
Abstract
Lipid rescue is used as treatment of various poisonings despite weak scientific evidence. Some experimental studies have indicated a positive effect, but others have not. Clinical studies are lacking, wherefore a systematic review of virtually all published human case reports is presented. The case reports were searched for in PubMed and Web of Science and examined by two experts according to an assessment form grading the probability for a causal connection between lipid rescue and improved symptoms. A total of 160 cases were finally included, of which 30 had no positive effect of lipid rescue. Among the 130 included cases with alleged positive effect, 94 were oral poisonings and 36 were cases with local anesthetic systemic toxicity (LAST). The experts’ assessment resulted in a “certain” causal connection in three cases with LAST but not in oral poisoning. Moreover, the mean assessment score among the oral poisonings was significantly worse than the corresponding score in the cases with LAST. The average log p-value of the main toxins among the oral poisonings was significantly lower than the corresponding p-value in the cases with LAST. Among the oral poisonings, 91% had received some other resuscitative treatment more or less simultaneously with lipid rescue. Considering the findings of this study and the increasingly reported adverse effects of lipid rescue, it’s reasonable to strictly limit its use in clinical practice. We would not recommend it in oral poisonings.
Introduction
In 1998, Weinberg et al. reported results from an experimental study that indicated reduced bupivacaine toxicity by the administration of intravenous lipid emulsion (ILE) in rats. 1 The first patient with local anesthetic systemic toxicity (LAST) to be ILE treated with alleged successful effect was reported in 2006 and the first patient treated because of an oral overdose was reported in 2008. 2,3 Since these publications, the use of ILE as an antidote (lipid rescue) has increased dramatically. Starting in Great Britain in 2007, anesthesia associations and societies in several countries have launched guidelines regarding the use of 20% lipid emulsion in severe LAST. 4 The American College of Medical Toxicology published a guidance statement regarding lipid resuscitation therapy in 2011. 5 Recently, two systematic reviews from the international expert team “Lipid Emulsion Therapy Workgroup” were published. 6,7 The review on ILE for LAST concluded that lipid rescue appears to be effective in some cases of LAST, but there is currently no convincing evidence showing that lipid rescue is more effective than vasopressors. 6 The review on ILE for non-local anesthetic toxicity (oral poisonings) concluded that the quality of evidence for lipid rescue being an effective antidote in these scenarios remains low to very low. 7 There was no recommendation given regarding indications for lipid rescue in neither of the articles. The aim of this study is to present a systematic review and case analysis of practically all published reports on humans treated with lipid rescue for LAST or oral poisoning.
Methods
Web of science and PubMed were used for the literature search. Specific mesh terms such as “lipid therapy,” “intravenous lipid emulsion,” and “lipid rescue” were used. This yielded 5374 articles. To limit the search, we used the following predefined criteria: original articles or abstracts, 1998 to November 14, 2015, English language, and ILE used as antidote in humans. This resulted in 195 articles that were chosen for further analyses. Two experts (both clinical toxicologists and experienced intensivists, Sune Forsberg (SF)/Jonas Höjer (JH)) independently reviewed the articles using a modified version of WHO-UMC causality categories. 8 This is a six-graded assessment scale that combines clinical and pharmacological aspects with the quality of documentation. As this scale was developed for assessment of adverse effects of pharmaceuticals, it was modified for evaluation of the effects of ILE used as an antidote (Table 1). The reviewers determined the probability for a causal connection between lipid rescue and improved symptoms in each case. A modified WHO-UMC score of 1 = A certain causal connection, 2 = Probable, 3 = Possible, and 4 = Unlikely causal connection. A score of 5 implies that no positive effect of ILE was reported. The cases who received a score of 5 were included in the study but not used in the statistical analyses of the WHO-UMC scores. Finally, cases with a score of 6 were excluded from the study. If the two experts had scored any case differently, consensus was obtained through discussion.
