
Abstract
Introduction:
Clozapine is a frequently prescribed atypical antipsychotic drug. Various case reports documented the successful recovery of acute antipsychotics toxicity in association with the administration of intralipid emulsion (ILE).
Aim:
This study aimed to assess the adjuvant therapeutic role of SMOF Lipid administration on the outcomes of acute clozapine poisoning.
Methods:
Forty patients with acute clozapine poisoning were randomly allocated into two equal groups. The control group received the standard supportive treatment only, whereas the intervention group received the standard supportive treatment plus SMOF Lipid 20% infusion. All patients were subjected to history taking, full clinical examination, and laboratory investigations. The study outcomes were evaluated.
Results:
The mean Glasgow Coma Scale (GCS) at 6 hours (13.1 ± 2.3 vs 9.2 ± 2, p < 0.001) and 12 hours (14.3 ± 1.5 vs 9.6 ± 2, p < 0.001) after admission was significantly higher in the intervention group compared to the control group. The intervention group showed a significantly lower frequency of prolonged QTc interval 12 hours after admission (p = 0.003), as well as a significantly shorter hospital stay (p < 0.001).
Conclusions:
SMOF Lipid infusion seemed to have improved GCS, the prolonged QTc interval, and shortened the length of hospital stay. Furthermore, there were no adverse effects related to its administration.
Introduction
Antipsychotics are a group of drugs that are mainly used to treat schizophrenia and a broad range of disorders; including bipolar mania and depression. 1 Clozapine is an atypical antipsychotic drug that is commonly prescribed because of the lower incidence of extrapyramidal symptoms such as tardive dyskinesia, and its efficacy in treating negative symptoms of schizophrenia. 2
Recently, the American Association of Poison Control Centers (AAPCC) ranked sedatives/hypnotics/antipsychotics class as one of the most frequent five xenobiotics involved in human exposure. Moreover, AAPCC reported a rapid increase in the incidence of these drug exposure over the previous 18 years. 3 In Egypt, recent studies from Tanta University Poison Control Centre (TUPCC) and the National Poisoning Center, Cairo have explored acute clozapine poisoning as a frequent category among central nervous system pharmaceutical drug poisonings. 4,5
Clozapine toxicity produces manifestations that affect multiple organ systems. Serious toxicity mainly affects the central nervous system (CNS) and the cardiovascular system (CVS). The most frequently reported manifestations are pronounced sedation, confusion, delirium, tachycardia, mild hypotension, and prolongation of the corrected QT (QTc) interval which is associated with increased risk of torsade de pointes and sudden death. Rarely, grand mal seizures and myocarditis might occur. 6,7 In absence of a specific antidote, the current recommendation from toxicology and poisons information centers for many antipsychotic drugs poisoning is supportive therapy dictated by the patient’s clinical status. 6
Intravenous lipid emulsion (ILE) is used as a source of calories and essential fatty acids in patients who require parenteral nutrition. 8 Various case reports documented the recovery of acute antipsychotics toxicity in association with the administration of ILE. 9 –12 Moreover, Yousefsani et al. 13 have demonstrated the successful use of ILE for the treatment of acute clozapine-induced ataxia as well as seizures in rats. Nevertheless, there are no reported clinical trials on humans to recommend its therapeutic use. Therefore, the objective of this study was to assess the adjuvant therapeutic role of SMOF Lipid administration on the outcomes of acute clozapine poisoning.
Patients and methods
Study design, settings, and ethical considerations
This phase II randomized controlled single-blinded, parallel-group clinical trial was conducted in Tanta University Poison Control Center (TUPCC), Tanta University Emergency Hospital, Egypt from December 2019 to the end of May 2020.
The present study was carried out according to the World Medical Association Declaration of Helsinki, after approval of the research ethics committee, Faculty of Medicine, Tanta University, Egypt (approval number: 32944/02/19) and approved registration on the Pan African Clinical Trial Registry (trial identification number: PACTR201911916675189). Written informed consent was obtained from each patient or his/her guardians (if the patient was unable to participate in the consent process) after receiving detailed information about the study. Confidentiality of data was maintained by making a code number for each patient and data were analyzed anonymously.
Sample size
Priori sample size calculation was carried out by using G power 3.1.9.4 software program, depending on the primary outcome; improvement of consciousness level measured by the Glasgow Coma Scale (GCS). According to the following assumptions; an effect size equals 0.95 which was calculated according to Taftachi et al. 14 , alpha error 5%, power of 80%, allocation ratio = 1, the total required sample size was 40 patients.
