We aimed to investigate the possible roles of nitric oxide (NO) and endothelin on the changes of cardiac muscle function in both hyper- and hypodynamic septic shock periods. Cecal ligation and puncture was performed in 50 Wistar albino rats to induce septic shock. Changes in atrium and right ventricle papillary muscle contractions, atrium beat rate, adrenergic and cholinergic responses in these tissues were evaluated in vitro. Atrium beat rate increased in hypodynamic period (p < 0.001) that was reversed by bosentan (p < 0.001) and NG-nitro-l-arginine methylester (l-NAME; p < 0.05). Atrium contractions decreased in both hyper- and hypodynamic periods (p < 0.001) that were partially ameliorated by bosentan in both periods (p < 0.01) and only in hypodynamic period by l-NAME (p < 0.001). l-NAME increased papillary muscle contractions in both periods (p < 0.01), but bosentan increased it only in hyperdynamic period (p < 0.01). Bosentan and l-NAME increased potency of isoproterenol on atrium beat rate in both periods and increased carbachol potency on atrium beat rate and atrium contraction amplitude only in hypodynamic period. Bosentan increased atrium contraction response to isoproterenol in hypodynamic period (p < 0.05). Papillary muscle contraction response to isoproterenol increased in hypodynamic period (p < 0.05). l-NAME increased papillary muscle contraction response to carbachol in both periods (p < 0.01, p < 0.05, respectively). These results show that NO and endothelin may play a role in positive inotropic and negative chronotropic effects for atrium in septic shock. Bosentan and l-NAME may change potency and efficacy of isoproterenol and carbachol via upregulation of adrenergic and cholinergic receptors and/or through post receptor factors.
Sepsis, severe sepsis (sepsis with organ dysfunction), and septic shock (sepsis with hypotension despite adequate fluid resuscitation) are serious public health problems that have fatal processes with high mortality rates of 30%, 50%, and 80%, respectively.1,2 It is the 10th leading cause of all deaths and occurs 0.3% in the United States.3,4
Inflammatory mediators, cytokines, and free radicals are necessary for the elimination of microorganisms, however, if the number of microorganisms increases massively as observed in sepsis, these substances also increase massive/uncontrolled and cause organ damage. These substances activate coagulation, free radicals directly damage the vessels, and so disseminated intravascular coagulation occurs that leads to hypoperfusion in many vital organs including heart, brain, liver, kidney, and lung.5,6
Nitric oxide (NO) and endothelin are two mediators derivating from vascular endothelium and have critical roles in septic shock. They are responsible for the formation of two successive and opposite features of septic shock periods: hyperdynamic and hypodynamic periods.7,8 After endotoxin infusion or cecal ligation and puncture (CLP), excessive NO leads to vasodilatation, decreases peripheral vascular resistance (PVR), and increases cardiac output (CO), which is named as hyperdynamic (“early,” “warm,” or “compassed”) period.9 Excessive production of endothelin leads to vasoconstriction, decreases CO,10 increases vascular resistance and vascular permeability, and causes fluid flux into the extravascular space, which is named as hypodynamic (“late,” “cold,” or “decompassed”) period.11 Thus, drugs that reduce the effects of NO and endothelin have been the subject of numerous sepsis studies. NG-nitro-l-arginine methylester (l-NAME) is a nonselective NO synthase inhibitor that increases mesenteric blood flow12 without any effect on survival,13 increases organ damage such as liver, kidney, and spleen,14 reduces CO, increases heart rate,15 and increases PVR and systemic vascular resistance (SVR) in septic shock. Bosentan is a nonselective endothelin receptor antagonist that has been shown to significantly prolong the survival,16 increase mesenteric blood flow8 and ameliorate organ damage such as liver, kidney, and spleen, increase CO, decrease PVR and SVR, but does not affect heart rate16 in septic shock.
Intraperitoneal (i.p.) injection of lipopolysaccharide (LPS) and CLP are the two widely used models of experimental septic shock. In this study, CLP model was chosen because CLP model mimics clinical conditions and hyper- and hypodynamic periods can be observed separately.17,18
Although changes in heart rate, cardiac contractility, and adrenergic and cholinergic responses of cardiac muscles in septic shock were shown usually by endotoxemia models in vivo,15,19 the roles of NO and endothelin in cardiac function changes in hyper- and hypodynamic septic shock periods are unclear. Thus, in this study, it is aimed to investigate the cardiac muscle function changes in septic shock periods using an experimental model of septic shock with CLP in vitro.
