
Abstract
Background
Although the survival of patients with systemic lupus erythematosus (SLE) has improved, irreversible organ damage remains a critical concern. We aimed to characterize damage accrual and its clinical associations and causes of death in Swedish patients.
Methods
Accumulation of damage was evaluated in 543 consecutively recruited and well-characterized cases during 1998−2017. The Systemic Lupus International Collaborating Clinics (SLICC)/American College of Rheumatology damage index (SDI) was used to estimate damage.
Results
Organ damage (SDI ≥ 1) was observed in 59%, and extensive damage (SDI ≥ 3) in 25% of cases. SDI ≥ 1 was significantly associated with higher age at onset, SLE duration, the number of fulfilled SLICC criteria, neurologic disorder, antiphospholipid antibody syndrome (APS), hypertension, hyperlipidemia, depression and secondary Sjögren's syndrome (SS). In addition, SDI ≥ 3 was associated with serositis, renal and haematological disorders and interstitial lung disease. A multiple regression model identified not only well-known risk factors like APS, antihypertensives and corticosteroids, but pericarditis, haemolytic anaemia, lymphopenia and myositis as being linked to SDI. Malignancy, infection and cardiovascular disease were the leading causes of death.
Conclusions
After a mean SLE duration of 17 years, the majority of today's Swedish SLE patients have accrued damage. We confirm previous observations and report some novel findings regarding disease phenotypes and damage accrual.
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease with diverse clinical manifestations and an unpredictable disease course, often including periods of increased disease activity followed by remission. Long-standing inflammation, drug-related side effects and comorbidities may eventually cause permanent organ damage in many patients, and such acquired damage is tightly linked to mortality.1–3
Since the 1950s, the 5-year survival rate in SLE has increased significantly from approximately 50% to almost 95% in the 2000s.4,5 The improved survival rate has been linked to increased awareness, including identification of cases with milder disease, earlier diagnosis and more efficient clinical care. 6 Yet age-related mortality remains significantly higher among patients with SLE compared to the general population, mainly due to disease activity, infections, thromboembolic events and cardio- or cerebrovascular disease.7–9 Despite progress in the understanding of SLE pathogenesis and development of more targeted therapies, data suggest that survival rates have plateaued since the mid-1990s.6,10 In addition, differences in accrual of damage and survival rates have been identified between high- and low-income countries, which may reflect diverse access to healthcare, the socio-economy and ethnicity.6, 11
The Systemic Lupus International Collaborating Clinics (SLICC) and American College of Rheumatology (ACR) damage index (SDI) is the only validated tool to quantify accumulated irreversible organ damage. 12 Attribution of organ damage to SLE is not mandatory. The SDI comprises 12 organ systems; damage that has occurred since the onset of SLE is recorded when it has persisted for 6 months. 12 Absence of an SDI increase is a measure of well-controlled or mild disease ,3,13 whereas increasing SDI scores are associated with increased risk of further damage as well as a higher age-related risk of mortality.1,3,13,14 Furthermore, damage accrual has been associated with patient-reported outcome measures, such as quality of life and activity limitations. 15
Several studies have identified risk factors for the development, or progression, of organ damage using the SDI but recent reports on the Swedish SLE population are lacking. The age at onset of SLE plays an important role for expression of disease manifestations and outcomes, including mortality risks. 16 Late-onset SLE can be milder, but may nevertheless accumulate irreversible damage over time. 16 Other factors associated with organ damage include disease duration, male gender, recurrent flares, hypertension, antiphospholipid antibody syndrome (APS) and the presence of antiphospholipid antibodies (aPL).17,18 Regarding treatments, use of cyclophosphamide and high accumulated doses of corticosteroids have been associated with higher SDI scores, whereas antimalarials seem to be protective.1,17,19,20 Given the heterogeneous clinical and immunological nature of SLE, in-depth knowledge of specific disease variables associated with accrual of damage and severe outcomes is indeed essential.
We primarily aimed to characterize accumulated organ damage and describe causes of death in two Swedish cohorts of well-characterized SLE cases. Secondly, we examined factors associated with damage accrual according to the SDI, including demographics, disease manifestations, medical therapies and autoantibody specificities.
Materials and methods
Cohorts
Swedish healthcare is public, tax-funded and offers universal access. This study was carried out in two separate geographical areas of Sweden. The University Hospital in Linköping serves the Östergötland region (n = 457,000) and Uppsala Akademiska Hospital serves the Uppsala region (n = 369,000) with rheumatological care. Five hundred and forty-three consecutively recruited and longitudinally followed SLE cases diagnosed at the rheumatology units in Linköping (n = 296) and Uppsala (n = 247) were included. The Linköping cohort was launched in 2008 and has previously been described in detail. 21 It includes more than 95% of the expected SLE cases in Linköping and ≥98% of all known SLE cases in the region. 22 The Uppsala cohort was launched in 1998 and has an estimated coverage of 84% in the area. 23 All patients met the 1982 ACR (ACR-82) and/or 2012 SLICC classification criteria (SLICC-12),24,25 and were included as prevalent or incident cases until 31 December 2017.
Variables
Background variables such as age, gender, ethnicity, disease duration and age at diagnosis were available for all cases from SLE diagnosis to 31 December 2017, or death. The numbers of fulfilled ACR-82 and SLICC-12 criteria, as well as data on smoking habits (ever/never) were recorded at the data extraction time point in each cohort. Clinical data on APS, secondary Sjögren's syndrome (SS), lymphoma and comorbidities such as diabetes mellitus, interstitial lung disease, hypertension, hyperlipidemia, depression, myositis and hypothyroidism were collected through review of medical records (definitions in Supplementary Table 1). Cause of death was recorded according to death certificates.
The use of antirheumatic drugs, including antimalarials and other disease-modifying antirheumatic drugs, glucocorticoids, biologics (rituximab and belimumab), antihypertensives, statins, levothyroxine and antidepressants were registered. Damage accrual was evaluated at the end of 2017 using the SDI, including detailed information on organ damage in each separate domain. 12 In accordance with Gonçalves et al., 26 comparisons of cases without damage (SDI = 0) and with damage (SDI ≥ 1), as well as with extensive damage (SDI ≥ 3) were performed. In addition, we evaluated time to first and second damage in relation to each variable.
