
Abstract
Benzodiazepines, often used to treat anxiety, insomnia, and other conditions, are prescribed more frequently to women than men, and emergency department visits and overdose deaths involving benzodiazepines have increased significantly among women in recent years. This study describes characteristics and trends associated with benzodiazepine exposures among women of reproductive age (15–49 years old) that were reported to United States poison control centers from 2004 through 2018. The National Poison Data System recorded 258,370 first-ranked benzodiazepine exposures among women 15–49 years old during the study period. More than one-half (56.9%) of exposures involved a single-substance and one-third (34.0%) occurred among women 20–29 years old. The majority were categorized as “intentional, suspected suicide” (73.2%) or “intentional” (12.9%). Exposures frequently resulted in admission to a psychiatric facility (20.6%), critical care unit (18.1%), or non-critical care unit (9.3%). Twenty percent of cases resulted in a serious medical outcome, including 205 deaths. The substantial percentage of benzodiazepine exposures among women of reproductive age that were intentional and associated with suicide attempts or suicide deaths indicate that increased prevention efforts are needed to address this issue.
Introduction
Benzodiazepines are used to treat medical conditions such as anxiety, insomnia, and seizures, and can be beneficial for their ability to induce a relaxed state. Prescribing and use of benzodiazepines has increased in the United States (US) in recent years, despite concerns about the drugs’ addictive qualities and their association with opioid analgesic misuse and overdose.1–6 Risk of benzodiazepine tolerance and dependence increases with prolonged use and efforts have been made to promote less risky alternatives when long-term treatment of anxiety or other conditions is needed.7–10
Between 1996 and 2013, the number of US adults filling at least one benzodiazepine prescription in a given year increased 67% to approximately 13.5 million individuals. 1 Simultaneously, the total quantity of benzodiazepine doses distributed to US adults more than tripled. 1 A recent study found that greater than one in eight US adults used a benzodiazepine drug in the past year, with 17% of all use categorized as misuse (e.g., using the drug without a prescription or more frequently than prescribed). 4 While benzodiazepine use increases with age, the drugs are also prescribed to children and adolescents.11–16
Benzodiazepine-related overdose deaths are rare when the drugs are used alone; however, using benzodiazepines in combination with other drugs, particularly opioids and/or alcohol, significantly increases the risk of overdose death.1,3,17–27 Concomitant use of benzodiazepine and opioid medications can amplify the drugs’ side effects, including respiratory and central nervous system depression.17,20,22,25,26,28 Despite the increased fatality risk, simultaneous benzodiazepine and opioid use is not uncommon.3,25,29–33 A study of opioid overdose deaths in 25 US states from January 2018 through June 2018 found 32.5% also involved benzodiazepines. 34 While some concurrent benzodiazepine and opioid medication exposures occur without awareness of the risks, others result from intentional drug abuse or misuse. 3
Benzodiazepines are used more frequently among women than men, resulting in higher rates of overdose among this population. 35 Overdose-related emergency department visits and deaths involving benzodiazepines have increased significantly among women in recent years.4,12,14,36 From 1999 to 2017, the rate of drug overdose deaths involving benzodiazepines among women 30–64 years old increased 830%. 37 This increase was observed across all age groups of women from 30–34 years to 60–64 years. 37
Benzodiazepine and benzodiazepine-like drugs (e.g., zolpidem) are the second most commonly used psychotropic medications among pregnant women. 38 The risks associated with benzodiazepine use during pregnancy are uncertain, but may include spontaneous abortion and congenital malformations.39–43 Infants exposed to benzodiazepines in utero may have increased risk of small head circumference and low birth weight, but these outcomes may also be independently associated with maternal anxiety.41,44–46 Benzodiazepine use near the time of delivery is associated with poor muscle tone, drowsiness, and feeding difficulties among newborns and the drugs can pass to infants through breastmilk.28,42
The purpose of the current study was to retrospectively investigate acute and chronic benzodiazepine exposures among women 15–49 years of age that were reported to US poison control centers (PCCs) over a 15-year period from 2004 through 2018. This work provides an epidemiologic overview of exposure characteristics and trends that may help to inform future recommendations related to benzodiazepine prescribing and use by women of reproductive age.
