
Abstract
This study was embarked upon to evaluate the effects of pantoprazole and palonosetron on experimental esophagitis in albino wistar rats. Groups of rats, fasted for 36 h, were subjected to pylorus and forestomach ligation, supervened by treatment with normal saline (3 ml/kg, po, sham control), esophagitis control (3 ml/kg, po), pantoprazole (30 mg/kg, po), palonosetron (0.5 mg/kg, po), and their combination. Animals were sacrificed after 12 h and appraised for the volume of gastric juices, total acidity, free acidity, and esophagitis index. Esophageal tissues were further figured out biochemically for markers of oxidative stress and inflammatory mediators. The combination therapy comparably inhibited the esophagitis index (52.86%), gastric volume (66.04%), free acidity (43.76%), and total acidity (42.60%) in comparison with toxic control. The combination therapy also subsidized the biochemical and inflammatory markers to the purview less than toxic control. The morphological changes were scrutinized by scanning electron microscopy and were observed to demonstrate momentous protection by the amalgamation therapy. Combination therapy with pantoprazole and palonosetron flaunted sententious protection against experimental esophagitis.
Introduction
The prevalence of gastroesophageal reflux disease (GERD) in India ranges from 8% to 20% according to recently conducted study. 1 The disease is delineated by a broad spectrum of clinical manifestations inclusive of heartburn and regurgitation (cardinal symptoms of GERD). In augmentation to cardinal symptoms, chest pain, asthma, hoarseness, and sleep disturbance are also contemplated as atypical or extra esophageal symptoms of GERD. 2 GERD is broadly classified into two groups on the basis of endoscopic findings, namely, having esophageal mucosal damage (erosive esophagitis/Barrett’s esophagus) and no mucosal damage (endoscopy-negative reflux disease or nonerosive reflux disease). 1 Recent inquisitions have proclaimed that the mucosal damage in GERD is due to diverse causative agents in the refluxate that exhilarate mucosal and submucosal cells to release mediators, calling forth an inflammatory reaction, leading to visceral hypersensitivity and other symptoms of GERD. 3 The enhanced acid secretion along with deficit reflux mechanism intimates to play a key role in the underlying pathogenesis of GERD.
Acid suppression has been the mainstay for therapy of GERD and proton pump inhibitors (PPIs) like pantoprazole is one of the most persuasive drug in this regard. The recidivating nature of GERD requires long-term maintenance therapy and none of the currently available medications can deliver the same. 4 In fact, a recent report has estimated that up to 40% of GERD patients fail to reciprocate symptomatically either partially or completely, to a standard dose of PPI. About 90% of the PPI-treated GERD patients are partially or completely passive to standard dose/duration of the therapy and use of amalgamation therapies can implement more symptomatic relief for long duration. 5,6
Palonosetron is a second-generation 5HT-3 antagonist and is extensively used in impediment and treatment of chemotherapy-induced nausea and vomiting (CINV). Palonosetron has strong binding affinity toward 5HT-3 receptor and has a long half-life (approximately 40 h), bestowing a long lasting inhibition of the 5HT-3 receptor. 7 5HT-3 receptors are stationed in the nerve terminals of the vagus in the periphery and centrally in the chemoreceptor trigger zone. In preclinical studies, palonosetron manifested potent antiemetic properties in considerable animal models and is used for both acute and delayed CINV after judicious or high emetogenic chemotherapy. 8
Antecedent research at our laboratory has knuckled down inquesting the therapeutic opportunities for GERD and in the same line, few amalgamation therapies were reported. 9,10 In perpetuation to our forgoing endeavor to pin down the therapy for long-term symptomatic relief in GERD and significant antiemetic potential of palonosetron, the present investigation was ventured to inquest the effect of fixed dose combination therapy of palonosetron and pantoprazole on experimental esophagitis in experimental animals.
Materials and methods
Drugs and chemicals
Palonosetron (Palozac, Ajanta Pharma Limited, Mumbai, Maharashtra, India) and pantoprazole (Pantocid, Sun Pharma Limited, Mumbai, Maharashtra, India) were solicited from local market. All other chemicals were procured from Hi-media chemicals private limited (Mumbai, Maharashtra, India) and were of analytical grade.