Patients’ selection criteria
Inclusion criteria: Male or female symptomatic patients of any age, with moderate to severe acute clozapine poisoning. The severity of CNS, CVS, and respiratory manifestations as well as any metabolic disturbances were assessed on admission according to the standardized Poisoning Severity Score (PSS). 15
Exclusion criteria: Patients reported coingestion of other substances in addition to clozapine, presented more than 12 hr after clozapine ingestion or received any treatment before admission to TUPCC, pregnant and lactating women, patients with major medical conditions (e.g. diabetes mellitus, cardiovascular disease, renal or hepatic failure), as well as patients with a known history of hyperlipidemia were excluded.
The diagnosis was based on history taking either from the patient himself or the relatives, reliable identification of the compound based on the container brought by patients’ attendants, and the presence of the suggestive CNS and CVS manifestations. Additionally, serum clozapine concentration was obtained on admission to confirm the diagnosis. 6
Methods
Forty patients were randomly assigned into two equal groups (20 patients each, allocation ratio:1:1) by using a random number generator website. To conceal the allocation sequence, we used the sequentially numbered, opaque sealed envelopes method stated by Doig and Simpson. 16
Group I (control group) received the standard supportive care, while group II (intervention group) received the standard supportive care plus SMOF Lipid infusion. The standard supportive care comprised of maintaining patent airways, oxygen administration, breathing support when necessary, treatment of hypotension by intravenous fluids, continuous cardiac monitoring until resolving of all symptoms as well as ECG abnormalities. Additionally, all patients in both groups administered a single dose activated charcoal (1 gm/kg) for gastric decontamination. When the patient had disturbed consciousness level and absent gag reflex, activated charcoal administration was preceded by cuffed endotracheal intubation to secure the airways and minimizing aspiration pnemonia. 17
Patients in group II received the standard supportive care and gastric decontamination measures as described in group I plus intravenous lipid emulsion (SMOF Lipid® 20%; a mixture of soybean oil, medium-chain triglycerides, olive- and fish-oil). According to Purg et al. 11 , SMOF Lipid was administrated as an initial bolus dose: 1.5 mL/kg over 1 to 2 minutes, followed by a maintenance dose (6 mL/kg) IV infusion over 1 hour. After the infusion was completed, the patient was continuously reassessed and the bolus dose might be repeated when necessary. For pediatric patients, the regimen of ILE was similar to the adult’s recommendations. 18 During SMOF Lipid administration and the hospital stay period, patients in group II were closely monitored to detect any adverse effects.
For all patients, sociodemographic, toxicological data, and time elapsed before hospital admission were collected. Full clinical examination including monitoring of vital signs and assessment of consciousness level by GCS. For children below 2-years, the modified pediatric GCS was applied. This was performed by a single person who was one of the researchers with great experience in managing acute poisoning cases in the emergency room.
A twelve-leads ECG was recorded on admission and repeated when an abnormality was observed on cardiac monitoring, as well as 12 hr after admission. Electrocardiograms were assessed by the same cardiology consultant who was blinded to the study hypothesis and the clinical status of patients. They were analyzed for rate, rhythm, axis, and the presence of any conduction defects or dysrhythmias. The corrected QT interval (QTc) was calculated according to Bazett’s formula; QTc = QT/vRR. Prolonged QTc is defined as more than 0.45 sec in males and more than 0.47 sec in females. 19,20 Vital signs were assessed in adults according to reference ranges. 21 In children (aged 12 years or younger), the normal range of temperature is 36.6°–37.9°C, rectally, 22 while the normal ranges of blood pressure, pulse, and respiratory rate of children were determined according to Hartman and Cheifetz. 23
Blood samples were obtained from each patient immediately on admission and before giving any medications, for measuring serum clozapine concentrations and baseline routine laboratory investigations; these included serum concentrations of triglycerides, sodium and potassium, alanine aminotransferase (ALT), aspartate aminotransferase (AST), creatinine, random blood sugar, as well as blood urea and arterial blood gases. Measurement of serum clozapine concentrations was done by Young Lin© (YL-9100) high-performance liquid chromatography (HPLC) system at Ain Shams Poison Control Center, Cairo, Egypt. Twelve hours after admission, another blood sample was withdrawn for the reevaluation of serum concentrations of triglyceride, AST, ALT, and platelet count as recommended by Spray. 24
Patients in both groups were prospectively monitored for consciousness levels, vital signs, ECG, and the development of any complications or idiosyncratic reactions until discharge from the Emergency Hospital. Patients with suicide attempts and/or psychiatric comorbidity were referred for psychiatric rehabilitation.