Materials and methods
Fifty male Wistar albino rats (weighing 200–300 g) obtained from the animal shelter of Department of Medical Pharmacology, Faculty of Medicine, Hacettepe University, Ankara, Turkey, were used in this study. The rats were fed with standard laboratory pellet dairy chow and water ad libitum at 21 ± 2°C temperature, 30–70% relative humidity, and 12-h dark/12-h light cycle. This study was performed in accordance with the recommendations of the Guide for the Care and Use of Laboratory Animals. It was approved by the Animal Care Committee at Hacettepe University Faculty of Medicine (approval number 2013/42-01).
Experimental protocols
Animals were allocated into seven groups as control, c4 (hyperdynamic period; tissues were isolated 4 h after the CLP), c20 (hypodynamic period; tissues were isolated 20 h after the CLP), and bosentan- or l-NAME-treated groups (c4 + bosentan, c4 + l-NAME, c20 + bosentan, and c20 + l-NAME).
Polymicrobial sepsis model
Polymicrobial sepsis was induced by CLP as described in previous studies (Hubbard et al., 2005; Yang et al., 2002).33 Rats were fasted overnight, but were allowed ad libitum access to drinking water before the experiment. The animals were anesthetized with chloral hydrate (400 mg/kg, i.p.), the cecum was exposed, and then ligated just below the ileocecal valve and punctured twice with an 18-gauge needle. A small amount of fecal material expelled via gentle massage of cecum. After the operation, normal saline (3 mL/100 g, subcutaneously) was injected immediately in the nape of the neck. Animals in treatment groups were given bosentan (30 mg/kg, i.p.) or l-NAME (10 mg/kg, i.p.) 2 h after the CLP.
Isometric measurements
Rats were anesthetized with diethyl ether without any other additional drug administration in the control group (n = 7); 4 h after the CLP in the c4 (n = 7), c4 + bosentan (n = 7), and c4 + l-NAME (n = 6) groups; and 20 h after the CLP in the c20 (n = 7), c20 + bosentan (n = 9), and c20 + l-NAME (n = 6) groups. Some of the test parameters could not be evaluated in all of the rats mentioned above due to the experimental procedure. The n values for each subsections were given separately in the table and figure legends for different test parameters. Both carotid arteries of the anesthetized rats were bled, the chest cavity was opened, and heart was removed. Then, right ventricle papillary muscle and spontaneous beating atrium were excised and isolated in a modified Krebs Henseleit solution (as mM; sodium chloride 118, sodium bicarbonate 25, potassium chloride 4.7, calcium chloride 2, magnesium sulfate 1.2, monopotassium dihydrogen phosphate 1.2, and glucose 10) aerated with 95% oxygen and 5% carbon dioxide at 4°C. The isolated atria and papillary muscles were suspended vertically into isometric force transducers under 0.5–0.75 g resting tensions in 10 mL glass chambers of the organ bath (MP150 from BIOPAC, Goleta, California, USA). Since the papillary muscle has no spontaneous contraction, its contraction amplitude was recorded under electrical field stimulation at 1 pulse per second (pps), 2 millisecond (ms) duration, and 80 volt (V) violence. Tissue preparations were washed every 15 minute (min) with fresh solution. During a 45-min equilibration period, basal atrium and papillary muscle contraction amplitudes and atrium beat rate were recorded. After this period, cumulative concentrations of isoproterenol (10−10 to 3 × 10−5 Molar (M)) were applied into the organ baths. For each concentration of isoproterenol, the increase in recorded beat rate and contraction amplitudes were expressed as a percentage of basal level. After isoproterenol responses, tissues were washed at every 15 min for about 45 min for resting, and then carbachol responses were obtained as isoproterenol responses.
Evaluation of all the parameters for each preparation was not possible for the organ bath experiments. Thus, the number of preparations was different for each parameter, and the number of preparations (n) was defined separately in the results section.