Modified WHO-UMC causality categories

Because of the commonly discussed lipid sink theory as a possible mechanism of action for lipid rescue, log p-values were identified for all main toxic substances involved. In a majority of the included cases, a mixture of toxic symptoms and signs were reported. The reviewing experts evaluated which main symptom most probably had led to the decision of giving lipid rescue. Seizures, unconsciousness, and unspecified neurological symptoms were all classified as neurological symptoms. Arrhythmias and significant widening of QRS complexes (>120 ms) were classified as arrhythmias. Ventricular fibrillation, pulseless electric activity, and asystole were classified as cardiac arrest. In patients poisoned by several drugs, the reviewers marked one as the main toxic substance. Pertinent data such as patient description, main toxic substance and its log p-value, main symptom, WHO-UMC score, other resuscitative treatments given contemporary with lipid rescue, and outcome were extracted from each case report with alleged positive effect of the ILE therapy.
Statistical methods
All variables were summarized with standard descriptive statistics such as mean, standard deviation, and frequency. Definite efficacy according to the modified version of the WHO-UMC causality categories was observed in only three cases. In the statistical analyses, this class was, thus, collapsed with the “probable” class. The statistical analyses were performed with parametric methods, one-way analysis of variance or Student’s t-test for group comparisons. The marker for the fat solubility of a toxic substance, the log p-value, was available for 128 of the 130 positive cases and was negatively distributed and therefore analyzed with the Kruskall–Wallis H test. The significant level in all analyses was 5%.
Results
The literature search yielded 195 publications. After exclusion of all cases that received a WHO-UMC score of 6, 164 cases of poisoning treated with lipid rescue remained. Four of these cases were parenteral poisonings with toxicants other than local anesthetics, wherefore they were excluded as well. In 30 of the finally included 160 cases (19%), no positive effect of lipid rescue was reported (WHO-UMC score of 5). Among the 130 included cases with alleged positive effect of lipid rescue (WHO-UMC score of 1–4), 94 were oral poisonings (72%) and 36 were cases with LAST (28%). The average age of the 160 included patients was 41 years (range: newborn to 92 years) and 58 percent 93 were women (58%). There were 10 children below the age of 11. Nineteen patients (12%) expired during the hospital course.