Outcome measures
The primary outcome was the improvement in consciousness levels measured by GCS, whereas secondary outcomes included; the need for intensive care unit (ICU) admission and/or mechanical ventilation, improvement in QTc interval, the duration of hospital stay started from the time of admission until discharge from the Emergency hospital, in addition to the total in-hospital mortality.
Statistical analysis
All data were tabulated and statistically analyzed by using SPSS program, version 22. All continuous variables were checked for normality by the Shapiro Wilk test. For normally distributed data, they were presented as mean ± SD, and differences between the studied groups were verified using Independent T-test. Alternatively, data that showed abnormal distribution were displayed as the median and interquartile range (25th–75th percentile) and were compared by using the Mann-Whitney U test. Categorical variables were summarized as frequencies and percentages and association between variables was tested using X 2 tests (Pearson’s Chi-Square for independence or Fisher’s Exact Tests as appropriate). Additionally, a Paired T-test was used to compare serum triglyceride concentration, platelet count, and liver enzymes assessed on admission and 12 h later. For significant outcomes, the effect size was calculated according to Cohen’s d for continuous outcomes, as well as relative risk for binary ones. A p-value of < 0.05 was considered statistically significant.
Results
In the present study, 68 patients reported toxic ingestion of clozapine were assessed for eligibility. Twenty-eight were excluded; 16 presented with mild poisoning, seven reported multiple drug ingestions, three provided a history of hyperlipidemia on admission, and two refused to participate in the study. After fulfilling the inclusion criteria, 40 patients with acute clozapine poisoning were randomly allocated into two groups (Figure 1).

CONSORT 2010 flow chart.
There were no significant differences between the studied groups regarding the patient’s demographics and toxicological data (Table 1).
Baseline demographics and toxicological data of the studied groups.
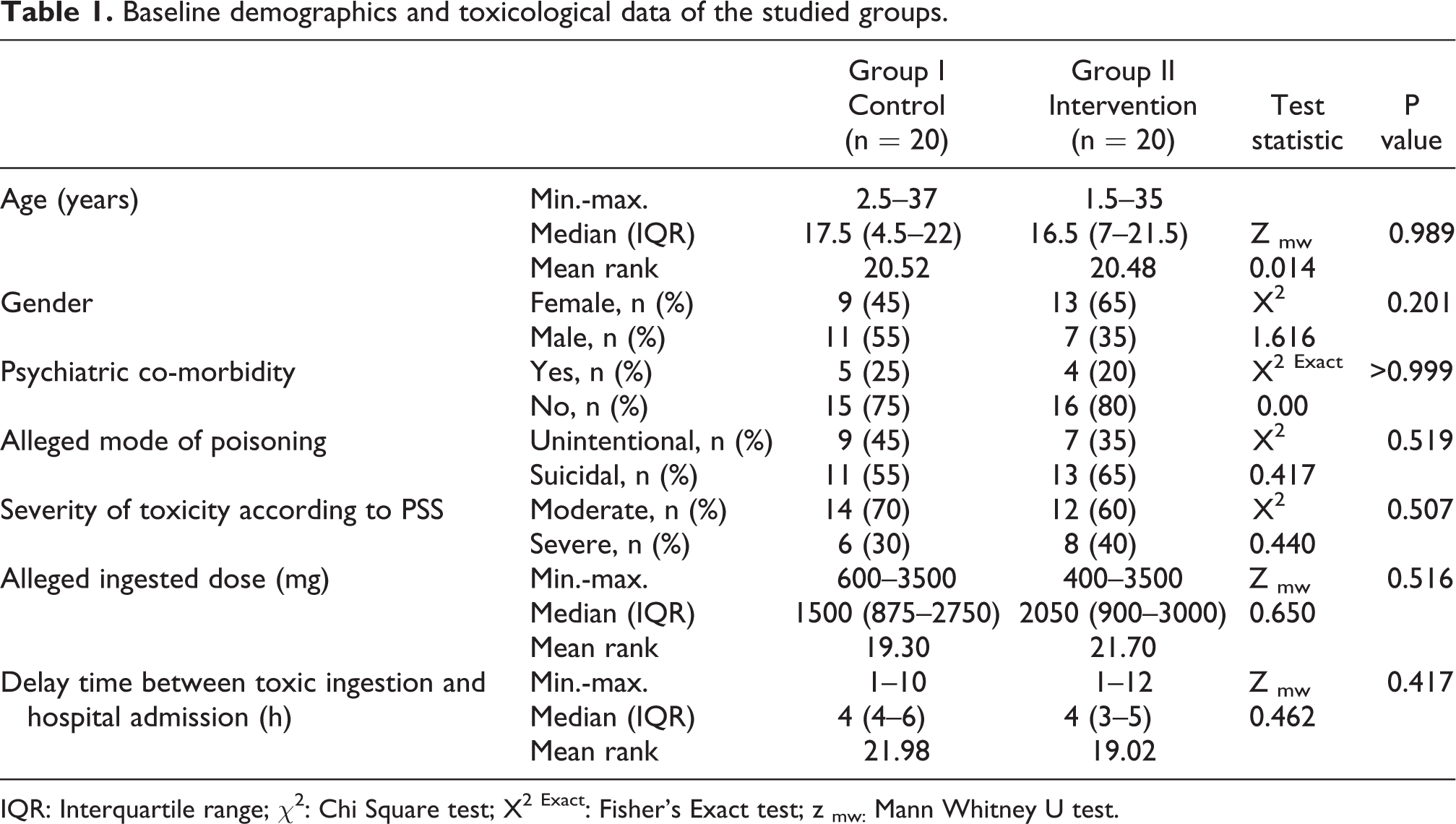
IQR: Interquartile range; χ2: Chi Square test; X2 Exact: Fisher’s Exact test; z mw: Mann Whitney U test.
Table 2 shows the absence of significant differences between both groups regarding their baseline vital data and clinical manifestations (p > 0.05). The mean GCS on admission was 8.5 ± 2.2 and 8.8 ± 2 in the control and intervention groups respectively. Baseline ECG revealed sinus tachycardia (60% vs 70%) and prolonged QTc interval (45% vs 65%) in both groups. Figures 2 and 3 illustrate abnormal ECG findings.
