
Abstract
Introduction
Methanol toxicity is a significant health concern with potentially severe outcomes. This study aimed to investigate the prognostic factors of patients with methanol toxicity referred to Tabriz Sina Hospital.
Methods
A descriptive-analytical retrospective study was conducted in methanol toxicity patients admitted in Tabriz Sina Hospital since 2019 to 2021. Demographic characteristics and management methods were extracted from the patients’ medical records.
Results
Patients were predominantly male (91.3%) with a median age of 30–40 years. Winter accounted for 48.7% of cases. Coma (OR = 8.0, 95% CI: 3.2–19.9) and arrhythmia (OR = 5.5, 2.0–15.1) at admission, pH <7.1 (OR = 4.2, 2.0–8.9), elevated creatinine (OR = 1.3/mg/dL, 1.1–1.6), opiate co-use (OR = 2.8, 1.2–6.5), and delayed ethanol therapy (>3 h, OR = 2.3, 1.1–4.8) independently increased mortality risk. Bicarbonate, Eprex, and methylprednisolone reduced complications. Time from ingestion to admission (48–72 h) did not affect mortality, but delayed hemodialysis initiation worsened outcomes.
Conclusion
Early presentation and providing early therapeutic modalities have a significant impact on the mortality rate and the patients’ outcome.
Introduction
Methanol intoxication is a life-threatening alcohol poisoning that can be related with a significant mortality if not early diagnosed and treated.1–3 It is highly toxic with sever morbidities (vision problems, blindness, metabolic, cardiac, and serious neurological disorders) even after hospital discharge. Necrosis of basal ganglia and white matter and diffuse cerebral edema can cause to poor prognosis.4–6 Methanol poisoning is mostly occurred by direct ingestion in doses as small as 15 mL and rarely through inhalation or skin absorption. This substance is rapidly absorbed from GI tract in less than 10 min and reaches the peak plasma concentration in 30–60 min. When it was metabolized into its metabolites, it is highly toxic especially for central nervous system.3,4
The prevalence of heavy alcohol use is variable in the world and reported as 7.5% in the general population. 7 There are no any exact reports of alcohol poisoning and its prognosis in Iranian society. Although heavy drinking in Iran has been reported as less than 1% of alcoholics, it should be assuming that most of alcohol abusers and their prognosis have not been reported because of the presence of social stigmas. 7
Methanol is widely used in industry; nevertheless, methanol poisoning is not common. 8 Illicit and informal productions are responsible for majority of methanol poisoning.3,4 In Iran because of religious issues and legal and social restricts, production, selling, buying and ingestion of alcohol is illegal and people who drink alcohol, use industrial or homemade ethanol. 9 In addition, fear of legal problems causes that these cases often present to health care centers too late. This causes treatment modalities to be insufficiently effective enough and subsequently lead to a severe morbidity and high mortality. However, in many centers, the privacy of patients is kept secret and alcohol poisoning is not reported. Consequently, there is no any exact report of alcohol poisoning and its outcome in Iranian society. 7 The leading causes of methanol intoxication are the unawareness of the society from the hazards of toxic alcohol together with the spread of fake information and recommendations across social networks. 10
Treatment involves administering a buffer to rectify metabolic acidosis and an antidote to impede the conversion of methanol into its deadly metabolite, formic acid. Haemodialysis is used, if required, to rectify acidosis and eliminate both methanol and formate. 11 Study conducted by Hovda et al. indicated that fomepizole can be useful and the effectiveness and adverse effect profile of fomepizole might alter the function of haemodialysis in cases of methanol poisoning. 12 However, a study conducted by McMartin et al. indicated that ethanol continues to be a significant option, since availability to fomepezole may be restricted, its cost may seem prohibitive, or the physician may choose ethanol based on prior experience. 13 Contemporary research underscores the importance of identifying prognostic biomarkers to stratify patient risk and optimize resource allocation. For instance, systemic acidosis, elevated creatinine levels, and altered mental status at admission have emerged as consistent predictors of mortality. 2 Studies also show that nutrition can have a significant impact on health. 14 Innovations in supportive care, such as erythropoietin (Eprex), 15 and corticosteroids, 16 have shown promise in mitigating optic neuropathy and inflammatory damage, though their integration into standardized protocols remains debated.
