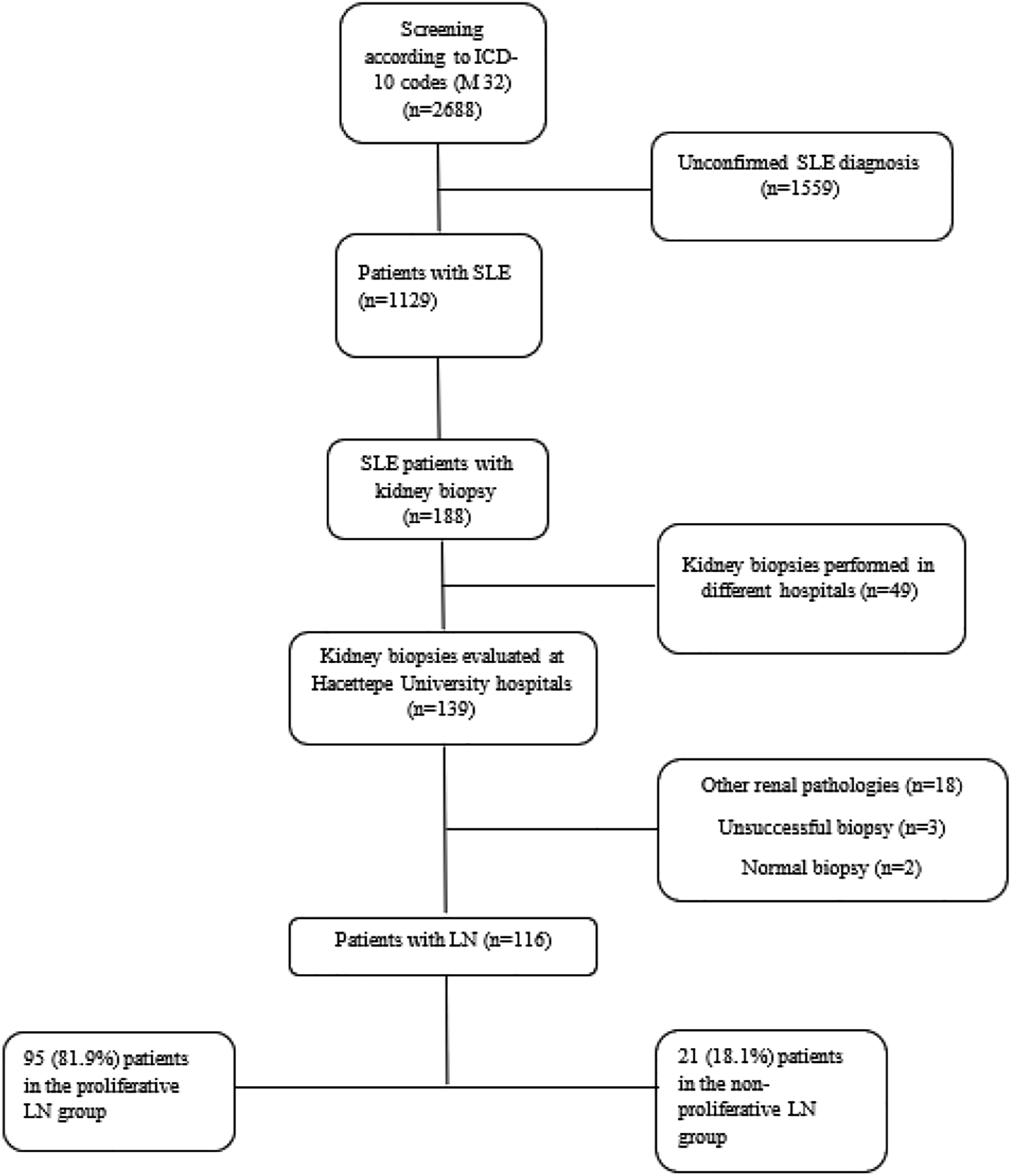
Patients’ baseline characteristics and LN classification
A total of 116 patients with biopsy-proven LN were included. Thirty-four (29.3%) patients had juvenile-onset LN (<16 years). The median (IQR) age at SLE diagnosis was 18.3 (16) years, and the median age at the time of kidney biopsy was 21 (17.7) years. Of the patients, 93 (80.2%) were female, and 65 (56%) patients had LN at the time of SLE diagnosis. The median follow-up time for LN was 5.5 (8) years.
Demographic and clinical characteristics of proliferative and non-proliferative LN patients.
