
Abstract
Fluoroacetic acid (FAcOH) was once a highly toxic rodenticide widely used in the world. In the past, studies on the toxicity of FAcOH have focused on animal experiments. The toxicity of FAcOH to humans and the changes of FAcOH in plasma have not been studied. Therefore, the present study aimed to describe the changes of plasma FAcOH concentrations, hematological, and biochemical characteristics in patients with FAcOH intoxication. According to clinical symptoms, 68 patients from the emergency department were divided into different groups: convulsion group, unconsciousness group, death group, and control groups. Plasma FAcOH concentrations, hematological, and biochemical parameters were investigated. Results demonstrated that patients in the convulsion group and the unconsciousness group had a significant increase (p < 0.01) in the level of neuron-specific enolase (NSE), creatine kinase MB (CKMB), glucose (GLU), and white blood cell count (WBC) and a significant decrease (p < 0.01) in serum potassium compared with the control group, respectively. Moreover, patients in the death group had a significant increase (p < 0.01) in the level of NSE, CKMB, N-terminal pro-brain natriuretic peptide, GLU, and WBC and a significant decrease (p < 0.01) in serum potassium and total calcium compared with the survival group. The concentrations of FAcOH in plasma in the convulsion group, the unconsciousness group, and the death group were 72.31 ± 42.29, 118.33 ± 55.41, and 163.78 ± 43.32 μg/mL, respectively. These changes and the plasma FAcOH concentrations may increase our understanding of the toxicity of FAcOH to humans and may help doctors to judge the clinical prognosis of patients with FAcOH intoxication.
Introduction
Sodium fluoroacetate and fluoroacetamide are all belong to organic fluorine rodenticides. The use of these two rodenticides has been severely restricted in many countries due to their high toxicity to human and animals. 1,2 However, driven by economic interests, the illegal production and sale of these rodenticides still exist in some developing countries. 3 Several suicide poisoning cases with these rodenticides continue to be reported in recent years. 4,5
Both sodium fluoroacetate and fluoroacetamide can be easily metabolized to fluoroacetic acid (FAcOH), which can block the tricarboxylic acid (Krebs) cycle, thereby producing a series of clinical symptoms such as seizures, arrhythmia, or even death. 3,6 FAcOH, as a highly toxic substance, is also found in many poisonous plants and can cause death to surrounding organisms. 7 Toxicity of FAcOH has been reported in literatures; the oral lethal doses of sodium fluoroacetate in human are about 2–5 mg/kg and are 0.06–0.20 mg/kg in dogs. 6,8
A few studies on FAcOH are animals’ experiments, such as sheep, cat, or rat. 9 –11 FAcOH has been reported to produce hematological and biochemical changes in different animal species. 1,10 There are significant species variations in the clinical presentation of FAcOH intoxication. 12 Also, published reports of physiological and biochemical responses to FAcOH are rather controversial. 13 Until now, toxicological information of FAcOH is quite limited in human beings. FAcOH is a common toxic substance in emergency department of our hospital. 4 In our previous work, we have established a qualitative and quantitative liquid chromatography–tandem mass spectrometry (LC-MS/MS) method for analysis of FAcOH in patient’s plasma. 4 Investigating the toxicity of FAcOH in human is very important for clinical emergency treatment. In this study, based on the above, we evaluated the changes of plasma FAcOH concentrations, clinical symptoms, the hematological, and biochemical characteristics in patient with FAcOH intoxication. These findings will allow us to have a better understanding of the FAcOH toxicity to human beings, which may lead to designing an effective treatment for FAcOH intoxication.
Material and methods
Study population
The study participants were acute organic fluorine rodenticides poisoning patients who were admitted to the First Affiliated Hospital of Harbin Medical University between January 2017 and December 2018. The diagnosis of organic fluorine rodenticides poisoning was based on the positive results of FAcOH in patient’s plasma. Patients with negative results were excluded from our study. Patients with coingestion of other toxic substances were excluded from our study. To make sure have identical ingestion–admission intervals, patients who were admitted over 5 h from ingestion were also excluded. Before the study, participants or their parents were informed about the study aim and the detailed process such as questionnaire and blood sampling. After that, informed consent was obtained from every participant or their parents in this study. This study was approved by the First Affiliated Hospital of Harbin Medical University Ethical Committee for Medical Research and Other Studies Involving Human Subjects.
