
Abstract
We assessed the prevalence and incidence of Systemic Lupus Erythematosus (SLE) in 2010 in adults from four cities in Russia, Kazakhstan and Ukraine. Individuals with SLE were identified retrospectively from the medical records of specialized centers. Prevalent SLE patients were nondeceased city residents, diagnosed prior to December 31, 2010; incident patients were residents newly diagnosed between January 1 and December 31, 2010. Population size was obtained from official census data.
The observed prevalence rates (per 100,000, 95% CI) were 9.0 (7.1–11.2) in Kursk and Yaroslavl, Russian Federation; 20.6 (15.4–27.0) in Semey, Kazakhstan; and 14.9 (10.9–19.9) in Vinnitsa, Ukraine. The cumulative incidence rates (per 100,000, 95% CI) were 1.4 (0.7–2.4); 1.6 (0.4–4.1) and 0.3 (0.0–1.8), correspondingly. All rates were higher among females compared to males, and incidence peaked in the population aged 25–44.
These rates appear slightly lower than those reported from Western Europe and the USA. This could be because of study design (case-ascertainment), local health care practices or true differences in disease risk. Case age and sex distribution was similar to the known epidemiology of SLE. The rates were highest in Kazakhstan, likely because of a predominantly ethnic Asian population.
Introduction
Systemic Lupus Erythematosus (SLE) is a chronic autoimmune disease with a wide spectrum of potentially serious symptoms that may require extensive consumption of health care resources. Describing the epidemiology of the disease will inform allocation of resources to improve SLE management.
The prevalence and incidence of SLE reported in published studies has varied widely. Reported prevalence rates have ranged from four to 250 per 100,000 in the adult population. 1 The majority of epidemiology studies have been conducted in Western Europe and the United States (US). In many countries the epidemiology of SLE remains unknown, and in the Russian Federation and countries of Commonwealth of Independent States (CIS) no information on the prevalence or incidence of SLE has been published to date and no registries have been created. The epidemiology of SLE is known to vary by race/ethnicity 2 and the burden of other systemic diseases has been shown to vary by region, 3 therefore it is important to generate local CIS regional information. This multinational, retrospective epidemiology study (GlaxoSmithKline (GSK) protocol # 116387) aimed to assess the prevalence and incidence of diagnosed SLE in 2010 in the adult population of cities in Russia (Yaroslavl and Kursk), Kazakhstan (Semey) and Ukraine (Vinnitsa). According to official census data, the total (all ages) population in 2010 was 606,900 (268,200 males and 338,700 females) in Yaroslavl, 4 413,500 (183,600 males and 229,900 females) in Kursk, 5 301,471 (138,914 males and 162,557 females) in Semey 6 and 367,500 (163,538 males and 203,962 females) in Vinnitsa. 7
This study is the first epidemiological study of SLE in these countries.
Materials and methods
Study area and population
Study cities were selected as (1) they have a relatively well-demarked population and (2) patient referral patterns are well characterized and (3) the population makeup is reasonably representative of the country as a whole (for example, no ethnic minority group was over-represented). Each city had a single or few large specialized rheumatologic centers at which all local SLE diagnoses would be performed or confirmed (Yaroslavl State Medical Academy, Kursk Regional Clinical Hospital, Semey State Medical University, Vinnitsa Scientific Research Institute of Rehabilitation of the Ministry of Health of Ukraine on the base of Pyrogov National Medical University). The study was overseen at each site by a qualified rheumatologist.
Ascertainment of SLE cases
Trained medical staff manually hand-searched clinical records to identify all patients aged 18 years and older with an established SLE diagnosis according to the American College of Rheumatology (ACR) criteria (presence of four or more criteria) 1 or clinical judgment according to medical records. To be counted in the current study, patients were required to have made at least one clinic visit in 2010 thus ensuring that only those with current disease were counted. Demographic information, the date of SLE diagnosis and the date of first patient-reported SLE symptoms (according to the medical history in source documents) were abstracted from the medical records. Where another local institution was known to provide care for SLE patients, investigators at the study institution contacted those medical care providers to identify any additional cases and to obtain additional patient data.