Methods
Data sources
Study data were obtained from the National Poison Data System (NPDS), which is maintained by the American Association of Poison Control Centers (AAPCC). 47 The NPDS captures data from calls to regional PCCs in the US and its territories. Trained poison specialists respond to telephone calls from the public and healthcare professionals 24 h a day, 365 days a year. They provide callers with information about poisonous substances and advice on exposure management. Poison specialists record data from all exposure calls in the NPDS and adhere to strict quality control processes to promote data accuracy and completeness. July 1 population estimates from the US Census Bureau were used to calculate annual exposure rates. 48
Case selection criteria
Data on single-substance and polysubstance benzodiazepine exposures reported to US PCCs from 2004 through 2018 were obtained from the AAPCC. Benzodiazepine exposures were identified using the AAPCC generic codes for benzodiazepines. The study was restricted to women of reproductive age (15–49 years), as defined by the World Health Organization. 49 Exposures were excluded from the study if (1) the medical outcome was coded in the NPDS as “confirmed non-exposure” (n = 391) or “unrelated effect, exposure was probably not responsible for the effect(s)” (n = 6527), (2) the reason for exposure was “unintentional—occupational” (n = 177), “unintentional—environmental” (n = 84), “unintentional—bite/sting” (n = 17), “unintentional—food poisoning” (n = 42), “other—contamination/tampering” (n = 274), or “adverse reaction—food” (n = 58). In addition, 26,423 duplicate cases were excluded from the dataset.
Study variables
Age was grouped into 15–19 years, 20–29 years, 30–39 years, and 40–49 years. Medical outcome was categorized as: (1) no effect; (2) minor effect; (3) moderate effect; (4) major effect; (5) not followed, minimal clinical effects possible; (6) unable to follow, judged as potentially toxic exposure; and (7) death. Per NPDS definitions, minor effect is defined as “minimally bothersome to the patient” and resolves rapidly. Moderate effect is “more pronounced, more prolonged, or more of a systemic nature than minor symptoms” and typically some form of treatment is indicated. When major effects are experienced, individuals develop symptoms that are “life-threatening or result in significant residual disability or disfigurement.” The term “serious medical outcomes” in this study includes outcomes of death, major effect, and moderate effect. Reason for exposure is categorized as the following: (1) unintentional; (2) intentional, suspected suicide; (3) intentional; (4) other; and (5) unknown. “Unintentional” includes the following NPDS-coded reasons for exposure: “unintentional--general,” “unintentional—therapeutic error,” and “unintentional—misuse.” The term “intentional” includes “intentional—misuse,” and “intentional—abuse.” “Other” includes “other—malicious,” “other—withdrawal,” “adverse reaction—other,” and “adverse reaction.” The category “unknown” includes exposures coded as “unintentional—unknown,” “intentional—unknown,” and “unknown reason.” According to NPDS coding definitions, unintentional exposures result from an “unforeseen or unplanned event” while intentional exposures result from a “purposeful action.” Exposures that are labeled as “unknown” may be identified as unintentional or intentional, but not have a specific motive (e.g., misuse) that can be determined.
Additional study variables included in the analyses were year of exposure, chronicity of exposure (acute, acute-on-chronic, chronic, or unknown), management site, level of health care received, related clinical effects, and performed therapies. Management site was categorized as the following: (1) patient already in (en route to) a health care facility (HCF) when PCC called; (2) patient was referred by PCC to an HCF; (3) managed on site (non-HCF); (4) other; and (5) unknown. Level of health care received was categorized as (1) admitted to critical care unit; (2) admitted to non-critical care unit; (3) admitted to psychiatric facility; (4) treated/evaluated and released; (5) no HCF treatment received; (6) patient refused referral/did not arrive at HCF; and (7) patient loss to follow-up/left against medical advice.
Statistical analyses and ethical considerations
NPDS data were retrospectively analyzed using SAS 9.4 (SAS Institute, Inc., Cary, NC, USA). When categorizing polysubstance exposures, the NPDS ranks each substance according to its likelihood of contributing to the observed clinical effects. For the current study, single-substance and polysubstance exposures for which benzodiazepines were ranked first were included when analyzing general characteristics. Only single-substance exposures were considered when calculating the frequency of the related clinical effects and the performed therapies, to avoid potential interaction effects that may be observed in polysubstance exposures. All exposures were included in the calculation of annual exposure rates. Simple or piecewise linear regression models, as appropriate, were used to analyze secular trends of exposures with break points based on preliminary evaluation of scatter plots. The estimated slope from the regression model (m) was reported with the associated P value. Statistical significance was determined at P = 0.05. This study was judged exempt by the institutional review board at the authors’ institution.
