
Abstract
Background:
Hydrofluoric acid (HF) is a dangerous chemical that can cause severe cutaneous burns as well as possible systemic toxicity.
Methods:
We retrospectively analyzed all human HF exposure cases reported to the National Poison Control Center of Taiwan between 1991 and 2010.
Results:
In this 20-year survey, 324 calls were identified, with a majority of dermal exposure (84%). Occupational exposure accounted for 80% of all cases, with workers in semiconductor industry (61%), cleaning industry (15%), chemical or metal industry (13%), and other industries (11%). Electrolyte imbalances were uncommon, hypocalcemia, hypomagnesemia, and hypokalemia were recorded in 8.6%, 1.2%, and 1.5% of all cases, respectively. Most cases (64%) of dermal exposure received antidotal treatment. Treatment modalities of dermal exposure included calcium gluconate soaking, 49.8%; intravenous calcium, 20.6%; and topical use of calcium gluconate gel, 13.9%. Twenty patients (7%) received surgery. Following HF exposure, the majority of patients presented with mild (56.5%) or moderate (36.7%) toxic effects. However, four patients were severely intoxicated; two patients died of HF-related dysrhythmia and shock.
Conclusions:
Significant symptomology may occur following HF exposure, and most of the HF exposure required hospitals evaluation. Calcium gluconate soaks appear to be effective in reducing local pain and tissue damage. Hyperkalemia should not be overemphasized as a common finding in HF exposure, hypokalemia tends to occur in cases of severe HF poisoning.
Introduction
Hydrofluoric acid (HF) is known to be one of the corrosive inorganic acids because of its ability to release toxic fluoride anions inside cells and its hydration and corrosion of tissues by free hydrogen ions. 1 HF is widely used in glass etching, the production of semiconductors, fluorocarbon, plastics, germicides, insecticides, and other industrial and domestic processes. 1,2 With the character of aggressive and destructive tissue penetration, fluoride ion can produce harmful systemic effects by any route of exposure. Symptoms are often delayed, particularly with exposure to a dilute solution.
The reported information on the epidemiology of HF poisoning was uncommon; epidemiological knowledge may aid health-care providers in providing appropriate diagnostic and treatment plan and also help government and industry in providing adequate preventive strategy. 3 –5 The study aimed to retrospectively analyze the nature of HF calls to the National Poison Control Center of Taiwan (PCC-Taiwan) in order to characterize the epidemiology of HF exposures in Taiwan.
Materials and methods
This was a retrospective study of data from PCC-Taiwan, which is located in the Taipei Veterans General Hospital, Taiwan. PCC-Taiwan served the 23 million populations in Taiwan and received approximately 4000–5000 calls related to poison exposures in Taiwan per annum. These calls come from the public, the person exposed, or family members, but mainly the health professionals.
Data of HF related human exposure were collected from PCC-Taiwan between 1991 and 2010. The diagnosis of HF poisoning was made by the treating physicians with the pertinent history and verification of the implicated agents. After careful review of the data, we eliminated records of unrelated exposures, cases with information inquiry only, and cases with inadequate general information. Data on types of caller, patient’s age, gender, profession, routes, and dose of exposure, reason for exposure, HF concentration, concurrently exposed substances, symptomology, serum electrolyte data, severity of poisoning, treatments, and outcomes were then extracted.
Follow-up of the patient’s clinical courses and outcomes was carried out by phone calls to the health-care facilities that originated the enquiries and/or the patient’s own residence. Attempts were also made to trace the medical records of patients with severe toxicity or death. After collecting the aforementioned information, clinical severity of poisoning was divided into asymptomatic, mild, moderate, severe, and death as described previously. 6
Results
Of the 340 HF exposure calls made to the PCC-Taiwan during this 20-year survey, 324 met the inclusion criteria (approximately 16 per year). The majority of calls came from physicians (72%), 7% from nurse, and 21% from patient himself or other individuals. Of them, 93% of patients received medical evaluation. Most HF exposures were single agent (95%), 15 had exposed to more than one substance. The second substances were other acids (12), ammonia/hydrogen peroxide (1), tetramethylammonium hydroxide (1), and hydrofluoroalkane (1). Most exposure occurred in men (79%) and 20- to 39-year-old adults (71%).