Patient characteristics and treatment
A structured questionnaire containing demographic information, clinical symptoms, and laboratory parameters was used in our study. The questionnaire was conducted by well-trained physicians who were highly educated and have rich experience in interview skill. The demographic and clinical characteristics of patients were recorded after admission. Mainly include age, gender, prehospital interval, blood pressure, temperature, pulse rate, respiratory rate, and clinical symptoms, such as nausea, vomiting, abdominal pain, convulsion, and unconsciousness. Until now, there are no current guidelines for the treatment of FAcOH poisoning. In our study, the patients with FAcOH intoxication were treated with the following treatments: (1) gastric lavage; (2) electrolyte correction: Na, K, Cl, and Ca; (3) acetamide, the antidote for FAcOH poisoning; (4) hemoperfusion; and (5) symptomatic treatment.
Blood sample collection
Single blood sample for FAcOH analysis was drawn from all patients by venipuncture into vacutainer tubes containing ethylenediaminetetraacetic acid after admission. Also, blood samples were collected from all patients for hematological and biochemical analyses on admission. To observe the continuous changes of FAcOH in plasma after poisoning, blood samples were collected in the morning from 18 patients (who hospitalized for more than 5 days, the longest time point was 11th day). Similarly, the changes of hematological and biochemical indexes were also observed in these 18 patients. The vacutainer tubes were stored in a portable fridge and brought to the clinical laboratories of the First Affiliated Hospital of Harbin Medical University.
Quantification of plasma FAcOH concentrations
Plasma FAcOH concentrations were determined using a LC-MS/MS method as previously described. 4 Simply, the blood samples were centrifuged at 4000 r/min for 5 min at 4°C to obtain plasma samples. Then, 20 μL of isotopic labeled internal standard (FAcOH-13C2, D2) was added into 200 μL of plasma in a 1.5-mL centrifuge tube. Acetonitrile (600 μL) was added into the tube and vortex mixed for 1 min to remove protein. The mixture was centrifuged at 13,000 r/min for 5 min in a refrigerated centrifuge. The supernatant (20 μL) was injected into LC-MS/MS system for analysis (AB Sciex, Framingham, Massachusetts, USA).
Hematology and biochemistry assays
The collected blood samples were sent to the laboratories for hematology and biochemistry assays. Hematological parameters were determined in fresh whole blood samples. These parameters included white blood cell count (WBC), red blood cell count (RBC), platelet, and hemoglobin. Biochemistry parameters were measured in serum samples, including neuron-specific enolase (NSE), creatine kinase MB (CKMB), N-terminal pro-brain natriuretic peptide (NT-proBNP), alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin (TBIL), gamma-glutamyl transferase (GGT), blood urea nitrogen (BUN), creatinine (Cr), serum sodium, serum potassium, total calcium, serum chloride, and glucose (GLU). Besides, arterial blood gases including arterial pH, PaO2, and PaCO2 were also measured in our study.
Statistical analysis
SPSS20.0 statistical software was used for all statistical analysis. Values are presented as the mean ± SD. For pairwise comparisons, the Student’s t test was applied. For comparisons of more than two groups, the one-way analysis of variance was performed. A p-value less than 0.05 was considered as statistically significant.
Results
Basic clinical characteristics of the patients
A total of 68 patients with FAcOH intoxication were enrolled in this study. The demographical and clinical characteristics of all patients are presented in Table 1. Of all the study participants, 52.94% (n = 36) were male and 47.06% (n = 32) were female. The average age of the patients was 50.28 ± 15.20 years (range 17–87 years). The average time from ingestion to blood sampling was 3.52 h ± 1.42 (range 0.5–5 h). Patient’s blood pressure, temperature, heart rate, and respiratory rate at the time of admission are also tabulated in Table 1.
The demographical and clinical characteristics of the study participants (n = 68).

SD: standard deviation; SBP: systolic blood pressure; DBP: diastolic blood pressure.
Clinical symptoms after poisoning
Previous literature reported that the cardinal symptoms of acute FAcOH poisoning include nausea, vomiting, abdominal pain, convulsions, and unconsciousness. In this study, we recorded the above symptoms of 68 patients after poisoning. There were 41 (60.29%) patients occurred nausea or vomiting in 68 patients. There were 17 (25.00%) patients suffered convulsion and 18 (26.47%) patients occurred unconsciousness in 68 patients. However, there were only two patients occurred abdominal pain with FAcOH intoxication. Six of 68 patients died in our study (mortality rate 8.82%).
