
Abstract
Introduction
At least 38% of patients with Systemic Lupus Erythematosus (SLE) experience cognitive impairment (CI). Patients report CI impacts their health-related quality of life (HRQoL) and social role participation.
Objectives
To synthesize and critically appraise the quantitative literature on the relationship of CI to HRQoL and social role participation in individuals with SLE.
Methods
Six electronic databases were searched in December 2018 and June 2020 by an information specialist. Two reviewers independently completed all screening phases and data extraction; a third reviewer resolved disagreements. The Mixed Methods Appraisal Tool was used to critically appraise the quality of included studies. Data has been synthesized and analyzed descriptively to present evidence on the relationship of CI to HRQoL and social role participation.
Results
A total of 7182 references were identified and screened, with 14 articles included. Four of the included articles investigated the relationship between CI and HRQoL and all identified a negative relationship. Ten of the 14 studies investigated CI and social role participation, eight identified a negative relationship. There was heterogeneity of measures used between studies to examine CI, HRQoL, and social role participation. As such, results were interpreted descriptively and could not be pooled for meta-analysis.
Conclusion
The presence of CI is negatively related to HRQoL and social role participation in patients with SLE. Healthcare professionals should be aware of this relationship so that it can be addressed in clinical practice. Further research, using consistent methods of quantifying CI, HRQoL and social role participation, is needed to enable data pooling.
Keywords
Significance and innovations
Fourteen studies were identified that quantitatively described the relationship between CI and a) health-related quality of life or b) social role participation There is heterogeneity of measures used to quantify cognitive impairment, health-related quality of life and social role participation in the literature The presence of CI is negatively related to HRQoL and social role participation in patients with SLE, indicating that CI is an important factor to consider for holistic SLE care and research.
Systemic Lupus Erythematosus (SLE) is a chronic autoimmune disease that affects multiple organ systems and presents with a myriad of variable symptoms.
1
The pooled prevalence of cognitive impairment (CI) in individuals living with SLE is 38%.
2
Patients with SLE are at a higher risk of developing CI symptoms compared to healthy subjects and patients with rheumatoid arthritis.
2
CI is defined as significant deficits or impairments in one or multiple cognitive domains including memory (learning and recall), simple and complex attention, visual-spatial processing, language (e.g. verbal, fluency), psychomotor speed and/or executive functions (behaviour initiation/inhibition, planning, organizing, sequencing; reasoning/problem solving; judgement).
3
Individuals with SLE who experience CI have reported it has a substantial impact on their health-related quality of life and social role participation.2,4 However, to date, the quantitative evidence on the relationship between CI and these outcomes has not been synthesized.
Health-related quality of life (HRQoL) describes the physical, mental, and social aspects of health that are influenced by an individual’s life experiences and expectations. 5 Individuals with SLE experience lower HRQoL compared to healthy individuals, especially with active SLE disease.6,7 Further, studies of adults with SLE report lower HRQoL compared to individuals with other chronic conditions.8,9 Two previous reviews of HRQoL of individuals with SLE have found various SLE related factors affect HRQoL.7,10 However, CI was not addressed in either review.
Social role participation encompasses any activity that is related to taking part in a “life situation” or “life role.” 11 SLE affects an array of daily activities and social roles.7,12–15 A recent review on employment in adult SLE patients, the primary social role studied in adults living with SLE,7,12–14 estimated that employment rates are 26 to 54% for adults with SLE, well below the employment rates of adults without chronic health conditions. 7 A 2009 review highlighted the relationship between employment and psychosocial and disease-related factors for individuals with SLE. 16 However, the relationship of CI and employment was not discussed in these reviews.7,16
While SLE has a documented influence on HRQoL and social role participation, and individuals with SLE have reported that CI symptoms significantly impacts these outcomes, the relationship of CI to HRQoL and social role participation of individuals with SLE has not been synthesized. Synthesizing these relationships within existing evidence can help to (a) determine the areas of HRQoL and social role participation influenced by CI that may require tailored interventions, and (b) identify evidence gaps for future research. Therefore, the
Methods and materials
A protocol using the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 17 guideline was developed a priori and was used to guide this review. This protocol was registered online with PROSPERO (registration number: CRD42019122630). This review used PRISMA guidelines. 18
Data sources
Six databases were electronically searched in December 2018 and June 2020 by an information specialist (MA) experienced in database searches and systematic review methods. The two separate searches overlapped, such that any literature published in November and December 2018 was identified in both literature searches. The following databases were searched: 1) OVID Medline ALL; 2) OVID Embase; 3) OVID Cochrane Database of Systematic Reviews; 4) OVID APA PsycINFO; 5) EBSCO CINAHL and 6) OVID Emcare Nursing. These databases include literature across health disciplines and geographical areas. Reviewers completed forward citation searches using the Web of Science database and backward citation searches (i.e. references) of included articles to identify all relevant literature.