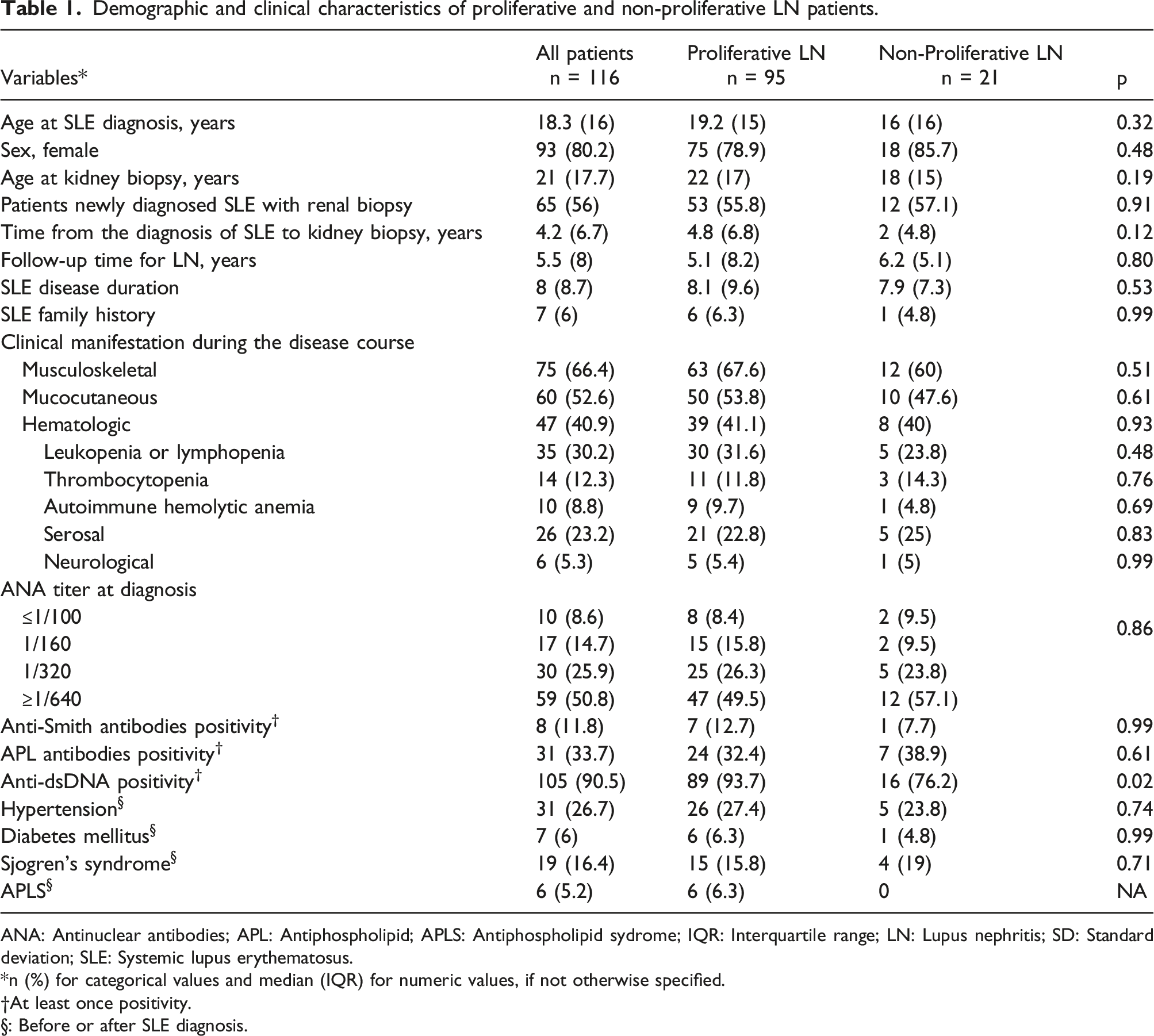
ANA: Antinuclear antibodies; APL: Antiphospholipid; APLS: Antiphospholipid sydrome; IQR: Interquartile range; LN: Lupus nephritis; SD: Standard deviation; SLE: Systemic lupus erythematosus.
*n (%) for categorical values and median (IQR) for numeric values, if not otherwise specified.
†At least once positivity.
§: Before or after SLE diagnosis.
Laboratory values at the time of kidney biopsy
Laboratory values at the time of kidney biopsy.