Drugs and chemicals
Bosentan (Ro 47-0203) was kindly provided by Dr Martine Clozel from Actelion, (Allschwill, Switzerland). Chloral hydrate (Merck, Kenilworth, New Jersey, USA), l-NAME (Sigma Chemical Co, St Louis, Missouri, USA), (−)-isoproterenol hydrochloric (Sigma Chemical Co), and carbachol (Sigma Chemical Co) were used in this study. All chemicals were dissolved in distilled water and prepared freshly on the day of the experiment.
Statistical analysis
Data were expressed as mean ± standard error of the mean (mean ± SEM). For statistical analysis, one-way analysis of variance (ANOVA) with post hoc Newman–Keuls multiple comparison posttest or two-way ANOVA with post hoc Bonferroni posttest was used. Half-maximal effective concentration (EC50) values were calculated by nonlinear regression analysis, and the differences between groups were shown by one-way ANOVA with post hoc Newman–Keuls multiple comparison test. Statistical analysis was carried out using the GraphPad Prism 5. Differences were considered to be significant when p < 0.05.
Results
Basal atrium beat rate did not change in hyperdynamic period, but increased from 232 ± 10 beats/min (bpm) to 304 ± 15 bpm in hypodynamic period (31%, p < 0.001). Atrium beat rate was not affected by bosentan and l-NAME treatment in hyperdynamic period, but in hypodynamic period decreased by bosentan (from 304 ± 15 bpm to 227 ± 6 bpm, p < 0.001) and l-NAME (from 304 ± 15 bpm to 271 ± 13 bpm, p < 0.05) treatment (Figure 1(a)). Basal atrium muscle contraction decreased 31% in hyperdynamic and 69% in hypodynamic periods (from 0.64 ± 0.04 g to 0.44 ± 0.02 g and to 0.20 ± 0.001 g, respectively, p < 0.001). While bosentan partially ameliorated atrium contraction in both periods (p < 0.01 for hyperdynamic and p < 0.001 for hypodynamic period), l-NAME partially ameliorated only in hypodynamic period (p < 0.001; Figure 1(b)). Basal papillary muscle contraction did not change in both periods. Papillary muscle contraction was increased from 0.40 ± 0.03 g to 0.85 ± 0.09 g by bosentan only in hyperdynamic period (p < 0.01) and was increased by l-NAME in both hyperdynamic (0.40 ± 0.03 g to 0.97 ± 0.10 g) and hypodynamic (0.42 ± 0.03 g to 0.79 ± 0.09 g) periods (142% increase and p < 0.001 for hyperdynamic and 98% increase and p < 0.01 for hypodynamic). In addition, values that were obtained by l-NAME exceeded the control values in hyperdynamic period (49%, p < 0.05, Figure 1(c)).
Comparison of atrium beat rate (a), atrium muscle contraction (b), and papillary muscle contraction (c) values among all groups. Data were expressed as mean ± SEM. n = 6–7 for the groups in (a) and (b) and n = 6–9 for the groups in (c) (n represents the number of tissues used in the organ bath). *Statistically significant difference between the control versus all groups. #Statistically significant difference between c4 versus c4 + bosentan, c4 + l-NAME and c20 versus c20 + bosentan, c20 + l-NAME groups (*,#p < 0.05; ##p < 0.01; ***,###p < 0.001). l-NAME: NG-nitro-l-arginine methylester.