Dermal exposures made up the majority of total HF exposures (84%) (Table 1). The second most common exposure was inhalation (7%). Occupational exposures predominated (80%), followed by accidental exposure (19%). One call involved deliberate self-poisoning. Of work-related exposures with known profession (183 cases), workers were in semiconductor industry (61%), cleaning industry (15%), chemical or metal industry (13%), and other industries (11%).
Reason and route of all HF exposure.

The sites of body contact were known in 192 cases, upper limb involved 79.6% (hand contact 65.6%), lower limb involved 17.2%, head–neck involved 10.9%, and trunk involved 7.3% (Figure 1). The burn sizes were recorded in 198 cases, ranged from 0.1 to 30% of total body surface area (TBSA). Majority cases (86.9%) had burn size less than 1% TBSA, 10.6% had burn size of 2–5% TBSA, 1.5% had burn size of 6–10% TBSA, and 1.0% had burn size of 11–30% TBSA.

Contact sites of dermal exposure (N = 192).
Electrolyte measurements were performed in most cases. Calcium data were available in 83% of “severe/death,” 73% of “moderate,” and 46% of “asymptomatic/mild” cases. Potassium data were available in 83% of “severe/death,” 68% of “moderate,” and 42% of “asymptomatic/mild” cases. Magnesium data were available in 50% of “severe/death,” 44% of “moderate,” and 18% of “asymptomatic/mild” cases. Electrolyte imbalances were uncommon, hypocalcemia, hypomagnesemia, and hypokalemia were recorded in 8.6%, 1.2%, and 1.5% of all cases, respectively. However, laboratory investigations showed that hypocalcemia, hypomagnesemia, and hypokalemia were common in severe or fatal cases, and hyperkalemia was not reported in any of our cases (Table 2).
Electrolyte imbalance among HF exposure cases reported to PCC-Taiwan.
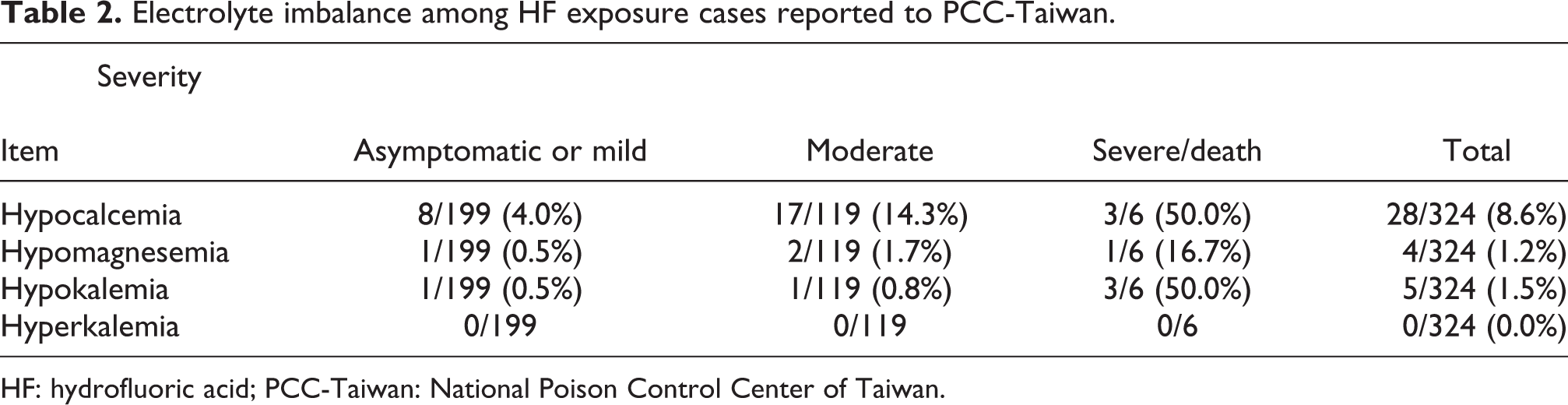
HF: hydrofluoric acid; PCC-Taiwan: National Poison Control Center of Taiwan.