Search terms, screening and selection
Search terms included those relating to SLE (n= 3 terms), HRQoL (n= 7 terms), social role participation (n= 88 terms) and CI (n= 82 terms). Social role participation terms were based on the World Health Organization’s International Classification of Functioning, Disability and Health, 11 to build a broad and inclusive search. Searches were limited to human subjects, but not limited by age group or year of publication. The search maps per database are in Online Appendix A.
Duplicates were removed and two reviewers independently screened titles, abstracts, and full text articles using a priori inclusion and exclusion criteria (Online Appendix B). Agreement was reached after title/abstract screening and full article selection. A third reviewer resolved any disagreements. Included studies were all a quantitative design, included an SLE sample, measured at least one cognitive domain or overall cognition, measured HRQoL or social role participation, and analyzed the association between CI and HRQoL/social role participation.
Critical appraisal, extraction and synthesis
Two reviewers independently completed data extraction for each included article using an a priori data extraction form. Extracted data included: a) demographics of participants; b) measures of cognitive impairment, HRQoL and social role participation; and c) study results. The extraction form was pilot tested on two articles to ensure data was extracted in a standardized and comprehensive manner. After piloting the form, the remaining articles underwent data extraction by two independent reviewers, who met to come to agreement; a third reviewer resolved any remaining disagreements.
The Mixed Methods Appraisal Tool (MMAT)19,20 was used to critically appraise the quality of the included articles. Specifically, two sections of the MMAT, Screening and Quantitative non-randomized studies (‘Results’ section), were used because these sections include appraisal items for cohort and cross-sectional design. Two reviewers independently rated each of the included articles and reviewed the scores in an agreement meeting. There were no disagreements that required a third reviewer.
Data was synthesized and analyzed descriptively, examining: 1) relationships between a) CI and HRQOL, and b) CI and social role participation; 2) measures of CI, HRQoL, and social role participation; and 3) socio-demographic characteristics and geographic regions of the SLE population in the included studies. Adult and pediatric data have both been reported and described separately. Due to the heterogeneity of statistical tests and measures used across the studies, results could not be pooled for a correlational meta-analysis. 21 Therefore, the analysis and synthesis were descriptive. For social participation, measures were grouped into employment, academic, and other valued life activities. When sufficient statistical data was provided, values were interpreted such that r <0.3 was indicative of a weak correlation, r= 0.3-0.7 was indicative of a moderate correlation, and r >0.7 was indicative of a strong correlation. 22
Results
After removing duplicates using referencing software, 5652 titles were identified in the 2018 search and 1028 titles in the 2020 update search. After screening and selection, 14 articles were included (Figure 1). Four articles23–26 explored the relationship between CI and HRQoL and 1027–36 articles examined the relationship between CI and social role participation. Twelve articles used a cross-sectional design23–26,28–33,35,36, while the remaining two articles were cohort studies.27,34 The pooled sample size across all fourteen studies was 3144 SLE patients, ranging from 15 to 897 per study. A summary of included studies is presented in Table 1.