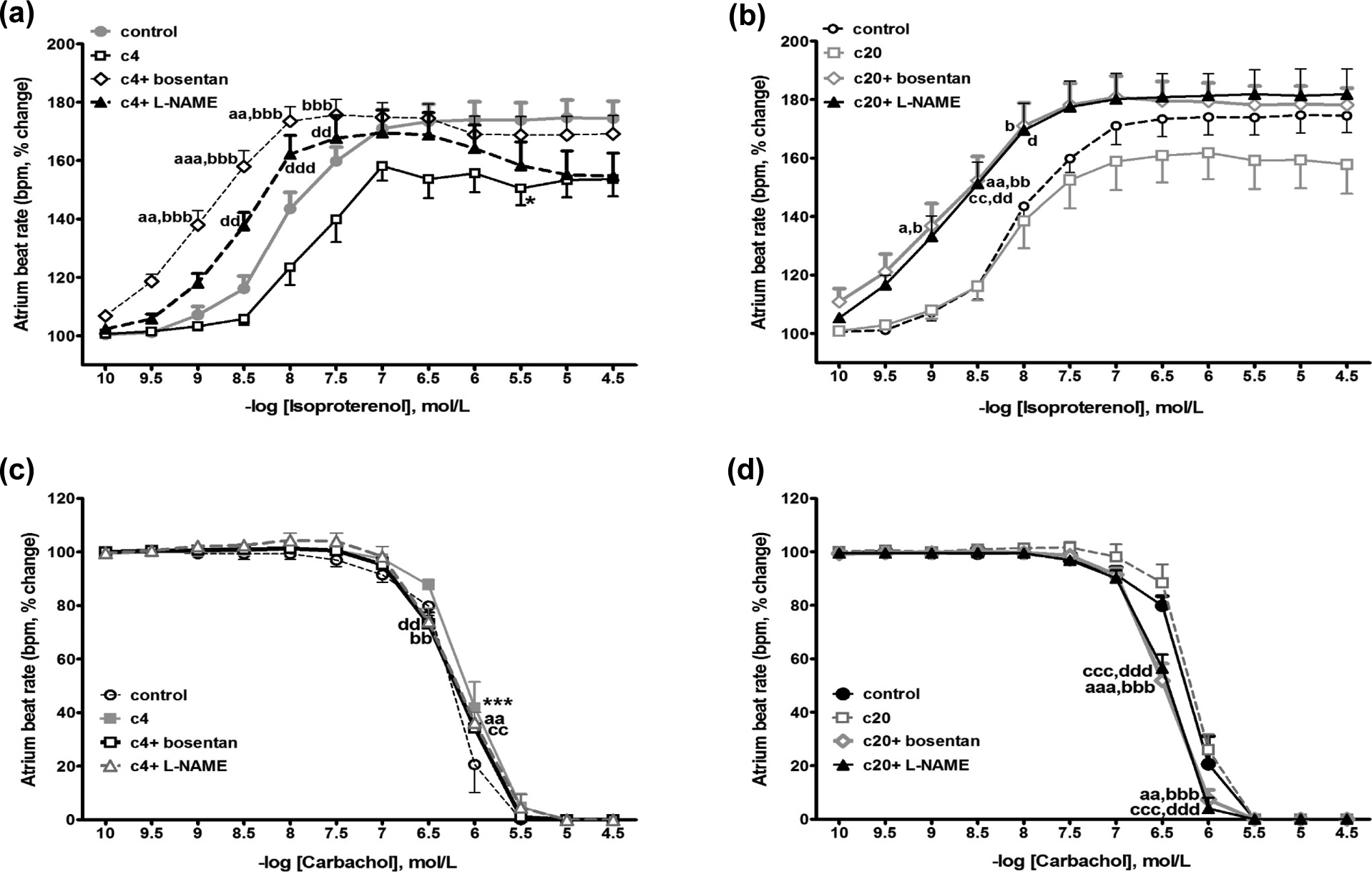
In both periods, potency of isoproterenol on atrium beat rate was increased in bosentan-treated (p < 0.001 for hyperdynamic and p < 0.05 for hypodynamic) and l-NAME-treated (p < 0.01 for hyperdynamic and p < 0.05 for hypodynamic) groups (Figure 2(a) and (b); Table 1), and carbachol potency on atrium beat rate and atrium contraction amplitude were increased only in hypodynamic period in both treated groups (p < 0.01; Figure 2(c) and (d); Table 1). Responses to isoproterenol of atrium muscle contraction amplitudes did not change significantly in hyperdynamic period but increased in bosentan-treated group in hypodynamic period (p < 0.05; Figure 3(a) and (b)). l-NAME didn’t affect this response. Responses to isoproterenol of papillary muscle contraction amplitudes did not change in hyperdynamic period. In hypodynamic period, these responses were increased in both bosentan-treated and nontreated groups (p < 0.05 for nontreated and pretreated groups, p < 0.01 vs. control group; Figure 4(a) and (b)) and responses to carbachol of papillary muscle contraction amplitudes were increased in l-NAME-treated groups in both periods (p < 0.01 for hyperdynamic period and p < 0.05 for hypodynamic period vs. control group; Figure 4(c) and (d)).