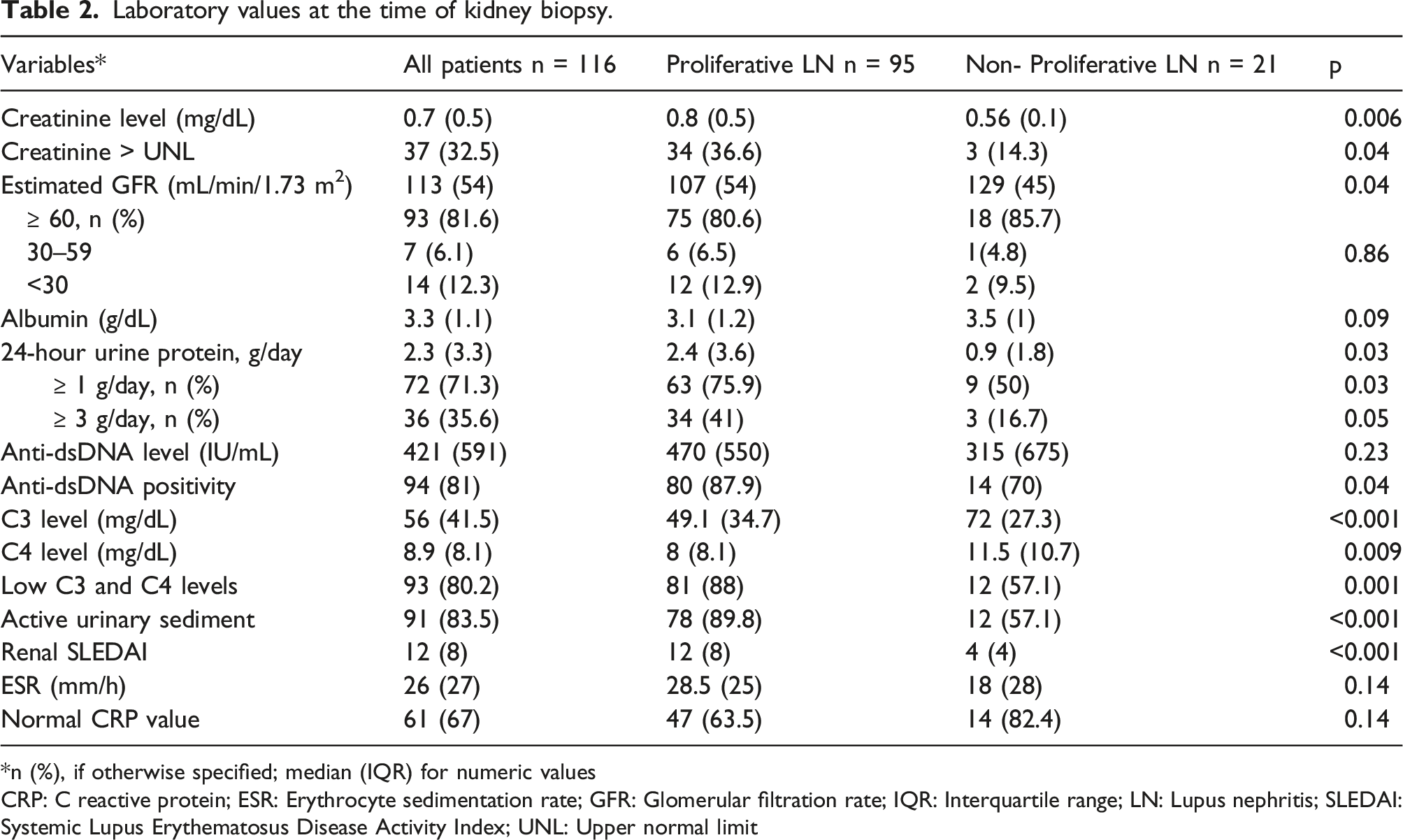
*n (%), if otherwise specified; median (IQR) for numeric values
CRP: C reactive protein; ESR: Erythrocyte sedimentation rate; GFR: Glomerular filtration rate; IQR: Interquartile range; LN: Lupus nephritis; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; UNL: Upper normal limit
Distribution of patients according to GFR
Of all patients, 93 (81.6%) patients had an eGFR ≥60 mL/min/1.73 m2 and 21 (18.4%) patients had an eGFR <60 mL/min/m2. In patients who had GFR ≥60 mL/min, 75 (80.6%) patients were class III or IV LN, and 18 (19.4%) patients were class II or V LN. Seven (7.7%) patients with combined LN (class III+V or class IV+V) had an eGFR ≥60 mL/min/1.73 m2. In patients who had an eGFR <60 mL/min, 18 (85.7%) patients were LN III or LN IV, one patient was LN II, and two patients were LN V. When the patients were compared regarding eGFR, the distribution of patients with proliferative LN and non-proliferative LN was similar (80.6 vs. 85.7% for proliferative LN, 19.4% vs. 14.3% for non-proliferative LN).
