
Abstract
Introduction:
Automatic dishwashing rinse aids are drying aids which contain non-ionic surfactants, usually ethoxylated alcohols, typically at concentrations of ≤30%.
Objective:
To assess the reported toxicity of rinse aids.
Methods:
Telephone enquiries to the UK National Poisons Information Service were analysed from January 2008 to June 2019.
Results:
Ingestion: Ingestion was involved in 976 cases and produced gastrointestinal features, coughing and central nervous system depression, particularly in young children. In those in whom the amount ingested was known, the majority (56%) of children <18 years and of adults (57%) ingested <50 mL of rinse aid. Although moderate or severe exposures (Poisoning Severity Score (PSS) ≥ 2) were uncommon, they occurred significantly (p < 0.0008) more often in adults (9.0%) than in children (1.8%); however, three of the four adults with PSS ≥ 2 co-ingested other substances. Eye exposure: Ocular exposure was reported in 35 cases, of whom 29 developed features. Eye irritation (n = 10, 28.6%) and eye pain (n = 10, 28.6%) were reported most commonly, and three patients (8.6%) developed corneal abrasions (PSS 2). Dermal exposure: Thirty-four patients were exposed dermally, and six (17.6%) reported features, including rash, numbness, pruritus and burns (PSS 1).
Conclusions:
Overall, clinical features developed in 47% of patients exposed to rinse aids, but more severe features (PSS ≥ 2) were rare (<3%) following exposure by any route.
Introduction
A recent survey has indicated that half of UK households have an automatic dishwashing machine. 1 Automatic dishwashing rinse aids are used in automatic dishwashing machines as drying aids. These products contain non-ionic surfactants at concentrations up to 100% by weight, although typically <30%. Most products contain ethoxylated alcohols as the non-ionic surfactant. Rinse aids act to reduce the surface tension of water so that water runs off crockery more easily and water droplet formation is less likely, thereby preventing ‘spotting’. Other constituents that may be present include citric acid (up to 5%) for lime scale removal, a caustic agent at low concentration (e.g. <0.01% sodium hydroxide) to hydrolyse fatty materials, sodium or potassium cumenesulfonate (often <5%) which helps to solubilize surfactants (to allow more concentrated formulations) and methylchloroisothiazolinone and/or methylisothiazolinone which act as preservatives and have antibacterial and antifungal properties. Most rinse aids are acidic with a pH of 2–3.
We have reported previously on the toxicity of rinse aids and have shown that the ingestion of dishwashing rinse aid only rarely produced features other than vomiting. 2 The relative lack of more severe symptoms was surprising given the potential toxicity of non-ionic surfactants and suggested that the amount ingested was relatively small. As no other studies have been published, we have extended the period of analysis to ascertain whether our earlier preliminary observations remain accurate.
Objective
To assess the human toxicity of automatic dishwashing rinse aids based on reports to the UK National Poisons Information Service (NPIS).
Methods
The UK NPIS (www.npis.org) provides information and evidence-based management advice about individual substances through its online database TOXBASE® and its 24-h telephone advice service, staffed by information scientists and supported by consultant clinical toxicologists. Each NPIS Unit (Birmingham, Cardiff, Edinburgh and Newcastle) takes telephone enquiries from National Health Service (NHS) healthcare professionals including doctors and other healthcare workers based in the United Kingdom, as well as from NHS Direct/NHS 111/NHS 24 (these services provide the public with advice on health issues).
An analysis of telephone enquiries to the UK NPIS from across the United Kingdom regarding automatic dishwashing rinse aids was undertaken for the period 1 January 2008 to 30 June 2019. The NPIS United Kingdom Poisons Information Database (UKPID) was searched for enquiries involving all types of automatic dishwashing products, and each exposure to an automatic dishwashing rinse aid was identified. Data (both from the text narrative as well as discrete data fields) extracted from the enquiries included age of patient, route(s) of exposure, source of enquiry, location where exposure occurred, circumstances of exposure, product information, features reported at the time of enquiry and the assigned Poisoning Severity Score (PSS). 3 The PSS score was assigned to each case based on an evaluation of the most severe symptoms reported overall, including any information obtained from follow-up (i.e. maximum PSS), and on the extensive criteria for PSS grading as detailed in Persson et al. 3 For example, in the case of ingestion, a single episode of vomiting was designated as of minor severity (PSS 1), whereas prolonged vomiting was graded as moderate severity (PSS 2). In cases of eye exposure, eye irritation was graded as minor (PSS 1) but corneal abrasion as moderate severity. The Glasgow Coma Scale (GCS) 4 was reported where appropriate.