Comparison of isoproterenol (a and b) and carbachol (c and d) responses of atrium beat rate in both hyper- and hypodynamic periods. Data were expressed as mean ± SEM. n = 6 for all groups. *Significant difference between control versus c4 and c20 groups. aSignificant difference between control versus c4 + bosentan and c20 + bosentan groups. bSignificant difference between c4 versus c4 + bosentan and c20 versus c20 + bosentan groups. cSignificant difference between control versus c4 + l-NAME and c20 + l-NAME groups. dSignificant difference between c4 versus c4 + l-NAME and c20 versus c20 + l-NAME groups. (*, a, b, dp < 0.05; aa, bb, cc, ddp < 0.01; ***, aaa, bbb, ccc, dddp < 0.001). l-NAME: NG-nitro-l-arginine methylester.
Comparison of −log EC50 values (as an indicator of potency) of isoproterenol and carbachol for the atrium beat rate, atrium contraction, and papillary muscle contraction in the study groups.a
Groups
Atrium beat rate
Atrium contraction
Papillary muscle contraction
Isoproterenol
Carbachol
Isoproterenol
Carbachol
Isoproterenol
Carbachol
Control
8.15 ± 0.14
6.19 ± 0.07
nm
6.37 ± 0.14
7.47 ± 0.37
6.77 ± 0.45
c4
7.89 ± 0.19
5.99 ± 0.09
nm
6.16 ± 0.06
6.95 ± 0.11
6.79 ± 0.43
c20
8.18 ± 0.15
6.13 ± 0.05
nm
6.09 ± 0.09
7.24 ± 0.28
6.11 ± 0.11
c4 + Bosentan
9.16 ± 0.11***,###
6.16 ± 0.03
nm
6.26 ± 0.09
7.89 ± 0.26
6.32 ± 0.07
c4 + l-NAME
8.73 ± 0.14*,##
6.14 ± 0.06
nm
6.50 ± 0.12
7.66 ± 0.09
6.46 ± 0.13
c20 + Bosentan
8.78 ± 0.15*,#
6.45 ± 0.04**,##
nm
6.56 ± 0.11#
7.33 ± 0.05
6.40 ± 0.12
c20 + l-NAME
8.73 ± 0.14*,#
6.44 ± 0.05**,##
nm
6.55 ± 0.08#
7.57 ± 0.14
6.60 ± 0.21
nm: nonmeasurable; EC50: half-maximal effective concentration; l-NAME: NG-nitro-l-arginine methylester; c4: hyperdynamic period, tissues were isolated 4 h after the CLP; c20: hypodynamic period, tissues were isolated 20 h after the CLP.
aData were expressed as mean ± SEM (n = 4–6 for the groups).
*Significant difference between control versus other groups.
#Significant difference between c4 versus c4 + bosentan, c4 + l-NAME, and c20 versus c20 + bosentan, c20 + l-NAME groups.
(*,#p < 0.05; **,##p < 0.01; ***,###p < 0.001).
Comparison of isoproterenol (a and b) and carbachol (c and d) responses of atrium contraction amplitude in both hyper- and hypodynamic periods. Data were expressed as mean ± SEM. n = 6 for all groups. *Significant difference between control versus c4 and c20 groups. aSignificant difference between control versus c4 + bosentan and c20 + bosentan groups. bSignificant difference between c4 versus c4 + bosentan and c20 versus c20 + bosentan groups. cSignificant difference between control versus c4 + l-NAME and c20 + l-NAME groups. dSignificant difference between c4 versus c4 + l-NAME and c20 versus c20 + l-NAME groups (*, b, c, dp < 0.05; **, cc, ddp < 0.01; ***, aaa, bbb, dddp < 0.001). l-NAME: NG-nitro-l-arginine methylester.
Comparison of isoproterenol (a and b) and carbachol (c and d) responses of papillary muscle contraction amplitude in both hyper- and hypodynamic periods. Data were expressed as mean ± SEM. n = 6 for all groups. *Significant difference between control versus c4 and c20 groups. aSignificant difference between control versus c4 + bosentan and c20 + bosentan groups. bSignificant difference between c4 versus c4 + bosentan and c20 versus c20 + bosentan groups. cSignificant difference between control versus c4 + l-NAME and c20 + l-NAME groups. dSignificant difference between c4 versus c4 + l-NAME and c20 versus c20 + l-NAME groups (b, c, dp < 0.05; aa, ddp < 0.01; ***, aaa, dddp < 0.001). l-NAME: NG-nitro-l-arginine methylester.