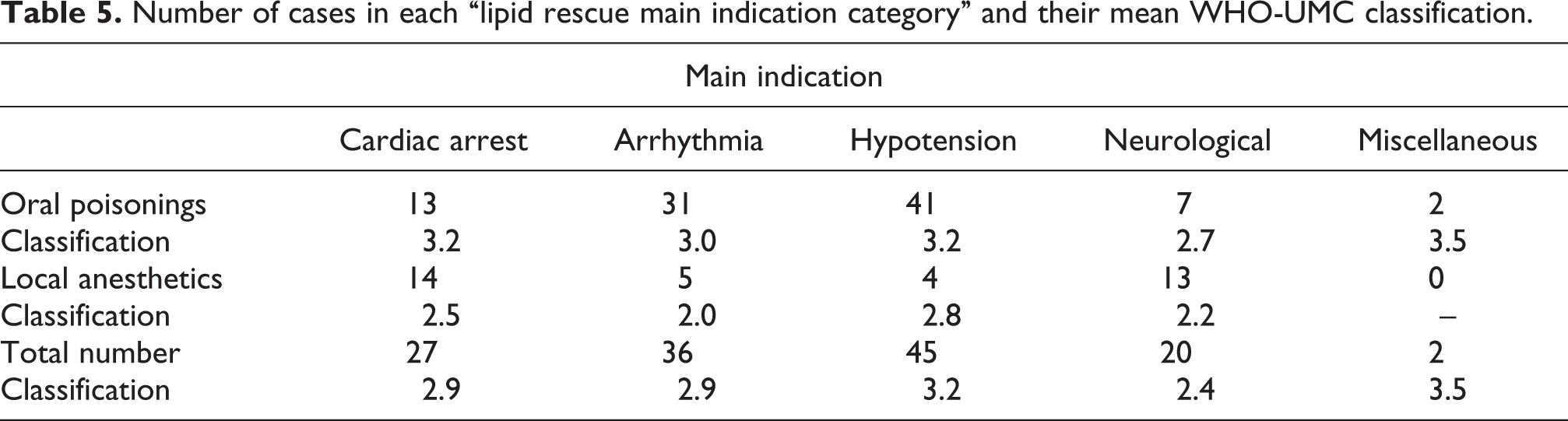
The most common main toxic substances among the oral poisonings were tricyclic antidepressants, calcium channel blockers, antiarrhythmics, and beta blockers, while bupivacaine and ropivacaine were most common in the cases with LAST (Table 2). The two experts’ initial WHO-UMC classification was identical in 83 of the 130 alleged positive cases (64%), and consensus was reached in the remaining 47 cases. The disagreement in the latter 47 cases was never greater than one WHO-UMC category. The result of the experts WHO-UMC scoring is demonstrated in Table 3. Three cases with LAST received a score of 1 (certain causal connection), but all oral poisonings received a score of 2, 3, or 4. The mean WHO-UMC score among the cases with LAST (2.3) was significantly lower than the corresponding mean score among the oral poisonings (3.1). Table 3 also shows that the average log p-value of the main toxins among the cases with LAST was significantly higher than the corresponding log p-value among the oral poisonings. A vast majority of all cases had received some other resuscitative treatment more or less simultaneously with lipid rescue, namely in 72% of the cases with LAST and in 91% of the oral poisonings as seen in Table 4. The main indications for lipid rescue in the respective groups are shown in Table 5. It can be noted that in 22 of the total 130 cases (17%), the main indication was not of a cardiovascular nature. Literature references of the 30 negative case reports as well as patient description, main toxic substance, log p-value, main symptom, WHO-UMC score, other resuscitative treatments given contemporary with lipid rescue, reported effect of ILE, outcome, and literature citation of each of the 130 cases with alleged positive effect of ILE therapy are shown in Online Appendices 1 and 2.
Main toxic substances among the 94 oral poisonings and the 36 accidents with local anesthetics.a

aThe mean WHO-UMC classification for each toxin group.
Total numbers of oral cases and cases with LAST.a
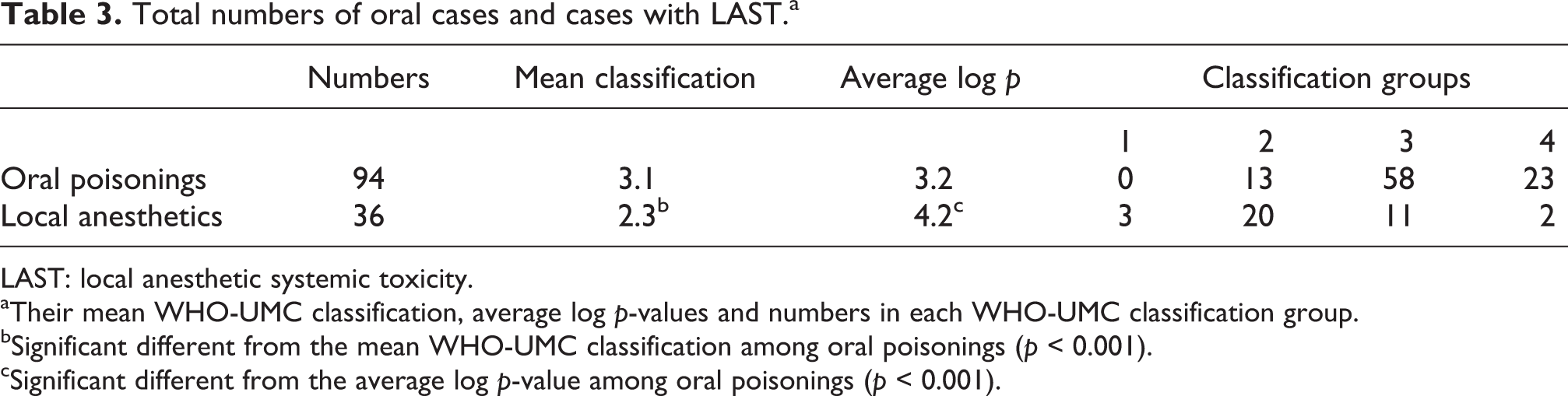
LAST: local anesthetic systemic toxicity.
aTheir mean WHO-UMC classification, average log p-values and numbers in each WHO-UMC classification group.
bSignificant different from the mean WHO-UMC classification among oral poisonings (p < 0.001).
cSignificant different from the average log p-value among oral poisonings (p < 0.001).
Total numbers of oral cases and cases with LAST in which lipid rescue was the only treatment given.a

LAST: local anesthetic systemic toxicity.
aThe mean WHO-UMC classification for each group.