Data were analysed, and comparisons were made between paediatric (≤5 years) and adult exposures. A two-sample χ 2 test was performed using GraphPad Prism Version 7.04 (La Jolla, California, USA) to determine whether there were statistically significant differences. Enquiries received from outside the United Kingdom were excluded from this study.
This study did not require approval by a UK Research Ethics Committee as the UK Health Research Authority has declared that ethical approval is not needed for research studies that use information collected routinely in any UK administration (England, Wales, Scotland and Northern Ireland) as part of usual clinical care, provided this information is passed to the researchers in a fully anonymized format.
Results
Over the study period, there were 1012 patients exposed to automatic dishwashing rinse aids. The majority (n = 937, 92.6%) involved children (<18 years) and most were aged 5 years or less (n = 916 of 1012, 90.5%), although in six cases, the age of the child was not known. Of the remaining 75 adult cases, there was one case where the patient age was not known.
In the majority of cases (n = 989, 97.7%) exposures occurred at home, although 13 of the remaining 23 exposures involved adults exposed in the workplace. There were a further six cases that occurred in a supermarket, two that occurred in a hospital, and one each in a nursing home or at school.
Ingestion
Ingestion was a route of exposure in 976 cases, and 44 cases involved adults. Most of the remaining exposures (n = 912 of 932) involved young children (≤5 years); in three of these cases, the clinical features and PSS were not known. In those in whom the amount ingested was known, the majority (56%) of children <18 years and of adults (57%) ingested <50 mL of rinse aid (Table 1).
Amount of automatic dishwashing rinse aid ingested overall and by adults and children (<18 years).

Features developed in 34 of 44 (77.3%) cases involving adults (Table 2). Oral discomfort (n = 11, 25.0%) was most commonly reported, although vomiting (n = 9, 20.5%) also occurred frequently (Table 3). A burning sensation in the mouth (n = 5, 11.4%) and nausea without subsequent vomiting (n = 3, 6.8%) were also reported by several individuals. Four of the 44 adults (9.0%) were more severely poisoned (PSS ≥ 2; Table 2), although in 3 of these other agents had been co-ingested including alcohol, paracetamol and sodium hydroxide. Two of the more severely poisoned patients who had co-ingested other substances developed central nervous system (CNS) depression and both had reportedly ingested a substantial amount (1 L and 250 mL) of rinse aid; the amount ingested in the third was not known. In the first case, the patient was admitted to hospital comatose (GCS 3/15) after ingesting rinse aid with other medications (paracetamol 8 g, ibuprofen 16 tablets and diclofenac 14 tablets (dosages not known)), shampoo and surface cleaner. In the second case, the patient was admitted in a stupor following co-ingestion of alcohol. Other reported features in the more serious cases included pulmonary oedema (n = 1), difficulty swallowing (n = 1), metabolic acidosis (n = 1) and abnormal liver function (n = 1). The patient co-ingesting sodium hydroxide developed gastric ulceration, oesophageal necrosis and oesophageal stricture. No patient died.
PSS in children and adults following exposure to automatic dishwashing rinse aid.

PSS: Poisoning Severity Score.
a Excludes from the total, the three paediatric ingestion cases where PSS was not known. Cases involving children aged >5 years but <18 years are not included in the table.
Most commonly reported features following the ingestion of automatic dishwashing rinse aid by children and adults.