Animals
Albino wistar rats of both sexes (100–140 g) were retrieved from the central animal house and kept in polypropylene cage under standard condition of temperature (37 ± 1°C) with 12-h light:12-h dark cycle and free access to commercial pellet diet and water ad libitum for acclimatization period of 10 days. The experimental protocol was approved by Institutional Animal Ethics Committee (approval no. UIP/IAEC/2014/FEB./14).
Induction of reflux esophagitis
Animals were randomized and divided into five groups of six animals each, fasted for 36 h, received sham control (normal saline, 3 ml/kg, po), toxic control (pylorus and forestomach ligated; normal saline, 3 ml/kg po), pantoprazole (pylorus and forestomach ligated; 30 mg/kg, po), palonosetron (pylorus and forestomach ligated; 0.5 mg/kg, po), and their combination (pylorus and forestomach ligated) as described in Table 1. After 1 h, coeliotomy was executed and esophagitis was induced by ligating the forestomach and pylorus with 2-0 silk suture, under thiopentone sodium anesthesia. 11 After 12 h, animals were sacrificed by cervical dislocation (under light ether anesthesia), the abdomen was opened with a median incision and the tissue esophagus and stomach were removed. The esophagus was dissected out by extending the dissection line along the major axis. The severity of esophagitis was calculated as represented in Table 2.
Effect of pantoprazole and palonosetron on gastric content, pH, free acidity, total acidity, and esophagitis index in albino rats.a

ANOVA: analysis of variance.
aEach group contains six animals. Data are represented as mean ± SD. Statistical significance compared with toxic control using one-way ANOVA followed by Bonferroni test. Values in parenthesis represent percentage inhibition.
b p < 0.001 was considered statistically significant.
c p < 0.05 was considered statistically significant.
d p < 0.01 was considered statistically significant.
Scoring of erosion and severity.
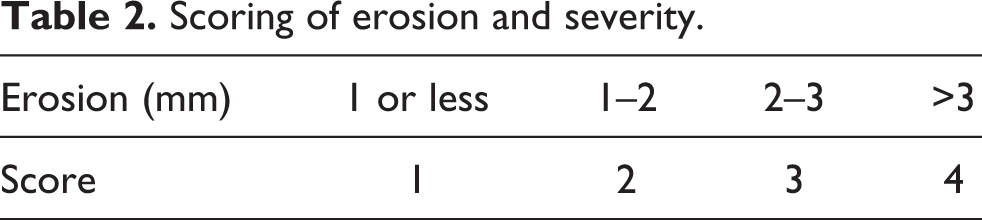
The sum of scores was divided by a factor of 10, which was designated as esophagitis index. 6 The volume of gastric content, total acidity, and free acidity were measured as described under “gastric secretion in pylorus ligated rats.” 11 The pH measurement of gastric content was done using a pen-type pH meter (HI 98107, Hanna instruments, Italy).
Estimation of free radical generation
Esophageal tissues were homogenized in ice-cold 0.01 M tris(hydroxymethyl)aminomethane-hydrochloric acid buffer, pH 7.4 and subjected to the estimations of thiobarbituric acid reactive substances (TBARS), 12 protein carbonyl, 13 tissue glutathione (GSH), 14 catalase, 15 and superoxide dismutase (SOD). 16 The tissue supernatant was also scrutinized for the levels of interleukin 1β (IL-1β; K0331212P), interleukin 6 (IL-6; K0331229P), and interleukin 10 (IL-10; K0332134P) using radioimmunoassay kits (Koma Biotech Inc., Seoul, Korea).
Morphological evaluation
Esophageal tissues were evaluated morphologically through a scanning electron microscope (SEM) using the method beforehand fortified at our laboratory. Briefly, samples were fixed in glutaraldehyde (2.5%) followed by washing in phosphate buffer (0.1 M). Post washing, the tissues were further fixed in osmium tetroxide (1%) with successive washing with phosphate buffer (1%). Subsequently, samples were dehydrated using the increasing concentration of acetone (30, 50, 70, 90, 95, and 100%). The samples were air dried and mounted to the aluminum stub with adhesive tape. The specimens were observed using a SEM (JEOL-JSM-6490LV, Japan). 17
In vitro cyclooxygenase (COX) and lipoxygenase (LOX) inhibition assay
The pantoprazole and palonosetron were evaluated for COX-1, COX-2, and 15-LOX inhibitory activity using COX inhibitor screening kit (catalog no. 760111) and 15 LOX inhibitor screening kit (catalog no.760700; Cayman Chemical Company, Ann Arbor, Michigan, USA). The stock solution of the pantoprazole and palonosetron were prepared in water for injection and further dilutions were made up to the concentration of 50 µg/ml. Percentage inhibition was calculated by comparing the absorbance intensities, measured spectrophotometrically with a 96-well plate reader (ALERE Microplate Reader, AM-2100, Waltham, Massachusetts, USA) at 590 and 490 nm for COX and LOX, respectively. Each test was performed in triplicate.