Identification of high-risk patients with poor prognosis is vital for early diagnosis and rapid treatment of methanol poisoning to prevent death and improve the outcome. Considering the high mortality of methanol poisoning and the high prevalence of short-term and long-term complications in these patients and the significant prevalence of methanol poisoning, especially in the young people, this study can identify effective factors in early referral and prognostic factors. Identifying the prognostic factors in these patients provide the basis for improving the quality of therapeutic interventions. The aim of this study was to evaluate the clinical and laboratory factors in patients with methanol poisoning to determine the prognosis and improve the outcome.
Methods
Study design and setting
This descriptive-analytical retrospective study was conducted in methanol toxicity patients admitted in Sina Trauma Center, Tabriz, Iran, since 2019 to 2021. Demographic characteristics and management methods were extracted from the patients’ medical records.
Participants
The study population comprised 667 initial cases of methanol toxicity, of which 552 were initially reviewed. After excluding cases with incomplete data or incorrect diagnoses, 242 patients were included in the final analysis (Figure 1). Medical records were retrieved using ICD-10 coding (T51.1 for methanol poisoning) combined with keyword searching (e.g., “methanol toxicity,” “methylated spirit”) in the electronic health system of Sina Center. STROBE-compliant flow diagram of patient screening and inclusion (667 screened → 242 included).
Data collection
For data collection, variables were categorized as follows:
Demographic and clinical characteristics
Age, sex, date and time of admission, year and season of hospitalization, level of education, and history of underlying diseases.
Symptoms and clinical findings
Presence of parkinsonism symptoms (e.g., tremors, rigidity), nausea/vomiting, altered level of consciousness at presentation, seizure occurrence, time elapsed since methanol ingestion, and blurred vision upon emergency room (ER) admission.
Treatment and management factors
Reason for methanol abuse, concomitant use of opium or benzodiazepines, heart rate and rhythm, arterial blood gas (ABG) parameters at admission and discharge, timing of dialysis catheter insertion, pre-dialysis interventions, timing and duration of first and second hemodialysis sessions, length of ER stay, total hospitalization duration, time to initiation of treatments (ethanol, folic acid, bicarbonate, Eprex, Fomepizole, methylprednisolone), and need for intubation.
Laboratory and diagnostic parameters
Serum levels of blood sugar (BS), sodium (Na), potassium (K), hepatic enzymes (ALT, AST), creatinine, and blood urea nitrogen (BUN).
Outcomes
Primary outcome was the need for hemodialysis; secondary outcomes included mortality and development of persistent symptoms (e.g., visual impairment, neurological deficits).
Diagnosis was based on clinical presentation, laboratory findings (e.g., anion gap metabolic acidosis), and exposure history, as direct methanol/formate measurements were unavailable due to limited resources.
Statistical analysis
The data were analyzed using SPSS-22 software. To assess the relation between evaluated factors and outcome of alcohol poisoning, Mann-Whitney test (to compare quantitative and ordinal data), Chi-square test, and Fisher’s exact test (for qualitative data) were used. To evaluate independent risk factors, a multivariate logistic regression was formulated to identify independent risk factors. p-values more than 0.05 were considered as the level of statistical significance. Multivariable logistic regression was performed to identify independent risk factors for mortality and poor outcomes (composite of death, visual sequelae, or neurological sequelae). Variables with (p < 0.1) in univariate analysis or clinical relevance were included in the initial model. Backward stepwise selection (retention threshold: p < 0.05 was used to derive the final model. Results are reported as adjusted odds ratios (OR) with 95% confidence intervals (CI).
Ethics approval and consent to participate
The study was reviewed and approved by the Ethics Committee of Tabriz University of Medical Sciences. This research was based on anonymized patient records, and all data were handled confidentially. The authors adhered to ethical guidelines for research conduct. Informed consent was waived by the ethics committee due to the retrospective design and exclusive use of de-identified data.
Results
This study conducted on 242 patients including 221 (91.3%) male and 21 female (8.6%) with age between 15 and 65 years (Figure 2). Distribution of the sex variable of participants.