Baseline vital data and clinical findings of the studied groups.

SD: Standard deviation; χ2: Chi Square test; t: Independent T test.

An ECG of a female patient aged 27 years with acute clozapine poisoning shows sinus tachycardia.

An ECG of a male patient aged 22 years with acute clozapine poisoning shows combined sinus tachycardia and prolonged QTc interval. Black arrow points to the prolonged QTC interval.
There were no significant differences between the two studied groups regarding baseline routine laboratory investigations (p > 0.05). In all the included patients, clozapine was detected analytically. The mean serum clozapine concentration was 2.258 ± 1.35 in group 1 compared to 2.308 ± 1.42 mg/ml in group 2, with no significant differences (p = 0.910) (Table 3).
Baseline laboratory investigations obtained on admission in the studied groups.

SD: Standard deviation; t: Independent T test; AST; aspartate aminotransferase ALT; alanine aminotransferase.
Table 4 illustrates the outcomes of the present study. The mean GCS assessed at 6 hours (13.1 ± 2.3 vs 9.2 ± 2, p < 0.001) and at 12 hours (14.3 ± 1.5 vs 9.6 ± 2, p < 0,001) after admission was significantly higher in the intervention group compared to the control group. Additionally, the frequency of fully conscious (GCS = 15) patients was significantly higher in the intervention group than the control group both at 6 and 12 hours after admission. The corrected QT interval was assessed 12 hours after admission, the frequency of prolonged QTc interval was 45% in the control group compared to 5% in the intervention group (p = 0.003).
Comparison of outcomes of the studied groups.

*Significant at p < 0.05; SD: Standard deviation; IQR: Interquartile range; Z mw : Mann Whitney U test; t: Independent T test; χ2: Chi Square test.
Furthermore, patients in the intervention group showed a significantly shorter period of hospital stay compared to those in the control group (median = 18 h versus 71 h respectively, p < 0.001). Four patients (20%) in the control group required ICU admission compared to 1 (5%) patient in the intervention group, with no significant differences (p = 0.339) (Table 4). After complete recovery, all patients were discharged from the hospital with no recorded in-hospital mortality in either group.
All patients in group II received the initial bolus dose of SMOF Lipid, followed by the maintenance dose, with no additional bolus doses were required. According to their weights, the total amount of received SMOF Lipid ranged from 75 to 750 ml, with a median amount of 337.5 ml (IQR = 140–537.5 ml).