Number of cases in each “lipid rescue main indication category” and their mean WHO-UMC classification.
Discussion
Before evaluating the main findings of this study, one should consider the importance of two well-known realities, namely the immense impact of publication bias and the fact that poisoning-induced signs and symptoms often rapidly vanish spontaneously or after established therapeutic measures. The latter is particularly obvious in cases of LAST where the toxin has been administrated parenterally. Despite this, no or negative effects of the lipid rescue administration were reported in 19% of the 160 included cases. Another important finding was that an overwhelming majority of the 130 alleged positive cases had received other treatments, such as catecholamines, high-dose insulin–euglycaemia, or sodium bicarbonate, more or less simultaneously with lipid rescue as shown in Table 4. Regarding the experts evaluation of a causal connection between lipid rescue and improved symptoms among the alleged positive cases, it may be concluded from Table 3 that 86% of the 94 oral poisonings received a score of 3 or 4, that is, a possible or unlikely causal connection. The mean WHO-UMC classification among the 36 cases of LAST was significantly better, even though only three cases received a score of 1. The initially proposed lipid sink theory as an antidotal mechanism of lipid rescue was readily assimilated but has later been questioned. Nevertheless, it may be noted from Table 3 that the ingested main toxins among the oral poisonings were on average less lipophilic than the local anesthetics involved in the LAST group. Table 5 shows that the main indications for the administration of lipid rescue among the alleged positive cases in this study were very diverse.
The present study comprises practically all published cases up to November 14, 2015, in which ILE has been used as an antidote. Seventy-two percent of these cases consisted of oral poisonings, despite the fact that lipid rescue originally was recommended only for cases of severe LAST. During the recent decade, a sliding of the indications for lipid rescue has obviously occurred in clinical praxis. Nowadays, it is not uncommon that emergency physicians give lipid rescue to patients who have overdosed on a lipophilic drug orally, despite the total lack of scientific support in this scenario. In fact, controlled experimental studies have shown worse outcome in orally poisoned animals given lipid rescue. 9,10 The enthusiasm for lipid rescue has reached a point when lipid emulsion is sometimes given as first-line therapy to patients with only moderate toxic symptoms after ingestion of modest toxic doses of lipophilic drugs. 11 If lipid rescue would be regarded as a primary therapy in patients with life-threatening symptoms, there is a risk that it steals valuable time from established potentially life-saving therapies.
Adverse effects of lipid rescue have been largely ignored but increasingly reported. This study was not designed to investigate this issue, but according to recent publications, side effects of lipid rescue have been shown to be a significant problem. Valuable laboratory analyses, such as glucose, electrolytes, and acid–base status, have not been possible to perform during several hours after the administration of lipid rescue. 12 –14 Further, lipid rescue has been associated with the development of pancreatitis, severe pulmonary injury in the form of ARDS, and of deep venous thrombosis. 11,13 –15 The use of extracorporeal membrane oxygenation after or during lipid rescue may be associated with fat deposition in the VA-ECMO circuits and increased blood clot formation. 16 It has also been repeatedly reported that lipid rescue has rendered renal replacement therapy impossible. 14,17,18 Moreover, Cole et al. reported two orally intoxicated patients who got cardiac arrest immediately after the lipid rescue bolus and finally had fatal outcomes. 19 According to a recent systematic review of clinical adverse events after lipid rescue, such events seemed to be proportional to the rate of ILE as well as to the total dose. 20
Limitations
In this systematic review, not only full case reports but also published abstracts were included. On the other hand, in accordance with the used modified WHO-UMC causality scoring system, all cases with low quality of the reported data were excluded. The use of the WHO-UMC causality system may be questioned, as this scale was not developed for assessment of treatments of poisonings but for adverse effects of pharmaceuticals. However, no scoring system specifically developed for assessment of poisonings is available, why also other authors have used the WHO-UMC causality categories in similar situations. 21
Conclusion
Considering the findings of the present study, the weak and contradictory scientific evidence for lipid rescue being an effective antidote and its increasingly reported adverse effects, it is reasonable to strictly limit its use in clinical practice. 6,7,20,22 We would not recommend its use at all in cases of oral poisoning.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.