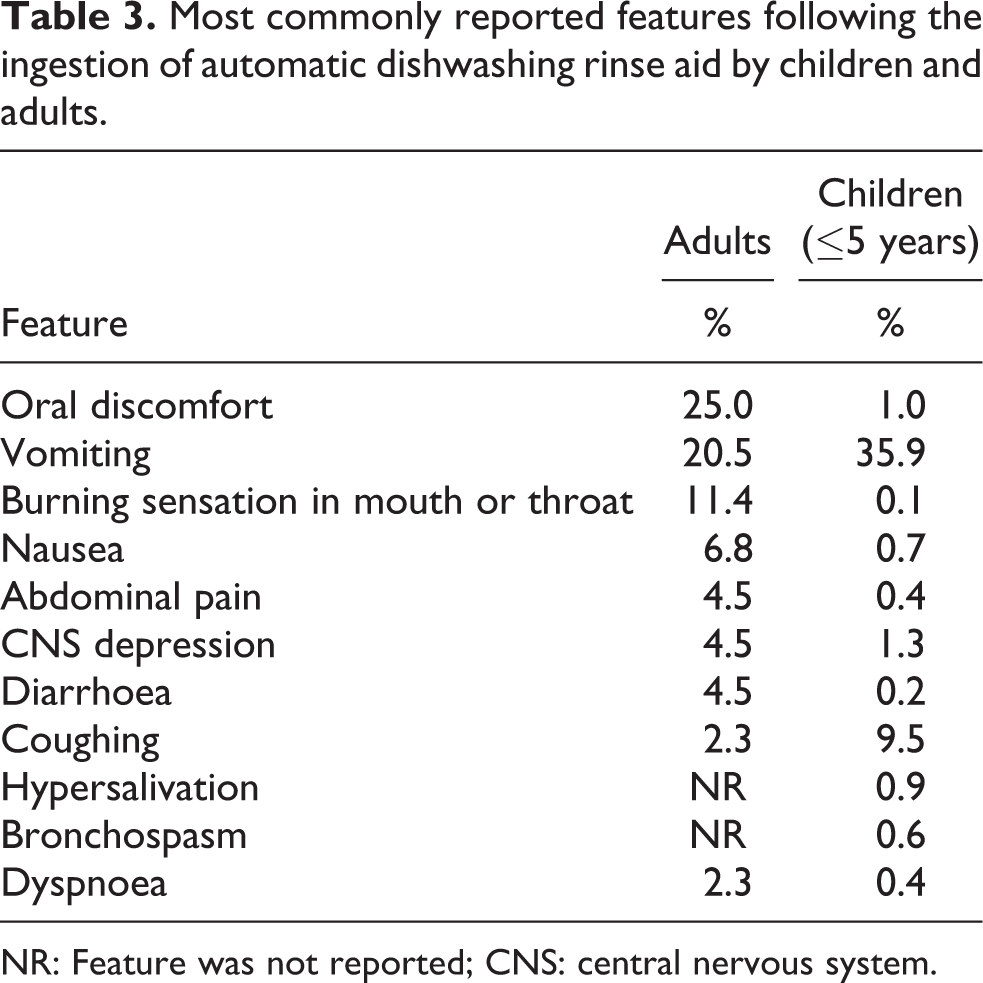
NR: Feature was not reported; CNS: central nervous system.
Features were reported in 408 (44.9%) children ≤5 years (Table 2), with over one-third (n = 326, 35.9%) of young children developing vomiting (Table 3). Coughing frequently developed (n = 86, 9.5%), while CNS depression (n = 12, 1.3%) and oral discomfort (n = 9, 1.0%) were reported occasionally. There were 16 more severe (PSS ≥ 2) cases, all involving children aged ≤ 2 years. Multiple vomiting episodes occurred in eight, CNS depression in four, hypoxaemia in two, dyspnoea in two, stridor in one, increased upper airway secretions in one and swallowing difficulties in one. Aspiration was suspected in three of these cases. One of these ingestions involved both a rinse aid and a dishwashing tablet.
Adults (76.3%) developed features significantly (p < 0.0001) more commonly than children ≤5 years (44.9%) and significantly (p < 0.0008) more adults (9.0%) were graded as PSS ≥ 2 than children (1.8%). Vomiting was reported significantly (p = 0.02) more frequently among children, whereas oral discomfort, burning sensation in the mouth or throat and nausea were reported significantly (p < 0.0001) more frequently in adults. There was no significant difference in the incidence of coughing or CNS depression between children and adults.
The majority (70%) of the 20 more severe (PSS ≥ 2) cases involved products similar in composition to those involved in less serious (PSS 1) cases. The amount ingested was not known in the majority, although 4 of the 20 patients with PSS ≥ 2 ingested other substances, as detailed above.
Eye exposure
Ocular exposure was reported in 35 cases; young children (≤5 years of age) accounted for 8 of these cases and another case involved an 11-year old. Twenty-nine patients developed features following ocular exposure (Table 2); however, there was no statistical difference between the percentage of symptomatic adults (84.6%) and young children (75.0%). Eye irritation (n = 10, 28.6%) and eye pain (n = 10, 28.6%) were the most commonly reported features. Three of 26 adults developed corneal abrasions (and were graded PSS 2), although in 2 cases it is likely that prolonged ocular contact occurred as the patients were not medically examined until 9 and 15 h post-exposure.
Dermal exposure
Thirty-four patients were exposed dermally, of whom eight were adults. All 26 children were aged 3 years or below. Dermal features were only reported in six cases, although they were reported significantly (p = 0.0001) more often by adults (62.5% of 8 cases) than children (3.8% of 26 cases). The features reported included burns (n = 2), pain (n = 2), rash (n = 2) and numbness (n = 2), itching (n = 1) or stinging (n = 1) at the contact site. In one of the two cases where burns developed another agent (a detergent containing potassium hydroxide) was also involved.