Prevalent cases were defined as all patients identified from medical records who were diagnosed with SLE prior to December 31, 2010, who were resident in the target city on December 31, 2010 and who were alive on December 31, 2010, according to clinical records. Incident cases were adults, newly diagnosed with SLE between January 1, 2010 and December 31, 2010, and who were resident in the target city at date of diagnosis in 2010 according to clinical records. Patients with miscoded diagnoses and drug-induced lupus were excluded.
Statistical analysis
The denominator for prevalence and incidence calculations was the population aged 18 years and older according to 2010 census data. Information was also obtained through official requests made to the regional statistical departments in Semey (Kazakhstan) and Vinnitsa (Ukraine). When census data were unavailable for the specific age group of 18 and older (for example, Kursk and Yaroslavl report a working population aged 15–16 years and older) the number of persons aged 18 and older was extrapolated using assumptions about age distribution by year of age.
Data from the two Russian cities were aggregated, given the similar ethnic and demographic makeup of the two cities.
City-specific prevalence estimates were adjusted to the age distribution of the region to permit extrapolation to the wider region. Exact 95% confidence intervals (CI) were calculated using the Clopper-Pearson method. 8
Results
Patient ascertainment
Review of medical records yielded the following number of prevalent cases on December 31, 2010: 52 in Yaroslavl, 27 in Kursk, 52 in Semey and 45 in Vinnitsa. The following number of cases with incident diagnosis of SLE between January 1 and December 31, 2010 were identified: 11 in Yaroslavl, one in Kursk, four in Semey and one in Vinnitsa.
Patient characteristics
Characteristics of prevalent cases

All male prevalent cases were from Yaroslavl city. Of 77 female cases, 27 were from Kursk.
Most of the prevalent patients were middle-aged with a median age of 39–47 years across the centers. The median age at SLE diagnosis, as well as at recording of first symptoms, ranged from 29 to 37 years.
Among incident cases in Russia one patient was male (in Kursk) and 11 were female; in Kazakhstan (Semey) all four incident cases were female and in Ukraine (Vinnitsa) one incident case was female. The median age at SLE diagnosis was similar to that recorded for prevalent cases: 42 in Russia, 34 in Kazakhstan (Semey) and 27 years in Ukraine (Vinnitsa). The median age at symptom onset (according to medical records) was 40, 34 and 15 years, correspondingly.
Prevalence of SLE
The prevalence of SLE by age and sex
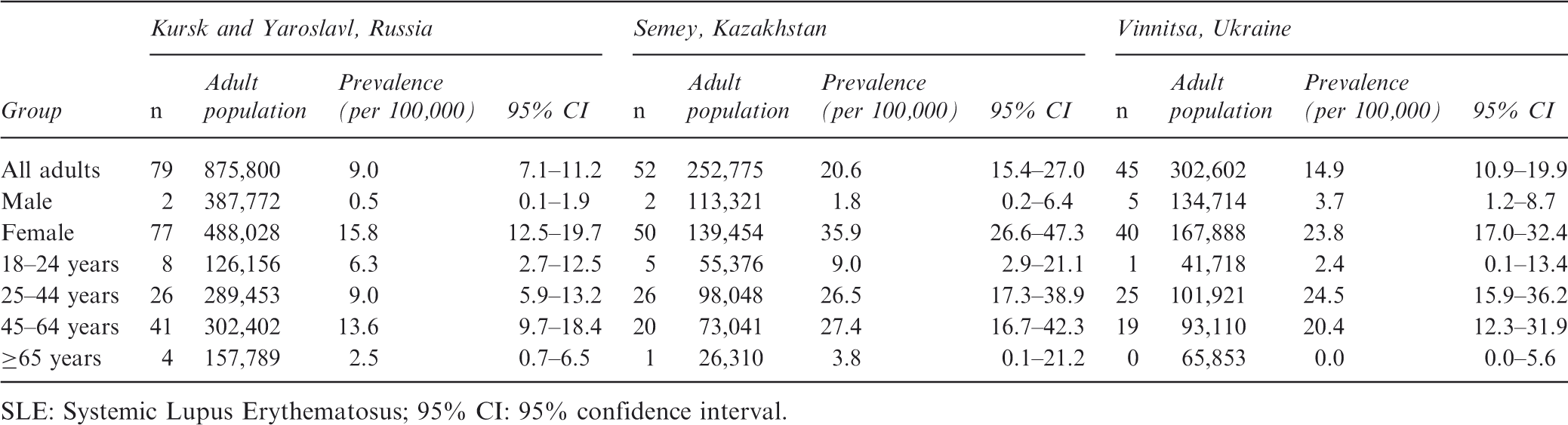
SLE: Systemic Lupus Erythematosus; 95% CI: 95% confidence interval.
