
Abstract
Purpose:
To investigate whether the sperm concentration of European men is deteriorating over the past 50 years of time.
Materials and Methods:
We analysed the data published in English language articles in the past 50 years in altering sperm concentration in European men.
Results:
A time-dependent decline of sperm concentration (r = −0.307, p = 0.02) in the last 50 years and an overall 32.5% decrease in mean sperm concentration was noted.
Conclusion:
This comprehensive, evidence-based meta-analysis concisely presents the evidence of decreased sperm concentration in European male over the past 50 years to serve the scientific research zone related to male reproductive health.
Introduction
There has been a recent controversy regarding changes in sperm counts during the last few decades. 1,2 It has been reported vastly in the last 20 years that sperm count is declining worldwide. The deterioration of semen quality was first reported in 1974 by Nelson and Bunge. 3 Then in a meta-analysis of 61 studies, Carlsen et al. found a significant worldwide decline in sperm counts between 1938 and 1990 among 14,947 men with no history of infertility from 23 countries. 4 In that investigation, they have found significant declines in sperm count in the United States, Europe and Australia, but no such decline in non-Western countries. The results of this meta-analysis showed that sperm density had declined globally by about 50% during the second half of the last century. After this report, in 1997, Swan et al. published a reanalysis of 56 studies that confirmed a significant decline in sperm density only in the United States and Europe. 5 However, the findings put forth by Swan et al. reflected a greater decline in sperm counts in European countries than that in the United States, the former being 3% decline per year, while the later suffered from 1.5% decline in sperm count per year. Again in 2000, in an extended meta-analysis of 101 studies, Swan et al. confirmed the decline of sperm concentration in the period of 1934–1996. 6 Subsequently, the report of Rolland et al. showed 32% decline in sperm count from 1989 to 2005. 7 Since those reports, the similar declines were also proclaimed by numerous other studies but were unable to establish a clear cause. 8 In our recent articles, we have reported decline in semen volume 9 and sperm count 10 in ageing male over the last three decades.
There are many reports regarding the altered sperm concentration in Europe (Table 1
Studies on changes of sperm concentrations in different age groups in the past 50 years in Europe.
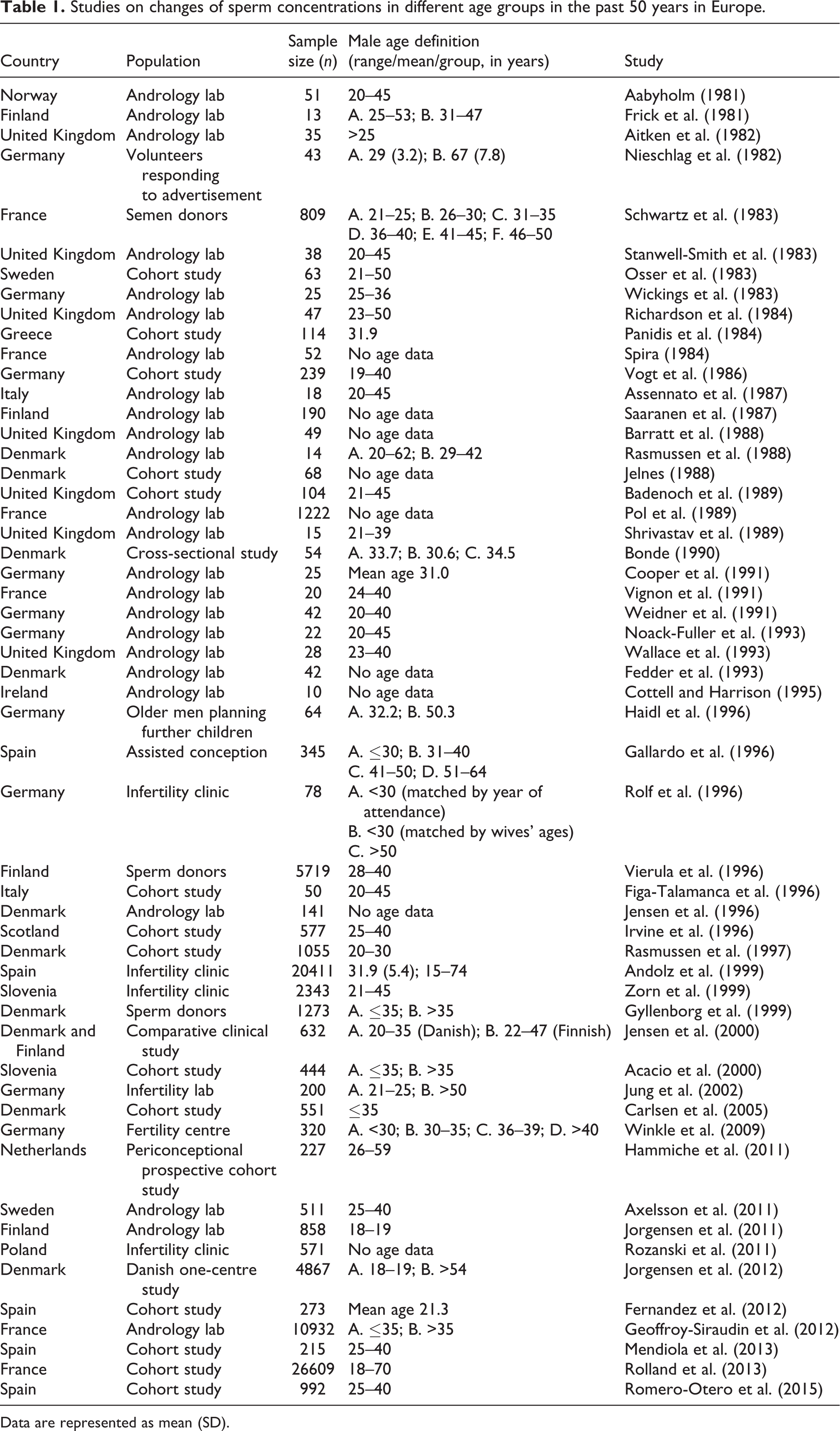
Data are represented as mean (SD).
Thus, the objective of this meta-analysis is to build up a substantial idea regarding alterations in sperm concentration in European population by picking the huge scattered reports of the past 50 years, moulding them in sequential pattern, statistically analysing and also correlating the trend with the studies describing the link factors of decreased sperm concentration.