Inhalation
Two adults were exposed to rinse aid by inhalation and in both cases, exposure occurred due to misting. In the first case, misting occurred directly from the automatic dishwashing machine, while in the second, a chlorine-containing sterilizing tablet was mixed with rinse aid which resulted in a chemical reaction which possibly produced chlorine gas. The rinse aid composition was not known in either case; however, the first case occurred in the workplace so likely involved an industrial product. The first patient developed headache approximately 7 h after exposure but the other remained well.
Discussion
Some of the features reported following ingestion, including nausea, vomiting, pharyngitis, numbness/burning sensation/irritation in the mouth and difficulty in swallowing, foaming from the mouth or nostrils, abdominal pain, diarrhoea and CNS depression, could be explained by the presence of non-ionic surfactants, 5 although co-ingestion of other substances including alcohol could also have contributed. Although citric acid could potentially contribute to the reported features, it is typically present in rinse aids at concentrations ≤5% and therefore the features are more likely to be due to the surfactants.
Some non-ionic surfactants, such as ethoxylated alcohols, have been shown to induce ataxia, loss of righting, respiratory depression, coma and death when administered intraperitoneally to rats, 6 although this exposure route may limit the relevance of these observations to human ingestion. Oral administration of non-ionic surfactants to rats and mice, either alone or in combination with anionic surfactants and ethanol, has caused sedation but only following the administration of large volumes of highly concentrated solutions. 6 The length of the alkyl chain does not appear to affect the toxicity of ethoxylated alcohols, although the degree of ethoxylation does. Compounds with ethylene oxide units between 5 and 14 are more toxic orally than those with less than 4 or more than 21 ethoxy units. 5 Automatic rinse aids typically contain C12–18 ethoxylated alcohols.
Gastrointestinal features are likely to be due to the ingestion of ethoxylated alcohols which can produce vomiting and diarrhoea. 5 Vomiting in a patient who develops CNS depression increases the risk of pulmonary aspiration.
A greater proportion of adults developed features and were more severely poisoned following ingestion than young children, although the amounts ingested by adults and children were of similar magnitude in those cases where the amount ingested was known. In addition, some features such as oral discomfort, burning sensation in the mouth or throat, and nausea may have been reported more often in adults because younger children could not communicate these features as effectively. In all probability, some of the reported oral exposures among children were ‘poison scares’ rather than true ingestions.
Although dermal exposure alone did not result in clinically significant effects, three adults developed corneal abrasions following eye exposure, however in two of the cases, eye contact was prolonged.
There were a total of 23 more severe (PSS ≥ 2) cases, which usually followed ingestion (n = 20), and proportionally affected more adults than children (9.0% vs. 1.8%). Only one of the 16 more severe paediatric cases involved other co-ingested substances (a dishwashing tablet), whereas three of the four more severe adult cases involved other ingested substances, one of which was corrosive. It is probable, therefore, that these adults were more severely poisoned due to the co-ingestants. Most of the products involved in these more severe cases had non-ionic surfactant concentrations similar to the products in cases of lesser severity. However, in 50% of these more severe cases, the amount ingested was not known and it is possible that larger volumes were ingested.
As the majority of the exposures in this study involved young children (90.6% were ≤ 5 years old), this reinforces the need to continue to educate consumers that these products should be stored where children cannot gain access to them.
The results of this study are limited by factors inherent to poison centre data, such as incomplete data reporting (e.g. incomplete product identification) and the lack of patient follow-up data until complete recovery. In addition, our data may be subject to bias as reports to the UK NPIS are voluntary and are more likely to occur if there is clinical concern, for example, because clinical features are present. As a result, the total number of exposures among the UK population may be much higher as asymptomatic exposures are less likely to be reported. In addition, selection bias may occur towards more severe cases when hospitals seek advice from the NPIS only when cases are more serious.
Conclusions
Rinse aids contain non-ionic surfactants at concentrations of up to 100%. Substantial ingestion produced not only gastrointestinal features and coughing but also CNS depression, particularly in young children (n = 12). Adults (34 of 44, 77.3%) developed clinical features significantly (p < 0.0001) more frequently than young children (408 of 909, 44.9%). In addition, although more severe exposures (PSS ≥ 2) were uncommon, they occurred significantly (p < 0.0008) more often in adults (9.0%) than in children (1.8%); however, three of the four adults with PSS > 2 co-ingested other substances. Three of 35 (8.6%) patients exposed ophthalmically developed corneal abrasions, although ocular contact was prolonged. Thirty-four patients were exposed dermally, and six (17.6%) reported features, including rash, numbness, pruritus and burns (PSS = 1).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The UK NPIS has received unrestricted educational grants to undertake studies on the toxicity of household products from the UK Cleaning Products Industry Association (UKCPI) and Procter and Gamble.