No major adverse effects e.g. allergic reactions to SMOF Lipid therapy were recorded during clinical monitoring of patients. Table 5 shows no significant differences between serum triglycerides levels, platelet count, and liver enzymes obtained on admission and 12 hours later during follow up of the interventional group (p > 0.05).
Comparison of serum triglyceride levels, platelets count, and liver enzymes obtained on admission and 12 h later in intervention group.

SD: Standard deviation; AST; aspartate aminotransferase ALT; alanine aminotransferase.
Discussion
There is an increasing concern for using ILE therapy in the management of lipophilic drug poisoning. Though, the contemporarily available evidence regarding the setting of non-local anesthetic drugs is insufficient and depending mainly on case reports and animal studies. 25 Hence, there is a need for randomized controlled trials for evaluating the efficacy, safety, indications, and the best regimen for ILE therapy. 26 In light of this knowledge gap, our study was designed to assess the adjuvant therapeutic role of SMOF Lipid administration on the outcomes of acute clozapine poisoning.
The present study explored important findings regarding the therapeutic efficacy of SMOF Lipid in clozapine toxicity. Administration of SMOF Lipid was significantly effective in improving the consciousness level as well as the prolonged QTc interval more rapidly. Additionally, the rapid recovery of patients who received SMOF Lipid was associated with a shorter period of hospital stay compared to their controls. Moreover, no adverse effects related to SMOF Lipid administration have been detected. These findings support the feasibility of SMOF Lipid in the setting of acute poisoning.
In the present study, all patients presented with depressed consciousness. In agreement with this finding, it has been reported that impaired consciousness is a common manifestation of acute antipsychotic poisoning that ranging from just sedation to frank coma. 27 As well, a high frequency of CNS depression has been documented in a retrospective analysis of patients with acute clozapine poisoning. 28 Furthermore, a progressive deterioration of consciousness with a drop of GCS from 12 to 7 has been reported in cases of clozapine intoxication. 29 Likewise, a prolonged coma for about 70 hours has been reported as the main manifestation in a patient who presented with intentional clozapine intoxication. 30 Altered consciousness is mainly due to clozapine-induced inhibition of central histamine H1receptors as well as muscarinic receptors including M1, M2, M3, and M5. 31
In the current study, assessment of GCS at 6 and 12 hours after admission revealed significantly faster regaining of consciousness in patients who administered SMOF Lipid compared to their controls. This coincides with Yousefsani et al. 13 who demonstrated a significant response of clozapine-induced neurotoxicity in rats to IV infusion of 18.6 mg/kg ILE 20% 15 minutes after receiving a toxic dose of clozapine. Responses to lipid emulsion were presented as a significant termination of ataxia and a more rapid decrease in seizure scores. Likewise, there was a successful restoration of haloperidol neurotoxicity after administration of different doses (6, 12, and 18 mL/kg) of ILE 20% in rabbits. 32 Furthermore, intervention with IV ILE 10% at a dose of 10 cc/kg was significantly effective in improving GCS 6 hours after admission in heterogonous types of acute non-local anesthetic drug poisoning. 14
Concerning baseline ECG changes, both sinus tachycardia and prolonged QTc interval were detected. This finding is in agreement with previous retrospective reports. 6,28,33,34 Moreover, a high frequency of prolonged QTc interval in atypical antipsychotics poisoning has been observed in a recent prospective analysis of patients admitted with acute antipsychotics poisoning. 4 Prolongation of QTc interval is a life-threatening complication of various atypical antipsychotics overdose. It may induce lethal arrhythmia including torsade de pointes and ventricular fibrillation. 7 However, factors that enable or attenuate the progression of QTc prolongation to torsade de pointes are still unclear and necessitate further research 35
Antipsychotic drugs including clozapine block voltage-gated potassium channels resulting in longer ventricular repolarization and consequently the QT interval. 36 Furthermore, clozapine intake has been associated with the development of potentially fatal myocarditis in previously healthy subjects. 37 Additionally, antagonism of alpha-adrenergic and muscarinic receptors by clozapine contribute to the frequently noticed tachycardia. 33
In this study, the administration of SMOF Lipid was associated with a decreased frequency of prolonged QTc interval at 12 hours after admission. A previous observational study reported a significant association between the prolonged QTc interval and the need for ICU admission and the increased rate of in-hospital mortality. 38 Hence, the observed impact of SMOF Lipid on the prolonged QTc interval might favor the rapid and uncomplicated recovery of these patients. Previous animal studies revealed the therapeutic role of ILE in restoring the mean arterial blood pressure and the wide QRS duration induced by combined amitriptyline and citalopram antidepressants in adult rats, 39 as well as correcting hypotension in clozapine intoxicated rats. 13