Methods and materials
Data extraction
Research articles on humans published in English from 1965 to 2015 have been included in this report. We have also included the reports of Carlsen et al., that is, reports from 1965 to 1992. 4 We selected publications about sperm concentration, with predefined criteria for inclusion and exclusion, as follows: (1) The non-Carlsen studies published during 1965–2015 were identified by using Medical Subject Headings of electronic databases which included Medline, National Library of Medicine, Bethesda, MD, with the keywords sperm count, sperm density, sperm concentration, semen quality, male infertility and semen analysis. (2) Relevant literature on changes of the sperm concentration and its influence on future natural and assisted conception cycles were retrieved. (3) Data of the subjects with clinical problems have been excluded. (4) Studies with insufficient numbers of subjects (n < 5) were excluded. In each case, sperm concentration and its outcome were evaluated. Analytic epidemiological studies were emphasized. Therefore, the current analysis is based on 54 European studies published in 1965–2015.
Data analysis
For simple statistical analyses, Microsoft Excel v.2013 was used and correlation and regression analyses of data were done using StatSoft (2011) and SPSS v.22.0 to calculate correlation coefficient, and it was considered to be significant if p was <0.05 or <0.001. 67 Mean sperm concentrations of all 54 reports were also analysed with linear regression weighted by number of subjects included in the individual publications.
Results
During the retrieval of relevant documents, we have found 54 retrospective studies which have been conducted on altered sperm concentration of European population in the last 50 years. The outcome of these studies is represented in Table 1. Most of the reports are based on andrology laboratories (44.44%) and others included epidemiological studies (33.34%) and infertility clinics (22.22%). Among the 54 published research works discussed in this article from 1965 to 2015, most are carried out in the United Kingdom, Germany and Denmark. Most of the studies have used sample size less than 500 men (68.51%) and only three studies included sample size >1000 (16.67%). Out of 54 reports, 83.33% have provided data about the age of subjects; 70.37% of these reports have depicted a significant decrease in sperm concentration from 1965 to 2015. A time-dependent decline in sperm concentration was observed from 1965 to 2015 (r = −0.307, p = 0.02; Figure 1) that reflected an overall 32.5% decrease in mean sperm concentration. In Figure 2, an analysis has been made based on the sperm concentration values from 1965-1970 to 2010-2015. It shows the first report with all of our inclusion criteria came up in 1980s and it also reveals a gradual decrease in sperm concentration since then. Though the mean sperm concentration is much higher than the WHO reference vale, still it showing a noticeable decrease in past few decades.

