
Abstract
Skin sensitization associated with allergic contact dermatitis is a common health problem and is an important consideration for toxicologists in safety assessment. Historically, in vivo predictive tests have been used with good success to identify substances that have the potential to induce skin sensitization, and these tests formed the basis of safety evaluation. These original tests are now being replaced gradually either by in vitro assays or by further refinements of in vivo methods such as the local lymph node assay. Human data have also been available to inform classification decisions for some substances and have been used by risk managers to introduce measures for exposure reduction. However, humans encounter hazards in the context of exposure rather than in the form of intrinsic hazards per se, and so in this article, we have examined critically the extent to which human data have been used to refine classification decisions and safety evaluations. We have also evaluated information on the burden of human allergic skin disease and used this to address the question of whether, and to what extent, the identification and evaluation of skin sensitization hazards has led to an improvement of public and/or occupational health.
Keywords
Introduction
Within the orbit of toxicology, it is probably skin sensitization and its association with allergic contact dermatitis (ACD) where the relationship between exposure and adverse health effects is most apparent and that best exemplifies the tenet of Paracelsus (1493–1541) that the dose makes the poison. The clinical condition of ACD is characterized by redness, swelling and itch and when the reaction is severe by blistering. Contact dermatitis per se can be readily subdivided into two main forms, irritant contact dermatitis (ICD) and ACD). The former results from the damage caused by direct interaction of chemical with the skin, often associated with disruption of normal barrier function, and is independent of a requirement for immune activation. 1 In contrast, ACD is driven by a form of delayed-type hypersensitivity reaction resulting from prior immunological priming (sensitization) to the inducing contact allergen. A detailed consideration of the mechanisms involved in ICD and ACD is beyond the scope of this article, but excellent recent reviews are available elsewhere. 2,3 The causative chemicals associated with ICD and ACD, often referred to as skin irritants and skin sensitizers respectively, are generally well known. 4,5 It is worth mentioning that the chemicals that give rise to these effects may overlap since a chemical may possess both irritant and allergenic properties (to varying degrees), but in addition it is also well known, clinically and experimentally, that the presence of irritation is an important cofactor for the acquisition (induction) of this type of allergy.6,7
In this review, the focus is on skin-sensitizing chemicals and their ultimate expression of adverse effects in humans, that is, ACD. This skin disease represents an important cause of occupational dermatitis and, taken together with occupational ICD, represents quite probably the largest single cause of occupational disease. 1,8 –10 However, ACD also occurs widely in the general population, as evidenced by recent epidemiological data that suggest that up to 25% of European adults are sensitized to at least one contact allergen. 11 In fact, several thousand substances have now been identified as known or suspected skin sensitizers. 12 It appears from retrospective analyses of regulatory data that a substantial minority, perhaps up to a third, of chemicals may possess this intrinsic hazard to a greater or lesser extent. 13,14 The epidemiology of ACD (i.e. the expressed disease) is less well characterized compared with contact allergy (the sensitized state identified via a diagnostic patch test). Whilst it is the case that the prevalence of immunologically mediated eczema is much lower than the prevalence of contact allergy, the state of being sensitized persists, only awaiting sufficient new dermal exposure to trigger an ACD.
The diagnosis of ICD and ACD has some similarities, but there is one important difference. In the case of ICD, diagnosis is frequently one of the exclusion of other possibilities, whereas for ACD there is a specific diagnostic test. 15 Clinical inspection of the involved skin sites and taking an appropriate medical history are common to both, but for ACD, substances that are suspected of causing the allergic skin reaction can be applied under patches to the skin of the back in a standardized way to determine whether an individual patient has acquired sensitivity to one or more chemicals. 15 As a consequence, uniquely in toxicology, it is possible to make the connection between intrinsic hazard and the expressed risk, both at an individual level and, by collation of patient data, at a population level. Importantly, because of the involvement of the immune system, the expression of the human risk can be interrogated both at the level of the induction of skin sensitization (contact allergy) and at the level of the expression of the adverse health effect (ACD).
The purpose of this review is not to discuss the mechanism of toxicity (or as it has become more popularly known ‘adverse outcome pathway’) nor to review in any detail the causative chemicals. What is of interest to us is the opportunity, possibly unique in toxicology, to access the substantial quantity of human data on the sensitization end points of contact allergy and ACD, to relate such information to the causative chemicals and then to use this knowledge to refine the toxicological process of hazard identification, characterization and risk assessment, including all areas of regulatory toxicology so that opportunities for the protection of human health are optimized. Since it will not be possible to discuss all global toxicology regulations, neither to consider all potential areas of safety assessment, attention will be focused on two key examples: the Registration, Evaluation, Authorisation and Restriction of Chemicals (REACH)/Globally Harmonized System (GHS) regulatory arena and cosmetic safety evaluation. 16,17 It is intended that the examples derived from those two areas are to be taken as broadly applicable to any area of regulation and safety assessment.
