
Abstract
Introduction:
There is a paucity of literature analyzing outcome of chlorpyrifos intoxication.
Methods:
A total of 40 patients with chlorpyrifos intoxication were seen at Chang Gung Memorial Hospital between 2008 and 2017. Patients were stratified into two subgroups according to their prognosis, as good (n = 12) or poor (n = 28). Good prognosis group were defined as patients who survived without serious complications, and poor prognosis group included patients who died and survived after development of severe complications. Demographic, clinical, laboratory, and mortality data were obtained for analysis.
Results:
Patients aged 53.8 ± 16.3 years and most were male (80.0%). All patients (100.0%) developed acute cholinergic crisis such as emesis (45.0%), respiratory failure (42.5%), tachycardia (30.0%), kidney injury (22.5%), and seizure (7.5%). Intermediate syndrome developed in 12.5% of patients, but none had delayed neuropathy (0%). The poor prognosis group suffered higher incidences of respiratory failure (p = 0.011), kidney injury (p = 0.026), and prolonged corrected QT interval (p = 0.000), and they had higher blood urea nitrogen level (p = 0.041), lower Glasgow coma scale score (p = 0.011), and lower monocyte count (p = 0.023) than good prognosis group. All patients were treated with atropine and pralidoxime therapy, but six patients (15.0%) still died of intoxication. In a multivariate logistic regression model, blood urea nitrogen was a significant risk factor for poor prognosis (odds ratio: 1.375, 95% confidence interval: 1.001–1.889, p = 0.049). Nevertheless, no mortality risk factor could be identified.
Conclusion:
The mortality rate of patients with chlorpyrifos intoxication was 15.0%. Furthermore, acute cholinergic crisis, intermediate syndrome, and delayed neuropathy developed in 100.0%, 12.5%, and 0% of patients, respectively.
Keywords
Introduction
Chlorpyrifos is a widely used chlorinated organophosphorus pesticide that is commonly associated with intentional intoxication in many Asian countries. 1,2 Chlorpyrifos is a common name for the chemical 0,0-diethyl 0-(3,5,6-trichloro-2-pyridinyl)-phosphorothioate. After exposure, the liver cytochrome P450 enzyme metabolizes chlorpyrifos to chlorpyrifos-oxon by replacing sulfur group with oxygen. 3 Chlorpyrifos-oxon is primarily eliminated by kidney to 3,5,6-trichloro-2-pyridinol, diethylphosphate, and diethylthiophosphate. 4,5 In a clinical study, Griffin et al. 5 reported an elimination half-life of urinary dialkylphosphates after chlorpyrifos ingestion was 15.5 h. On the other hand, Nolan et al. 4 reported that the elimination half-life of urinary 3,5,6-trichloro-2-pyridinol was 27 h following oral ingestion. Chlorpyrifos is not soluble in water but is soluble in many organic solvents. The addition of chlorine group increases the lipid solubility and half-life in the human body, producing prolonged suppression of body cholinesterase levels after intoxication. 2
As other organophosphorus pesticide, the clinical courses of chlorpyrifos intoxication include acute cholinergic crisis following cholinesterase depression, intermediate syndrome with unclear mechanism, and delayed polyneuropathy caused by the suppression of neuropathy target esterase. 6
According to the toxicity classification of World Health Organization, chlorpyrifos is a moderately hazardous pesticide. It is also considered as one of the major environmental pollutants in Japan. 7 In an Agricultural Health Study involving 55,071 pesticide applicators, 8 1851 deaths (588 chlorpyrifos users) were detected. The relative risk of mortality from all causes in the chlorpyrifos applicators was slightly lower than that of the unexposed applicators. However, the relative risks of mortality from suicide and non-motor vehicle accidents had doubled in the highest category of chlorpyrifos exposure days. The published mortality rates of chlorpyrifos intoxication ranged from 4.42% to 8.0%. 9 –11 Nevertheless, these studies were on many different types of organophosphorus pesticides, lacking a detailed spectrum and clinical course of chlorpyrifos intoxication.
Therefore, the objective of this study was to examine the clinical course, laboratory tests, and outcomes of chlorpyrifos intoxication and to attempt to determine what association, if any, might exist between these findings.