Results
General characteristics
From 2004 through 2018, US PCCs managed 445,862 benzodiazepine exposure cases, 258,370 of which met the study criteria. More than one-half (56.9%) of the cases were single-substance (n = 146,999). The age group with the most cases was females 20–29 years old (34.0%; Table 1). The majority of the cases were intentional and most resulted from suicide attempts (73.2%). Most cases were acute (66.4%). Regarding level of health care received, 21.6% of cases were treated/evaluated and released, 20.6% were admitted to a psychiatric facility, and 18.1% were admitted to a critical care unit. More than one-third of cases (37.3%) resulted in minor effects, and 19.6% experienced serious medical outcomes.
Characteristics of benzodiazepine exposures among women 15–49 years of age, NPDS 2004–2018.

HCF: Health care facility; PCC: Poison control center.
a Polysubstance exposures include only cases in which benzodiazepines were the first-ranked substance.
b The column percentages may not sum to 100.0% due to rounding errors.
c Frequencies in the unknown category were omitted from the denominator during calculation of percentages.
Single-substance exposures
Among 146,999 single-substance exposures, most cases were acute (67.3%), involved women 20–29 years old (36.1%), and were attributed to a suspected suicide attempt (68.4%; Table 1). The most common medical outcome for single-substance exposures was minor effect (35.2%) and 13.0% of single-substance exposures resulted in serious medical outcomes.
Polysubstance exposures with benzodiazepine as the first-ranked substance
Among 111,371 polysubstance exposures with a benzodiazepine as the first-ranked substance, cases most commonly involved women 20–29 years old (31.3%), were acute (65.3%), and were coded as intentional suicide attempts (79.6%). One-quarter (25.5%) of women with a first-ranked benzodiazepine exposure were admitted to a critical care unit and 21.7% were admitted to a psychiatric facility. More than one-quarter resulted in a serious medical outcome (28.4%) (Table 1). Among cases resulting in serious medical outcomes, the substances most frequently used with benzodiazepines in polysubstance exposures included ethanol beverages (10.0%), atypical antipsychotics (8.1%), other types of selective serotonin reuptake inhibitors (4.7%), acetaminophen with hydrocodone (4.0%), and other types of sedative/hypnotic/anti-anxiety or anti-psychotic drugs (3.9%).
Clinical effects and therapies
Among the 146,999 single-substance cases, most resulted in drowsiness/lethargy (61.8%). Other observed clinical effects included slurred speech (9.6%) and tachycardia (5.1%) (Table 2). Among the therapies performed, the most common were intravenous fluids (38.8%) and charcoal (28.1%) (Table 3).
Selected related clinical effects among single-substance benzodiazepine exposures.

aOnly the number of cases with clinical effects which are “related” were considered in the denominator while calculating percentages.
bMultiple clinical effects for each exposure were included when applicable.
Selected performed therapies among single-substance benzodiazepine exposures.