LN treatment
Treatment characteristics for proliferative and non-proliferative lupus nephritis patients.
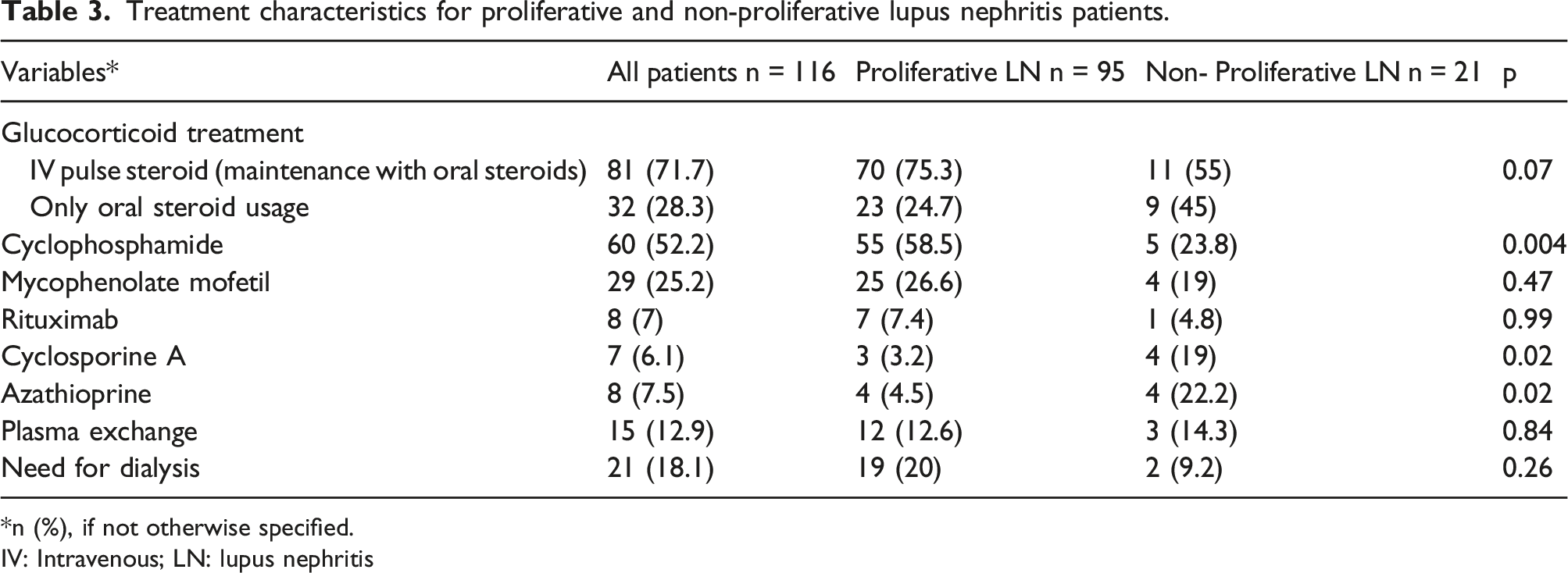
*n (%), if not otherwise specified.