Statistical analysis
All data were presented as mean ± SD and analyzed by one-way analysis of variance followed by Bonferroni test for the possible significance identification between the various groups. c p < 0.05, d p < 0.01, and b p < 0.001 were considered as statistically significant. Statistical analysis was performed using GraphPad Prism software (3.2, San Diego, California, USA).
Results
The combination therapy of pantoprazole with palonosetron manifested conspicuous protection in opposition to the esophageal damage induced by pylorus and forestomach ligation. The combination therapy comparably inhibited the esophagitis index (52.86%), gastric volume (66.04%), free acidity (43.76%), and total acidity (42.60%) in comparison with toxic control (Table 1). The beneficial effects produced by the amalgamation therapy were analogous to pantoprazole alone. When assayed biochemically, the combination therapy also validated conspicuous restoration of the antioxidant defense system in comparison to toxic control. There was a significant increase in the TBARS generation (6.80 ± 0.05 nmol of malondialdehyde (MDA)/mg of protein) in toxic control in collation to normal control (0.70 ± 0.02 nmol of MDA/mg of protein) indicating participation of reactive oxygen species (ROS) generation and oxidative stress. Concomitant administration of the pantoprazole and palonosetron as a monotherapy and combination therapy momentously inhibited the lipid peroxidation manifested by decreased TBARS levels, that is, 2.73 ± 0.02, 1.95 ± 0.02, and 1.05 ± 00.02 nmol of MDA/mg of protein, respectively (Table 3). A significant increase in protein carbonyl content was ascertained in toxic control as analogous of sham control and combination therapy afforded convincing inhibition of oxidative stress. Similar line of observation was documented for GSH as well, with diminished level of GSH (0.87 ± 0.10 mg%) and restoration comparable to control (2.10 ± 0.12 mg%) after combination therapy (2.08 ± 0.12 mg%). Correspondingly, experimental esophagitis subsided the level of SOD (3.42 ± 1.13) and catalase (6.17 ± 0.76) in toxic control and the amalgamation therapy significantly accompanied to restore the same (i.e. 6.09 ± 2.98 units of SOD/mg of protein and 22.47 ± 2.33 nM of hydrogen peroxide (H2O2)/mg of protein) in analogs to normal control (Table 3).
Effect of pantoprazole and palonosetron therapy on TBARS, protein carbonyl, GSH, catalase, and SOD in albino rats subjected to forestomach and pylorus ligation.a

TBARS: thiobarbituric acid reactive substances; GSH: glutathione; SOD: superoxide dismutase; MDA: malondialdehyde; H2O2: hydrogen peroxide; ANOVA: analysis of variance.
aEach group contains six animals. Data are represented as mean ± SD. Statistical significance compared with toxic control using one-way ANOVA followed by Bonferroni test.
b p < 0.001 was considered statistically significant.
c p < 0.05 was considered statistically significant.
d p < 0.01 was considered statistically significant.
The esophageal tissue demonstrated apparent increase in the cytokine (IL-1β, IL-6, and IL-10) levels after the forestomach and pylorus ligation (Figure 1). Interestingly the monotherapy and combination therapy with pantoprazole and palonosetron subsidized the proinflammatory markers to the purview less than toxic control (Table 4). Convincing ultrastructural changes including dilated intracellular spaces and mucosa degeneration is a well-studied phenomenon and same was beheld when deliberated microscopically in the present experiment. Pronounced ultrastructural damage with mucosa degeneration was contemplated in toxic group in collation to sham control and amalgamation therapy demonstrated a marked microscopic protection as well (Figure 2).

Demonstration of forestomach and pylorus ligation.