Statistical analysis
Comparisons between groups, for example, cases without damage (SDI = 0) vs. cases with damage (SDI ≥ 1) or cases with extensive damage (SDI ≥ 3), were performed for frequency distributions and measures on interval-/ratio scales. Comparisons of frequency distributions were performed using chi-square tests of homogeneity (or Fisher's exact test when assumptions were not fulfilled) with the phi coefficient as a measure of effect size (ES). The comparisons of measures on interval-/ratio scales were performed using independent t-tests or Mann–Whitney U tests (when assumptions were not fulfilled) with r as a measure of ES. Comparisons between groups with different SDI scores and disease duration were carried out with the Kruskal–Wallis test.
Characteristics of the 543 systemic lupus erythematosus cases
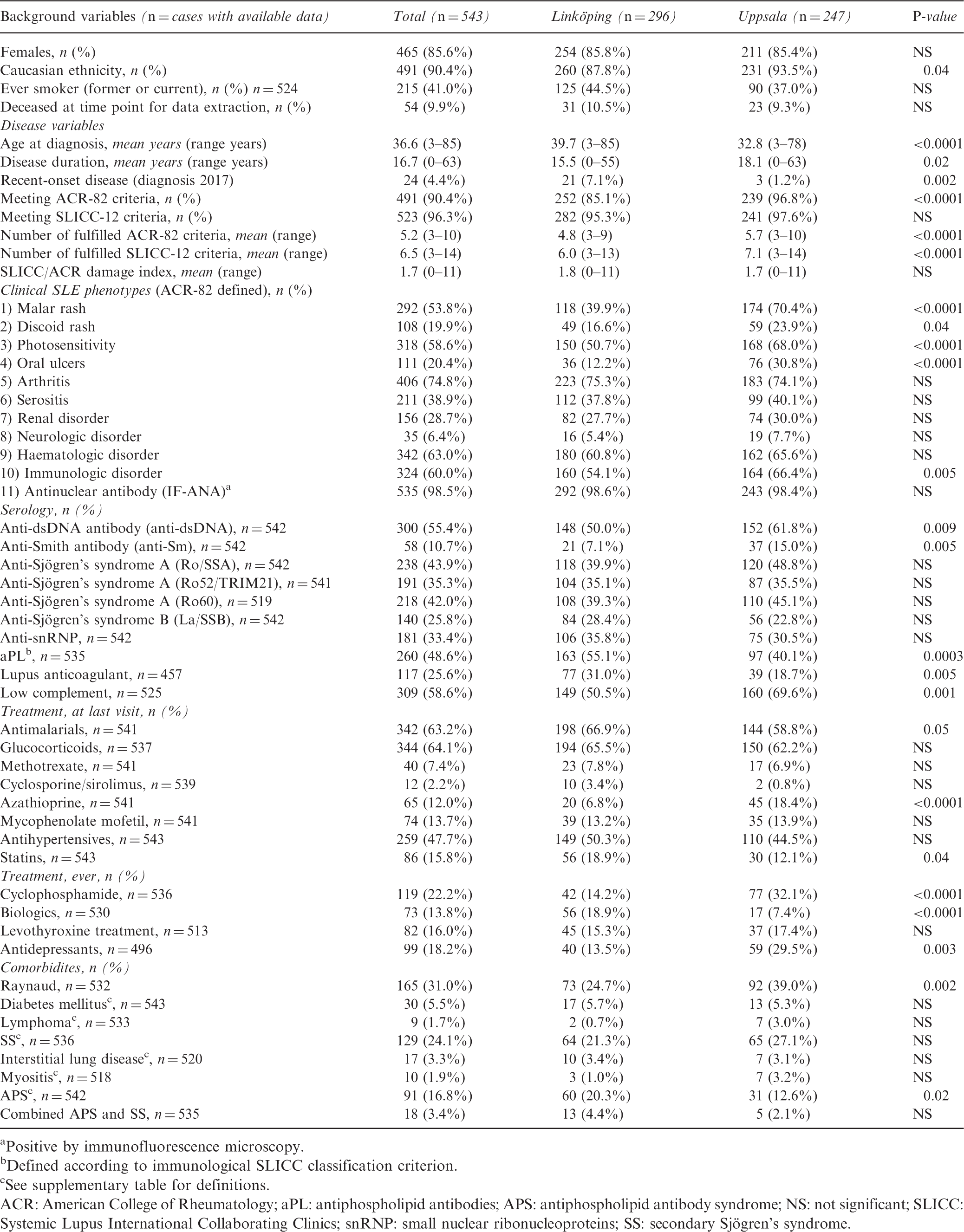
Positive by immunofluorescence microscopy.
Defined according to immunological SLICC classification criterion.
See supplementary table for definitions.
ACR: American College of Rheumatology; aPL: antiphospholipid antibodies; APS: antiphospholipid antibody syndrome; NS: not significant; SLICC: Systemic Lupus International Collaborating Clinics; snRNP: small nuclear ribonucleoproteins; SS: secondary Sjögren's syndrome.
P-values < 0.05 were considered significant, but since this is an exploratory study, significances should be interpreted in association with the reader's knowledge of what hypotheses can be posed (it would not be possible to list every hypothesis for each association examined in this study). For informative purposes, the exact p-values are provided.
Ethics
Oral and/or written informed consent was obtained from all participants. The study protocols were approved by the regional ethics review boards in Linköping (M75-08/2008) and Uppsala (2016/155 EPN Uppsala 00-227).