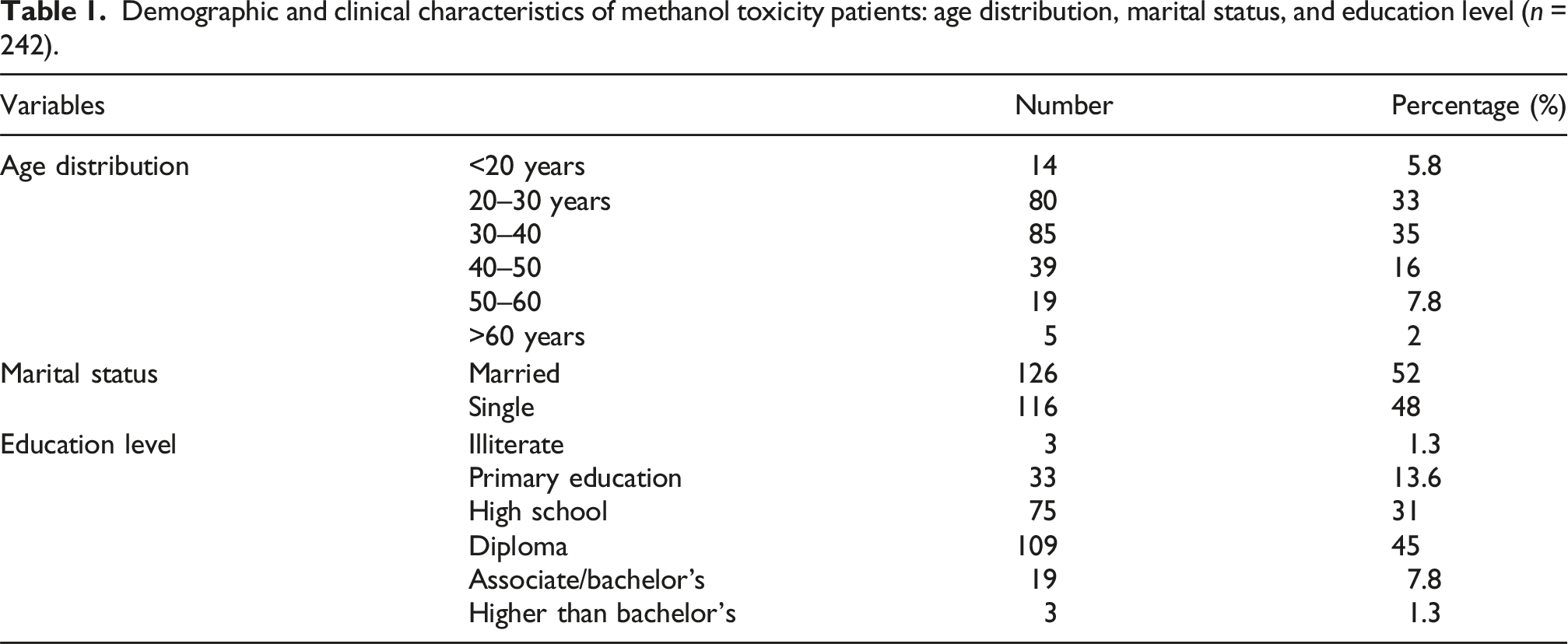
Demographic and clinical characteristics of methanol toxicity patients: age distribution, marital status, and education level (n = 242).
According to the obtained results in Figure 3, the prevalence of toxic methanol is not the same in different seasons. The most common season for presentation was winter with 118 cases (48.7%), followed by spring with 81 (33.5%), autumn with 24 (10%), and summer with 19 (7.8%). The consumption cycle starts from late of autumn and peaks in winter and reaches its minimum in summer (Figure 3). Sex distribution of methanol toxicity patients.
Association between level of consciousness at admission and clinical outcomes in methanol toxicity patients (n = 242).

The relation of mortality and outcome with some variables at the admission with using Spearman’s Rho (n = 242).