All cases of dermal exposure (287 cases) received water irrigation except four cases (1.4%) of having hexafluorine irrigation. Most patients (64%) with dermal exposure received treatment that included calcium gluconate soaks (49.8%), systemic intravenous infusion of calcium (20.6%), topical use of calcium gluconate gel (13.9%), calcium gluconate local injection (3.8%), and regional calcium gluconate infusion (2%). Calcium gluconate soaks is effective for relieving pain in 80% of patients. Twenty patients (7%) were recorded of having a surgical procedure, which included debridement (20), local flap (3), nail removal (2), amputation of four fingers (1), and neurectomy (1).
Following HF exposure, the severities of poisoning were asymptomatic (4.9%), mild (56.5%), moderate (36.7%), severe (1.2%), and fatal (0.6%). The cause of death was HF-related dysrhythmia and shock. Ingestion had highest fatality rate (16.7%). Among cases with dermal exposure, majority (64.8%) were exposed to an unknown concentration of HF solution, 11.5% were exposed to a 20% or less of a HF solution, 18.5% were exposed to 20–50% of a HF solution, and 5.2% were exposed to a HF solution of at least 50% (Table 3).
Distribution of HF concentration and severity of poisoning among dermal-exposure cases.

HF: hydrofluoric acid.
Illustrated fatal cases
A 26-year-old male plastic factory worker was accidentally exposed to pure HF resulting in 6.5% TBSA third degree burn to left forearm, low abdomen, and left thigh. Water irrigation of the burn area was initiated at the scene. The patient was transported to an Emergency Department 23 min later. Local injection with calcium gluconate was performed by a surgeon. Initially, his total calcium was 8.4 mg/dL (normal 8.5–10.5 mg/dL). The patient had a seizure and became unconsciousness 30 min into his Emergency Department course. Intravenous calcium chloride (10%) 20 mL and diazepam 10 mg was immediately administered. Hypokalemia (3.1 mmol/L, normal 3.5–4.9 mmol/L) and ventricular tachycardia was noted during resuscitation. He died 6 h following his HF exposure. Throughout the hospital course, he received calcium gluconate (10%) of 20 mL and calcium chloride (10%) of 80 mL, which was equivalent to 118 mEq calcium.
A 42-year-old woman ingested 80 mL of a rust remover obtained from a local dry cleaning shop in an attempted suicide. She was transported to a local hospital 90 min from the time of her ingestion, where first aid, gastric lavage, and activated charcoal were administered. The patient developed severe vomiting with coffee-ground vomitus and hypotension (blood pressure 70/40 mmHg) 70 min into her hospital course. After an intravenous infusion of 1500 mL normal saline, she was transferred to a medical center 60 min later. At the medical center, the patient was hypotensive (78/38 mmHg), tachycardic (102 per min), irritable, and complaining of muscle cramping, numbness of mouth and limbs. Laboratory investigations revealed white blood cell count of 14,020 per cumm, hemoglobin 10.4 g/dL (normal 12–16 g/dL), creatinine 1.8 mg/dL (normal 0.5–1.2 mg/dL), sodium 142 mmol/L (normal 135–145 mmol/L), potassium 4 mmol/L, chloride 114 mmol/L (normal 96–106 mmol/L), aspartate transaminase 78 U/L (normal 5–45 U/L), and alanine transaminase 23 U/L (normal 0–40 U/L). Her ionized calcium was 0.46 mmol/L (normal 1.13–1.31 mmol/L) at 7.5 h postingestion, and an intravenous calcium gluconate (10%) of 20 mL was administered. One hour later, the patient developed seizure, ventricular tachycardia, cyanosis, and was comatose. Follow-up laboratory investigations showed serum creatinine 2.7 mg/dL, potassium 3.3 mmol/L, ionized calcium 0.50 mmol/L, chloride 113 mmol/L, and amylase 504 U/L. The patient died at 11 h postingestion. Throughout the hospital course, she received calcium gluconate (10%) 100 mL, which was equivalent to 46.5 mEq calcium.