Discussion
Sepsis is an infectious syndrome that has a progressive and fatal process with increasing incidence. It causes acute failure in many vital organs.1,2,5 NO and endothelin are two main mediators in septic shock that lead to the formation of two successive and opposite features of septic shock states: hyperdynamic and hypodynamic periods.7,8 In this study, it was aimed to investigate the changes in cardiac contractility, atrium beat rate, and adrenergic and cholinergic responses on these parameters and possible roles of NO and endothelin in these changes in septic shock CLP model.
In previous studies, in early and late septic shock periods, the increased heart rate has been shown in both LPS20,21 and CLP22,23 experimental septic shock models in vivo. The increased heart rate was associated with sympathetic hyper activation and some inflammatory mediators that increased in septic shock.24 However, in a CLP study, isolated right atrium beat rate did not change in hypodynamic period. Isolated atrium beat rate did not change and was lower than in vivo heart rate, indicating that there is no basal sympathetic tone in isolated right atrium preparation.20 In that recent study, isolated atrium beat rate was investigated only in hypodynamic period, but we investigated both hyper- and hypodynamic periods separately and evaluated the effects of bosentan and l-NAME on this parameter. In our study, we showed that isolated atrium beat rate did not change in hyperdynamic period, but increased in hypodynamic period. Bosentan and l-NAME treatment did not affect atrium beat rate in hyperdynamic period, but in hypodynamic period bosentan treatment decreased it to the control values and l-NAME treatment partially decreased it. This contradictory finding may be the result of the difference in methodology. We used both left and right atriums as a whole in the organ bath, but Contreas et al.20 only suspended right atrium. The basal sympathetic tone may vary in the left and right atriums and this may explain the different findings.
In another study, it was shown that isoproterenol responses of atrium beat rate did not change and l-NAME did not affect this response.25 Gholami et al. showed that isoproterenol response of atrium beat rate did not change in endotoxemic animals, but carbachol responses and carbachol potency on atrium beat rate decreased. Antimuscarinic effect of l-NAME was same in the control and endotoxemia groups.26 Jaue et al. expressed that the reduction in carbachol response of atrium beat rate was not associated with receptor downregulation but may be associated with post receptor factors.27 In these previous studies, atrium beat rate, adrenergic and cholinergic responses of atrium beat rate, and the effect of l-NAME on these parameters were investigated, but the effect of bosentan on these parameters in the literature is not known. In our study, we showed that isoproterenol and carbachol responses of atrium beat rate did not change, and bosentan and l-NAME did not affect this responses in both periods. Potency of isoproterenol on atrium beat rate was increased in bosentan- and l-NAME-treated groups in both periods, but carbachol potency on atrium beat rate was increased only in hypodynamic period in both treated groups. Carbachol responses and carbachol potency conflict with previous studies, and these contradictory findings may be due to the methodologic difference. Gholami et al., Jaue et al., and Price et al. used endotoxemic model as a septic shock model, but we used CLP model.25–27
In recent studies, usually in endotoxemia models, atrium muscle contraction decreased in septic shock and l-NAME could not ameliorate this reduction.28,29 In a septic shock with LPS model, isoproterenol response of atrium contraction decreased and l-NAME did not reverse it.25 In those previous studies, atrium contraction, adrenergic responses of atrium contraction, and the effects of l-NAME on these parameters in septic shock were investigated by generally using LPS-induced septic shock model, but the effect of bosentan on these parameters has not been reported. Additionally, it has been shown that ventricle papillary muscle contraction decreased in septic shock, and l-NAME could not ameliorate this reduction.29 Adrenergic and cholinergic responses of papillary muscle contraction, the effects of bosentan and l-NAME on these parameters are unclear. Our results demonstrated that atrium muscle contraction amplitudes decreased in both periods, and more decreased in hypodynamic period. While bosentan partially ameliorated atrium contraction in both periods, l-NAME partially ameliorated it only in hypodynamic period. Isoproterenol responses of atrium muscle contraction amplitudes increased in bosentan-treated group only in hypodynamic period, and