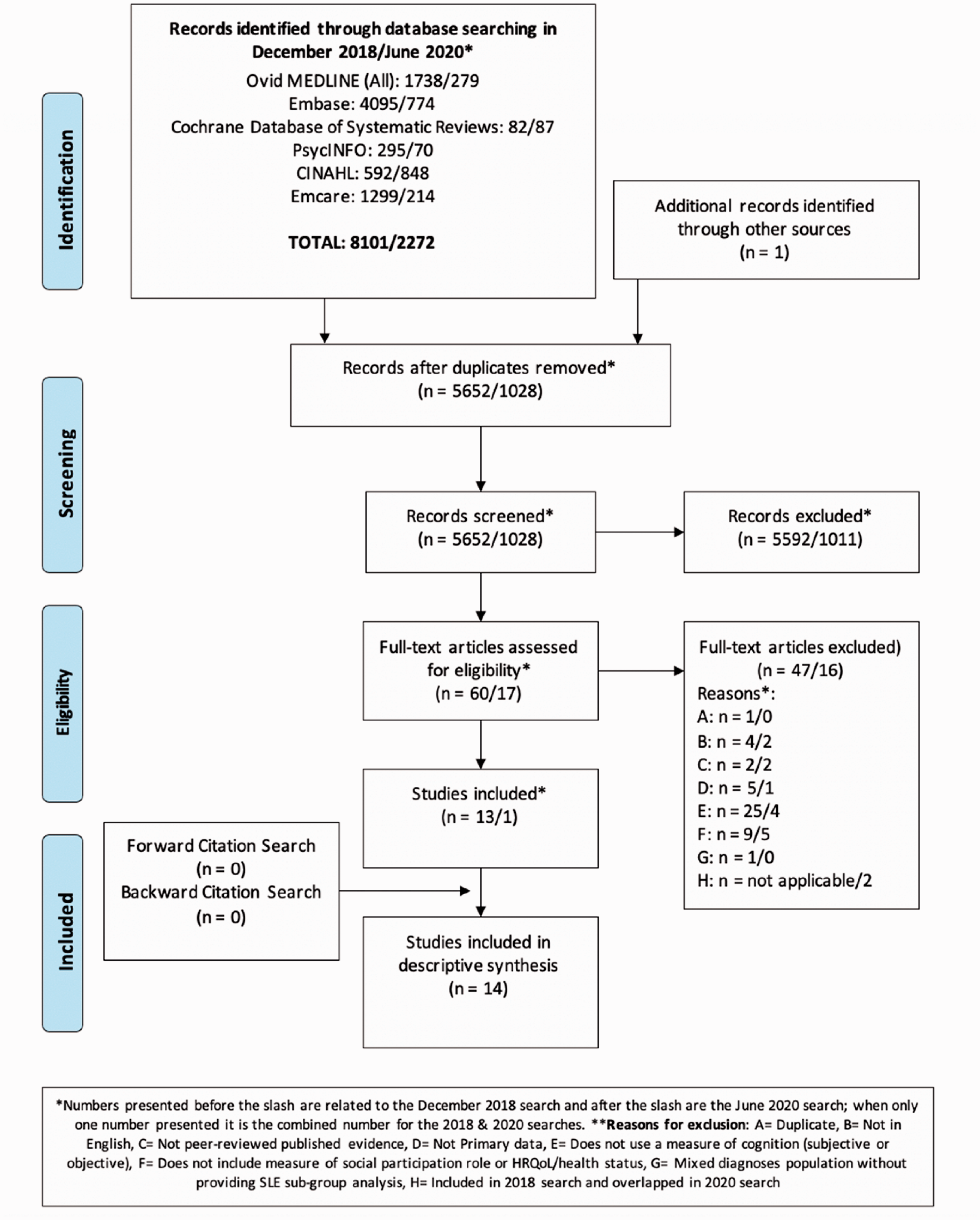
PRISMA table.
Characteristics of included studies grouped by the outcomes of HRQoL and Social Role Participation.
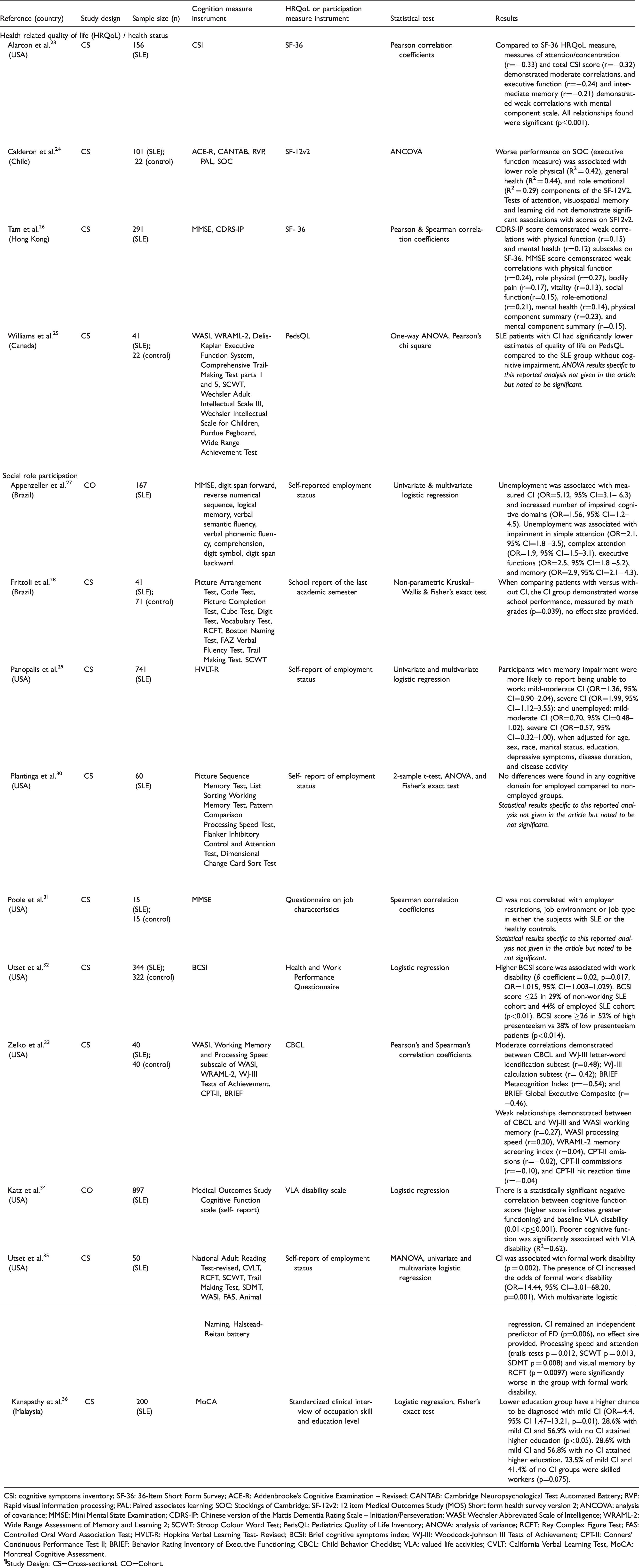
CSI: cognitive symptoms inventory; SF-36: 36-Item Short Form Survey; ACE-R: Addenbrooke’s Cognitive Examination – Revised; CANTAB: Cambridge Neuropsychological Test Automated Battery; RVP: Rapid visual information processing; PAL: Paired associates learning; SOC: Stockings of Cambridge; SF-12v2: 12 item Medical Outcomes Study (MOS) Short form health survey version 2; ANCOVA: analysis of covariance; MMSE: Mini Mental State Examination; CDRS-IP: Chinese version of the Mattis Dementia Rating Scale – Initiation/Perseveration; WASI: Wechsler Abbreviated Scale of Intelligence; WRAML-2: Wide Range Assessment of Memory and Learning 2; SCWT: Stroop Colour Word Test; PedsQL: Pediatrics Quality of Life Inventory; ANOVA: analysis of variance; RCFT: Rey Complex Figure Test; FAS: Controlled Oral Word Association Test; HVLT-R: Hopkins Verbal Learning Test- Revised; BCSI: Brief cognitive symptoms index; WJ-III: Woodcock-Johnson III Tests of Achievement; CPT-II: Conners' Continuous Performance Test II; BRIEF: Behavior Rating Inventory of Executive Functioning; CBCL: Child Behavior Checklist; VLA: valued life activities; CVLT: California Verbal Learning Test, MoCA: Montreal Cognitive Assessment.
¶Study Design: CS=Cross-sectional; CO=Cohort.
Relationship between CI and HRQoL