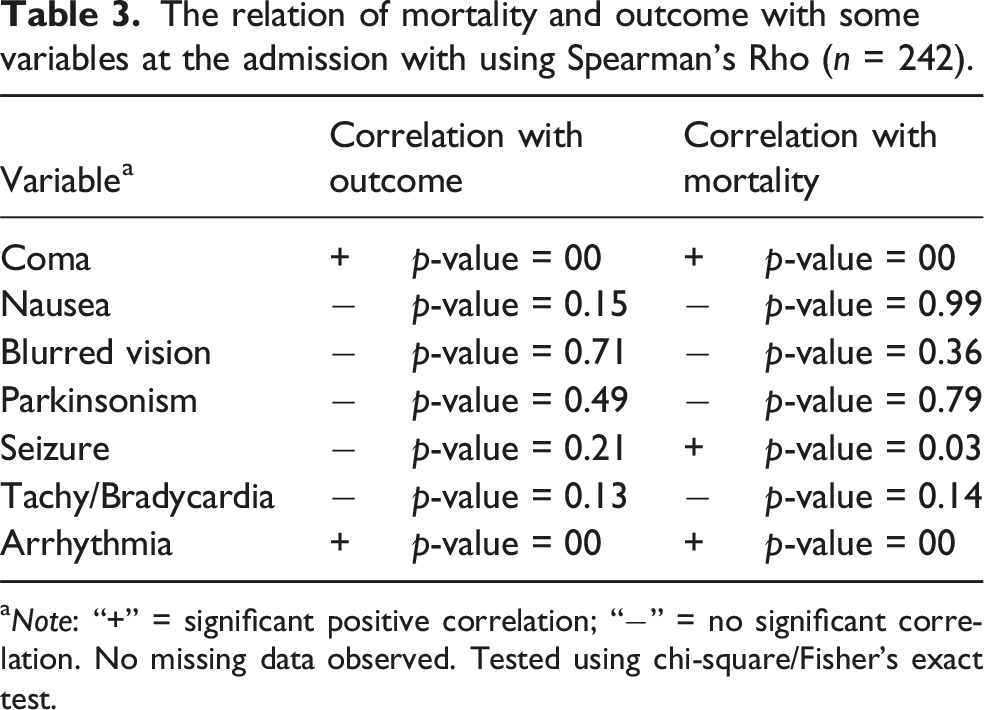
aNote: “+” = significant positive correlation; “−” = no significant correlation. No missing data observed. Tested using chi-square/Fisher’s exact test.
Correlation of laboratory parameters with outcomes using Spearman’s Rho.

aNo missing data observed.
The relation between the concurrent use of opiates and mortality was significant (p < 0.05), while we did not any significant relation between the use of benzodiazepines and mortality (p < 0.05) and outcome (p < 0.05). According to the results of the Wilcoxon test, the laboratory results at admission were significantly different from those at discharge (p = 0.00), indicating that the therapeutic measures have improved the patient’s condition. Of therapeutic measures performed, prescribing Bicarbonate (p = 0.03), Eprex (p = 0.03), and Methylprednisolone (p = 0.01) had a significant relation with the disease outcome, and significantly have reduced the complications caused by methanol abuse. Fomepizole was used with no significant outcome association (p > 0.05).
Multivariate logistic regression analysis for mortality.

aNote: Variables included in the multivariate model were selected based on univariate analysis (p < 0.1) or clinical relevance.
Discussion
In this study, we evaluated the clinical and para-clinical factors affecting the prognosis of methanol toxicity in 242 patients. The findings indicated that presence of some complications on admission, including loss of consciousness, arrhythmias, blood glucose, sodium, and potassium imbalances, impaired liver and renal function, acidosis, concurrent drug or substance abuse, as well as delay in hemodialysis, were associated with poor prognosis (Death and Sequelae).