in l-NAME-treated group it did not change in both periods. Carbachol potency on atrium contraction amplitude was increased only in hypodynamic period in both treated groups. Papillary muscle contraction did not change in both periods. While bosentan increased papillary muscle contraction only in hyperdynamic period, l-NAME increased it in both periods. In addition, values obtained by l-NAME effect exceeded the control values in hyperdynamic period. Responses to isoproterenol of papillary muscle contraction amplitudes increased in the bosentan-nontreated and treated groups in hypodynamic period. Responses to carbachol of papillary muscle contraction amplitudes increased in the l-NAME-treated group in both periods. Some of our results conflict with the previous studies, such as l-NAME partially ameliorated atrium contraction only in hypodynamic period, isoproterenol response of atrium contraction did not change in both periods, and ventricle papillary muscle contraction did not change in both periods and was increased by l-NAME in both periods. In previous reports, septic shock method was endotoxemic models, but we used a different septic shock model, CLP. This may be one of the reasons for different findings compared with the previous studies.26,28,29
These results show that a number of inflammatory mediators and cytokines such as NO and endothelin may increase the activity of the synoatrial (SA) node in hypodynamic period. Increase of this activity may be provided by inhibition of adenosine triphosphate (ATP)-sensitive potassium ion (K+) channels, the inward leak of sodium (Na+) and calcium (Ca2+) ions into the SA node, and release Ca2+ from sarcoplasmic reticulum.30,31 Endothelin may play a role on atrium contraction dysfunction in hyperdynamic period, and in hypodynamic period, endothelin and NO may play role together. Bosentan and l-NAME may increase atrium contraction in septic shock via increase of Ca2+ entry in atrium muscle fibers and Ca2+ sensitivity, and increasing expression enzymes related with contraction, upregulation/downregulation of receptors, and/or inhibition of Na+/K+ ATPase pump. Additionally, bosentan and l-NAME may increase potency of isoproterenol and carbachol on the atrium beat rate and atrium contraction via adrenergic and cholinergic receptor upregulation and/or post receptor factors. Furthermore, endothelin-1 blocks positive chronotropic and inotropic effect of isoproterenol by decrease in cyclic adenosine monophosphate (cAMP),32 elimination of this effect by bosentan can explain that isoproterenol response and potency on atrium beat rate and atrium contraction are increased by bosentan. Bosentan and l-NAME may increase papillary muscle contraction in septic shock via increase of Ca2+ entry in papillary muscle fibers and Ca2+ sensitivity, increasing expression enzymes related with contraction, upregulation/downregulation receptors, and/or inhibition of Na+/K+ ATPase pump. In addition, l-NAME may increase carbachol response of papillary muscle contraction by cholinergic receptor upregulation and/or via post receptor factors.
Clinical perspectives
In conclusion, our results show that NO and endothelin play significant roles in septic shock-induced cardiac dysfunction. Bosentan and l-NAME may have therapeutic effect. β-adrenergic and muscarinic receptor densities and the parameters that play a role in muscle contraction such as cAMP levels, Ca2+ levels, and both sympathetic and parasympathetic neurotransmitter levels should be analyzed in blood and heart muscle.
Footnotes
Conflict of interest
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
1.
JawadILuksicIRafnssonSB. Assessing available information on the burden of sepsis: global estimates of incidence, prevalence and mortality. J Global Health2012; 2: 010404.
2.
MayrFBYendeSAngusDC. Epidemiology of severe sepsis. Virulence. 2014; 5: 4–11.
3.
AngusDCLinde-ZwirbleWTLidickerJ. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med2001; 29: 1303–1310.
4.
KungHCHoyertDLXuJ. Deaths: final data for 2005. National vital statistics reports. The Centers for Disease Control and Prevention, National Center for Health Statistics, Hyattsville, MD.National Vital Statistics System2008; 56: 1–120.
5.
AshareAPowersLSButlerNS. Anti-inflammatory response is associated with mortality and severity of infection in sepsis. Am J Physiol Lung Cell Mol Physiol2005; 288: L633–L640.
6.
DinarelloCA. Biologic basis for interleukin-1 in disease. Blood1996; 87: 2095–2147.
7.
GroeneveldABBronsveldWThijsLG. Hemodynamic determinants of mortality in human septic shock. Surgery1986; 99: 140–153.
8.
IskitABSungurAGedikogluG. The effects of bosentan, aminoguanidine and L-canavanine on mesenteric blood flow, spleen and liver in endotoxaemic mice. Eur J Pharmacol1999; 379: 73–80.