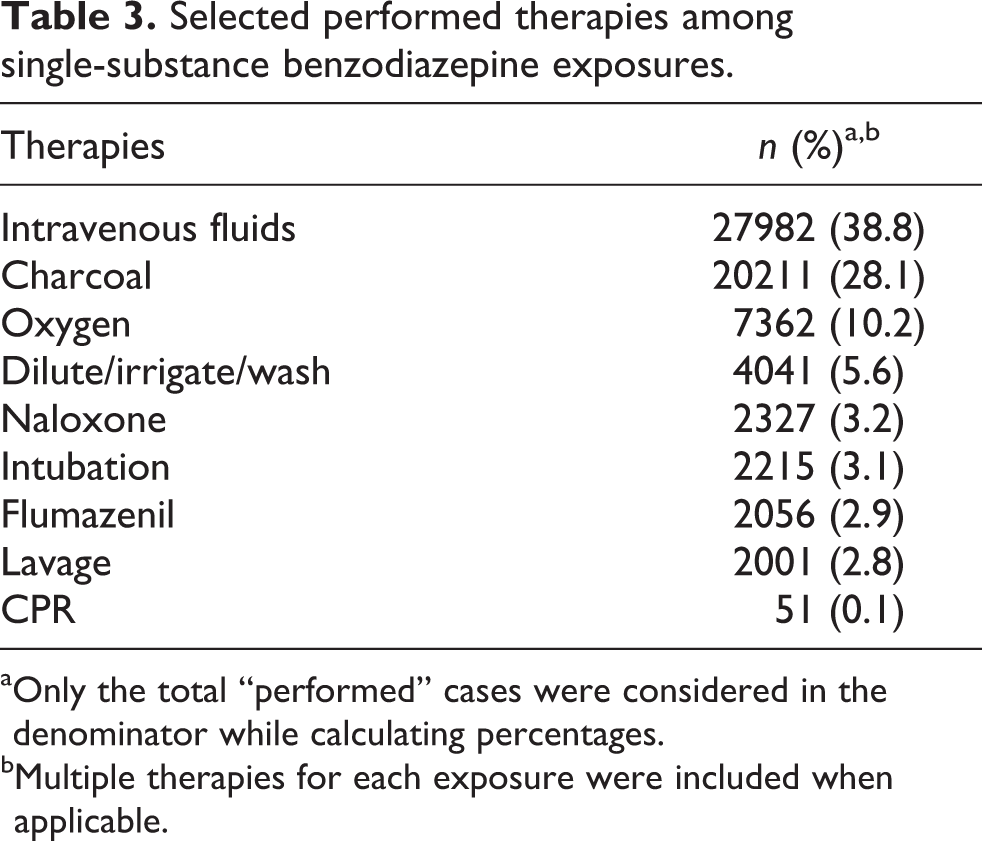
aOnly the total “performed” cases were considered in the denominator while calculating percentages.
bMultiple therapies for each exposure were included when applicable.
Exposure trends
From 2004 through 2018, the annual rate of single-substance benzodiazepine exposures among women in our study decreased significantly by 33.7% (m = −166.2; p = 0.001) and polysubstance exposures decreased by 5.5% (m = −13.2; p = 0.918) (Figure 1). However, when rates were examined by age group, differences were found. Among women 15–19 years, the annual rate of single-substance and polysubstance exposures increased significantly by 16.5% (m = 70.0; p < 0.001) from 2004 through 2018. In comparison, among women 20–29 years old, the annual rate of exposures increased by 20.2% (m = 458.6; p = 0.0021) from 2004 to 2010, then decreased by 47.3% (m = −389.4; p = <0.0001) from 2010 to 2018; among women 30 to 39 years old, the annual rate of exposures increased by 15.2% (m = 323.8; p = 0.0026) from 2004 to 2010, then decreased by 41.7% (m = −311.2; p = <0.0001) from 2010 to 2018; and among women 40 to 49 years old, the annual rate of exposures increased by 19.3% (m = 347.3; p = 0.0002) from 2004 to 2010, then decreased by 46.0% (m = −369.8; p = <0.0001) from 2010 to 2018 (Figure 1).

Annual rate of single-substance and polysubstance benzodiazepine exposure by age group among women 15–49 years of age.
Among women whose reason for exposure was “unintentional,” the annual rate of cases decreased significantly by 69.5% from 2004 through 2018 (m = −105.1; p < 0.001). In comparison, among cases coded as “intentional, suspected suicide,” the annual rate of cases increased by 19.9% from 2004 to 2010 (m = 979.5; p = 0.0011), then decreased by 31.3% from 2010 to 2018 (m = −569.5; p = 0.0003). Among cases coded as “intentional” (excluding suspected suicide), the annual rate of exposures decreased by 33.1% (m = −41.9; p = 0.124; Figure 2).