IV: Intravenous; LN: lupus nephritis
Renal outcome
The treatment response could not be evaluated in 17 (14.6%) patients because of missing clinical data. During the 2-year follow-up after LN diagnosis, 70 patients (70.7%) achieved CRR, and 23 patients (23.3%) achieved PRR. CRR and PRR achievement rates were similar for both the proliferative and non-proliferative groups. Twenty of the 93 patients (21.5%) experienced at least one renal relapse during the 2-year follow-up after LN diagnosis. Six (6.1%) patients were accepted as non-responsive to treatment, and all of them were in the proliferative group. Four patients (4.2%) developed ESRD, and three patients deceased in the proliferative LN group. The causes of death were pneumonia, urosepsis, and cardiomyopathy (Figure 2). Treatment response and renal outcome of proliferative and non-proliferative lupus nephritis patients during the 2-year follow-up after LN diagnosis.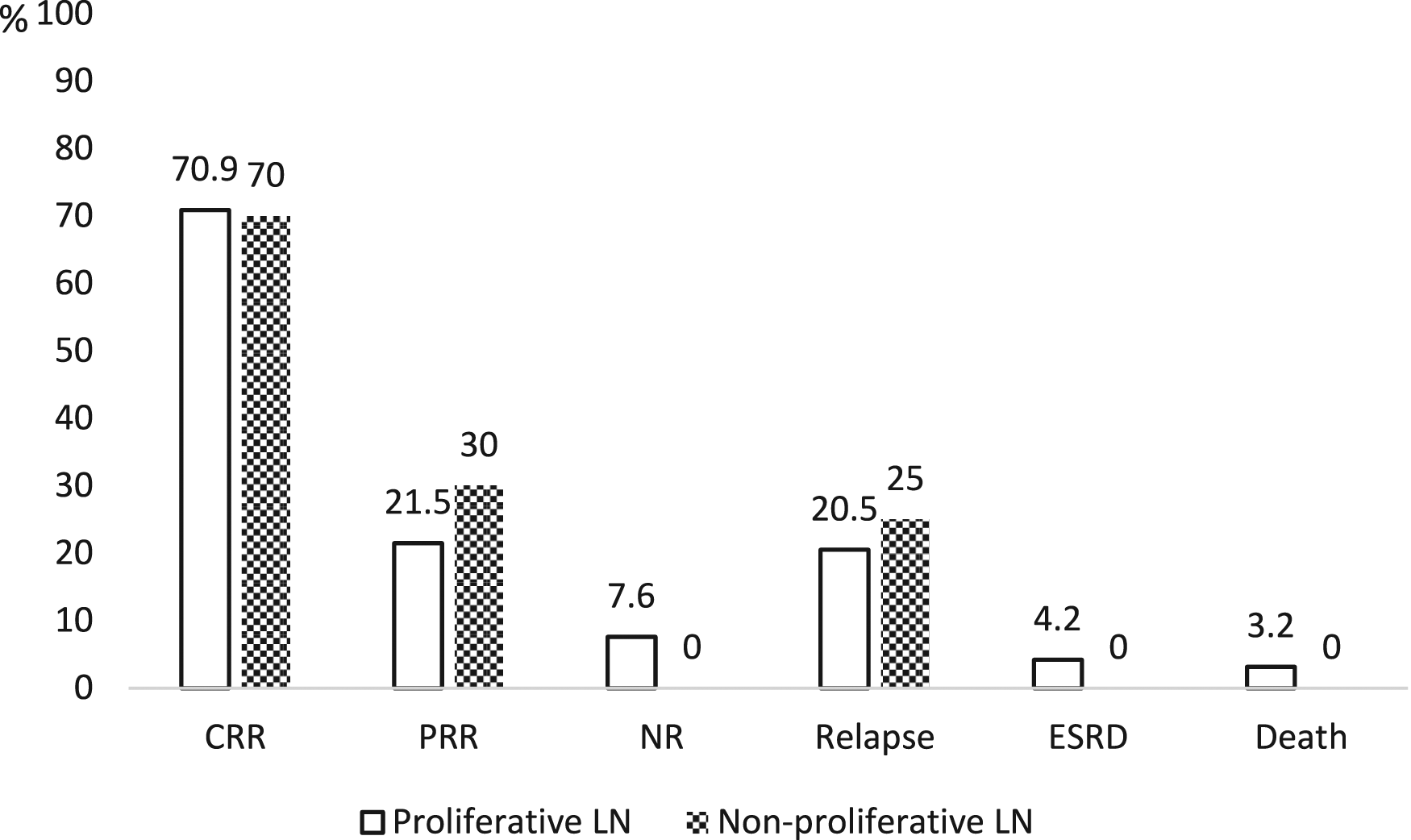
Among the patients included in the study, 13 (11.2%) patients were diagnosed to have ESRD, 8 (7%) patients died, and 5 (4.3%) patients received a kidney transplant. The rates of these events were similar in both groups.