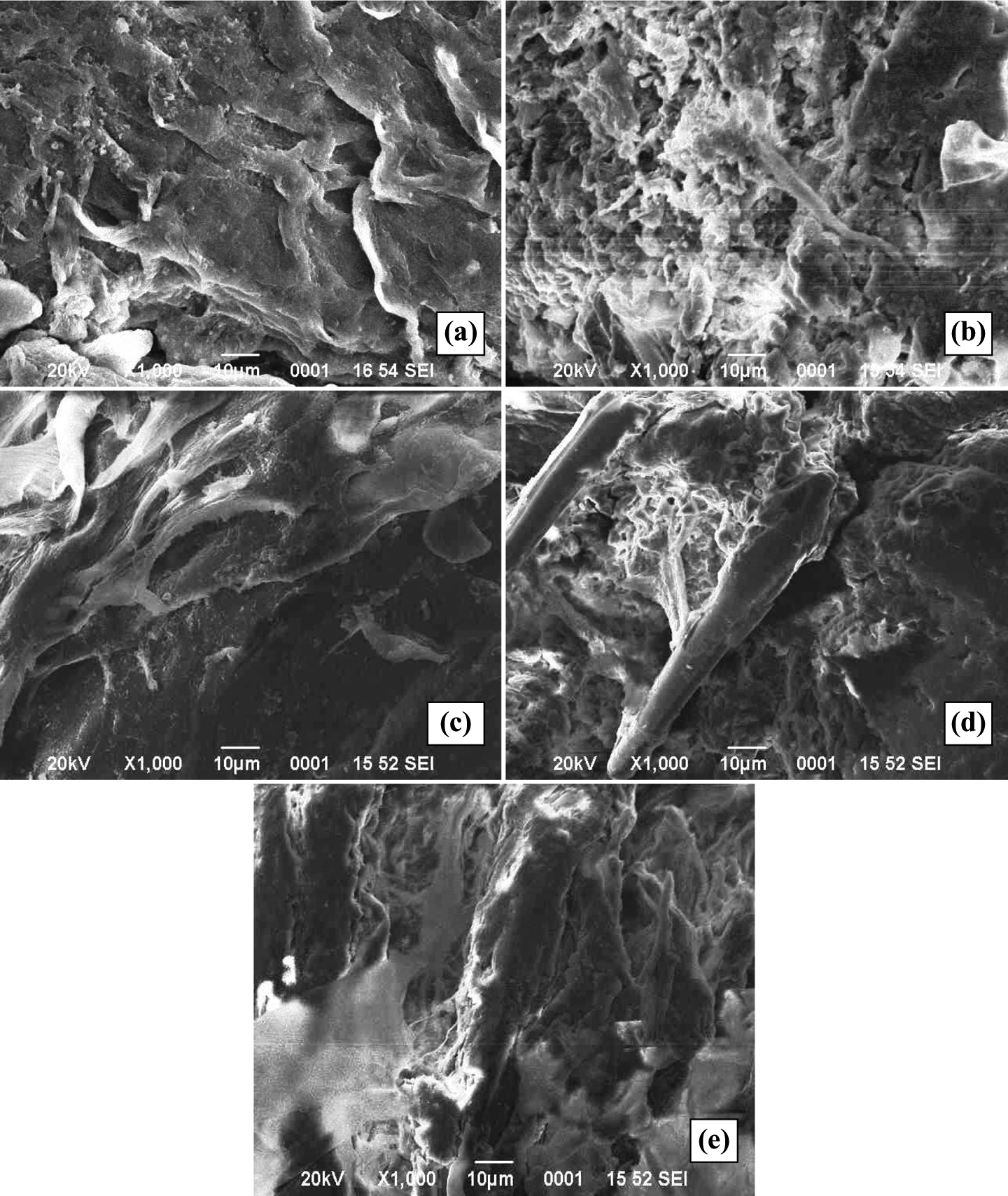
SEM images of the esophageal tissue (a) Sham control (3 ml/kg, normal saline); (b) esophagitis control (pylorus and forestomach ligated; 3 ml/kg, normal saline); (c) pantoprazole (pylorus and forestomach ligated; 30 mg/kg); (d) palonosetron (pylorus and forestomach ligated; 0.5 mg/kg); and (e) pantoprazole + palonosetron (30 + 0.5 mg/kg) (pylorus and forestomach ligated).
Effect of pantoprazole and palonosetron on proinflammatory and anti-inflammatory cytokines in esophageal tissues.a

ANOVA: analysis of variance; IL-1β: interleukin 1β; IL-6: interleukin 6; IL-10: interleukin 10.
aEach group contains six animals. Data are represented as mean ± SD. Statistical significance compared with toxic control using one-way ANOVA followed by Bonferroni test.
b p < 0.01 was considered statistically significant.
c p < 0.001 was considered statistically significant.
d p < 0.05 was considered statistically significant.