Materials and methods
Ethical statement
This retrospective cohort study complied with the guidelines of the Declaration of Helsinki and was approved by the Medical Ethics Committee of Chang Gung Memorial Hospital, Taiwan. Since this study included retrospective evaluation of existing data, the Institutional Review Board approval (No. 201800245B0) was acquired, but without specific informed consent from the patients. All individual data were protected (by delinking identifying information from the main data set) and were accessible to researchers only. The Institutional Review Board of Chang Gung Memorial Hospital waived the need for consent as all data were analyzed anonymously. Lastly, all primary data were collected according to strengthening the reporting of observational studies in epidemiology guidelines.
Patients
Between 2008 and 2017, a total of 40 patients with chlorpyrifos intoxication were seen at Chang Gung Memorial Hospital, Linkou, Taiwan. Of the 40 patients, 39 were adults and there was only one 5-year-old child. All pesticide exposures were oral, and none of the patients had co-ingestion. Demographic, clinical, and laboratory data were obtained. Treatment modalities and mortality data were also collected. Notably, the quantities of ingested pesticide were very inaccurate and always subjected to recall bias. Some patients ingested chlorpyrifos directly, whereas many patients choose to ingest beverages that mixed with chlorpyrifos. The laboratory data were collected at admission.
Patients’ group
Patients were stratified into two subgroups according to their prognosis. Good prognosis group were defined as patients who survived without serious complications, and poor prognosis group included patients who died and survived after development of severe complications such as acute kidney injury, seizures, prolonged corrected QT, intermediate syndrome, and respiratory failure.
Diagnosis of chlorpyrifos intoxication
The diagnosis was based on the clinical history of chlorpyrifos exposure, clinical effects, physical examinations, and laboratory findings. Serum cholinesterase activity was determined using an enzymatic method (DF51, Siemens Healthcare Diagnostics, Newark, Delaware, USA). The normal values were 7–19 U/mL, and limit of quantification was 0.8 U/mL.
Clinical evaluation and management
Patients were treated with gastric lavage with 2 L of normal saline, followed by 1 g/kg activated charcoal and 250 mL of magnesium citrate infused via nasogastric tube. 1,6 Magnesium citrate was used to prevent constipation after charcoal therapy. Since all patients had depressed serum cholinesterase levels, they were treated with antidotes that included anticholinergic and oxime drugs. Intravenous atropine was initiated at 2 mg every 1–2 h and titrated to the resolution of bronchial secretions and bronchospasm. Pralidoxime therapy (1 g every 4 h, intravenous) was also prescribed to those patients with cholinergic crisis. The main indications for emergency hemodialysis were severe hyperkalemia (K ≥ 7 mmol/L), pulmonary edema, or severe metabolic acidosis (pH < 7.2 or base excess ≤ 10). On the other hand, the indications for endotracheal intubation were respiratory failure, consciousness disturbance, or hemodynamic instability. Since resource for intensive care unit was very limited, the indications for critical care admission were respiratory arrest, cardiac arrest, shock, severe consciousness disturbance, or epilepsy.
Inclusion and exclusion criteria
All patients who were diagnosed with chlorpyrifos intoxication at Chang Gung Memorial Hospital between 2008 and 2017 were eligible for inclusion in this study. Laboratory measurement of chlorpyrifos was not available at our hospital, but family members were asked to collect the pesticide container to confirm chlorpyrifos ingestion. Patients were excluded from this study if they did not have depressed serum cholinesterase levels despite suspicions of chlorpyrifos exposure. Furthermore, patients with co-ingestion were excluded from analysis.
Statistical analysis
Continuous variables are expressed as the mean and standard deviation and categorical variables as the number with percentage in brackets. For comparisons between patient groups, Student’s t-test was used for quantitative variables and χ 2 test for categorical variables. An initial univariate logistic regression analysis was performed to compare the frequency of possible risk factors associated with mortality or poor prognosis. To control for possible confounding factors, a multivariate logistic (backward stepwise approach) was performed to analyze factors that were significant in univariate models (p < 0.05). Results that rejected the null hypothesis with 95% confidence were considered significant. All analyses were performed using SPSS, version 12.0 for Windows (SPSS Inc., Chicago, Illinois, USA).