Skin sensitization hazard identification and characterization
The toxicology of skin sensitization commences with efforts to identify whether a substance possesses this intrinsic hazard. Predictive methods have been available for decades and have been reviewed in detail previously. 18 –21 Using methods in the guinea pig and the mouse, extensive lists of the results of testing of many hundreds of chemicals for skin sensitization potential have been published. 22 –25 In addition, these methods have been adopted into European regulatory classification systems as well as into the United Nations GHS. 16,26,27 By means of these regulatory systems, large numbers of chemical substances have been formally classified as skin sensitizers.28,29
Where a chemical has been identified as a skin sensitization hazard, the important next step is to characterize that hazard in terms of its relative potency. Of the common in vivo assays, only one, the murine local lymph node assay (LLNA) has been developed not only to identify hazard but also to offer a quantitative measure of relative sensitization potency. 30,31 The forthcoming in vitro alternatives currently will replace hazard identification in vivo but will not offer this type of potency information. 32 –35 Intensive research is underway to address this limitation of the in vitro portfolio. 32,36,37 Quantitative information on the potency of the sensitizer can be used as the basis for human risk assessment, with detailed guidelines for how this may be achieved having been promulgated. 38 –40
In response to the above question, firstly, it is evident that predictive assays in the mouse and the guinea pig have had considerable success in the identification of substances that are known to cause contact allergy in humans. 22 –25,41 There are situations where substances known to cause contact allergy in humans have proven to being negative in predictive tests, but generally these have arisen either because of suspected inadequate test conduct (examples include methyldibromo glutaronitrile and methylisothiazolinone (MI)) or because of substances termed ‘non-sensitizers’, which in reality represent the examples where the cut-off for regulatory classification and labelling of the sensitizer can be shown to be due to that cut-off representing a higher threshold than that actually found in practice in humans. 41,42 Figure 1 endeavours to characterize this situation in a generic form for skin sensitization.

An overview of regulatory classification for skin irritants and sensitizers.
Human data can be used in relation to regulatory classification, and detailed guidance on this has been published. 27,43 Various types of data exist, including historical experimental information (new experimental testing is not allowed for regulatory purposes) as well as results of clinical investigations. These may point to the presence or absence of skin sensitization hazards, and if the quality of information is sufficient, it may even suggest whether the potency is in a higher or a lower category (Figure 1). Generally, such information does not exist for most chemicals; where it does, it can override false negative in vivo data (e.g. nickel) or help to demonstrate that a substance is false positive (e.g. sodium lauryl sulphate). Detailed discussion of this topic, with several examples, has been published elsewhere.44–47
Clinical data on skin sensitization
Hazard identification and characterization are only the initial steps in ensuring human safety. Consequently, it is interesting to interrogate the available human evidence concerning ACD since if it is accepted that hazard identification for skin sensitization and subsequent potency characterization is sufficient and properly applied to assess the risk, then really it should be apparent and since the advent of these methods that the burden of human skin disease has been either eliminated or at least substantially demonstrably decreased. For ACD, although there do not exist decades of epidemiological investigation in the general population, there do exist substantial accumulations of dermatology clinic data in which a large number of eczema patients have been evaluated with a well-standardized procedure, the diagnostic patch test. 15,48 The history, general principles and practices of such patch testing can be found elsewhere. 49 In brief, they involve application of common and suspected sensitizers to the back of the patient for 2 days, followed by removal and reading of skin reactions over the subsequent 2–5 days. The most frequent substances known to cause ACD in humans are collected in a baseline (or ‘standard’) series. Therefore, the first indication of whether hazard identification regulatory classification and labelling have had any impact on disease could be to ask whether that standard series has changed significantly since it was first detailed four decades ago. 50 Table 1 shows that of the original 20 materials, even 40 years later some 75% of the substances remained.
Standard series in 1974 versus 2014.