Laboratory parameters on admission in patients
The patients were divided into six groups based on whether they have the following clinical symptoms (convulsion, unconsciousness, or death). The mean plasma FAcOH concentration in convulsion group, unconsciousness group, and death group were 72.31 ± 42.29, 118.33 ± 55.41, and 163.78 ± 43.32 μg/mL, respectively. Patients with convulsion had significantly higher level of NSE, CKMB, GLU, and a higher count of WBC compared with the control group (Table 2). On the contrary, the serum potassium level decreased significantly in the convulsion group compared with the control group. The similar changes in these parameters were also found in the unconsciousness group as compared with the control group. In the death group, we found NSE, CKMB, GLU, NT-proBNP, and WBC were significantly higher than the survival group. However, the total calcium and serum potassium were significantly decreased compared with the survival group. The detail data are presented in Table 2.
Plasma FAcOH concentration and laboratory parameters in patient with different clinical symptoms.
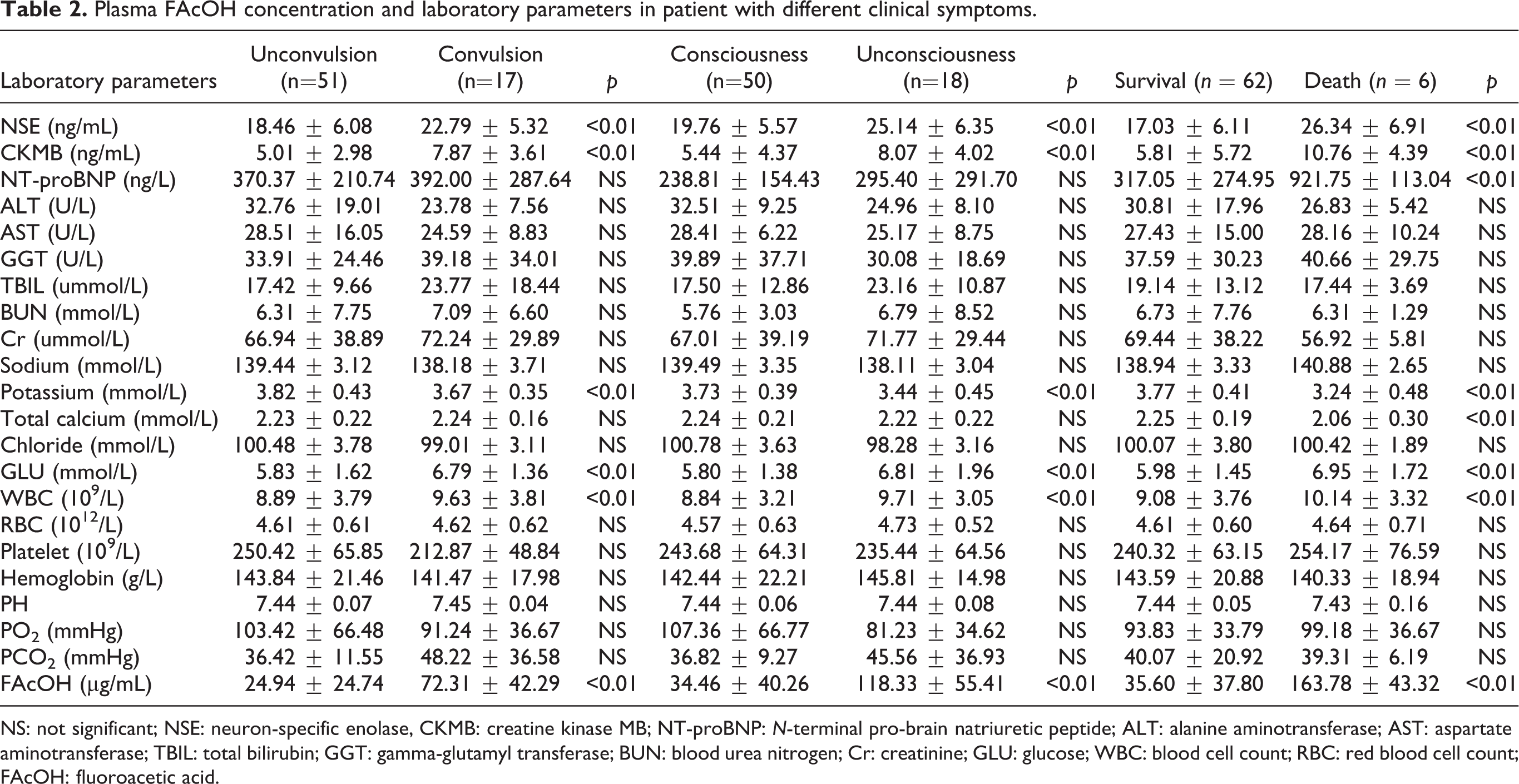
NS: not significant; NSE: neuron-specific enolase, CKMB: creatine kinase MB; NT-proBNP: N-terminal pro-brain natriuretic peptide; ALT: alanine aminotransferase; AST: aspartate aminotransferase; TBIL: total bilirubin; GGT: gamma-glutamyl transferase; BUN: blood urea nitrogen; Cr: creatinine; GLU: glucose; WBC: blood cell count; RBC: red blood cell count; FAcOH: fluoroacetic acid.