The crude prevalence estimates were age-adjusted to the general adult population of each country. The age-adjusted prevalence rates were 7.7 (95% CI 6.1–9.7) in Kursk and Yaroslavl, 17.3 (95% CI 12.9–22.6) in Semey and 12.2 (95% CI 8.9–16.4) in Vinnitsa.
The race/ethnicity-specific prevalence of SLE was estimated in Semey (Kazakhstan), where Caucasians are 43.3% and Asians are 56.0% of total population according to 2010 census data. In Caucasians the SLE prevalence rate per 100,000 persons was 4.6 (95% CI 1.5–10.7). In the Asian population the prevalence was 33.2 (95% CI 24.4–44.2).
Incidence of SLE
Twelve incident cases of SLE were observed in Kursk and Yaroslavl in 2010, four in Semey and one in Vinnitsa. Most incident patients were aged between 25 and 44 years old. The estimated incidence of SLE in the adult population per 100,000 was 1.4 (95% CI 0.7–2.4) in Kursk and Yaroslavl, 1.6 (95% CI 0.4–4.1) in Semey and 0.3 (95% CI 0.0–1.8) in Vinnitsa.
The incidence rates age-adjusted to the general adult population of each country were 1.2 (95% CI 0.6–2.1), 1.3 (95% CI 0.4–3.4) and 0.3 (95% CI 0.0–1.5), respectively.
Discussion
This study is the first epidemiological study conducted to evaluate the prevalence and/or incidence of SLE in CIS countries. A standardized methodology was applied to facilitate comparisons between countries.
The catchment-area based approach, where a catchment area is defined and efforts are made to ascertain all cases within the defined area, is a well-established tool to evaluate prevalence or incidence of rare diseases. 9 In the current study, study cities were selected because they had a well-demarked population with known local referral patterns to a single or a few specialist centers thus reducing the possibility that cases were missed because of referral to another regional center. The population of the study cities was also known to be reasonably representative of the demographics of the study country.