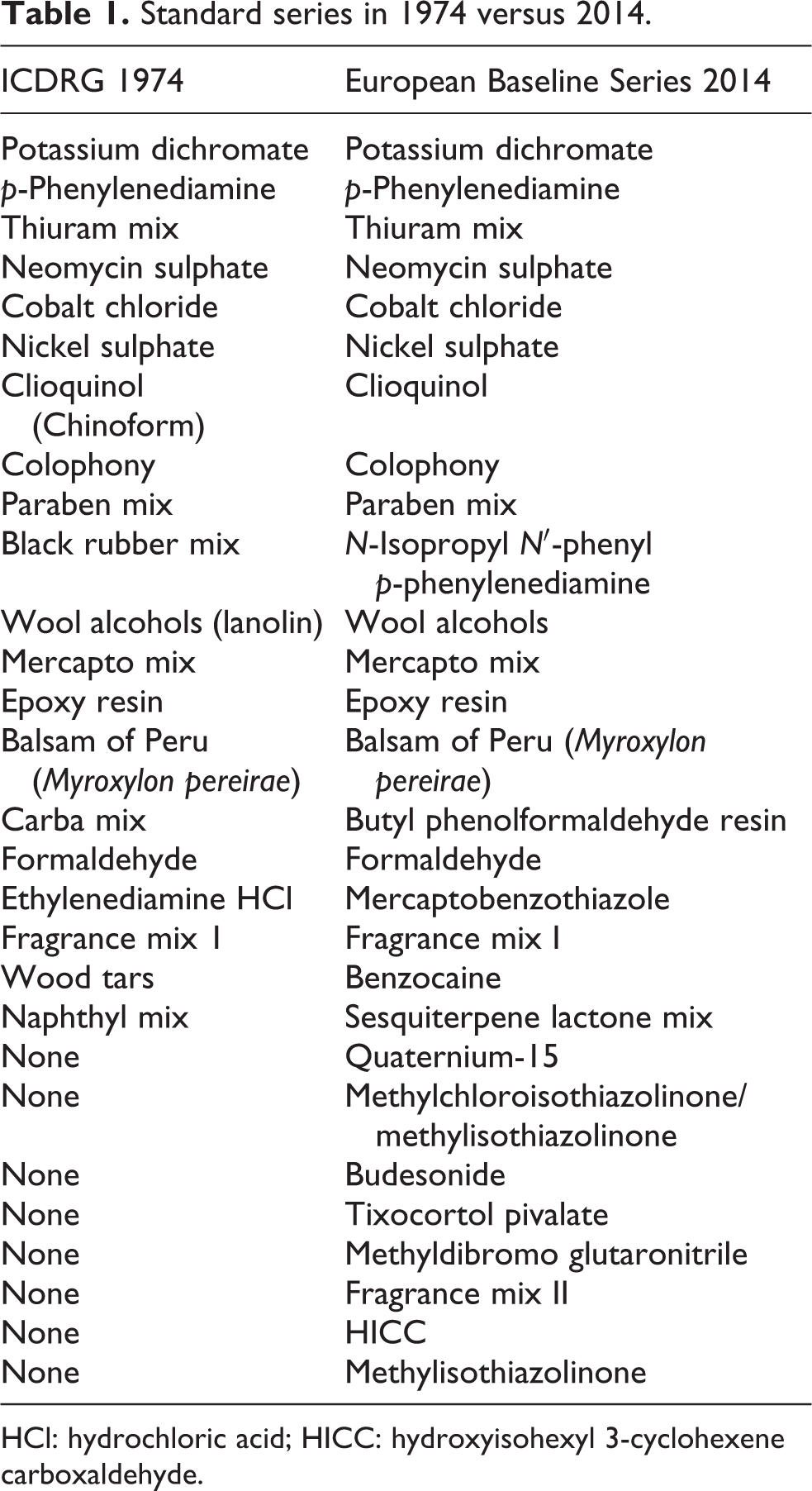
HCl: hydrochloric acid; HICC: hydroxyisohexyl 3-cyclohexene carboxaldehyde.
Another measure of the impact of the (regulatory) toxicological processes is to ask whether the frequency of positive reactions to known common contact allergens has changed over the last few decades. An exhaustive review of the extensive published data on this topic is beyond the scope of this work, but some examples may serve to illustrate the situation. The North American contact dermatitis group regularly published collated diagnostic patch test data (Table 2). 51,52 The number of contact allergens tested in the earlier period was much lower, but for the 15 where a direct comparison can be made, it is evident that the passage of more than a quarter of a century has not been associated with a general reduction in the rates of response to these common sensitizers. A sample of data from Europe is displayed in Table 3, which contains results from a French baseline series applied in 1991 and 2011. 53 Clearly, some contact allergens are less common at the later time point, for example, neomycin, probably through its decreased use, and formaldehyde, probably because it is a less popular preservative in the 21st century. Other contact allergens have become more frequent, for example, epoxy resin, but the rate of response to the majority has remained relatively static. Of special note are nickel and potassium dichromate, both subject to European Union (EU) regulation 54,55 These are still common, at least in this French dermatology clinic, and allergens such as the preservative methylchloroisothiazolinone/MI, the hair dye p-phenylenediamine (PPD) and fragrance, all ostensibly controlled by aspects of cosmetic regulation but persistently delivering a frequency of contact allergy in excess of what many would judge to be acceptable. Similar examples of the frequency of contact allergy and its change with time can be found from collated Danish data and the results from London concerning fragrance allergy (Figure 2).56,57
North American contact dermatitis group results.