Results
As postulated in Table 1, mean age at diagnosis was 37 years, mean disease duration at data extraction was 17 years and 86% were women. More than 90% of patients were of Caucasian ethnicity whereas the majority of the remainder of patients were Asian, Hispanic or Middle Eastern in origin. The SLE duration of non-Caucasian patients was significantly shorter compared with Caucasians (11 vs. 17 years, p = 0.0006). The majority of cases had an established disease at data extraction (31 December 2017) and only 4% had recent-onset SLE with less than 1 year's disease duration. The most common ACR-82 criterion was arthritis (75%), followed by haematologic disorder (63%), photosensitivity (59%) and malar rash (54%). Renal involvement (ACR-82) was observed in 29% and neurologic disorder (ACR-82) in 6% of cases. A positive antinuclear antibody (ANA) test was detected in 99% and aPL (SLICC-12) in 49% of patients at least once during their disease course.
When comparing the cohorts of Linköping and Uppsala, gender, percentage of fulfilled SLICC-12 criteria and the mean SDI scores as well as the majority of clinical manifestations, including renal and neurological involvement, were similar (Table 1). The Uppsala cohort comprised more cases with malar rash, photosensitivity, oral ulcers, anti-dsDNA and anti-Sm. The Linköping cohort included older patients with shorter disease duration and had a lower percentage of cases meeting ACR-82, whereas the presence of aPL and APS was more frequent compared to Uppsala (Table 1). However, as the differences between the cohorts were considered negligible further statistical analyses were performed on merged data.
In total, the study population consisted of 543 patients, of whom the majority had accrued damage from SLE onset and onwards (Figure 1a). At the time point of data extraction, 59% (n = 318) had accrued ‘any damage’ (SDI>0; Figure 1b). Among the 318 cases with any damage, extensive damage with an SDI score of ≥3 (n = 137, 25%, mean disease duration 26 years) was most common, followed by an SDI score of 1 (n = 119, 22%, mean disease duration 14 years) and an SDI score of 2 (n = 62, 11%, mean disease duration 19 years, p < 0.0001). Subsequently, involvement of one organ domain (n = 138, 25%) was most common, but some individuals were affected by severe impairment involving several domains (Figure 1c).
Figure 1a indicates the accumulation of organ damage in the study population from SLE onset and onwards. Figure 1b shows the distribution of points according to the Systemic Lupus International Collaborating Clinics/American College of Rheumatology damage index (SDI), whereas 1c illustrates number of involved SDI domains. Figure 1d demonstrates the frequencies (%) of involved separate organ domains in all 543 cases. Figure 1e presents the median time to the first damage in relation to organ domain involvement.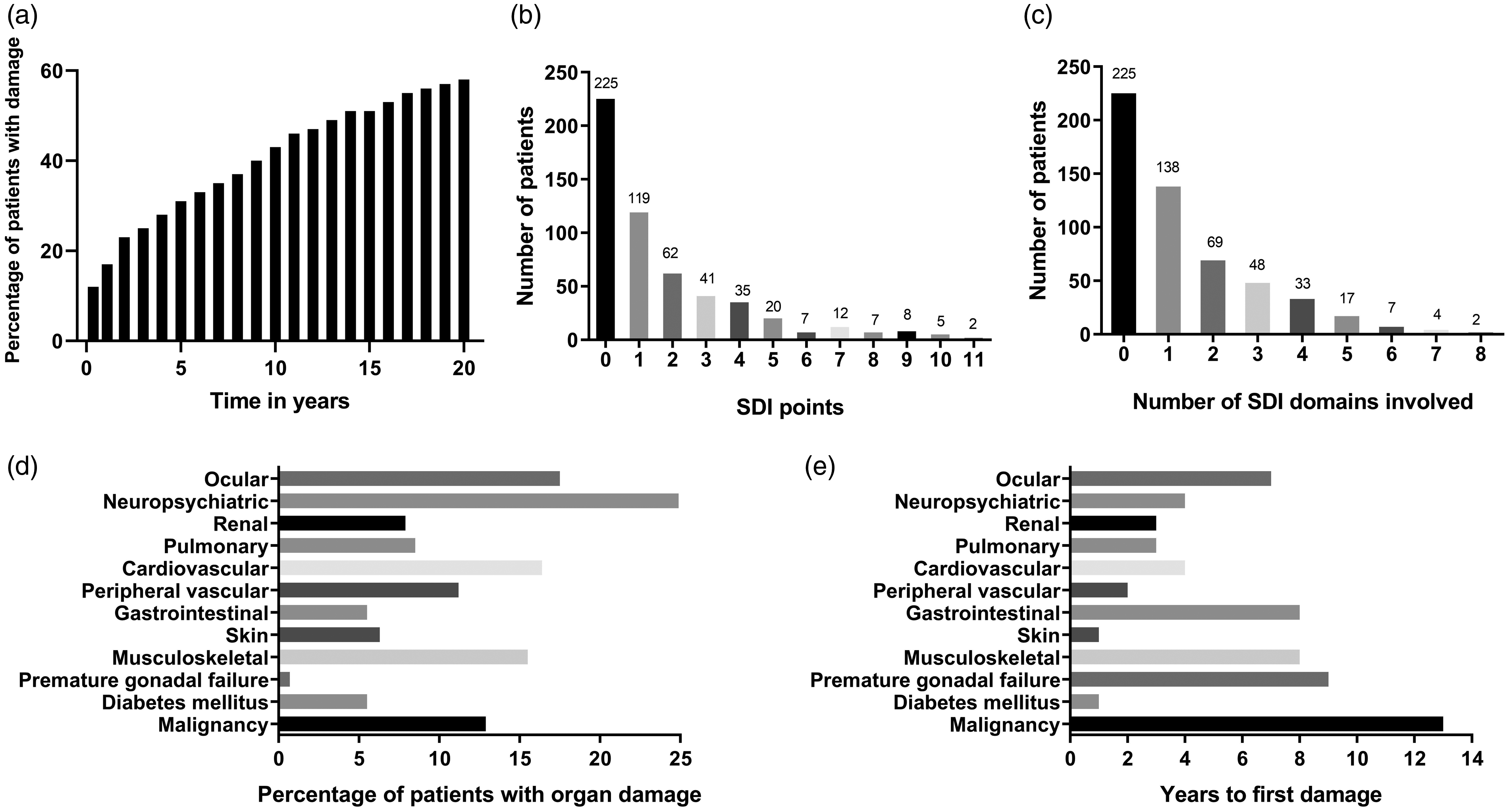
The distribution of damage in each organ domain is demonstrated in Figure 1d. Of patients with SDI ≥ 1, involvement of the neuropsychiatric (25%), ocular (18%), cardiovascular (16%), musculoskeletal (16%) and malignancy (13%) domains were most prevalent (Figure 1d). A binary comparison of damage vs. no damage in these five most commonly affected organ domains did not identify further variables of predictive importance.