Reported SLE prevalence and incidence across different regions
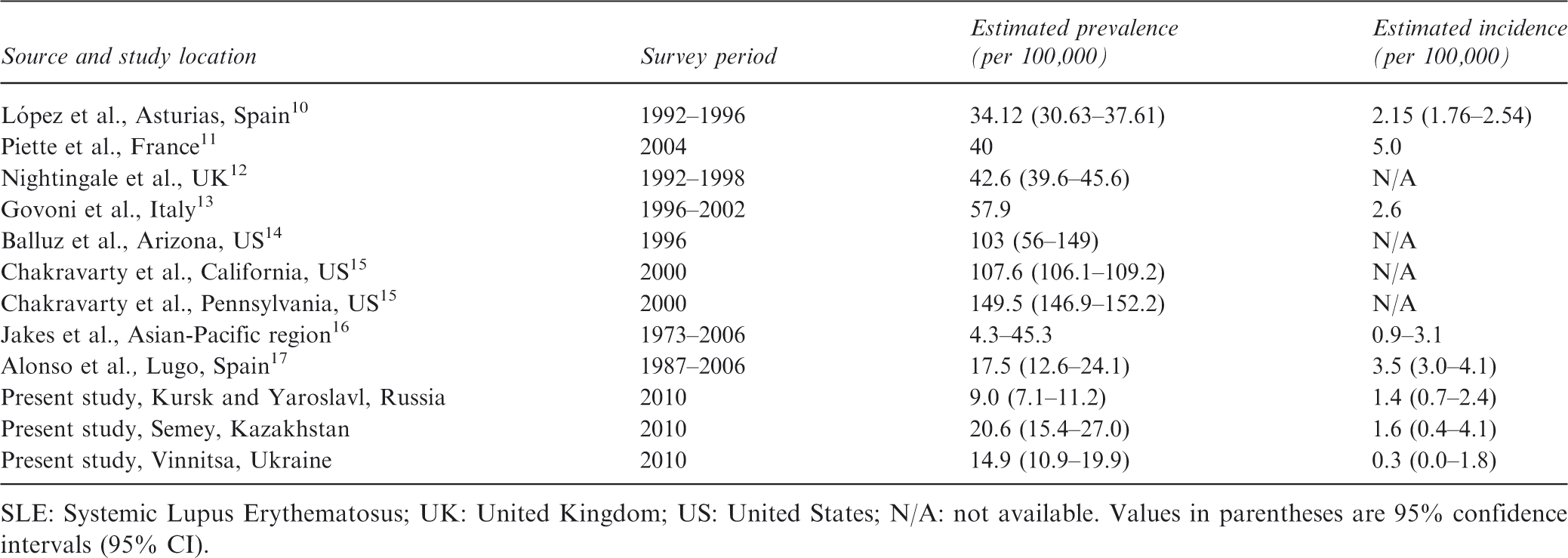
SLE: Systemic Lupus Erythematosus; UK: United Kingdom; US: United States; N/A: not available. Values in parentheses are 95% confidence intervals (95% CI).
This variability may reflect true differences in the burden of SLE across countries or may be the result of methodological differences between studies, 2 and it is difficult to ascertain the extent to which the differences have been real or artifactual. Study design aspects such as differences in the rigor of case ascertainment (one versus multiple sources) or the over-representation of a high-risk sub-population in the study (such as females, or non-white populations) or even differences in health care systems (such as access to rheumatology services) could have led to variation in estimates. However, the incidence of SLE is known to be higher in non-white populations compared to white populations 2 and therefore different nations or regions may have a truly increased or decreased burden of SLE as a result of true biological phenomena.
The current study found a crude prevalence of SLE of 9.0 per 100,000 persons in Russia, 14.9 in Ukraine and 20.6 in Kazakhstan. Although these figures are within the range reported previously in studies, the rates do appear low compared to recent Western European studies, particularly the figures from Russia and Ukraine. This could be due partly to study design. Many Western European studies have been based within long-term funded registries of SLE that have included prospective case-reporting. Others have cross-referenced cases identified in clinical institutional settings with local SLE patient advocacy organizations or registries. Given the absence of these resources in the countries studied, we have been limited to a few settings for case ascertainment within each city. While efforts were made to cross-check cases with other potential local providers (where these existed), there is still the possibility that diagnosed SLE cases were missed.
Further, to be counted in the current study, patients were required to have made at least one clinic visit in 2010. As all patients with SLE would be expected to make at least one visit per year for routine follow-up (and more commonly >1), it was not expected that we would miss patients with current SLE by requiring at least one visit. Most previous studies have not limited case ascertainment to those with sufficient disease activity during the prevalence period to be actively seeking medical care and it may be that previous studies, which have often involved counting those with any record of SLE over a lengthy follow-up time, may have counted patients with long quiescent disease who were no longer actively consuming health care resources.