Results
Table 1 presents the baseline characteristics of 40 patients with chlorpyrifos intoxication, stratified into good (n = 12, 30.0%) and poor (n = 28, 70.0%) prognosis group. The patients aged 53.8 ± 16.3 years and most were male (80.0%). All intoxications were oral ingestion (100.0%) and patients arrived hospital at 2.4 ± 1.0 h. Their occupations were farmer (20.0%), non-farmer (20.0%), and unemployed (60.0%). It was found that poor prognosis group had higher medical history of hypertension than good prognosis group (p = 0.007). Otherwise, there were no significant differences in other baseline variables between both groups.
Baseline characteristics of 40 patients with chlorpyrifos intoxication, stratified into two subgroups according to their prognosis, as good or poor (n = 40).

a p < 0.01.
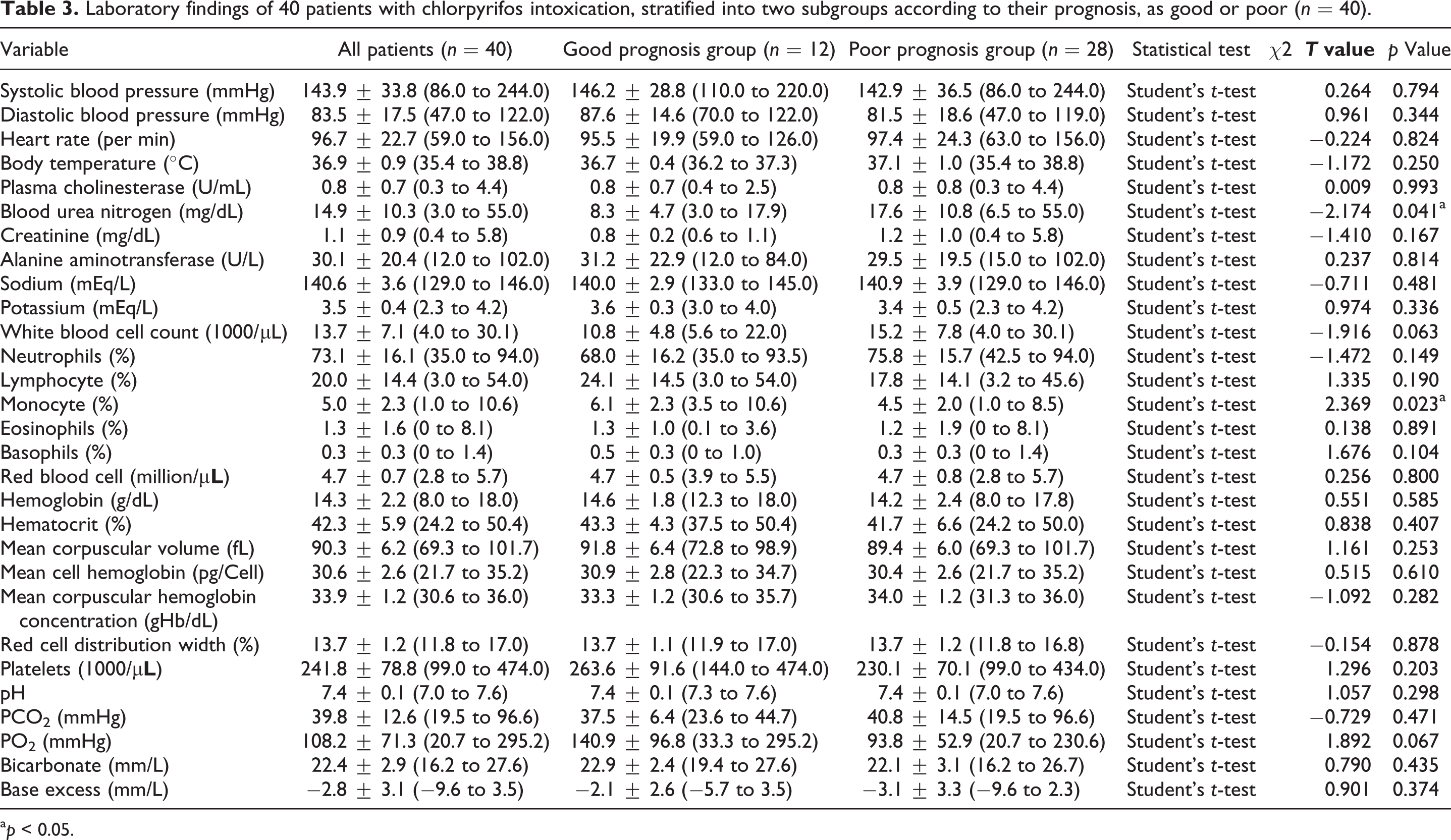
After ingestion, the patients developed acute cholinergic crisis (Table 2) such as emesis (45.0%), respiratory failure (42.5%), tachycardia (30.0%), acute kidney injury (22.5%), and seizure (7.5). Depressed serum cholinesterase and prolonged corrected QT interval were noted in 100.0% and 55.5% of patients, respectively. Intermediate syndrome developed in 12.5% of patients, but none of them had delayed neuropathy (0%). Furthermore, the poor prognosis group suffered higher incidences of acute respiratory failure (p = 0.011), acute kidney injury (p = 0.026), and prolonged corrected QT interval (p = 0.000) and had lower score of Glasgow coma scale (p = 0.011) than the good prognosis group. No significant differences in other clinical variables between the two groups. Laboratory analysis revealed that the poor prognosis group had higher blood level of urea nitrogen (p = 0.041) and lower monocyte count (p = 0.023) than good prognosis group (Table 3).
