
Abstract
Objective:
Paraquat (PQ) poisoning is a significant cause of mortality and morbidity in developing countries. Poor prognostic outcomes have been attributed to the herbicide’s toxicity and the lack of effective treatments. Our study aims to investigate the changes in lymphocyte count in both patients who survived and died from PQ poisoning and explore the prognostic value.
Method:
This is a retrospective case serials observational study. Adult patients admitted with acute PQ poisoning. The notes of 1000 patients who presented with acute PQ poisoning were reviewed. One hundred thirty patients having the T lymphocyte met the inclusion criteria and were grouped into those that survived the poisoning (95) and non-survivors (35).
Results:
On admission, non-survivors had a higher ingestion volume of PQ and urine PQ concentration as well as higher severity indices (Acute Physiology and Chronic Health Evaluation 2, Sequential Organ Failure Assessment, and Poisoning Severity Score). Patients in the survival group had a higher dosage of immunosuppressant and a longer hospital stay. Leukocytes, especially neutrophils, were higher among non-survivors; however, the converse was found with lymphocytes. T lymphocyte (CD3) count was consistently higher among survivors as well as the subgroups CD4+ and CD8+. No differences in the ratio of CD4/CD8 were found between the groups.
Conclusion:
Our study has shown that changes in lymphocyte count as its subgroups could indicate a host’s immune status and lymphocytes play an important role as a surrogate marker of host immunity, which could be a useful prognostic tool in the assessment of this disease.
Introduction
Paraquat (PQ) poisoning is still a very serious challenge in China and other developing countries, with a mortality about 50–70%. 1,2 After ingestion and absorption, PQ-derived reactive oxygen species generates rapidly, and systemic inflammation response syndrome (SIRS) is activated, which may result in multi-organ failure and eventual death. 3
In the current literature, there are studies reporting on the changes of leukocytes in PQ-poisoned patients, in which elevations of leukocytes, especially neutrophils, and falls in lymphocytes can be seen in non-survivors. Zhou et al. retrospectively reviewed 202 cases of PQ poisoning and found that the lymphocyte count was lower in the non-survivors than in the survivors (median 0.90 vs. 1.20, p < 0.001), but lymphocyte count was not an independent risk factor. The neutrophil–lymphocyte ratio, leukocyte, and neutrophils were the independent risk factors, and neutrophil–lymphocyte ratio had the largest area under the curve of 0.916 for prognosis prediction. 4 In a study by Tang et al., 96 PQ-poisoned patients and 188 healthy persons were enrolled, and the lymphocyte count in the PQ group was lower than the healthy group (0.96 + 0.45 vs. 1.96 + 0.54). Lymphocyte count among non-survivors was lower than among survivors (0.05 + 0.02 vs. 0.09 + 0.05, p < 0.001). 5 Conversely, Kang et al. conducted a retrospective study of 136 patients and found that the absolute lymphocyte count was significantly higher among non-survivors than in the survivors. Absolute lymphocyte count was categorized in four levels: <1700, 1700–3200, 3200–5000, and >5000; increased mortality was associated with a lymphocyte count of over 5000. 6
Lymphocytes are one type of leukocyte and form an integral part of the immune system. Lymphocytes consist of three major types—B cells, natural killer cells, and T cells. Lymphocytopenia is usually defined as below 2.5 × 109 L−1, and lymphocytosis is defined as an increase over 4.0 × 109 L−1.
In the light of the controversy surrounding lymphocyte count prediction role and there being no previous studies on the change of T lymphocyte subgroup, our case control observational study was designed to retrospectively review lymphocyte and its T subgroup cell changes in PQ-poisoned patients and explore these changes between survivors and non-survivors.
Methods
The notes of patients, who presented with acute PQ poisoning from July 2013 to March 2018 to the first affiliated hospital of Zhengzhou University, were retrospectively reviewed.
The inclusion criteria were acute ingestion of PQ (admitted within 48 h after ingestion) confirmed by PQ urine testing (normal range 0–0.2 µg mL−1) 7 and available blood results of T lymphocyte counts including CD3, CD4, and CD8 counts. The exclusion criteria were co-ingestion of other toxins or drugs, pregnancy or lactation, past history of immunological disease, organ transplantation, or other conditions involving steroid and/or other immunosuppressant therapy.