Discussion
This study conceded that the unification therapy of pantoprazole and palonosetron illustrates plausible protection against the experimental esophagitis. Pantoprazole is a PPI that blocks the proton/potassium ion adenosine triphosphatase pump and exhibit carbonic anhydrase in gastric mucosa. Pantoprazole covalently binds to cysteine residue of proton pump and inhibits the gastric secretion. 18 Pantoprazole is one of the most persuasive type of acid suppressants and is a well-established drug for the treatment of peptic ulcer. It impedes the secretion from gastric cells and helps in implementing consolation in reflux disease and mucosal curing in gastric ulcer and GERD. 19 Pantoprazole manifested significant protection through reduction in gastric volume and acidity (total and free), which could be accredited to its antisecretory potential. The decreased production of gastric juices through the parietal cells further accounted diminished mucosal injury and thereby decreased esophagitis index in the present experiment.
Palonosetron when used alone was observed to be appreciably less effective than pantoprazole in monitoring the pH, gastric content, and esophagitis index due to its inability to counteract the secretion of gastric contents. Whatsoever, efficacy of palonosetron observed could be accredited to its 5HT-3 antagonistic action, which monitored the reflux of gastric content toward the esophageal tissues. Palonosetron homogenous pantoprazole monotherapy validated momentous conservation in terms of monitoring the pH, volume of gastric juices, acidity (total and free), and esophagitis index. The integration therapy of pantoprazole and palonosetron perceived to have a credible protection against the pylorus and forestomach ligation and the same could be endorsed to the antisecretory potential of pantoprazole and antirefluxate property of palonosetron.
Precedent study has unfolded the role of free radicals in the pathogenesis of reflux esophagitis. 9 The reflux esophagitis has been divulged to increase MDA, a stable product of lipid peroxidation and a sensitive marker of membrane damage. 20 The MDA is a reactive substance that reacts to form a color complex with TBA and we observed a momentous upsurge in MDA augmentation in toxic control group, advocating active participation of the ROS and oxidative stress after the forestomach and pylorus ligation, which is in alignment to our antecedent reports. 17 It is apropos to mention that contemporaneous administration of pantoprazole and palonosetron as a fixed dose monotherapy and combination therapy momentously inhibited the lipid peroxidation as attested by decrease in MDA formation. The combination therapy was ascertained to be innumerably effectual than monotherapy.
The generation of ROS can damage all types of biological molecules including proteins, lipids, and deoxyribose nucleic acid. The proteins are the uttermost vehicle to force upon the oxidative damage of cells. Carbonyl group is produced on the protein side chain when they are oxidized either by α-amidation pathway or by oxidation of glutamide side chain. 21 Hence the presence of amino acid residues and the protein carbonyl content is one of the most general indicators for the protein oxidation. 22 As validated by the investigators, we also perceived a momentous escalation in the protein carbonyl content in toxic group. 23,24 However, the monotherapy as well as merger therapy of pantoprazole and palonosetron abetted to reestablish the marked up protein oxidative products.
GSH is an omnipresent tripeptide and is the most profused low-molecular weight thiol and is convoluted in wide spectrum of enzymatic reactions. GSH serves as the reductant in the oxidation–reduction process, a function resulting in the formation of glutathione disulfide. GSH is contemplated to be a marker of short-term oxidative stress and is contemplated with downturn in activity meanwhile the ROS attack. The aforementioned is accredited to the marked up diminution of GSH in the first few hours of oxidative stress. The ligation of the forestomach and pyloric end flaunted subsided levels of GSH due to increased utilization by the cells. The fixed dose therapy of pantoprazole and palonosetron decidedly reestablished GSH levels and aforesaid could be imputed either to decreased oxidative stress or increased biogenesis of GSH.
The antioxidant enzymes, SOD and catalase, fudge together a major supportive team of defense against ROS attack. SOD is a free radical scavenging enzyme that counterpoises superoxide-free radical by forming H2O2 and combats oxidative stress. 25 The antecedent studies have advocated/demonstrated the subsidence in SOD level in the course of oxidative stress. 25,26 Aligning the previous reports, ligation of the forestomach and pyloric end was ascertained with momentary decreased SOD level and same could be accredited to the repercussion of physiological reimbursing mechanism to affray oxidative stress in early phase. Catalase catalyzed the dismutation of H2O2 (generated through scavenging effect of SOD) to water and molecular oxygen and synchronic decrease in catalase activity is cardinal with decrease in SOD activity to negate the detrimental effects of oxidative stress and we contemplated the same in our study. The treatment with pantoprazole and palonosetron was ascertained with decreased oxidative stress as manifested through increased activity of SOD and catalase in esophageal tissue.