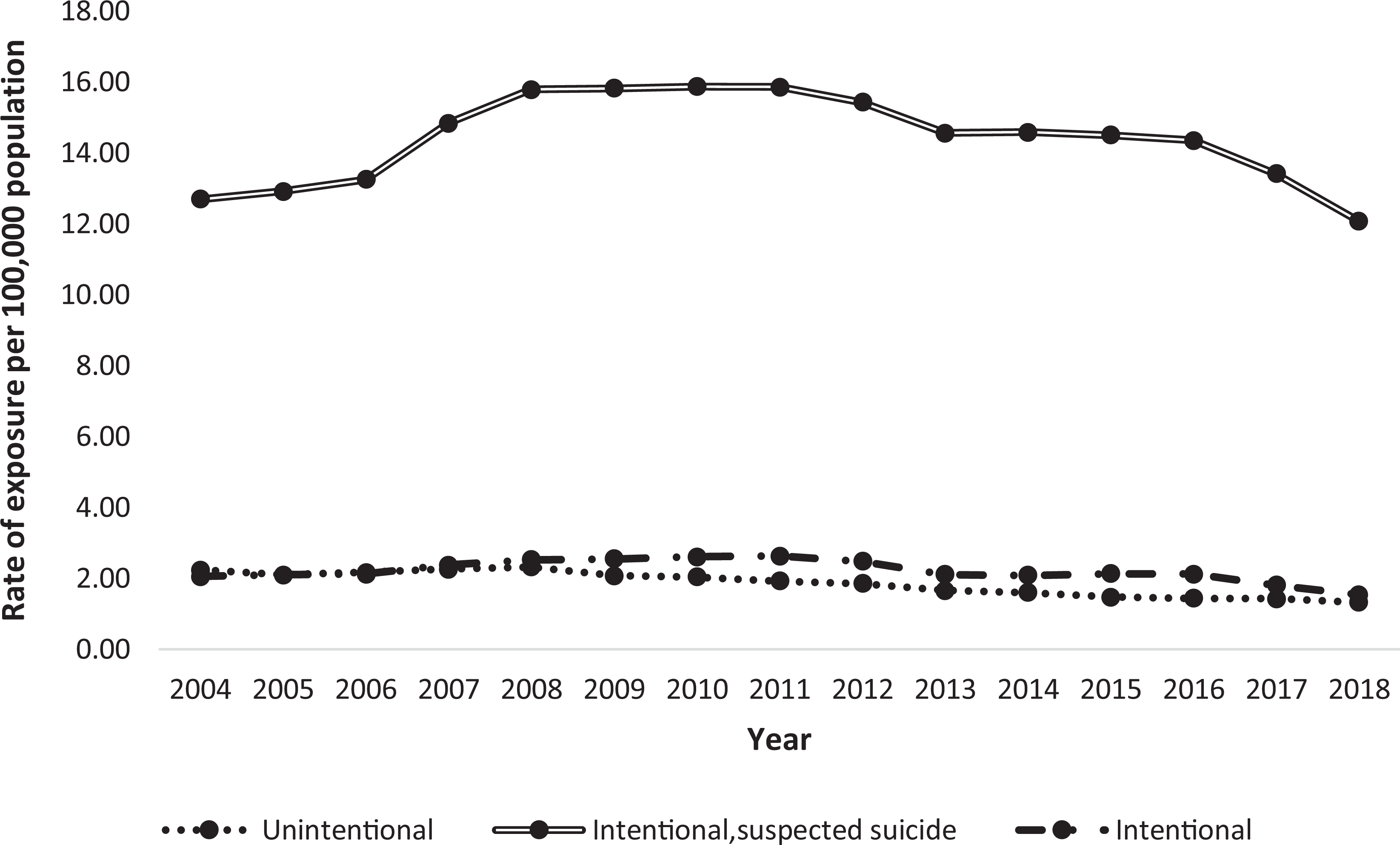
Annual rate of benzodiazepine exposure by “reasons for exposure” among women 15–49 years of age.
Discussion
During the 15-year study period, 2004–2018, there were 258,370 single-substance and first-ranked benzodiazepine exposures among US women 15–49 years old reported to the NPDS. One-fifth of all benzodiazepine cases resulted in a serious medical outcome and nearly one-half resulted in admission to a psychiatric facility, critical care unit, or non-critical care unit. Rates of single-substance benzodiazepine exposures decreased significantly among the study population, while polysubstance exposures decreased slightly. There were also differences in trends by age group, with cases increasing significantly among women 15–19 years old but decreasing non-significantly among older age groups. Prior research has also identified increases in the rate and severity of benzodiazepine cases among adolescents in the US, with a substantial proportion of exposures attributable to intentional causes, including abuse, misuse, and attempted suicide. 2 In the current study, the majority of all exposures were intentional and 73.2% were attributed to suspected suicide attempts or deaths. Suicide-related benzodiazepine exposure rates increased early in the study period and then decreased, for reasons that are unknown.