Patients underwent the following established treatment regime, which was laid out with more details in our previous study and national guideline in China. 2,8 Gastric lavage was performed on admission; smectite powder was then given with a dose of 6 g every 4 h on the day after admission. Immunological therapies were started on admission. Cyclophosphamide (CP, 10–15 mg kg−1 day−1) was given for 1 week. Methylprednisolone (MP, 15 mg kg−1 day−1) was prescribed for the first 3 days, decreased to 8 mg kg−1 day−1 on the fourth day, and tapered 1 week later by 40 mg every 3 days. As soon as the dose of MP reduced to 40 mg day−1, oral tablets of prednisone were prescribed with 5 mg decreases every other day. Oxygen therapy would only be commenced if the patient has dyspnea, and pulse saturation was below 70% (or arterial oxygen pressure below 50 mmHg). Hemoperfusion was performed after admission as quickly as possible for 4 h and repeated once a day for at least 3 days. Hemofiltration would only commence if acute renal failure occurred.
Baseline data of the patients were retrieved from patient notes including age, gender, ingestion volume and time, vital signs on admission, and medical history. If the exact ingestion volume was uncertain, it was estimated by mouthfuls (one male mouthful 40 mL, one female mouthful 30 mL).
T lymphocyte counts, including CD3, CD4, and CD8 on the first, third, fifth, and seventh day after admission and the day before discharge, were retrieved. CD4 and CD8 were counted by combining monoclonal antibodies with antigens on the surface of lymphocyte and polychromatic fluorescent dyes, the lymphocyte subsets with different functions could be distinguished, and the relative proportion and absolute number of each subset could be obtained. The fluorophores used were CD4-APC and CD8-PE, and Novocyte D2040R was the model of the machine.
Other routine laboratory tests, which included leukocyte, lymphocyte, and neutrophil percentage, platelet, plateletcrit, mean platelet volume; pH, partial pressure of carbon dioxide (PaCO2) and partial pressure of oxygen, arterial lactate; alanine transaminase (ALT), total bilirubin, lactate dehydrogenase (LDH), γ-glutamyl transpeptidase; blood urea nitrogen (BUN) and creatinine; cystatin C; creatine kinase and creatine kinase-MB; serum amylase and lipase; and so on, were recorded. Acute Physiology and Chronic Health Evaluation 2 (APACHE 2), Sequential Organ Failure Assessment (SOFA), and Poisoning Severity Score (PSS) were recorded for all patients on admission.
Based on the outcome in hospital, patients were classified into two groups: the survival group and the deceased group. Data were expressed as median (25 quantile, 75 quantile). Each variable above was compared between survivors and non-survivors. The kinetic changes of T lymphocyte counts were plotted and compared. Two-tailed p values were used, with a statistical significance defined as p < 0.05. SAS 9.2 software was used to perform all the statistical analyses.
Ethical statement
Institutional review was approved by the First Affiliated Hospital of Zhengzhou University’s ethics committee on June 8, 2015, with the serial number of 2015LW75. The study was performed strictly as approved. Methods were carried out in accordance with the approved guidelines.
Results
From July 2013 to March 2018, a total of 1000 patients were admitted to our hospital (451 died, while 549 survived, with a mortality of 45.1%). The weight was 61.63 ± 15.86 kg in the survivor group and 59.33 ± 8.17 in the non-survivor group. Eight hundred seventy patients were excluded mainly because of the lack of T lymphocyte count tests. After screening, 130 patients were included with 65 males and 65 females, and there were 35 patients in the non-survivor group, 95 cases in the survival group (Figure 1).

The flowchart of the patient enrollment.
On admission, eventual non-survivors had a higher ingestion volume of PQ (80 mL vs. 20 mL, p < 0.0001) and urine PQ concentration (20.66 µg mL−1 vs. 15 µg mL−1, p < 0.0001) than survivors. In addition, non-survivors had higher severity index scores in terms of APACHE 2, SOFA, and PSS with statistical difference, suggesting that severity is strongly associated with ingestion volume and urine concentration. Lactate, ALT, aspartate aminotransferase, LDH, BUN, creatinine, lipase, and amylase were higher among non-survivors; however, pH, PaCO2, and bicarbonate were lower. Patients in the survival group had a longer hospital stay, with a statistical significance (p < 0.0001; Table 1).
Baseline data between the two groups: median (25 quantile, 75 quantile).

ALT: alanine transaminase; PQ: paraquat; APACHE 2: Acute Physiology and Chronic Health Evaluation 2; SOFA: Sequential Organ Failure Assessment; PSS: Poisoning Severity Score; LDH: lactate dehydrogenase; BUN: blood urea nitrogen; PaCO2: partial pressure of carbon dioxide; PaO2: partial pressure of oxygen; HCO3: bicarbonate; CRP: C-reaction protein. Note: the value of X2 is 4.731, with a p value of 0.030.
Leukocytes were higher among non-survivors and had significant difference at each measurement point in time, except for day 7. Neutrophils were higher in the death than the survival group and showed significant difference at all the five time points (day 1, 3, 5, 7, and on discharge day). Lymphocytes were lower in the death than the survival group and had significant difference only at the discharge time (median 0.6 vs. 0.8, p = 0.042) (Table 2). T lymphocyte (CD3) counts were higher in the survival group as well as its subgroups CD4+ and CD8+; however, the difference shown in CD8+ cell count was only apparent on day 5 (p = 0.041). No differences in the ratio of CD4/CD8 were found between the groups (Table 3).