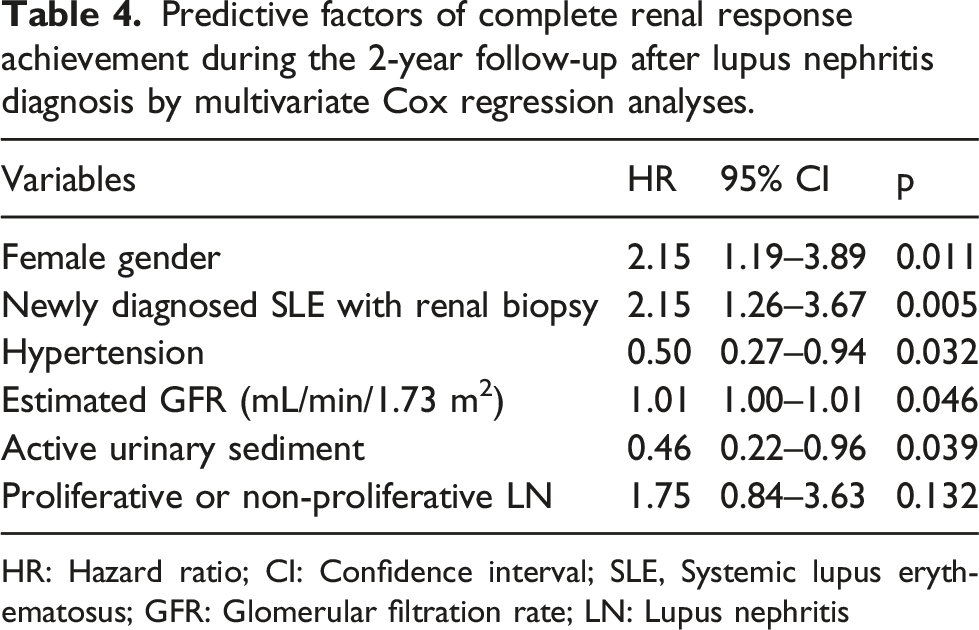
The Kaplan–Meier analysis showed no difference between the proliferative and non-proliferative groups in terms of the time to achievement of CRR during the 2-year follow-up after LN diagnosis (Figure 3). The Cox proportional hazards model after adjustment showed that, achievement of CRR was associated with female gender (HR: 2.15 (1.19–3.89 95% CI), p = 0.011), newly diagnosed SLE with renal biopsy (HR: 2.15 (1.26-3.67 95% CI), p = 0.005), hypertension (0.40 (0.27-0.94 95% CI), p = 0.032), eGFR increase (HR: 1.01 (1.00-1.01 95% CI), p = 0.046), and the presence of active urinary sediment (HR: 0.46 (0.22-0.96 95% CI), p = 0.039) (Table 4). Kaplan–Meier survival curve for complete renal response (CRR) achievement during the 2-year follow-up according to the kidney biopsy results. Predictive factors of complete renal response achievement during the 2-year follow-up after lupus nephritis diagnosis by multivariate Cox regression analyses. HR: Hazard ratio; CI: Confidence interval; SLE, Systemic lupus erythematosus; GFR: Glomerular filtration rate; LN: Lupus nephritis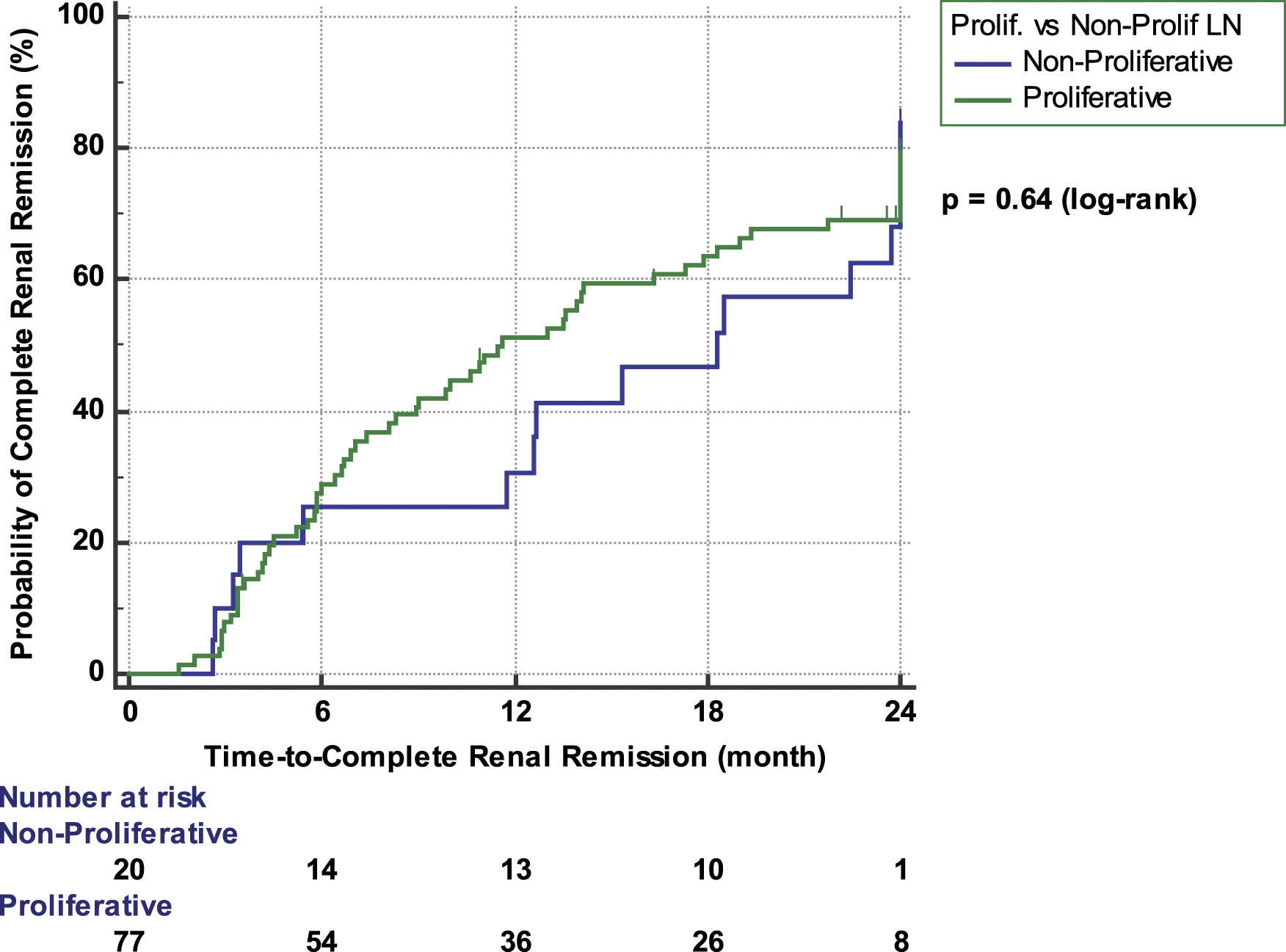
Discussion
In this study, we highlighted the differences between proliferative and non-proliferative LN patients in terms of laboratory characteristics, treatment approaches, and renal outcomes. Most of our patients were in the proliferative group. The percentage of patients with increased creatinine level, active urinary sediment, positive anti-dsDNA, low level of C3 and C4, median daily proteinuria, and renal SLEDAI scores were higher in this group. Interestingly, CRR achievement rate during the 2-year Follow-up was similar for both proliferative and non-proliferative groups.
The presence of proteinuria and active urinary sediment is primarily suggestive of LN in patients with SLE. Kidney biopsy plays a crucial role in the diagnosis of both specific LN forms and other causes of non-LN. In an American cohort, the rate of non-LN in kidney biopsy of SLE patients was found to be 5%. 3 In our study, this rate increased up to 13%, and the most common pathology was FSGS. This result emphasized the importance of biopsy in the evaluation of renal involvement in patients with SLE.