Clinical manifestations of 40 patients with chlorpyrifos intoxication, stratified into two subgroups according to their prognosis, as good or poor (n = 40).

a p < 0.05.
b p < 0.001.
Laboratory findings of 40 patients with chlorpyrifos intoxication, stratified into two subgroups according to their prognosis, as good or poor (n = 40).
a p < 0.05.
As presented in Table 4, all patients (100.0%) were intensively treated with systemic atropine and pralidoxime therapy. Nevertheless, six patients (15.0%) died despite intensive treatment. Furthermore, there were more intubations in the poor than good prognosis group (p = 0.011).
Treatments and outcomes of 40 patients with chlorpyrifos intoxication, stratified into two subgroups according to their prognosis, as good or poor (n = 40).

a p < 0.05.
In a multivariate logistic regression model (Table 5), it was revealed that blood urea nitrogen was a significant risk factor for poor prognosis after chlorpyrifos intoxication (odds ratio: 1.375, 95% confidence interval: 1.001–1.889, p = 0.049). Nevertheless, no mortality risk factor could be identified.
Prediction of poor prognosis and mortality using logistic regression analysis (n = 40).

a p < 0.05.
Discussion
The mortality rate of patients with chlorpyrifos intoxication was 15.0%. Furthermore, acute cholinergic crisis, intermediate syndrome, and delayed neuropathy developed in 100.0%, 12.5%, and 0% of patients, respectively.
There is a paucity of literature that explores the spectrum and clinical course of chlorpyrifos intoxication. In 1993, Aiuto et al. 12 reported a 3-year-old American child with life-threatening chlorpyrifos-induced delayed polyneuropathy with transient bilateral vocal cord paralysis. The recovery was slow after prolonged mechanical ventilatory support. Shahar and Andraws 13 reported a 17-year-old Israeli female with extrapyramidal parkinsonism and had a suicide attempt with chlorpyrifos. On admission, the patient was stuporous, with diarrhea and excessive drooling that caused respiratory failure and coma. Following treatments with atropine and toxogonin, she developed obvious extrapyramidal parkinsonism and encephalopathy. The patient was administered amantadine therapy and fully recovered. Guadarrama-Naveda et al. 14 described a Venezuela case of intermediate syndrome secondary to ingestion of chlorpyrifos.
Mattingly et al. 15 noted an unusual case of intermediate syndrome in an American toddler after chlorpyrifos ingestion, that is, the syndrome was still developing despite continuous oxime therapy. Meggs 16 reported an American case of permanent paralysis at sites of dermal exposure to chlorpyrifos during work and emphasized the importance of protective equipment. Pankaj and Krishna 17 described an Indian case of chlorpyrifos intoxication complicated by acute coronary syndrome. Lee and Lin 18 showed a case of intermediate syndrome after chlorpyrifos intoxication in a Taiwanese hemodialysis patient. The authors suggested that such sensitive patients suffering from chlorpyrifos intoxication are at a greater chance of having intermediate syndrome.