From the above discussion it became evident that the combination therapy of palonosetron and pantoprazole can roll out oxidative damage, biochemically in experimental esophagitis.
In an experiment model of esophagitis, and in the patients affected with GERD, the mediators considered to be analytical along with ROS are inflammatory prostanoid and cytokines 27,28 and therefore to have a worthier insight into the current treatment approach, the cytokine levels of IL-1β, IL-6, and IL-10 were evaluated. IL-1β is a member of IL-1 family cytokines and is chiefly produced by the actuated macrophages. IL-1β is aforethought to be an important mediator of inflammatory response and is involved in variety of activities including, cell proliferation, differentiation, and apoptosis. 29
IL-6 is secreted by T cell/macrophages and stimulates immune responses. Consonant to IL-1β, IL-6 is proinflammatory cytokine, and both IL-1β and IL-6 can stimulate the inflammatory and autoimmune response in many diseases like diabetes and cancer, including esophagitis. 30 Our study ascertained with increased expression of IL-1β and IL-6 in response to forestomach and pylorus ligation. The monotherapy as well as combination therapy of palonosetron and pantoprazole was perceived with conspicuous depletion in the levels of these two proinflammatory cytokines. Several lines of investigations commend that the major physiological importance of IL-10 is to constrain inflammation (anti-inflammatory) through inhibiting the release of proinflammatory cytokines and prevent adequate immunological reactions. In contradiction to precedent reports, we contemplated significant increase in the IL-10 levels following the pylorus and forestomach ligation. 31,32 Similar lines of contrary results were observed with subsequent treatment through pantoprazole and palonosetron therapy. This unexpected behavior of IL-10, as observed in present experiment, could be accredited to various factors including the physiological compensatory mechanism to combat inflammation/expression of IL-10 requires triggering by commensal and is minimal in unstimulated tissue/pleiotropic effects of IL-10 in immunoregulation and inflammation. However, the correct explanation for such observation is beyond the scope of the present manuscript.
The esophagitis is a manifold disorder and intricacies are resultant of multifactorial mechanism in which acid and pepsin are the two important pernicious factors tangled. 33 The protracted contact of esophageal mucosa with refluxate (acid and pepsin), due to flawed antireflux barrier, can bulge to further morphological changes in esophageal epithelium. 34,35 To review the same, esophageal tissues were further investigated for morphological diversification using SEM. The forestomach and pylorus ligation illustrated compelling ultrastructural alteration including dilated intracellular spaces, extensive erosion of esophageal mucosa, and detachment of epithelial layer, as reported previously. 36,37,38 The monotherapy and amalgamation therapy of pantoprazole and palonosetron were perceived to bring back the ultrastructural alterations when ascertained microscopically. IL-10 is anti-inflammatory cytokine and recently has been suggested as immunostimulatory in nature. 39 To further intrude, we probed COX and LOX inhibitory activity for pantoprazole and palonosetron, in vitro (Table 5). Both the drugs manifested sententious inhibition of 15-LOX, COX-1, and COX-2 enzymes, manifesting the dual inhibitory potential of palonosetron and pantoprazole against the arachidonic acid pathway. The dual inhibition of archidonic acid pathway will lead to the diminished production of proinflammatory cytokine 40 and could be aforethought as one of the feasible mechanisms for the therapeutic efficacy of the drugs in the present experiment.
In vitro COX and LOX inhibition by pantoprazole and palonosetron.a

LOX: lipoxygenase; COX: cyclooxygenase.
aData are represented as mean ± SD. Experiment was performed in triplicate.
It is noteworthy that palonosetron retained its ameliorative effects alone as well as in combination with pantoprazole without any untoward effect, which is not the case for current therapeutic options for GERD. From the above line of evidences, we would like to accomplish that the amalgamation therapy of palonosetron and pantoprazole can demonstrate protective effects against GERD.
Footnotes
Acknowledgement
Authors would like to thank University Grants Commission, New Delhi for providing fellowship to SG, MS, and JKR.
Conflict of interest
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.