All four studies investigating a relationship between CI and HRQoL in individuals with SLE identified a negative relationship, such that CI was associated with decreased HRQoL23–26 (Table 1). Three studies used samples of adult SLE patients and measured HRQoL using the Medical Outcome Study Short Form Survey (SF-36) and 12-item Medical Outcomes Study Short Form Health Survey version 2 (SF-12v2). 23 ,24,26 Weak and moderate correlations between scores in CI and the mental component summary (MCS) and its domains were identified23,24,26. Calderon et al. also found a negative correlation between CI and physical domains of the SF-12V2, specifically the domains of role physical and general health. 24 The studies using the SF-36 did not find a similar relationship between CI and the physical component summary (PCS) or physical domains.23,26 When results were stratified by cognitive domains,23,24 Alarcon et al. reported that attention/concentration had a moderate correlation, and executive function and intermediate memory demonstrated weak correlations with the MCS scores of the SF-36. Calderon et al. also reported a negative relationship between executive function and physical components of the SF-2V12, but did not find a relationship between attention, visuospatial memory, or learning and SF-2V12 scores. 24 Williams et al., using the overall Pediatric Quality of Life Inventory (PedsQL) score to explore the relationship between CI and HRQoL in a pediatric and adolescent SLE population, 25 found that PedsQL scores were lower in participants who also had measured CI.
Relationship between CI and social role participation
Ten studies examined social role participation as one of three main categories: employment,27,29–32,35,36 academics28,33,36 and other valued life activities 34 (Table 1).