Up to 50% of SLE patients have clinically evident kidney disease at presentation and during follow-up; kidney involvement occurs in approximately three-quarters of patients, with an even greater representation among children and young adults. 15 Similarly, in our research, LN was present in 56% of the patients at the time of SLE diagnosis, and the age at SLE diagnosis was 18 years, and the age at LN diagnosis was 21 years. In previous studies, the age at SLE diagnosis and the age at LN diagnosis were usually in the third and fourth decades.19–22 However, these studies did not include the patients with juvenile-onset LN while our cohort was younger, which was associated with the presence of juvenile-onset LN patients.
Serum creatinine, eGFR, urinary sediment, urinary proteinuria, and complement and ds-DNA levels are the frequently used laboratory parameters in the clinical follow-up of LN. Unfortunately, these tests are not sufficient to predict the histopathological type of LN. Only a few studies reported anti-C1q alone or in combination with anti-dsDNA and complement levels as a reliable test in differentiating proliferative and non-proliferative LN.23,24 In our study, the percentages of patients with anti-dsDNA positivity and low complement level were significantly higher in the proliferative LN group; these rates were 70% and 57% in the non-proliferative LN group, respectively. In addition, median daily proteinuria (0.9 g/day) was significantly lower in the non-proliferative group. Similarly, Moroni et al. 24 reported that the percentage of patients with anti-ds DNA positivity was 50%, those with low complement levels was 65%, and median daily proteinuria was 1.9 g/day in non-proliferative LN patients. The fact that non-LN causes may be detected in kidney biopsies of patients with SLE and that the markers used in daily practice cannot guide the differentiation of proliferative and non-proliferative LN reveal the requirement of kidney biopsy before the treatment decision.
As our study has a retrospective design, there was no standard treatment protocol for the treatment of LN, and different clinicians have treated the patients. For induction therapy, oral and/or IV corticosteroids were given to all patients, and CYC was used in approximately half of the patients, particularly in the proliferative LN group. Mycophenolate mofetil (MMF) was the second commonly used induction agent. Although RTX is a promising therapy for the treatment of LN due to its significant clinical efficacy and favorable safety profile, 25 it has been preferred in fewer patients in our study since it is off-label for LN treatment in Turkey. Therefore, no additional comments could be made for renal response in this study because of the small number of patients using RTX.