GroeneveldABKesterADNautaJJ. Relation of arterial blood lactate to oxygen delivery and hemodynamic variables in human shock states. Circ Shock1987; 22: 35–53.
11.
van LambalgenAAvan den BosGCThijsLG. Changes in regional plasma extravasation in rats following endotoxin infusion. Microvasc Res1987; 34: 116–132.
12.
BaykalAKavukluBIskitAB. Experimental study of the effect of nitric oxide inhibition on mesenteric blood flow and interleukin-10 levels with a lipopolysaccharide challenge. World J Surg2000; 24: 1116–1120.
13.
IskitABGucMO. The timing of endothelin and nitric oxide inhibition affects survival in a mice model of septic shock. Eur J Pharmacol2001; 414: 281–287.
14.
LiaudetLRosseletASchallerMD. Nonselective versus selective inhibition of inducible nitric oxide synthase in experimental endotoxic shock. J Infect Dis1998; 177: 127–132.
15.
GibsonRLBergerJIReddingGJ. Effect of nitric oxide synthase inhibition during group B streptococcal sepsis in neonatal piglets. Pediatr Res1994; 36: 776–783.
16.
IskitABSenelISokmensuerC. Endothelin receptor antagonist bosentan improves survival in a murine caecal ligation and puncture model of septic shock. Eur J Pharmacol2004; 506: 83–88.
17.
İSKİTAB. Sepsiste Deneysel modeller. Yoğun Bakım Dergisi2005; 5: 133–136.
18.
YangRCWangCIChenHW. Heat shock treatment decreases the mortality of sepsis in rats. Kaohsiung J Med Sci1998; 14: 664–672.
19.
WeitzbergEHemsenARudehillA. Bosentan-improved cardiopulmonary vascular performance and increased plasma levels of endothelin-1 in porcine endotoxin shock. Br J Pharmacol1996; 118: 617–626.
20.
ContrerasPMigliaroERSuhrB. Right atrium cholinergic deficit in septic rats. Auton Neurosci2014; 180: 17–23.
21.
Oliveira-PelegrinGRde AzevedoSVYaoST. Central NOS inhibition differentially affects vasopressin gene expression in hypothalamic nuclei in septic rats. J Neuroimmunol2010; 227: 80–86.
22.
EumHAParkSWLeeSM. Role of nitric oxide in the expression of hepatic vascular stress genes in response to sepsis. Nitric Oxide2007; 17: 126–133.
23.
YangSCioffiWGBlandKI. Differential alterations in systemic and regional oxygen delivery and consumption during the early and late stages of sepsis. J Trauma1999; 47: 706–712.
PriceSEvansTWMitchellJA. Nitric oxide supports atrial function in sepsis: relevance to side effects of inhibitors in shock. Eur J Pharmacol2002; 449: 279–285.
26.
GholamiMMazaheriPMohamadiA. Endotoxemia is associated with partial uncoupling of cardiac pacemaker from cholinergic neural control in rats. Shock2012; 37: 219–227.
27.
JaueDNMaZLeeSS. Cardiac muscarinic receptor function in rats with cirrhotic cardiomyopathy. Hepatology1997; 25: 1361–1365.
28.
AshorobiRBKpohrarorBO. Effects of calcium ions and atropine on endotoxin-induced contractility deficit in rat atrial muscle. East Afr Med J1995; 72: 263–266.
29.
KellerRSJonesJJKimKF. Endotoxin-induced myocardial dysfunction: is there a role for nitric oxide?Shock1995; 4: 338–344.
30.
JoungBOgawaMLinSF. The calcium and voltage clocks in sinoatrial node automaticity. Korean Circ J2009; 39: 217–222.
31.
HanXLightPEGilesWR. Identification and properties of an ATP-sensitive K+ current in rabbit sino-atrial node pacemaker cells. J Physiol1996; 490(Pt 2): 337–350.
32.
ZhuYYangHTEndohM. Does nitric oxide contribute to the negative chronotropic and inotropic effects of endothelin-1 in the heart?Eur J Pharmacol1997; 332: 195–199.
33.
HubbardWJChoudhryMSchwachaMG. Cecal ligation and puncture. Shock2005; 24 Suppl 1: 52–57.