Employment. Of the seven studies that examined the relationship between CI and employment, four identified a negative relationship 27 ,29,32,35, while three did not report a relationship between CI and employment.30,31,36 Appenzeller et al. reported that the odds of being unemployed correlated with the presence and number of impaired cognitive domains. 27 They further stratified results by cognitive domain and reported that impairments in simple attention, complex attention, executive functions, and memory were more frequently associated with unemployment compared to impairment in other cognitive domains. 27 Panopalis et al. reported greater odds of being unable to work with impaired memory. 29 Utset et al. reported associations between high scores on the patient reported Brief Cognitive Symptoms Inventory (indicative of greater cognitive impairment) with increased unemployment, poor work presenteeism (performance quality when present at work), and increased work disability. 32 Utset et al. reported that CI was an independent predictor of formal work disability. 35 Of the studies that did not find a relationship, they specifically reported the absence of a relationship between CI and employment status, 30 employer restrictions, job environment, job type, 31 and skill of occupation. 36
Academics. An association between CI and academics was identified in all studies investigating this relationship. 28 ,33,36 Specifically, Frittoli et al. found a significant relationship between CI and lower math grades in a pediatric SLE population. Zelko et al. also investigated a pediatric SLE population and found moderate correlations between school competence scores and impairments in executive function, letter-word identification, and calculations. 33 Weak correlations were detected between school competence and omission, commission, reaction time, memory, and processing speed impairments. 33 Kanapathy et al. investigated an adult population and identified that significantly less SLE participants with CI attained higher-level education. 36
Other valued life activities. Katz et al. identified a significant relationship between CI and disability in valued life activities in an adult population, which is a 21-item list of obligatory, committed, and discretionary activities. 34
CI measurement instruments
There were 53 different cognitive assessment instruments used across the 14 included studies. Fifty instruments were objective measures, three were self-report (patient reported) questionnaires, and one was a cognitive screening instrument (Online Appendix C). Whether an objective or self-report measure was used did not influence the relationships observed between CI and HRQoL and social role participation. The number of CI assessment instruments used in each study ranged from one23,29,31,32,34,36 to 11 measures. 28 CI measures varied between studies and no measure was repeated across studies more than three times. The Mini-Mental State Examination (MMSE); 26,27,31 the Wechsler Abbreviated Scale of Intelligence (WASI); 25,33,35 and the Stroop Color and Word Test (SCWT); 25,28,35 were used in three of the 14 included studies.
Twelve overall cognitive domains were investigated across the 53 assessment instruments used (Figure 2). Most commonly measured were memory, attention, executive function, language, and visuo-spatial functioning.
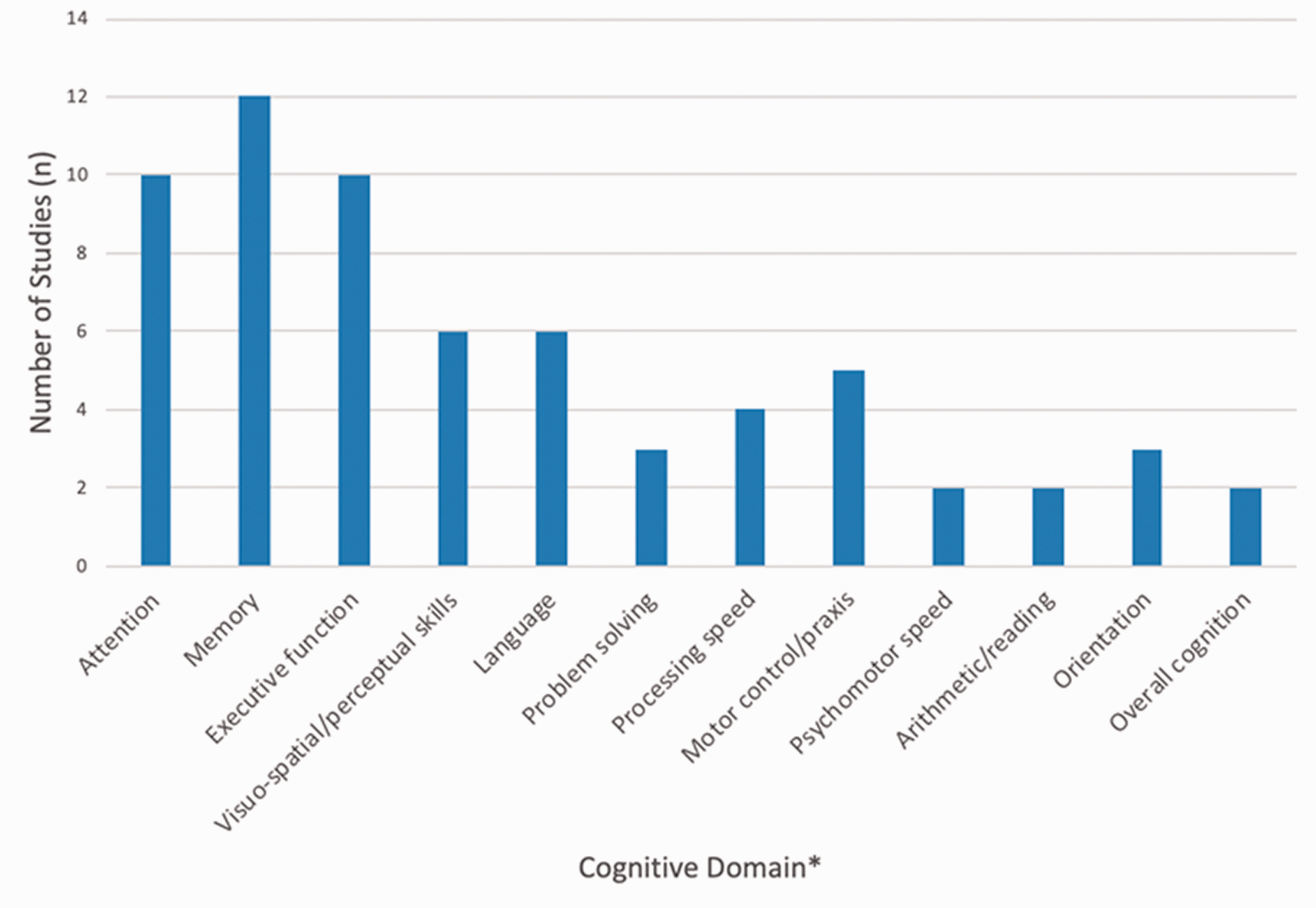
Number of studies measure each cognitive domain. * See Online Appendix C for details about cognitive domains measured by each study.
HRQoL and social role participation measurement instruments