Benzodiazepines and suicidal behavior
Suicide is the 10th leading cause of death in the US across all ages, and rates of suicide deaths and attempted suicide have increased in recent years.50–54 Suicide rates among women increased 55% from 1999 to 2018. 55 Overall, intentional self-poisoning is the third most common mechanism used in suicide deaths. 50 Prior research has identified an association between benzodiazepine use and misuse with suicidal ideation and suicidal behaviors and benzodiazepines are one of the classes of drugs most frequently involved in suicidal acts.56–59 Drug selection may vary according to accessibility, however. A study of adolescent suicidal ingestions reported to the NPDS found that most ingestions involved over-the-counter medications, perhaps reflecting more limited access to prescription medications.60–62 However, our findings indicate that benzodiazepines are accessible to at least some adolescents with suicidal intent, although the source of the drugs cannot be determined.
Use of benzodiazepines and overdose prevention
Although there are risks associated with benzodiazepine use, untreated mental health conditions can also be harmful. Therefore, women and their healthcare providers should carefully consider the pros and cons of benzodiazepine use. Long-term benzodiazepine use is particularly high-risk and not uncommon.8,12 Among adult women who filled at least 1 benzodiazepine prescription in the past year, 14% of 18- to 35-year-olds and 22% of 36- to 50-year-olds were prescribed the drug for long-term use (≥120 days). 12
It is estimated that as much as 17% of benzodiazepine use in the US can be categorized as misuse. 4 Reasons for benzodiazepine misuse include to aid in relaxation, relieve tension, or help with sleep. 4 Individuals who take benzodiazepines without a prescription often receive the drugs from a friend or relative. 4 Healthcare providers should inquire about non-prescription/non-medical use of benzodiazepines as part of their screening procedures, as this could aid in substance misuse and suicide prevention efforts. Healthcare providers should also use their state’s prescription drug monitoring program, when available, to check for concomitant benzodiazepine and/or opioid prescription before prescribing either drug.
Potential strategies for reducing unnecessary benzodiazepine use and preventing overdoses include: expanding access to behavioral health services, including telehealth services; the implementation of unit-dose or “blister” packaging for all solid dosage forms of benzodiazepines and opioids sold to the public; and the distribution of naloxone, an opioid overdose reversal drug, to patients who are concurrently using benzodiazepines and opioids.63,64 In 2016, the US Food and Drug Administration began requiring “black box” warnings on prescription opioids, opioid-containing cough medications, and benzodiazepines warning of the serious risks associated with using these medications simultaneously. 27 However, greater awareness may be needed.1,11,20–22 For women who are dependent on benzodiazepines, it is important to consider the barriers women may face when seeking treatment for a substance use disorder, including stigma, employment concerns, caregiving responsibilities, and fears of losing custody of their children.65–70
Study limitations
NPDS data are obtained from voluntary reports to US PCCs by healthcare professionals and the public and are an underestimate of the true number of benzodiazepine exposures in the US. The NPDS does not collect personal identifiers; therefore, each reported exposure may not necessarily represent one unique individual. Reported exposures do not necessarily represent a poisoning or an overdose. Information gathered by PCCs is self-reported and may not be completely verifiable by PCCs or the AAPCC. However, PCCs adhere to strict quality control protocols, including the use of specially trained poison experts to respond to inquiries and record exposure data for the NPDS. We were unable to determine whether benzodiazepines were identified by history or were reported in a urine drug screen. Also, the sources of the benzodiazepines in this study are unknown; therefore, the proportion of exposures attributable to prescribed versus diverted medications (i.e., those not prescribed to the recipient by a medical provider), is unknown.
Conclusions
The majority of benzodiazepine cases among women of reproductive age that were reported to US PCCs during the study period were intentional, and nearly three-quarters were associated with suicide attempts or suicide deaths. A substantial proportion of cases resulted in serious medical outcomes and nearly one-half required admission to a health care facility for treatment. While reported benzodiazepine case rates increased early in the study period, they decreased beginning in 2010 among most age groups, for reasons that are unclear. It is notable that benzodiazepine exposures rates among 15- to 19-year-olds demonstrated a unique trend, showing an overall increase over the study period. Our findings support prior research linking benzodiazepines and suicidal acts and highlight the need for increased prevention efforts to address benzodiazepine use in the context of suicidal behavior among women of reproductive age.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.