The plasma FAcOH concentration in 18 patients
Figure 1 showed the changes of plasma FAcOH with days of poisoning in 18 patients. Plasma FAcOH concentrations fell rapidly during the first 5 days after ingestion, but after 5 days, they declined more slowly. A low plasma concentration of FAcOH could be observed in one patient on the 11th day of admission.

Plasma FAcOH concentration–time curves of 18 patients. FAcOH: fluoroacetic acid.
Hematological and serum biochemical characteristics in 18 patients
In our study, we found that the count of RBC was no significant differences between different groups (Table 2). However, in the observation of 18 patients for 5 consecutive days, we found that the count of RBC was gradually decreased in the 5 consecutive days in 18 patients with FAcOH intoxication, though did not reach the significant level (Figure 2(a)).

(a) The mean value of red blood cells in 18 patients with FAcOH intoxication for 5 consecutive days after admission (n = 18). (b) The mean value of BUN in 18 patients with FAcOH intoxication for 5 consecutive days after admission. (c) The mean value of Cr in 18 patients with FAcOH intoxication for 5 consecutive days after admission (n = 18). *p < 0.05 versus day 1. FAcOH: fluoroacetic acid; BUN: blood urea nitrogen; Cr: creatinine.
In the study of the serum biochemistry, we found that the values of liver enzymes, such as ALT, AST, TBIL, and GGT, have no significant differences between different groups, data were presented in Table 2. Additionally, we compared these liver enzymes for 5 consecutive days in the 18 patients after admission. There were also no significant changes in these markers between the five consecutive days after intoxication with FAcOH (data not shown).
For the markers of kidney injury, we investigated changes of Cr and BUN; there were no significant changes on admission in different groups (Table 2). However, the mean value of BUN was significantly higher at the fifth day compared with the first day in the 18 patients (Figure 2(b)). The mean value of Cr was higher at the third day compared with the first day, though did not reach the significant level (Figure 2(c)).
Discussion
Although organic fluorine rodenticides have been banned for many years, they are still illegally produced and used in many countries. 14 Cases of organic fluorine rodenticides poisoning are still reported in many areas. The organic fluorine rodenticides such as sodium fluoroacetate or fluoroacetamide can be easily converted into FAcOH in vivo and cause metabolic disorders.3.6 However, clinical data on FAcOH poisoning in human beings are very limited due to the scarcity of poisoning cases. Until now, there was no study concerning the concentrations of FAcOH in human plasma. Our study was the first report to describe the plasma FAcOH concentrations in patients with different clinical symptoms. Moreover, we investigated the hematological and biochemical characteristics in different groups with FAcOH intoxication.
The clinical symptoms of FAcOH intoxication have an extraordinarily wide variation in various species of animals. 14 Several previous researches have reported the common clinical symptoms in patients with FAcOH. 15,16 According to clinical symptoms, we divided the patients into six groups and compared the concentrations of FAcOH in the different groups. The results revealed that patients with FAcOH poisoning are at high risk of death when plasma FAcOH concentration reached to 163.78 μg/mL, despite gave rapid treatment. Additionally, according to the plasma FAcOH concentration, we can assess the degree of FAcOH poisoning and give reasonable relief.