Three different HRQoL measures were used: SF-36, 23 , 26 SF-12v2, 24 and the PedsQL. 25 Across included studies five instruments measured employment from participant self-reports27,29,30,35,36 and two used standardized questionnaires of objective employment experiences.31,32 Whether a standardized questionnaire or self-report measure was used did not appear to influence the results. Academics were measured using school reports, 28 the School Competence scale of the Child Behaviour Checklist (CBCL), 33 and a standardized clinical interview. 36 Valued life activities were measured using the Valued Life Activities scale. 34
Socio-demographic and disease characteristics
In the 14 articles included in this review, 73% to 100% of participants were female. The age of the pooled sample ranged from 9-67 years. Three out of the 14 articles examined a pediatric and adolescent population with age ranging from 9-21.8 years,25,28,33 while the remaining studies investigated an adult SLE population with age ranging from 18-67 years. Thirteen studies reported education level, and the study that did not report it, investigated a pediatric population. 25 Highest level of education achieved was heterogeneous within and across studies, ranging from four years of formal education to obtaining a university degree. The studies investigating a pediatric population that did report on education provided proportions of sample in elementary, middle and high school. Ten studies reported racial background. Two studies had predominantly Caucasian participants,29,34 five were predominantly African American,23,30,32,33,35 and one study had predominantly Hispanic participants. 25 Disease duration was reported by all studies and the average duration across studies ranged from 1.45-17.7 years. The SLE Disease Activity Index (SLEDAI) 37 was reported in seven studies, five of which reported a mean or median SLEDAI >4 for the included sample.24,27,28,31,33 The Systemic Lupus International Collaborating Clinics American College of Rheumatology (SLICC/ACR) Damage Index 38 was reported in eight studies, with a mean ranging from 0.21-2.32. Study demographics and disease characteristics are provided in Online Appendix D.
Quality appraisal of the included studies
Using the Mixed Methods Appraisal Tool,19,20 all fourteen studies indicated a positive response to the screening questions (i.e. clarity of research question and data addressing research question). To compare quality judgements between studies, an overall score was computed, such that the maximum score was 100% which required yes to be answered for all five MMAT questions used. Overall the quality of the included studies per the MMAT was high, with thirteen of the studies given an overall score of 100% and one study given an overall score of 80%. 31 In the latter study, participant recruitment was not reported and therefore the question “are the participants representative of the target population?” was answered as “can’t tell”, leading to a lower score.
Discussion
The objective of this study was to systematically synthesize the literature regarding the associations between CI and (a) HRQoL and (b) social role participation in individuals with SLE. Only fourteen articles fulfilled the inclusion criteria for this review indicating there is limited research exploring these relationships in individuals with SLE. Studies used a variety of CI, HRQoL, and social role participation measures, therefore meta-analysis across the included articles was not feasible. The descriptive analysis across the included studies supports that there is a negative relationship between CI and HRQoL and social role participation in SLE patients, in adults and children. This analysis highlighted multiple areas of study insight and avenues to continue and improve this area of SLE care and research.