Temporal decline in sperm concentration (×106/ml) from 1965 to 2015, bubble size corresponds to the number of men in the study.

Box and whisker plot of sperm concentration data of European men of the past 50 years.
Discussion
Data analysed in this present study suggest that the sperm concentration of European men seems to be deteriorating over time. Our results showed with evidence that the sperm concentration in European men has declined 32.5% in the past 50 years, that is, 1965–2015.
Our results support previous reports of similar findings concerning sperm concentration have been reported in German, 14,18,34,35,39 Spanish, 40,60,62 Scottish, 45 French, 7,21,29,33 Norwegian, 11 Italian, 23,43 Danish, 27,28,31,37,44,49 Polish 58 and Greek. 20 Conversely, many studies failed to demonstrate a time-related decline in semen quality. 15,22,24,26,32,40,41,48,51,54,56 We have also noticed most of the studies in the past 50 years had been conducted in the United Kingdom, Germany and Denmark. Other than these, Finland, Norway, Sweden, Greece, Italy, Spain and France also reported the same trend. In a study in 2001, Jorgensen et al. reported the regional variations in semen quality in Europe. In that study, they reported lowest sperm concentrations and total counts were detected for Danish men, followed by French and Scottish men, and Finnish men had the highest sperm counts. 68 Another study, via numerous data, had also showcased most rapid sperm count decline in Danish men, while an overall decline in sperm count in European men owing to two- to four-fold increased occurrence of testicular cancer over the past 50 years. 69
Recently, one of our meta-analysis reported a significant decrease in sperm concentration worldwide between 1980 and 2015 from 91.65 × 106/ml to 39.34 × 106/ml (r = −0.313, p = 0.0002). It has reflected almost 57% decline in sperm count worldwide from 1980. 10 It has also showed recruitment of larger population for this type of study has been increased predominantly after 1995, also found in this study. Recent studies on semen quality when brought together bring conflicting evidence to the forefront regarding sperm counts with some showing a significant decline, while some have found no change. In our study, we reported a more declining trend in North America, Europe and Asia, whereas studies based on South America and Australia do not depict such trend, which suggested the biologically meaningful regional differences in global sperm counts. 10 Conversely, a recent review from Cocuzza and Esteves 70 showed that there is no enough evidence confirming a global decline in semen parameters. Curiously, some studies observed that semen quality has not declined nor remained steady but slightly increased in recent years. 14,47,53,57 Nevertheless, follow-up studies are necessary to investigate whether this finding is a real phenomenon or purely random variation. The discrepancy in the results obtained in the studies may be explained by selection criteria of volunteers or other confounding factors, such as the number of subjects included in each study. It is noteworthy that the observed time trend in semen quality might be an artefact, since the methodological variances amongst studies might be time dependent. In many studies, historical data collected for other purposes have been used without close attention to important and specific factors relevant to an analysis of secular or geographical trends.