Figure 1e illustrates time to first damage for each separate domain. The skin domain (median time 9 months) and diabetes mellitus (12 months) showed shortest time from SLE onset to first damage, followed by peripheral vascular (2 years), renal and pulmonary domains (both 3 years). The malignancy domain had the longest time to first damage (median time 13 years). Time to first damage was shorter for men compared with women (median 2 vs. 6 years, p < 0.001) and for lupus anticoagulant (LA) positive patients compared with LA negatives (median 3 vs. 6 years, p = 0.005). APS was borderline significant (median 4 vs. 5 years, p = 0.07) and cases with combined APS/SS did not significantly differ in time to first damage compared with the others (p = 0.75). Conversely, time to first damage was longer for anti-La/SSB antibody positive patients (median 8 years vs. 4 years, p = 0.006), patients with malar rash (7 years vs. 3 years, p < 0.001) and patients treated with levothyroxine (10 vs. 4 years, p = 0.002) or antidepressants (8 vs. 4 years, p = 0.03). Second damage was acquired earlier in cases who were deceased at the time of data extraction (9 vs. 14 years, p = 0.03) and for those who had been treated with biologics (8 vs. 14 years, p = 0.02). A positive LA test almost met statistical significance regarding earlier second damage (10 vs. 14 years, p = 0.06). Patients with malar rash showed longer disease duration until second damage (15 years vs. 10 years, p = 0.009).
Demographic, clinical characteristics and medication in SLE cases with and without organ damage
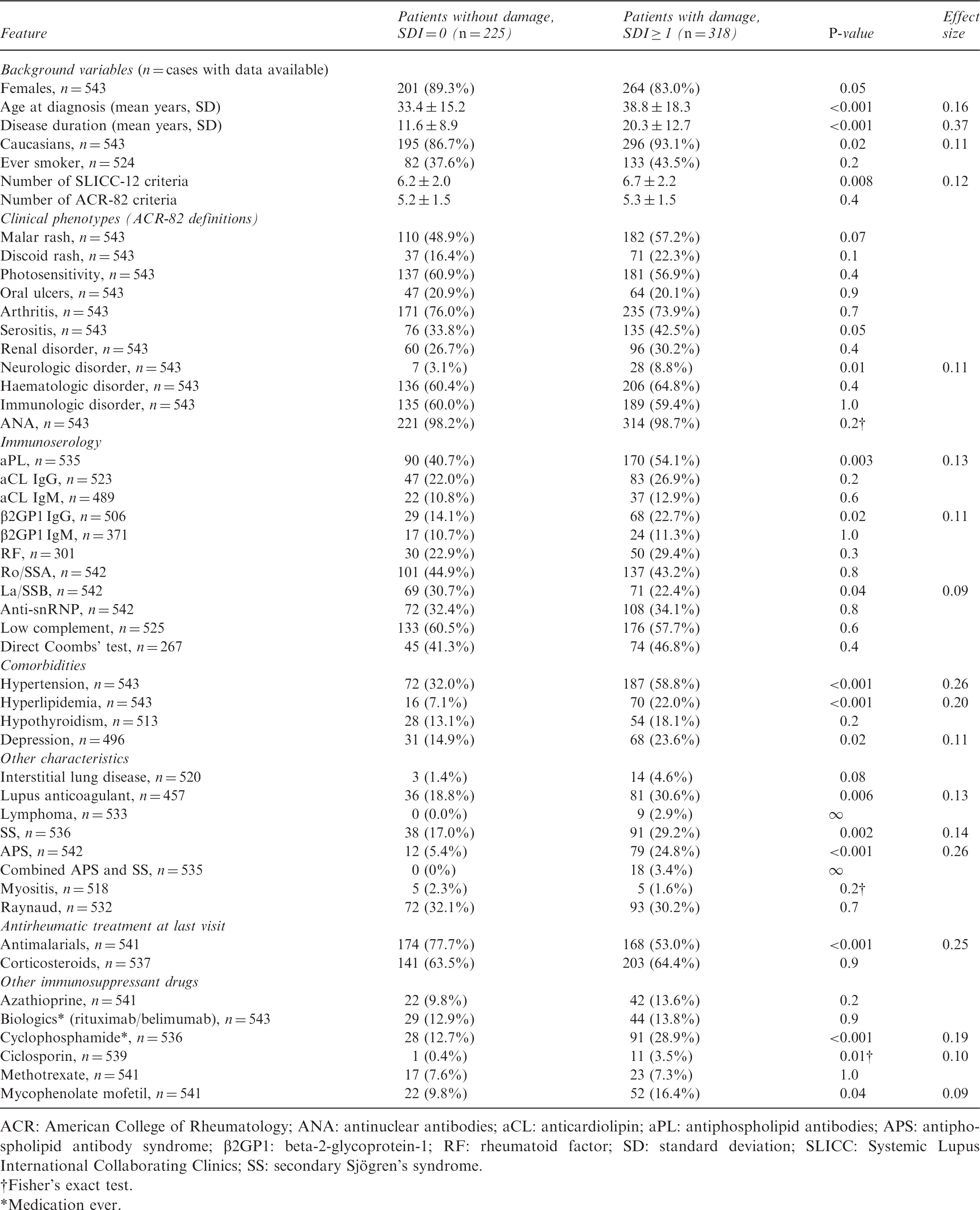
ACR: American College of Rheumatology; ANA: antinuclear antibodies; aCL: anticardiolipin; aPL: antiphospholipid antibodies; APS: antiphospholipid antibody syndrome; β2GP1: beta-2-glycoprotein-1; RF: rheumatoid factor; SD: standard deviation; SLICC: Systemic Lupus International Collaborating Clinics; SS: secondary Sjögren's syndrome.