First, the common cognitive domains assessed in this review were memory, attention, and executive function. Other cognitive domains such as language, visuospatial function, and processing speed were also assessed, but less often. The cognitive domains measured align with those described in the literature as being affected by SLE.2,39,40 In this review medium and weak relationships between impaired executive function and HRQoL and social role participation were found.24,33 These findings are consistent with research in other populations; for example, impairment in executive function has been associated with negative employment outcomes in populations with acquired brain injuries and multiple sclerosis.41,42 Findings from this review suggest executive function is an important cognitive domain that should be measured and addressed, because individuals with SLE that do experience impaired executive function may be at risk of greater impacts on HRQoL and social role participation.
Further, when examining social role participation, two major life roles were identified: employment for adults and academic performance for children with SLE. Four included studies reported a negative relationship between CI and employment status.27,29,32,35 Employment provides a sense of self-worth, socialization opportunities, financial resources, and social status. 12 Moreover, not being able to engage in work can further limit psychosocial functioning and HRQoL. Recent literature has suggested disease invisibility, fatigue, and fluctuation to be the key barriers in maintaining employment for individuals with SLE. 12 The findings of this review provide important insight into CI as a contributing factor to poor employment outcomes for individuals with SLE. The identification of CI as an additional barrier to employment suggests the need for interventions to address employment disability for those with SLE who are experiencing CI.
Academic participation and performance are major life roles for children, adolescents and young adults. Although the research in this area is limited, the findings in this review suggest a moderate strength relationship between CI and academics. Children with SLE and their parents have reported that SLE has a significant impact on school performance and attendance. 15 Further, these school-related issues have a significant impact on HRQoL in children with SLE. 15 Therefore, identifying and addressing CI as a contributing factor in the relationship between SLE and impaired academics is critical.
While very salient life roles, employment and academics are not the only social participation roles that may be affected for people with SLE. The World Health Organization’s International Classification of Functioning, Disability and Health outlines many other social participation roles, including relationships, recreation, and leisure. 11 Many of these areas are conceivably influenced by CI and require further research. Indeed, the third area of social role participation identified in this review by one included study, valued life activities, addressed many of these additional social participation roles. 34 More studies investigating this and an expansion of the examination to more varied life roles would enrich the understanding of the full impact of CI for people living with SLE.
It is important to note that the relationship of CI to HRQoL and social role participation is complex. This is likely why strong correlations and consistency across all included studies was not observed. There are many intersecting factors contributing to the relationship of CI to HRQoL/social role participation. For example, adequate social supports and contextual/environmental demands could influence the association of CI to HRQoL and social participation roles; as has been found in other diagnostic populations.42,43 Further, only four of the 14 included studies reported glucocorticoid dose of the SLE sample.24,26,27,33 However, glucocorticoids are a critical component of standard of care for SLE, and cumulative dose has been associated with an increased risk ratio of cognitive impairment. 44 Therefore, glucocorticoids are a potential variable mediating the relationships observed in the literature. As such, greater attention to glucocorticoids in future research is necessary. Socioeconomic status, disease activity and disease damage may also influence the relationship of CI to HRQoL and social role participation. However, data is not reported consistently across studies and it is therefore unclear what role demographics and disease characteristics play in these relationships. Future studies should report this information to allow for a point of analysis.
This complex relationship may be related to inconsistent findings across all studies; two included studies did not find any significant relationship between CI and employment outcomes. However, methodology of these studies may be contributing to the inconsistent findings. In one study the statistical data supporting the results were not available making it unclear how the results were determined. 30 The other study had a sample size of 15 subjects with SLE, the smallest sample size of all the articles included in this review. 31
A significant relationship between CI to the outcomes of HRQoL and social role participation has been described in this review. Yet, there is a lack of CI intervention literature for SLE patients. Only one study has investigated non-pharmacological interventions for CI in SLE patients.45,46 This non-randomized uncontrolled pilot group study of 17 SLE patients, published in 2005, examined an intervention program that included both individual and group sessions and addressed memory. 47 The results indicated positive outcomes related to memory performance. However, the impact of the intervention on HRQoL, social role participation, or other commonly affected cognitive domains was not investigated. Consequently, there are limited evidence-based interventions to target HRQoL or social role participation issues related to CI for SLE patients. Research in the rehabilitation of various cognitive domains will be beneficial to improve care for SLE patients experiencing CI.