The most putative mechanism of ILE is the “lipid sink” theory. It suggests that intravascular lipid leads to redistribution of lipophilic drugs from the target tissues to the bloodstream down a concentration gradient. This reduces the volume of distribution of the lipophilic drugs. 40 According to this theory, responses to ILE depend likely on the drug lipophilicity and the pharmacokinetic phase at the time of ILE administration. Therefore, highly lipophilic drugs and ILE administration after peak absorption dictates favorable reversal of toxic effects. 41,42 In this regard, clozapine is known to be a highly lipid soluble drug with a peak absorption and plasma concentration reached around 3 hours, as well as a considerable volume of distribution (1.6–7.3 L/kg). 43 These made ILE suitable for the treatment of clozapine intoxication. However, there is wide interindividual variability in these pharmacokinetic parameters. 44
The “lipid sink” effect of ILE has been argued as a sole mechanism of action. 41 Further direct actions of ILE have been emerged, adding the pharmacodynamic components to ILE actions. It has been suggested that ILE increases myocardial energy substrate, thereby improving cardiac function. 45 Furthermore, the high concentration of long-chain fatty acids directly increases cardiomyocyte calcium concentration with a positive inotropic effect. 46 At the molecular level, activation of free fatty acid G protein coupled receptor-40 in cardiac muscles has recently been discovered. 47 Comparable direct actions of ILE on the nerve cells, with increased intraneuronal calcium concentration, have also been demonstrated. 32
Another important impact of SMOF Lipid use in this work was a significant shortening of the hospital stay. This might be attributed to its role in the rapid regaining of consciousness. We observed a lower incidence of aspiration pneumonia and the need for ICU admission in patients who received SMOF Lipid. Despite it was a non-significant association, it is a clinically important finding that might be more pronounced in future research including a larger sample size. Supporting evidence has been reported by Mubarak et al. 4 who found a significant association between GCS and the duration of hospital stay. Moreover, they demonstrated a low GCS as a predictor of the prolonged hospital stay. Indeed, shorter hospital stay saves costs, staff, and bed capacity.
In the present study, all patients survived with no recorded deaths in either group. This might be linked to the absence of fatal ventricular dysrhythmias in these patients. This coincides with Brett et al. 48 who reported less likelihood of case fatalities per overdose for most acute antipsychotics poisoning, particularly the atypical ones.
Careful attention to the potential adverse effects of SMOF Lipid was considered in this study. Clinical as well as laboratory monitoring of serum triglycerides, liver enzymes, and platelet count in patients who received SMOF Lipid revealed the absence of adverse effects. Thus, the applied SMOF Lipid regimen was well-tolerated and safe. A comparable safety study of lipid emulsion 20% in acute organophosphate poisoning revealed supporting evidence. 49 Results obtained from an online lipid registry of ILE use in the treatment of drug toxicity revealed a favorable safety profile. Out of 48 recorded cases, only one serious (bronchospasm) and two minor (hyperamylasaemia and lipemia) complications have been reported. 50
It has been postulated that the infusion rate and the total dose are predetermining factors of adverse effects. Adherence to a maximum infusion rate of 0.55 ml/kg/min and a total daily dose of 10 ml/kg make adverse effects rare occurrence. 51
Limitations
Despite being a randomized controlled trial that helps to provide high-quality evidence, it is limited by being single-blinded with a risk of bias. Additionally, the small sample size and being a single center study made stratification of patients according to severity inapplicable. As well, monitoring of serum clozapine concentrations after SMOF Lipid administration to show any measurable effects of SMOF Lipid in this regard could not be performed. The results are specific to the investigated SMOF Lipid, they may not be applicable if a different lipid is used.
Conclusion
Intravenous SMOF Lipid may be used as an adjuvant therapy to the standard supportive care in patients with moderate to severe acute clozapine poisoning. The administration of SMOF Lipid was associated with a significant rapid recovery of disturbed consciousness, the prolonged QTc interval and a shorter duration of hospital stay with no adverse effects. These promising responses encourage reasonable consideration of SMOF Lipid as a new treatment modality. However, further multicenter studies on larger numbers of patients are necessary, so that solid conclusion about SMOF Lipid efficacy can be elucidated.
Footnotes
Acknowledgement
The authors are greatly thankful to all patients included in the current study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Trial registration
Pan African Clinical Trial Registry (PACTR): PACTR201911916675189.