Fisher's exact test.
Medication ever.
Demographic, clinical characteristics and medication in cases without and with severe damage
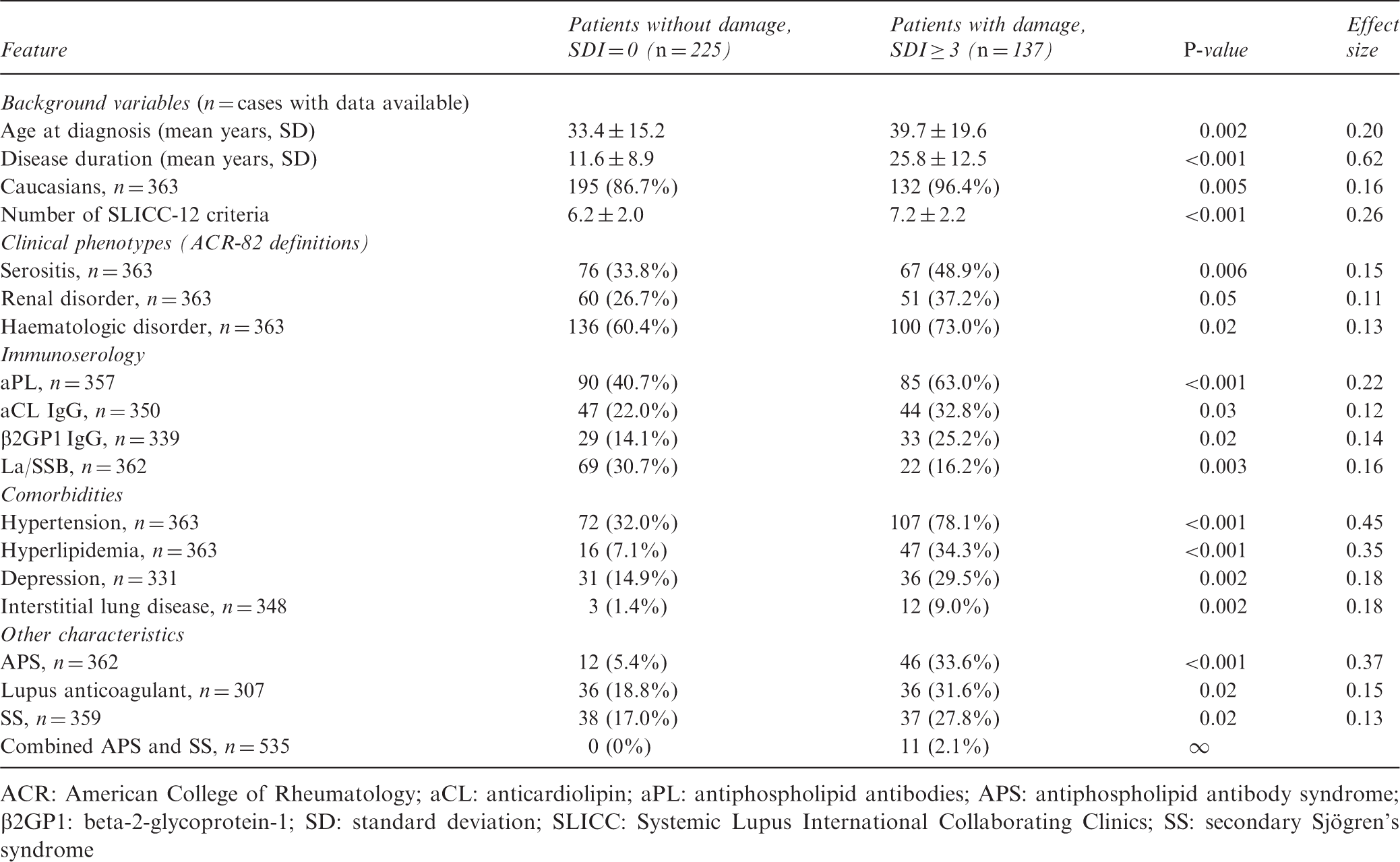
ACR: American College of Rheumatology; aCL: anticardiolipin; aPL: antiphospholipid antibodies; APS: antiphospholipid antibody syndrome; β2GP1: beta-2-glycoprotein-1; SD: standard deviation; SLICC: Systemic Lupus International Collaborating Clinics; SS: secondary Sjögren's syndrome
Poisson regression models to establish empirical relations with organ damage accrual (global SDI score)
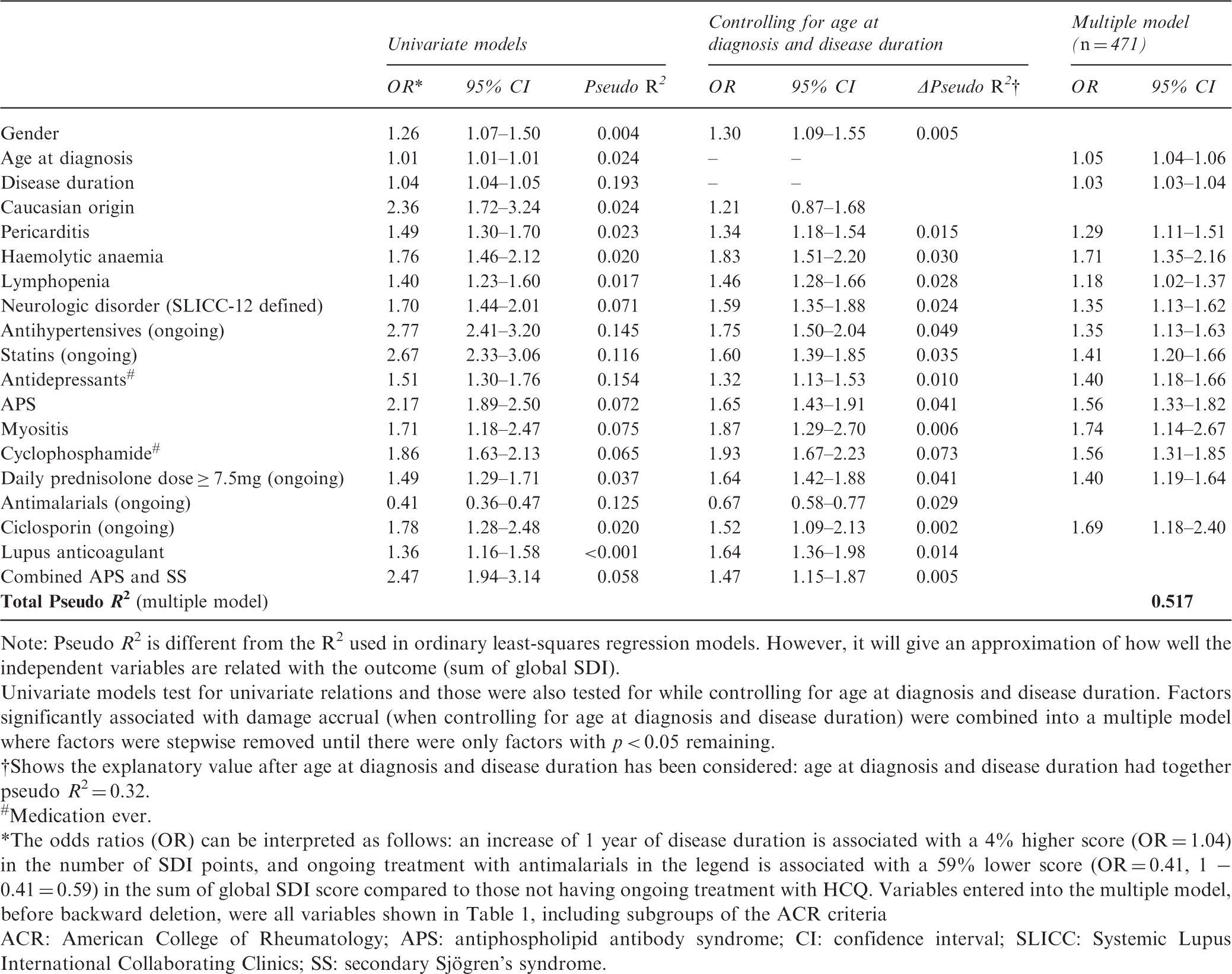
Note: Pseudo R2 is different from the R2 used in ordinary least-squares regression models. However, it will give an approximation of how well the independent variables are related with the outcome (sum of global SDI).
Univariate models test for univariate relations and those were also tested for while controlling for age at diagnosis and disease duration. Factors significantly associated with damage accrual (when controlling for age at diagnosis and disease duration) were combined into a multiple model where factors were stepwise removed until there were only factors with p < 0.05 remaining.
Shows the explanatory value after age at diagnosis and disease duration has been considered: age at diagnosis and disease duration had together pseudo R2 = 0.32.
Medication ever.
The odds ratios (OR) can be interpreted as follows: an increase of 1 year of disease duration is associated with a 4% higher score (OR = 1.04) in the number of SDI points, and ongoing treatment with antimalarials in the legend is associated with a 59% lower score (OR = 0.41, 1 − 0.41 = 0.59) in the sum of global SDI score compared to those not having ongoing treatment with HCQ. Variables entered into the multiple model, before backward deletion, were all variables shown in Table 1, including subgroups of the ACR criteria
ACR: American College of Rheumatology; APS: antiphospholipid antibody syndrome; CI: confidence interval; SLICC: Systemic Lupus International Collaborating Clinics; SS: secondary Sjögren's syndrome.
At the end of follow-up, 54 patients (10%) were deceased, 7 of which were included in our cohorts as incident cases. Ten of the 54 cases died before the age of 60, including five from malignancies. The mean age at death among the 54 cases was 70 years (range 27–96) and the mean SLE duration was 20 years (range 2–63). The causes of death are presented in Figure 2. Malignancy (n = 18; whereof five were haematological malignancies and five lung cancer) was the leading cause of death, followed by infections and cardiovascular disease. The deceased cases had a significantly higher SDI score compared with patients alive at follow-up (SDI 5.3 vs. 1.3, p < 0.0001).