HCl: HCl: hydrochloric acid.
aAdapted from Rudner et al. 51
bAdapted from Warshaw et al. 52
An example of European diagnostic patch test results.a

MCI: methylchloroisothiazolinone; MI: methylisothiazolinone; PPD: p-phenylenediamine; IPPD: N-isopropyl-N′-phenyl-p-phenylenediamine; PTBP: p-tert-butylphenol formaldehyde.
aData adapted from the work by Schoeffler et al. 53

What evidence is available on the overall burden of ACD in occupational or consumer settings? As mentioned above, epidemiological data on the extent of ACD in the general population are, at best, sparse. 58,59 There has however been some evaluation of the extent of the induction of contact allergy, where there are four primary sources of information – a Danish epidemiology study in 1990 with follow-up in 1998; 60,61 a statistically based extrapolation from extensive German survey 62 and Danish survey; 63 and most recently a multicentre European study involving six countries. 64
In the original Danish study, a frequency of 15.2% of positive contact allergy was identified in a random sample of the general population. Some 6.7% were positive to nickel, with fragrance allergy occurring in approximately 1%. 60 Follow-up 8 yearslater demonstrated that new contact allergies had developed, notably to nickel (6%) and to fragrance, where the prevalence of responses to the original fragrance mix (FM1) had effectively doubled to 2%. 61 Such figures are consistent with the later prediction model extrapolating from clinical patients, indicating a 10-year prevalence of up to 1.7% contact allergy to fragrance. 62 Across all contact allergens, the 10-year prevalence for Danish adults was approximately 10%. Similar figures were obtained for Germany, with the worst case prediction being 16.6%. 63 In the light of such figures, it is interesting to note that the prevalence of contact allergy in the general adult population of six European countries has been reported recently to be the order of 20% to 25%. 64
An illustrative example – MI
MI has been selected as a suitable example due to its recent prominence as a cause of ACD. 42,65,66 MI itself has been recognized as a skin sensitizer for decades, being a component of a preservative system long associated with ACD. 67 Since then, evaluation of MI in the LLNA demonstrated it was sensitizing and confirmed that its potency was in the higher category for classification and labelling (an EC3 value of <2.0%). 27,68,69 In the last 10 years, use of MI alone as preservative has become much more common. In cosmetics, use was restricted to a maximum of 100 ppm in all product categories, but this opinion has been revised recently. 70 However, the absence of classification and labelling of all other types of product, including medicines, meant that the use of MI was limited largely by commercial considerations. What transpired was the greatest epidemic of contact allergy seen in the 21st century, this despite validated predictive toxicology methods, new quantitative risk assessment tools and long-standing EU legislative strategy for classification and labelling of skin sensitizing substances and the preparations that contain them. 16 At the time of writing this review, the MI epidemic is almost 3 years old, but except for updated guidance from the European trade association for the cosmetics industry (Cosmetics Europe) detailing that MI should not be used in leave on products (the statement dated 12 December 2013 can be downloaded from https://www.cosmeticseurope.eu/news-a-events/statements.html), no legislative action in any product category has been proposed nor has even basic classification and labelling been implemented.
Given the above, what has gone wrong with MI and how can it inform for the future? Firstly, classification and labelling are of zero value if not used – although it is worth noting that for MI, this would only impose labelling if the level of use was at least 0.1%, with a warning if the level was between 0.1% and 0.01% (i.e. above 100 ppm). This is unhelpful when it is already widely known that levels below this induce contact allergy and elicit ACD. Regarding cosmetics, it may be more appropriate in future to allow new preservatives only in rinse-off products for an initial period of 5–10 years. However, ultimately, what is really required is full ingredient information for all products (consumer and occupational), widespread adoption of quantitative risk assessment for products prior to marketing and rapid reaction to feedback from the dermatology community in response to information on emerging contact allergy. 43
Discussion
The important questions that need to be addressed are whether, and to what extent, hazard identification and risk assessment processes, including regulatory classification and labelling, can be shown to have had an impact on the human disease burden, expressed as ACD. In reality, the simple answer to all is ‘none’. The only regulations that can be shown to have had impact have been those focused on ‘cleaning up’ after a major health problem has been identified. Future action needs to be focused on prevention, not cure. The requirements for progress to be made in achieving this end, which will affect both the determination of hazard and the management of risk have been identified in this article.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.