SLE is a difficult condition to diagnose because of the broad and nonspecific symptom spectrum. It may be, then, that we have captured all individuals diagnosed with SLE but that there are a large number of individuals with SLE who have not been appropriately identified, referred to a specialist and diagnosed. Any screening for systemic diseases is absent in CIS countries; usually people will visit a rheumatologist only if symptoms become troublesome or if the disease begins to flare. As patients with SLE who are well may not regularly visit their provider, we may have missed counting patients whose disease has been quiescent for a number of years. Another possibility, related to health care provision, is that SLE-related mortality may be higher in CIS countries compared to other parts of Western Europe. The incidence of SLE, while lower than many reported figures from Western Europe, is not markedly lower. As point prevalence is approximated by incidence multiplied by duration of disease, it may be that the duration of SLE is shorter in the current countries (either because of higher remission rates or shorter survival). Finally, it may be that the populations in Russia and Ukraine are at lower risk of SLE because of true biological differences. This will need to be established in future studies.
The increased prevalence in Semey, Kazakhstan relative to the other cities was likely because of the large Asian population in Kazakhstan. SLE is known to occur more often in Asian and Afro-Caribbean populations than in the white population.18–21 A recently established registry of SLE patients in Kazakhstan may have contributed to increased identification of SLE prevalence/incidence cases in this country compared to Russia and Ukraine, although the influence of this factor on the study results is not considered substantial.
We acknowledge that the current study has several limitations. The catchment-based approach assumes no net-migrations into or out of the catchment area plus relies on complete case ascertainment within the area. While we made every effort to capture all cases in the region, it is possible that some diagnosed patients were missed and that some cases may have been missed because of misdiagnosis. While the requirement that patients made at least one clinic visit during 2010 may have reduced comparability with other studies, we believe that the current rates represent the frequency of SLE severe enough to consume health care resources. These figures are arguably more relevant for planning of health care resources.
In addition to using a single, primary site for case ascertainment (because of lack of additional sources), limitations of the study included the following considerations. The study was conducted within single cities that contained a leading rheumatology center. These settings were selected on the basis that they were quite “contained” in terms of health care as the full range of health care services was available and local residents would be expected to attend local services for all health care needs. The populations of these cities, however, may not be representative of each country in general. We have tried to reduce this effect by adjusting for age but it still remains possible that residents of these cities differ from the wider national population. SLE risk factors and health care provision (including access to specialized SLE centers) may widely vary within the countries.
In conclusion, the prevalence and incidence of SLE in selected cities from the CIS region were within the range of estimates reported previously, but were lower compared to that in Western European studies. The rates were highest in Semey (Kazakhstan) likely because of a predominantly ethnic Asian population.
Contributors
All authors took active part in this study. Authors participated in critical revisions of the manuscript and have approved the article for publication. The authors contributed to manuscript review, applying their clinical, epidemiology, and study design expertise.
Footnotes
Funding
The funding for the study was provided by GlaxoSmithKline, Brentford, Middlesex, United Kingdom. GlaxoSmithKline eTrack study identifier: EPI116387. GlaxoSmithKline study acronym: ESSENCE.
Conflict of interest statement
The study was sponsored by GSK.
AG received payments for consultancy from Novartis Pharma. AG was a member of the SLE Advisory Board organized by GSK and participated in clinical trials of GSK. OI received fees from MSD, Abbott, Servier and Roche, and has received payment for lectures and educational presentations at advisory boards organized by GSK and at an internal meeting organized by GSK. S Shevchuk received payments for clinical trials sponsored by Boehringer Ingelheim and AstraZeneca.
No information of collaboration with specific companies is provided by GT and ZO.
AL has collaborated with MSD, Abbott, Dr Reddys, Bayer, Novartis, GSK, Berlin-Chemie, Rompharma and Stada.
S Soloviev has collaborated with Orion Corporation, Roche, UCB, Novartis, and GSK.
EN has collaborated in the past five years with Roche, UCB, Novartis, GSK, MSD, Abbott, Medac, Eli Lilly, Bristol-Myers Squibb, Amgen and Servier.
AV, ZS, VC and KM are employed by GlaxoSmithKline. JD and MH are employed by and own stock in GlaxoSmithKline.
Acknowledgments
We thank all investigators for their contribution to the study, allowing the first epidemiology study of SLE in these countries to have been conducted with a high level of integrity.