Cause of death according to death certificates among the 54 deceased cases at the time point of data extraction (31 December 2017). CVI: cerebrovascular insult.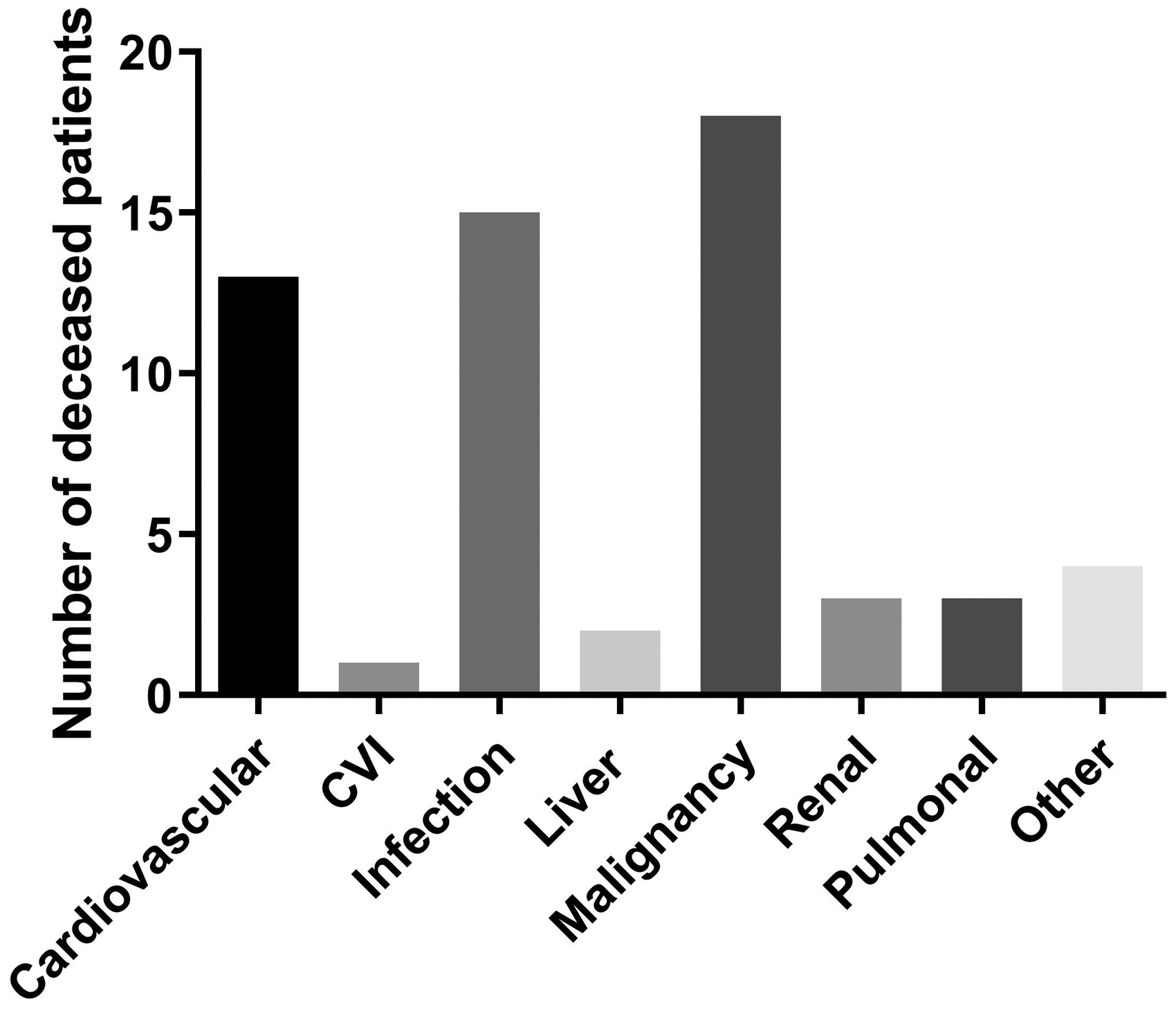
Discussion
In this Swedish SLE population with a mean disease duration of 17 years, more than half of the cases (59%) had acquired organ damage involving at least one organ domain. Studies of European populations with comparable follow-up and a similar distribution of ethnicity have shown a prevalence of organ damage between 36 and 69%.14,18,26,28 In the SLICC cohort, including patients with approximately 50% Caucasian ethnicity, 51% were already presenting with organ damage after 6 years' disease duration. 1 The corresponding percentage in the present study in the sixth year was 38%, and this is essentially in line with older observations from Sweden (Lund University), Spain and the United Kingdom.9,13,14
The most frequently affected organ domains among the Swedish SLE cases herein were the neuropsychiatric, ocular, cardiovascular, musculoskeletal and malignancy domains. Similar results were found in a Portuguese study 26 with exceptions including higher frequencies of pulmonary, renal and musculoskeletal damage, whereas malignancies and cardiovascular damage were slightly more common in our study. Divergent findings could reflect genetic variation as well as differences in coverage of the study population, a shorter follow-up time, and the cross-sectional design of the Portuguese study.
As previously shown by others, we demonstrate that age, disease duration and a higher number of fulfilled ACR-82 classification criteria are associated with global damage.9,18,19,26 As the SDI does not demand attribution to SLE, factors like comorbidities and increased susceptibility to drug adverse effects in the elderly are also of importance. One should bear in mind that certain types of damage, such as osteoporosis, cataracts and cerebrovascular accident, in general are more common in the older population and may thus not only be explained by raised activity, long disease duration or corticosteroid side-effects. 1
Persistent proteinuria and/or renal disorder have been associated with a more aggressive SLE.4,9,11 17,26 This was confirmed here, as renal disorder was more common in patients with extensive damage compared to patients without damage. Patients with African-American, Asian and Hispanic heritage have been shown to be afflicted by damage earlier during their disease course than other ethnicities, and they also have an increased risk of renal involvement and a worse outcome overall.17,29,30 Although socio-economics can contribute, increased genetic burden and a higher number of ANA subspecificities may contribute to more severe disease phenotypes in non-Caucasians.17,29,31 However, differences with regard to ethnicity were not observed in the present study. Possibly, this could be explained by the longer SLE duration of Caucasians as well as by the low percentage of non-Caucasians included, albeit comparable with the numbers of other Scandinavian cohorts.32,33
Antidepressant therapy was more prevalent in patients with any damage as well as extensive damage and remained a risk factor in the multiple regression model. Whether this is directly related to SLE, or if it constitutes a consequence of high disease burden, remains to be clarified. Furthermore, SS was more frequent among patients with any damage and extensive damage, which is in line with the observation by Gonçalves et al. 26 Similar to our findings, a frequency of approximately 20% of SS in SLE has been reported.34,35 One study observed worse outcomes including more damage and increased mortality in patients with additional autoimmune diseases, such as SS. 27 In addition, SS was shown to be more common among Caucasians than among other ethnicities. 27 These results corroborate our observation of considerable organ impairment in SLE cases with combined APS and SS. Importantly however, hypothyroidism was not associated with damage in the present study. With La/SSB and aPL as exceptions, we did not identify associations between damage accrual and specific autoantibodies, which corroborates most previous observations.1,18,28,36 Thus, we could not confirm the association between damage accrual and anti-dsDNA that was reported from the Hopkins Lupus cohort. 17
In the multiple regression model, well established risk factors such as APS and hypertension were associated with damage accrual.9,11,26 Antihypertensive therapy could also be a proxy for nephritis as angiotensin-converting enzyme inhibitors are renoprotective and are used to reduce proteinuria. Regarding SLE manifestations, we identified haemolytic anaemia, lymphopenia, neurologic disorder (SLICC-12), pericarditis and myositis to be significantly associated with global SDI scores (Table 4). Neurologic involvement has been suggested as a risk factor for damage, but the other manifestations described above (haemolytic anaemia, lymphopenia, pericarditis and myositis) have not been, to our knowledge, previously reported in association with SDI. 26 Myositis in SLE has been associated with a more active disease, which could explain the association with SDI. 37 In addition, haematological disorder, interstitial lung disease, serositis and aPL (IgG anticardiolipin, anti-β2-glycoprotein-I and LA) were more common among patients with extensive organ damage (Table 3). Possibly, this could reflect the frequent and long-term usage of high doses of corticosteroids in manifestations such as severe cytopenias, serositis and pulmonary involvement where other immunosuppressants occasionally may be insufficient.38,39 Regarding antirheumatic drugs, cyclophosphamide and corticosteroid doses corresponding to ≥7.5 mg prednisolone daily (at last visit) as well as ciclosporin were significant in the multiple regression model for SDI (Table 4). It is conceivable that drugs like cyclophosphamide and ciclosporin are more commonly used in patients with severe lupus (e.g. neuropsychiatric involvement or proliferative nephritis) or as a late alternative treatment in cases who have already acquired damage. An association between use of cyclophosphamide and SDI has been reported, and premature gonadal failure can also be a consequence of this treatment. 19