Although not an a priori objective, when country of study was examined, it was noted that the majority of the included studies were conducted in the USA, which may indicate bias in the literature. However, studies from five other countries (Canada, Brazil, Chile, Hong Kong, Malaysia) did support the findings from the USA-based studies. SLE, HRQoL, and social roles may vary between countries, 48 implicating the importance of continuing this field of research in other countries or populations.
As with all reviews, this review has limitations. It is possible that applicable articles were missed, which may occur if relevant search terms were only in the full text. Nonetheless, five mitigation strategies to identify all relevant literature were used: (1) three different search methods; (2) an experienced librarian completed all database searches; (3) search of six multi-disciplinary databases; (4) a broad search map; and (5) use of an a priori registered search protocol. Another limitation was that although the database searches were not limited by language, the screening/selection process included only articles with full-text English options available, secondary to the language abilities of the reviewers. Six non-English articles were excluded from this review during screening/selection. This selection bias may influence the generalizability of the findings that were captured, since non-English knowledge was not included. Finally, this review was limited to published, peer-reviewed articles. Articles that may not have found a relationship between CI and HRQoL or social role participation may be less likely to have been published due to publication bias. 49
In addition to areas of future research already noted, the small number of articles included in this review suggests more research should be done to strengthen the knowledge base on CI and HRQoL and social role participation. Additionally, uniformity in the measures and statistics used in future research would allow for pooling and direct comparisons of data. As such, standardization of methods and measures in research investigating CI and its impact on HRQoL and social role participation is needed in the future. Furthermore, this review found limited literature regarding children with SLE. Considering that SLE has been suggested to be more severe in children than in the adult population, 50 more research in the juvenile population is required.
This review and synthesis found that CI is negatively related to HRQoL and social role participation outcomes in SLE patients. Healthcare professionals and researchers need to be aware of this relationship so that it can be addressed in clinical practice and future research. Considering the importance of HRQoL and social role participation on the well-being and everyday lives of individuals living with SLE, it is crucial to address CI in routine and holistic SLE care.
Supplemental Material
sj-pdf-1-lup-10.1177_09612033211031008 - Supplemental material for Cognitive impairment in systemic lupus erythematosus is negatively related to social role participation and quality of life: A systematic review
Supplemental material, sj-pdf-1-lup-10.1177_09612033211031008 for Cognitive impairment in systemic lupus erythematosus is negatively related to social role participation and quality of life: A systematic review by Sierra Mendelsohn, Lina Khoja, Sofia Alfred, Jennifer He, Melanie Anderson, Denise DuBois, Zahi Touma and Lisa Engel in Lupus
Supplemental Material
sj-pdf-2-lup-10.1177_09612033211031008 - Supplemental material for Cognitive impairment in systemic lupus erythematosus is negatively related to social role participation and quality of life: A systematic review
Supplemental material, sj-pdf-2-lup-10.1177_09612033211031008 for Cognitive impairment in systemic lupus erythematosus is negatively related to social role participation and quality of life: A systematic review by Sierra Mendelsohn, Lina Khoja, Sofia Alfred, Jennifer He, Melanie Anderson, Denise DuBois, Zahi Touma and Lisa Engel in Lupus
Supplemental Material
sj-pdf-3-lup-10.1177_09612033211031008 - Supplemental material for Cognitive impairment in systemic lupus erythematosus is negatively related to social role participation and quality of life: A systematic review
Supplemental material, sj-pdf-3-lup-10.1177_09612033211031008 for Cognitive impairment in systemic lupus erythematosus is negatively related to social role participation and quality of life: A systematic review by Sierra Mendelsohn, Lina Khoja, Sofia Alfred, Jennifer He, Melanie Anderson, Denise DuBois, Zahi Touma and Lisa Engel in Lupus
Supplemental Material
sj-pdf-4-lup-10.1177_09612033211031008 - Supplemental material for Cognitive impairment in systemic lupus erythematosus is negatively related to social role participation and quality of life: A systematic review
Supplemental material, sj-pdf-4-lup-10.1177_09612033211031008 for Cognitive impairment in systemic lupus erythematosus is negatively related to social role participation and quality of life: A systematic review by Sierra Mendelsohn, Lina Khoja, Sofia Alfred, Jennifer He, Melanie Anderson, Denise DuBois, Zahi Touma and Lisa Engel in Lupus
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Touma’s research is supported by the CRA (CIORA)-Arthritis Society Clinician Investigator Award and the Department of Medicine University of Toronto, the Canadian Institutes of Health Research, the Physicians’ Services Incorporated Foundation, the Rocca Family, and the Kaiser Family. Dr. Engel’s work on this project was supported by a post-doctoral research fellowship from the Arthritis Society.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.