Methanol poisoning is a significant risk factor for mortality and disability. According to the Global Burden of Disease (GBD) study, alcohol use ranked as the seventh risk factor for premature mortality and disability-adjusted life years (DALYs) in 2016, relative to other risk factors. 17 A study by Aghababaeian et al. revealed that 768 individuals in Iran were reported as poisoned from September 7 to October 7, 2018, due to the consumption of informal alcohol containing methanol, resulting in 76 fatalities (10.1% fatality rate); 460 individuals sought treatment at state hospitals for acute methanol poisoning, of which 42 (9.13%) succumbed. A total of 177 participants (38.4%) were hospitalised, whereas 241 subjects (52.3%) were evaluated and subsequently released. Men constituted 93% of the fatalities. 18 The patient cohort was predominantly male (91.3%), aged primarily 20–40 years, aligning with global patterns indicating a higher prevalence of methanol poisoning and related mortality among men, often attributed to increased alcohol consumption rates.7,9,19–22
Methanol itself is relatively inert; its severe toxicity arises from its metabolism to formic acid. 23 This metabolite accumulates, particularly in the retina and basal ganglia, causing visual disturbances (including blindness) and neurological damage, while also inducing profound metabolic acidosis and histotoxic hypoxia.24,25 The slow metabolism contributes to delayed symptom presentation, and fatalities often occur before hospitalization. 22 The mortality rate in the present study was 6.6%. In comparison, it has been reported as 12.5% by Navabi et al., 20 20% by Baghi et al., 7 17.9% by Eghbali et al., 19 and 34.4% in the Taiwanese patients. 26 Methanol poisoning causes high mortality and morbidity. Studies in Estonia, Norway, and Czech have reported the acute mortality of 18–21%, and the sequelae after survival ranged between 10 and 34%. 27
Despite advances in diagnosis and treatment of methanol poisoning, the long-term prognosis for survivors of methanol poisoning is not good.24,25 Mortality and poor prognosis has been associated with pH less than 7, coma on admission and more than 24-h delay from intake to admission.19,28 Hongyi et al. showed that methanol poisoning can lead to severe visual impairment, and the prognosis of visual acuity was highly relevant to the duration of toxic exposure, delayed admission, and severity of acidosis. 29 If treatment is delayed or inadequate, mortality may raise up to 40%, and even if the patients survive, it can lead to permanent blindness and long-standing complications on their central nervous system. 22
Methanol poisoning is the most common indication for hemodialysis amongst toxic alcohol intoxications. 24 In Bagi et al. study, the mean of time interval between consumption to admission was 7.8 ± 16.4 h (range: 1–96). 7 In the present study, the time between drink and admission (48 to 72 h) was not in significant relation with mortality (p > 0.05) or complications (p > 0.05). The time between admission and insertion of the hemodialysis catheter (an average of 1:27 h) had a significant relation with outcome (p < 0.05), but not with mortality (p > 0.05). Also, the time interval between catheter insertion and performing hemodialysis (2:58 h on average), had a significant relation with outcome (p < 0.05), but has not with mortality (p > 0.05).
Metabolic acidosis, and an altered mental status on admission have been reported to be associated with mortality in methanol poisoning. 2 Need for dialysis and elevated creatinine level were reported as independent risk factors of mortality. 7 Also, increasing the potassium, blood glucose, 29 and hematocrit have been a significant relation with death. 7
In the present study, the mortality and outcome have a significant relationship with presence of arrhythmias and loss of consciousness at admission and the mortality was more in patients presenting with coma (p > 0.05). Also, there was a significant relationship between the laboratory results including pH, bicarbonate, Na, AST, Cr and urea level with the mortality (p < 0.05). The pH less than 7.1 at admission has a significant relationship with outcome (p < 0.05) and mortality (p < 0.05).
Navabi et al. in 5-years study showed that consciousness level, creatinine level, and pH of methanol-poisoned patients in admission can predict the outcome of treatment or mortality.20,26 Study of Desai et al. on 122 patients showed that degree of acidosis at presentation appears to determine final visual acuity; early presentation and treatment did not seem to significantly alter the visual outcome, especially in severe poisoning. 30
Lee et al. indicated that Glasgow Coma Score score, and serum creatinine level predict mortality after methanol poisoning. 26 In Gulen et al. study, High anion gap metabolic acidosis, low GCS were found to be associated with poor prognosis and mortality. 31 Paasma combined the data from methanol outbreaks in Norway, Iran and Tunisia, and found that unconsciousness on admission was associated with a bad prognosis, as well as having sever acidemia. 21 In the study by Navabi et al. there was a significant relationship among mortality and coma, blurred vision, laboratory symptoms (glucose, urea, creatinine, AST, ALT, pH and bicarbonate), and cardiac arrhythmias. 20 Yousefinejad et al. showed that the time interval from methanol intake to hospital admission, and higher blood glucose, creatinine and potassium had a significant correlation with poor prognosis; but, pH and HCO3 did not had a significant association with bad outcome. 22
In the present study, the relation between the concurrent use of opiates and mortality was significant (p < 0.05), while we did not any significant relation between the concurrent use of benzodiazepines and mortality (p < 0.05) or outcome (p < 0.05). Similar study showed that drug history, alcohol consumption history, smoking, and opium use do not relate to mortality. 7
In the present study, the laboratory results at admission were significantly different from those at discharge (p = 0.00), indicating that the therapeutic measures have improved the patient’s condition. Of therapeutic measures performed, prescribing Bicarbonate (p = 0.03), Eprex (p = 0.03), and Methylprednisolone (p = 0.01) had a significant relation with the disease outcome, and significantly have reduced the complications caused by methanol abuse.