Use of antimalarials was associated with absence of damage (Table 2) and was potentially protective against accrual of damage (Table 4), which is in line with observations of other studies.1,40 Antimalarials remain the cornerstone of SLE treatment since they not only reduce flares and are efficient for skin and joint manifestations, but they also improve the blood lipid profile and glucose levels, as well as contributing to antithrombotic effects. 41 A Canadian study showed a stronger cholesterol-lowering effect of antimalarials in steroid-treated patients, and other authors have reported lower incidence of osteoporosis following use of antimalarials.42,43 However, patients with highly active or severe SLE are more likely to receive glucocorticoids and other immunosuppressants in addition to antimalarials, whereas the milder cases are more likely to receive antimalarials as monotherapy (i.e. confounding by indication). In this cohort, only 63% of the patients were still taking antimalarials at last visit. As antimalarials are important for inhibiting interferon-signalling in SLE, it will be important to develop alternative treatments for patients unable to tolerate hydroxychloroquine in order to target this pathway and reduce the long-term risk of damage accrual.1,2,40
As previously demonstrated, our data support that male gender and a positive LA test are associated with a shorter time to first damage.28,44 Somewhat surprisingly, diabetes was among the domains with shortest time to first damage. One reason for this could be the increased attention due to the SLE diagnosis, which is often followed by consecutive blood and urine sampling, combined with high doses of glucocorticoids during the first year of disease. The reason for a significantly longer time to first damage in patients with malar rash, depression, hypothyreosis and La/SSB antibodies is not apparent but these factors may constitute markers of milder disease. 22 Of note, all these four factors were more common among female compared to male SLE cases and could thus to some extent explain the gender difference of SDI.
Since the 1950s survival rates have improved, but during the last decades mortality rates have stagnated and unfortunately remain higher than in the general population.6,10 In our cohort, 10% were deceased at the data extraction time point. Malignancy was the leading cause of death, followed by infections and cardiovascular disease. This is partly in line with previous reports, of which some have shown higher rates for ‘active disease’, thrombotic events and cerebrovascular disease.14,33,45,46 A plausible explanation for this is an underestimation of the SLE-related causes of death in Sweden, which was recently highlighted by Falasinnu et al. 47 Among the malignancies, lung and haematological cancers (including malignant lymphomas) were the most common, each constituting almost one third of the malignancy-related deaths in our cohort. Similar observations were made both in a large international SLE cohort study in which hepatobiliary cancer was also found to be overrepresented, as well as in a recent meta-analysis.45,48 Infection, which was the second most common cause of death, has been identified as a frequent cause of death in early SLE and can be linked to high disease activity, high doses of corticosteroids, immunosuppressive therapy and hospitalization.46,49 Early cardiovascular disease has frequently been reported as being overrepresented in SLE, especially in women, and remains a prevailing cause of death, also corroborated in this study.14,50
The large size and well-characterized population as well as the patients' universal access to healthcare constitute strengths of the present study. This, together with our university hospitals being tertiary referral centres, resulted in a high coverage of cases and a subsequent low risk of selection bias. The low number of non-Caucasians and the lack of data on accumulated corticosteroid doses are limitations that may hinder generalization to other parts of the world.
To conclude, despite Swedish healthcare being tax-funded and offering universal access, the majority of patients are still affected by irreversible organ damage over time. We confirmed previously established associations between variables and damage accrual in this study. In addition, SS was associated with (extensive) damage, whereas pericarditis, haemolytic anaemia, lymphopenia and myositis were linked to global SDI in a multiple regression model. Among the modifiable factors, a judicious use of corticosteroids seems to be very important as well as surveillance and prevention of cardiovascular disease and vigilance for malignancies to prevent damage and premature mortality.
Supplemental Material
Supplemental material for The majority of Swedish systemic lupus erythematosus patients are still affected by irreversible organ impairment: factors related to damage accrual in two regional cohorts
Supplemental Material for The majority of Swedish systemic lupus erythematosus patients are still affected by irreversible organ impairment: factors related to damage accrual in two regional cohorts by M Frodlund, S Reid, J Wetterö, Ö Dahlström, C Sjöwall and D Leonard in Lupus
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Swedish Rheumatism Association, the County Council of Östergötland and Uppsala, the Swedish Society of Medicine and Ingegerd Johansson donation, the Selander foundation, the King Gustaf V's 80-year Anniversary foundation and the King Gustaf V and Queen Victoria's Freemasons foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.