Solomon and Moodley 19 detected an African case of chlorpyrifos intoxication in the third trimester of pregnancy. The patient responded well to the parenteral atropine therapy. Although the mother survived, the infant was born prematurely and expired 2 days after birth. Notably, Lee et al. 20 disclosed a Taiwanese boy with recurrent chlorpyrifos intoxication due to deliberate chlorpyrifos poisoning by the stepmother. Rajasekaran et al. 21 presented an unusual Indian case of Guillain-Barré syndrome caused by organophosphate compound poison. Soummer et al. 22 stated a French case of subcutaneous chlorpyrifos self-injection, which resulted in delayed cholinergic manifestations, prolonged coma, and permanent neurologic injury, suggesting overlapping intermediate syndrome and distal peripheral neuropathy. The patient developed a considerable number of neuromuscular complications after 1 year. Rajasekharan et al. 23 reported an Indian case of opsoclonus and lingual myoclonus after chlorpyrifos intoxication. Moreover, Thivakaran et al. 24 demonstrated a case of chlorpyrifos-induced delayed myelopathy and pure motor neuropathy in a 15-year-old Sri Lanka female. Of note, the patient visited hospital 6 weeks after discharge with motor neuron signs of lower limbs without sensory loss. By the end of the seventh week, there was urinary incontinence. The patient suffered from progressive spasticity at 2-month follow-up. Finally, Cavari et al. 25 revealed an Israeli case of acute renal failure induced by chlorpyrifos intoxication. The patient was treated with continuous venovenous hemofiltration and the renal function was fully recovered.
In our study, acute cholinergic crisis occurred in all the cases (100%). However, five patients (12.5%) had intermediate syndrome and none (0%) developed delayed neuropathy. According to our analysis, three patients developed intermediate syndrome on the 2nd day after admission, one on the 7th day, and one on the 12th day. As mentioned, although all published cases (100%) developed acute cholinergic crisis following chlorpyrifos intoxication, only a certain proportion of patients developed intermediate syndrome or delayed neuropathy. The exact mechanism of intermediate syndrome is still unclear, 26 and it is presented in 20–50% of cases depending on the severity of intoxication and the type of organophosphorus pesticide. 27 One hypothesis is that the intermediate syndrome could be mediated by prolonged nicotinic receptor stimulation at the neuromuscular junction, and its onset is between 24 h and 96 h post pesticide ingestion. In a study, 28 it was demonstrated that prolonged jitter recorded with single fiber electromyography <24 h of ingestion of an organophosphate predicted the risk of subsequent intermediate syndrome.
The poor prognosis group had higher hypertension history than good prognosis group (p = 0.007, Table 1). In a laboratory study, Smith and Gordon 29 presented that spontaneously hypertensive rats exhibited a greater and more sustained elevation in blood pressure after chlorpyrifos treatment. Furthermore, the rise in blood pressure lasted for 56 h in spontaneously hypertensive rats compared to 32 h in Wistar Kyoto normotensive controls rats. Using the spontaneously hypertensive rats as a model to study human disease, it was suggested that hypertensive patients may be more sensitive to chlorpyrifos, as manifested by an exacerbated hypertensive response. Nevertheless, none of our chlorpyrifos patients suffered the exacerbated hypertension reaction after intoxication.
As given in Table 1, the nonoccupational exposure represented 80% of the entire cases, and most patients with chlorpyrifos intoxication were unemployed (60.0%). These data are compatible with our previous observation of patients with paraquat intoxication, 30 as 51.0% of the paraquat cases were unemployed. Chlorpyrifos is the most widely used insecticide in Taiwan. Farmers and their families often have easy access to chlorpyrifos in places of work and in their homes, and this increases their chances of exposure. The relationship between unemployment and suicide is not surprising. Unemployment is a vital variable in both suicide and attempted suicide, acts that are themselves woven from a complex tapestry of interacting factors. 31 In a meta-analysis study, Milner et al. 32 proved that long-term unemployment is associated with greater incidence of suicide. Moreover, the risk is highest in the first 5 years and continues at a lower but increased level up to 16 years after unemployment.