Plasmapheresis as an add-on therapy is a helpful tool to induce a faster remission in LN; however, it does not contribute to immunosuppressive therapy in terms of long-term renal prognosis.26,27 Therefore, plasmapheresis is not routinely used in patients with LN; however, it can be an additional treatment option in patients with severe crescentic LN or proliferative LN with co-existing antiphospholipid antibodies. In our study, plasmapheresis was applied to eleven of 21 patients with severe LN who needed dialysis at the beginning of the treatment.
In the present study, the patients' treatment response during the 2-year follow-up after renal biopsy were evaluated. CRR and PRR were achieved in 70 and 23% of the patients, respectively. In these patients, the rate of renal relapse was 21.5%. Recent studies indicated that the rate of CRR varied between 20 and 65%, and the rate of PRR is between 18 and 27%.10,21,28 Renal response rates obtained in our study were rather consistent with previous reports. Factors predicting CRR during the 2-year follow-up were also analyzed. In multivariate survival analysis, we found that female gender, newly diagnosed SLE with renal biopsy, and increased GFR were independent indicators of CRR, and the presence of hypertension and active urinary sediment were associated with decreased probability for CRR achievement. In a large LN cohort from Egypt, elevated basal serum creatinine, renal relapse, and hypertension were associated with poor renal outcome. 10 Similarly, in another study, hypertension, lower GFR, and failure to achieve complete remission in the first year of treatment were significant predictors of the development of chronic kidney disease in LN patients. 29 A multicenter cohort including 499 LN patients revealed that male gender, hypertension, absence of maintenance immunosuppressive therapy, increased serum creatinine, and a high index of activity and chronicity were independent predictors of ESRD. 30 In a study regarding the histopathologic findings of LN, class IV and chronic interstitial damage at initial renal biopsy were associated with worse renal outcomes. 21 In our study, although all patients who did not respond to treatment, developed ESRD, and died during the 2-year follow-up were in the proliferative LN group, the complete or partial renal response rates were similar in both groups. This situation may be explained by the small number of patients in the non-proliferative group.
The LN patients were followed for a median of 5.5 years in this study. During this time, 11% of the patients developed ESRD, and 7% of the patients died. In a meta-analysis, the cumulative incidence of developing ESRD in LN patients at 5, 10, and 15 years ranged from 3 to 11%, 6 to 19%, and 19 to 25%, respectively. 31 Previous studies demonstrated that the 5-year mortality rate changed between 7.4% and 13% and the 10-year mortality rate increased up to 17%.10,32 Our findings were similar to those reported in the literature.
The strength of our study was that all patients had renal biopsy evidence for LN, and 85% of them had follow-up data during the 2-year follow-up, although the study has a retrospective design. However, our study had also some limitations. The main limitation was the small number of patients with non-proliferative LN included in the analysis, as our study was a single-center study. Another limitation was the retrospective observational study design, which prevented to draw clear conclusions about the follow-up of patients, such as switching or tapering treatment. The other limitation was that there was no standard treatment regimen as the patients were followed up in different departments. In addition, the absence of activity and chronicity findings in kidney biopsies was the last limitation. Finally, we think that most patients with non-proliferative LN do not undergo kidney biopsy. This may have created a bias in patient selection for the study.
In conclusion, the characteristics of patients with biopsy-proven LN followed in a single-center are presented in the present study. Renal involvement other than LN can be established at a significant rate in renal biopsies of patients with SLE. During the 2-year follow-up after induction therapy, 70% of the patients achieved CRR. We found that achievement of CRR after induction therapy was associated with female gender, newly diagnosed SLE with renal biopsy, hypertension, eGFR increase, and the presence of active urinary sediment. Our results indicated the importance of kidney biopsy in the decision-making of treatment of LN patients and the factors associated with CRR achievement would help to predict good renal response.
Footnotes
Authorship contributions
Emine Duran and A.Ihsan Ertenli designed the study. Tolga Yıldırım and Umut Kalyoncu supervised the project. Arzu Taghiyeva collected data. Emine Duran, Umut Kalyoncu, and Emre Bilgin performed the data analysis and wrote the manuscript. Mustafa Arıcı, Seza Özen, Yunus Erdem, Emine Arzu Sağlam, and Meral Üner reviewed the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by Hacettepe University Ethics Committee (Approval number: GO 2020/07-14).