The kinetic value of blood cells between the two groups: median (25 quantile, 75 quantile).
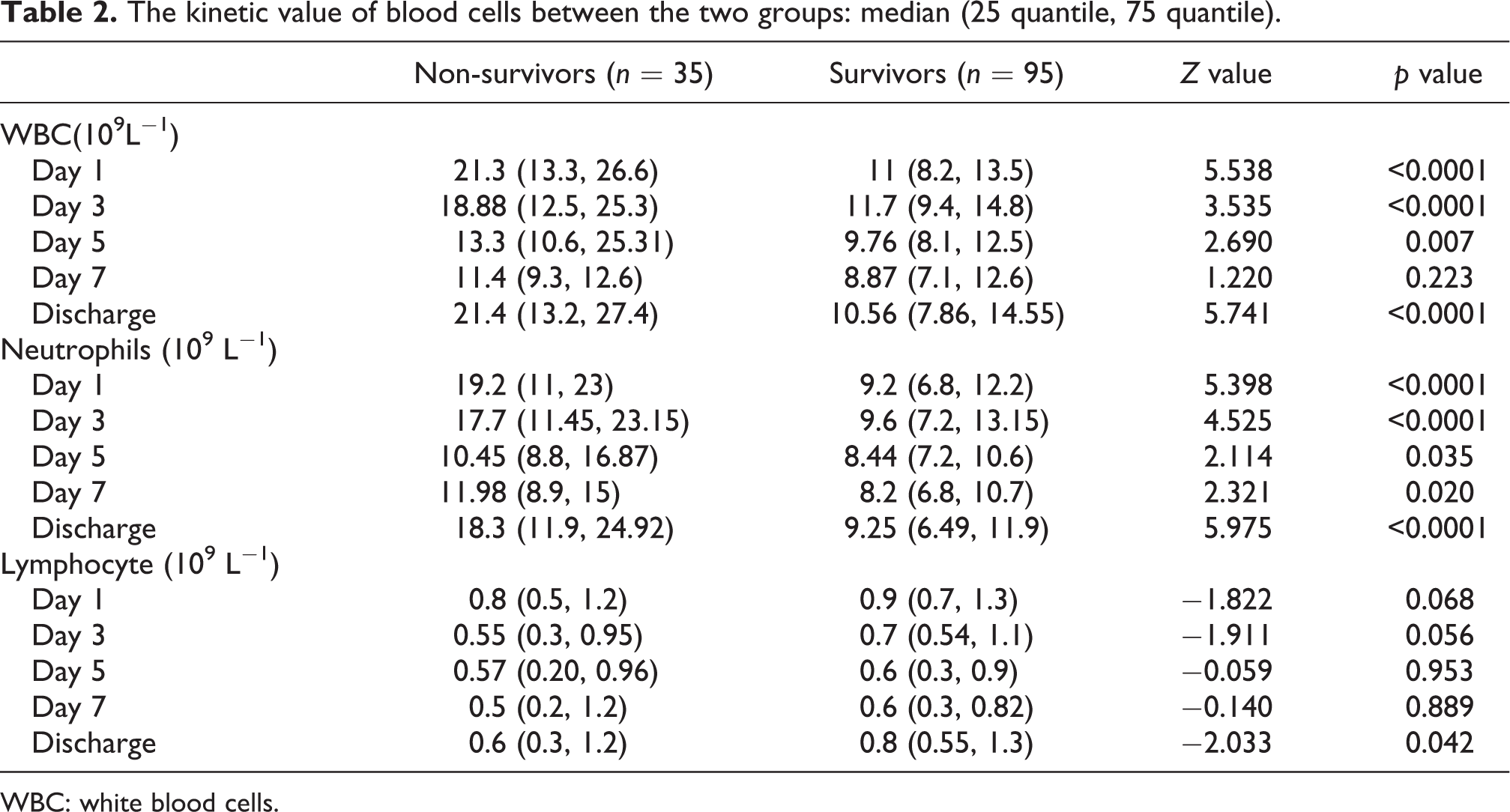
WBC: white blood cells.
The kinetic value of CD counts between the two groups: median (25 quantile, 75 quantile).a

aThere were 35, 5, 2, 1, and 35 patients having the count of CD T cell counts in the non-survivor group and 95, 35, 16, 9, and 95 patients in the survivor group on the day 1, 3, 5, 7, and the day of discharge, respectively.
Discussion
The findings of our study are (1) the level of lymphocyte is lower among non-survivors and (2) the levels of T lymphocyte (CD3) and the CD4, CD8 subgroups at each time point are higher in the survival group with statistical differences found between the two groups.