The poor prognosis group has lower monocyte count than good prognosis group (p = 0.023, Table 3). The mechanisms of hematological alterations produced by chlorpyrifos intoxication remain unclear. Previous works on the immunotoxicity of pesticides were mostly laboratory based and included mixture of pesticides or confounded by mild occupational exposure such as in retailers. In an in vitro study, Das et al. 33 reported that chlorpyrifos could induce apoptosis and necrosis in cultured human peripheral blood lymphocytes even at low cytotoxic doses. Furthermore, Ojha and Gupta 34 demonstrated significant dose- and time-dependent increases in lipid peroxidation, DNA interstrand cross-links formation, and increase of intracellular active caspase 3 and caspase 9 in cultured peripheral rat blood lymphocytes after chlorpyrifos treatment. In a mouse model of pesticide-induced hypoplastic/aplastic marrow failure, Chatterjee et al. 35 reported a moderate depression in the peripheral blood cell count at 30 days after treatment, and the depression was significantly increased up to 60th and 90th days of pesticide treatment. Pesticides used for the study were mixture of different compounds such as alphamethrin, cypermethrin, profenofos, and chloropyrofos. In a study of 102 patients with organophosphate poisoning, Kang et al. 36 demonstrated that levels of red cell distribution width that exceeded 13.5% were associated with increased mortality. In another study of 246 farmers, Hu et al. 37 found that pesticide application during the past 3 days produced adverse effects on many blood cells, such as monocytes, monocyte percentage, red blood cell, hemoglobin, hematocrit, mean corpuscular volume, mean corpuscular hemoglobin, mean corpuscular hemoglobin concentration, red cell distribution width coefficient of variation, platelet count, and platelet distribution width. The pesticides used were mostly pyrethroid and organophosphates. In another study of 70 pesticide retailers and 64 controls, Neghab et al. 38 noted that the mean values of monocyte, hemoglobin, hematocrit, mean corpuscular volume, mean corpuscular hemoglobin, and platelet distribution width were significantly lower, whereas mean corpuscular hemoglobin concentration and red blood cell distribution width were significantly higher in the retailers. Notably, organophosphates, pyrethroids, and carbamates were the there most common pesticides sold by the retailers.
In a logistic regression model, the Glasgow Coma Scale score (p = 0.010) and blood creatinine level (p = 0.023) variable were significant risk factors for mortality in univariate analysis but were no longer significant after multivariate analysis. In a study by Acikalin et al., 39 low Glasgow Coma Scale score was a poor prognostic factor for organophosphate intoxication. Sam et al. 40 also indicated a significant negative correlation between Glasgow Coma Scale score and mortality rate. In our previous study, 1 patients with organophosphate intoxication also revealed that hypotension (p = 0.000), respiratory failure (p = 0.042), coma (p = 0.023), and corrected QT interval prolongation (p = 0.002) were significant risk factors for mortality. In a nationwide population-based cohort study, 41 patients with highly severe organophosphate intoxication were associated with a substantially increased risk of acute kidney injury. The pathogenesis of renal damage by organophosphate remains unclear, but multiple different mechanisms such as oxidative stress, direct renal tubular damage, rhabdomyolysis, and hypovolemia due to dehydration are suggested. 42 In our study, none of the variables were found to be significant predictors for mortality after multivariate analysis, perhaps due to the small sample size.
Laboratory measurement of chlorpyrifos is not available for most hospitals. Our analytical results revealed that blood urea nitrogen carried a significant risk for poor prognosis (p = 0.049, Table 5). Therefore, clinicians should be aware of the possibility of chlorpyrifos intoxication by medical history checking. Furthermore, it is recommended to regularly follow-up blood urea level in these patients. The use of antidotes and other supportive measures could rapidly alter the clinical course of the disease and prevent the development of fatal complications. Finally, the limitations of this study included retrospective nature, small patient population, and a lack of electromyography study.
Conclusions
In summary, the data are important, because it is the only original report on patients with chlorpyrifos intoxication. The mortality rate was 15.0%. Acute cholinergic crisis, intermediate syndrome, and delayed neuropathy developed in 100.0%, 12.5% and 0% of patients, respectively.
Footnotes
Acknowledgment
The authors would like to thank the Center for Big Data Analytics and Statistics at Chang Gung Memorial Hospital for their support.
Author contributions
HFL involved in data collection and manuscript writing; SSC, CMC, and IKW carried out data analysis; CHK, HYY, CHW, WHH, CWH, and THY helped in patient care and management; THY performed study design and supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Chang Gung Memorial Hospital under research grants [CORPG3H0501, CORPG3H0491, and CLRPG3D0017].