In the study of continuous changes of FAcOH, we found the plasma FAcOH concentrations fell rapidly at first 5 days and slowly thereafter. This downtrend is similar to a study in rabbits. 17 The rapid decline may be due to the conversion of FAcOH into fluorocitric acid (another toxic form) in the body. Although the FAcOH concentration decreased rapidly, FAcOH can remain in plasma at low concentration for a long time (shown in Figure 1).
GLU is considered to be one of the key substances most affected by FAcOH intoxication; however, the mechanism is not clear. 2 In our study, the mean value of GLU in different groups (convulsion, unconsciousness or death) was higher than the control group, which indicated that FAcOH could induce an imbalance in GLU. This may be due to the accumulation of citrate in vivo, which can inhibit the activity of phosphofructokinase, a key enzyme in glycolysis. 18 NSE, as a biomarker of nerve injury, has not been reported in patients with FAcOH intoxication. In our study, we found that the NSE was significantly increased in different groups compared with the control group. This increase may be related to the neurotoxicity caused by FAcOH. The damaged neurons caused by FAcOH can release NSE into the bloodstream. The main clinical significance of increased NSE is that patients with FAcOH intoxication may develop toxic encephalopathy or other neurological diseases during the clinical recovery period, which should be attention during treatment. Similarly, we also found that the CKMB were significantly increased in different groups compared with the control group. The increase in CKMB was also confirmed in the study of Collicchio-Zuanaze et al., 10 which indicated that FAcOH can cause damage to cardiomyocytes, which can lead to arrhythmia or even cardiac arrest. In the study of electrolytes, the most obvious change was a decrease in serum potassium. The decrease of serum potassium may also be a cause of arrhythmia or cardiac arrest. 19 In addition to the above parameters, we found significant differences in NT-proBNP and total calcium in the death group compared with the survival group. The plasma NT-proBNP may provide important prognostic information for the risk of heart failure in patients with FAcOH intoxication.
The hepatic injury markers such as AST, ALT, TBIL, and GGT have no significant differences between different groups. Also, these markers have no significant changes in 18 patients between the first 5 days after poisoning. These results agree with the previous study, 10 indicating that FAcOH may have weak toxicity to the liver. This may because FAcOH in the liver was at a lower concentration after poisoning. 20 For the markers of kidney injury, the elevated Cr and BUN during the 5 days after admission showed that the FAcOH may have a damaging effect on the kidney, which will be further investigated in the further.
In the study of the hematological profile, we found that the count of WBC was significantly increased in different groups compared with the control group, which was different from the study 10 where the transient decrease was observed in cats exposed to FAcOH. This difference could be explained by species diversity or the different time points of blood collection. Furthermore, the inflammation caused by toxic stress can lead to an increase in the count of WBC. 21 Although many diseases can lead to leukocytosis, this study proved that leukocytosis can serve as an auxiliary indicator for clinical FAcOH poisoning. In our study, there was no significant difference in the count of RBC between the groups. However, the count of RBC was gradually decreased in the 5 consecutive days in 18 patients with FAcOH intoxication. The decrease of RBC was probably due to the intravenous fluid during treatment.
Conclusions
There were obvious changes in hematological and biochemical parameters in patients with FAcOH intoxication, such as increases in NSE, CKMB, GLU, and WBC and decreases in serum potassium and calcium. There were no significant changes in liver enzymes, such as ALT, AST, TBIL, and GGT after FAcOH poisoning. Combined with these parameters, physicians can make a better diagnosis of patients with FAcOH intoxication. Moreover, this study showed the plasma concentration of FAcOH in patients with different clinical symptoms and the changes of FAcOH in patient’s plasma. These data will make us have a better understanding of the toxicity of FAcOH in human beings. However, further investigations are recommended to elucidate the toxicity of FAcOH.
Footnotes
Authors’ contributions
LL and FL contributed equally to this work. XH and KY designed the study. LL and FL extracted the data. ZD and GD analyzed the data. LL and FL drafted the manuscript. JX, WL, and XW revised the text for critical content. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors’ work on this study was supported by the foundation of The First Affiliated Hospital of Harbin Medical University (No. 2019M05), the project of health commission of Heilongjiang Province (No. 2019-006), the foundation of Heilongjiang Postdoctoral Special Program (No. LBH-TZ16), the Postdoctoral Program of Heilongjiang Province, the Natural Science Foundation of Heilongjiang Province For Excellent Youths (No. JJ2019YX0862), the China Postdoctoral Science Foundation, and the Natural Science Foundation of Heilongjiang Province (No. H2017040).