PQ poisoning is a very serious disease with high mortality and morbidity, and many indices of disease severity have been identified. The serum PQ may provide the most reliable parameter; however, the logistics of undertaking this test using specialist laboratory equipment may inhibit its day-to-day use in the clinical setting. The PQ semiquantitative urine test, which can be determined by assessing the color of urine, is convenient but limited by urine output and the renal function. The routine serum tests, including the arterial blood gas analysis (pH, PaCO2), 9 amylase, 8 lactate, 10 and so on, have been recommended for prognosis prediction. It has been suggested in some reports that the counts of blood cells, including leukocytes, neutrophils, and lymphocytes, play a role in predicting disease progression.
In previous reports, blood cells, one of the most routine lab tests, including higher leukocyte and neutrophils, had been found related with higher mortality. However, conflicting findings with lymphocytes have also been observed—lower lymphocyte counts have been found among non-survivors in some trials, 4,5 but the converse was noted in another study. 6
Our study has found lower lymphocytes among non-survivors, which is consistent with some reports in the literatures. 4,5 The most obvious statistical difference was observed with lymphocyte count at the time of discharge, which suggests that lymphocyte is a key index. We also found the lymphocyte counts were below 2.5 × 109 L−1, in all the patients at all the time points, with a greater drop among non-survivors, suggestive of T cell immunoparalysis. A decrease was found in both CD4 and CD8, which is difficult to explain, because usually the changes of CD4 and CD8 counts are divergent.
T lymphocyte, especially CD4+, plays an important role in cell immunity and is an important indicator for the HIV treatment. 11 The first report about the CD4 level of 180 in a PQ patient was in 1996, 12 which patient had a history of HIV and complicate the CD4 interpretation in the prognosis. Thereafter, another two case reports having CD4 levels were presented, with the CD4 levels of 380 13 and 400, 14 respectively, but both were HIV patients too. Based on the unusual results of the three PQ poisoning suffered hypoxia and acute kidney injury in HIV patients, Dr YQ Lu’s hypothesis that the lower levels of the lymphocyte and CD4 T cell counts may contribute to the survival of the three cases and suggest the need of CD4 targeted immunologic therapy. 15
Our research seems to be the first report having CD4 counts in PQ patients without HIV infection. The decrease in lymphocyte and CD4 counts is found not only in the survivor but also in the non-survivor, and the non-survivor had a lower level than the survivor, which does not support Dr YQ Lu’s hypothesis.
One of the main treatments for PQ poisoning is immunosuppression therapy commonly with MP and CP for the pesticide-induced SIRS, but the effect of immunosuppression therapies is doubtful and no consensus has been reached in the literature. Some report the effectiveness of immunosuppression in lowering mortality, 16,17 but the meta-analysis from the study by Eddleston et al. challenged this claim. 18 This was further challenged by Gawarammana et al. in a recent randomized controlled trial, in which the largest sample size, up to now, was recruited. Two hundred ninety-nine patients were randomized to compare MP and CP treatments with those without immunosuppression therapy. The authors found no improvement from MP and CP treatments further supporting Eddleston and colleagues’ meta-analysis findings. 19 One concern of the poor effectiveness of MP and CP treatments may be the unclear immunological state of the patient and individual goal of the immunosuppression therapies. If the SIRS reaction derived from PQ has not been suppressed enough, organ dysfunction cannot be treated on time; conversely, if it has been over suppressed, infection, bone necrosis, and so on may happen and result in death. Thus, SIRS and anti-SIRS reaction may paradoxically occur together in sepsis.
Therefore, the immunologic state should be monitored to decide when to start immunosuppression therapy and what is the optimal dose and the duration of treatment. Thus, it is important to find out the kinetic changes of T lymphocytes, including the CD4 and CD8 levels for the individual targeted immunosuppression treatment in PQ poisoning patient.
Limitations of our study are that it is a retrospective case serials study, and there are some data at some time points which were not retrievable. In addition, 130 patients were selected from 1000 patients mostly because lack of the T lymphocyte records, which may bias the result.
In the future, a prospective study with a larger sample size may need to further explore our findings and assess the value of CD T in disease severity and optimal cutoff values for the three CD T cell counts during treatment.
Conclusion
The lymphocyte, especially the CD4 count in PQ patients, is decreased, but the exact kinetic changes and their prognostic role need further investigation.
Footnotes
Author contributions
YL and YG set up the idea to do the trial. YW, SY, and XL collect the data. MW did the statistical analysis. SG refined the paper and made the final version of the paper with YG and YL.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the Grants from National Natural Science Foundation of China (Grant Nos. 81701893 (Y-XG) and 81550034 (YL)).