In that report, we have also mentioned about the possible causes of the decreasing sperm concentration. It has been suggested that the increased frequency of male reproductive abnormalities reflect adverse effects of environmental or lifestyle factors, such as occupational and environmental exposures, medications and sexually transmitted diseases. 64,65 These factors play a key role in determining reproductive health and can influence fertility. Over the last few decades, there have been progressive changes in aspects of our diet, lifestyle as well as environment. Report in recent years has shown that the incident of male infertility has increased as a result of various factors such as environmental pollution, stress and lifestyle. Among lifestyle, factors such as tobacco smoking, smokeless tobacco chewing and alcohol intake have a profound negative impact on general health. The association of lifestyle factors with deterioration of reproductive health receiving attention, such as tobacco smoking and chewing, alcohol, high temperature and some modern electronic gadget, has shown to affect reproduction adversely. These factors may impair male fertility by interfering with spermatogenesis, spermiogenesis, motility, sperm DNA and chromatin integrity, hormonal regulation or by reducing the fertilizing capacity of spermatozoa. In our previous reports, we have also indicated the root causes of this trend in declining semen quality, highlighting on the effects of several lifestyle factors on male reproductive health. 1,2,9
The expansion and demanding agricultural and industrial activity worldwide, along with repeated disrespect for environmental protection measures, are a risk to human population’s health. Recently, the effect of pollutants and occupational factors on reproductive health has been a matter of debate. Indeed, environmental pollutants such as methyl mercury, pesticides, lead, welding, organic solvents, radiation, endocrine-disrupting compounds and household glues have been shown to compromise male reproductive function. 64,71 –76 A recent report has indicated the reproductive health risk among male after exposure of bisphenol A (BPA) and other pesticides. It has reported an altered semen quality from 2007 to 2013 after exposure to BPA. BPA exposure has been reported to be associated with adverse birth outcomes, hyperandrogenism, sexual dysfunction and impaired implantation in humans. 77 In one of our previous reports also we have mentioned the impact of several pesticides and endocrine disruptors, including BPA, on declining male reproductive health. 64 Alteration of the male reproductive health may be due to effects on the endocrine control of reproductive system 78 –80 or by direct effect on spermatogenesis. 81,82 However, one possible mechanism associated with adverse pregnancy outcomes due to paternal exposure to organic solvents is a direct effect on sperm DNA, producing mutations or chromosomal abnormalities. 83
In their study in 2001, Jorgensen et al. reported that the incidence of testicular cancer is five times higher among Danish men than among Finnish men, 84,85 which may reflect in their sperm concentration. They had also added, concerning the gradient in the incidence of hypospadias between Denmark and Finland seems to parallel that of testicular cancer 86 and contributing in reduced sperm count. However, the proper causes and their correlation with declining sperm concentration in European population in the past 50 years still remain to be elucidated. It should be mentioned that concrete confirmatory data regarding the causative agent for declining trends in sperm count are not available which demands extensive research in this stratum to find out exactly which environmental factors or other ‘endocrine disruptors’ are acting as the culprits of the declining trend of sperm count. 87 –89
The potential drawbacks of this study are (i) sperm concentration data were retrospectively reviewed and, therefore, (ii) we were unable to collect information on potential confounders, including occupation of the subjects, smoking, food habits and level of stress. Moreover, (iii) the inclusion of potential sub-fertile men attending an infertility centre might be a selection bias. Moreover, as mentioned by Velde and Bonde in their article about misconceptions regarding decreasing sperm counts and fertility in Europe, we are not claiming this decrease is the sole cause of declining fertility rate and male reproductive health in Europe. There are innumerable factors which can contribute to reduced fertility rate. 90 Thus, from this study, we cannot correlate the contributing factors of declining sperm concentration in Europe in the past 50 years as well as cannot claim this is the cause of decreasing fertility in Europe. Following this analysis, we feel that future prospective studies including representative samples addressing lifestyle, occupational and other related factors from each region in general population are needed to confirm whether sperm concentration is still declining in Europe.
Conclusion
This study demonstrated with pertinent evidences that there is an overall 32.5% decline in sperm concentration in European men over the past 50 years. Through this meta-analysis, we are also reporting a time-dependent decline of sperm concentration (r = −0.307, p = 0.02) in the last 50 years in European countries. Although the evidence linking environmental factors and impaired male fertility is weak, there are still some evidences suggesting that semen quality may be influenced by environmental factors and lifestyle. This finding might have implications on fertility status of European men and emphasizes the need for further studies addressing lifestyle and other factors in order to find the proper correlation with the causative agents.
Footnotes
Acknowledgements
The authors are thankful to Datuk Dr Abdul Gani Bin Mohammed Din, Dean, Faculty of Medicine and Deputy Vice Chancellor (Academic), Lincoln University College, and Professor Dr Amiya Bhaumik, CEO and Vice Chancellor, Lincoln University College, for their kind support and encouragement. The authors are also thankful to Dr Sandeep Poddar, Research Manager, Lincoln University College, for his valuable suggestions during this research work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.