Early hemodialysis, ethanol, bicarbonate and supportive therapy can be life-saving in methanol intoxication. 32 Hemodialysis is the best method to fast removal of toxic acid metabolites and alcohol itself, and it plays a central role in treating severe poisoning. Nizhu et al. recommend early hemodialysis to reduce complications and improve outcome. 33
Bicarbonate administration in severe acidosis caused by methanol may reverse visual deficits and help reduce the amount of active formic acid creation.34,35 Thereafter, methanol and its serum metabolites can be removed by hemodialysis.24,25,35
In the study by Navabi et al. prescription of ethanol, corticosteroid and bicarbonate, and timely frequent hemodialysis improved the outcome. 20 Protective effect of erythropoietin (Eprex) on methanol-induced optic nerve may be efficient at the start of mediation. 36 Intravenous erythropoietin can improve the visual acuity in optic neuropathy caused by methanol; it can represent a new promising treatment for methanol-induced optic neuropathy. 37 Nekoueifard and Majidi indicated that the low doses of subcutaneous erythropoietin relieved the acute optic neuropathy in methanol intoxication and reversed the blindness to normal vision. 38
It seems that multidisciplinary strategies are required for controlling adverse effects of methanol intoxication. These policies must be directed to reduce the harmful effects of alcohol consumption and its complications. These strategies can be planned in national, regional, and universal levels and may involve all aspects of production, sales, and education of consumers, preventive interventions, and therapy in emergency wards and health care systems. Health organizations have also a crucial role in managing the various problems of alcohol poisoning by providing preventive, therapeutic, and rehabilitation services, and improving the knowledge and attitude of the society to prevent alcohol abuse especially homemade products, and informing people from risks of alcohol abuse specifically methanol.
Limitations
The study had some limitations. It was a retrospective study, and timing and quality of interventions may differ. The retrospective design inherently carries risks of recall bias and missing data, particularly for sensitive information such as alcohol consumption history, which may have been underreported due to social stigma. A problem was social stigma against alcohol consuming in our society. So that, the information about the history of alcohol consumption and other substance abuse may be not accurate enough. On the other hand, lack of laboratory equipment to measure the blood methanol level caused that methanol poisoning could not exactly have separated from ethanol poisoning. The data have not laboratory confirmation (methanol, formate), and diagnosis is based on clinical features, laboratory tests, and blood gas analyses. Additionally, the small number of deaths (n = 16) limits the power to detect weaker associations. While we prioritized parsimonious modeling, future studies with larger cohorts are needed to validate these findings.
Conclusions
The study identified several critical prognostic factors influencing outcomes in patients with methanol toxicity, emphasizing the importance of early recognition and intervention. Coma at admission, arrhythmia, severe metabolic acidosis (pH < 7.1), elevated creatinine levels, concurrent opiate use, and delayed ethanol administration (>3 h post-admission) were independently associated with increased mortality risk. Conversely, timely hemodialysis initiation, along with therapeutic interventions such as bicarbonate, Eprex, and methylprednisolone, significantly improved outcomes by mitigating complications. These findings underscore the need for rapid clinical assessment, prioritization of ethanol therapy within the critical window, and close monitoring of metabolic and cardiac parameters to reduce mortality and long-term sequelae in methanol-poisoned patients.
Footnotes
Ethical considerations
The study was reviewed and approved by the Ethics Committee of Tabriz University of Medical Sciences. This research was based on the information in the patients’ records, and the studies and findings were kept completely confidential. Additionally, the authors read the guidelines of ethical codes in research and followed them. The need for informed consent was waived by the ethics committee of Tabriz University of Medical Sciences due to the retrospective nature of the study, and the use of anonymized patient data only.
Author contributions
AS: Conceptualization, Methodology, Writing, Reviewing and Editing; OA: Data Curation, Conceptualization, Original draft preparation; CH; Data Curation, Original draft preparation; AH: Writing, Original draft preparation, Reviewing and Editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.