Discussion
In Taiwan, HF is mainly used in the semiconductor industry. It is also commonly used in cleaning, chemical and metal industries, and consumer products. Common products include cleaning agents, such as rust removals, automobile wheel cleaners, air conditioner cleaners, tile-cleaning agent, glass cleaning solution, aluminum brighteners, and some heavy-duty cleaners. As in other case series, the largest group at risk of HF exposure is adult males in the workplace and digit dermal exposure was the most common route of exposure. 2 –5 HF exposures in females, children, and the elderly individuals is less common probably because of less occupational exposure and product use among them.
Dermal exposures often cause local tissue injury with signs and symptoms developing over time, and a patient may not seek urgent medical evaluation resulting in a potentially worse clinical outcome. Excruciating pain accompanied by tissue maceration, erythema, blister, ulcer, and necrosis. 1 –5 Serious skin damage and tissue loss may occur, if not treated early and properly. In our study, a 69-year-old man exposed his bare hands to a 48% HF solution. There was a delay in the diagnosis, and four of his fingers had to be amputated.
Dermal exposure to higher doses of HF can result in systemic toxicity. This is characterized by hypocalcaemia, hypomagnesemia, tetany, seizure, QTc prolongation, ventricular dysrhythmias, cardiac arrest, and death. Hypocalcemia may occur following burns of greater than 1% TBSA from exposure to a HF solution of 50% or greater; 5% or greater body surface area with any HF concentration; vapor inhalation from 60%, or greater HF concentration. 2,7 Prompt correction of hypocalcemia and/or hypomagnesemia is paramount to improve patient survival. Two fatal cases in our study developed hypocalcemia (total calcium 8.4 mg/dL, ionized calcium 0.46 mmol/L) and hypokalemia (3.1 mmol/L, 3.3 mmol/L); unfortunately, they received inadequate electrolyte therapy. One worker developed hypocalcemia (calcium 6.9 mg/dL), hypomagnesemia (1.41 mg/dL), hypokalemia (2.6 mmol/L), and cardiac arrest, but he was resuscitated successfully by the administration of calcium, magnesium, and potassium. 8
Treatment of HF burn includes decontamination, topical application of calcium gluconate, and intravenous calcium and magnesium therapy for significant intoxicated cases. 1,2 Calcium gluconate local injection and regional intravenous and intra-arterial infusion can be cautiously used in severe cases. Intralesional injection of calcium gluconate has been reported to be effective in relieving pain and decreasing the severity of poisoning. 1,2 In our experience, patients often experienced intolerable pain related to the procedure itself. Therefore, this technique is not routinely recommended in our center. Although topical calcium gluconate gel may be an effective treatment following decontamination of HF, due to the license issue, its availability was still a question. In our study, only 13.9% received topical therapy of calcium gluconate gel. Up to date, calcium gluconate gel is neither a licensed pharmaceutical nor commercially available in Taiwan. However, some large-scale semiconductor manufactures does have a stock of calcium gel at work-site. Calcium gluconate gel can be compounded by mixing calcium gluconate solution and lubricating jelly, but due to unconfirmed efficacy of the product itself, it was not recommended to be applied in our cases. Calcium gluconate soaks were recommended by our center when patients presented to a hospital, and almost 50% of the patients received this treatment. This method was demonstrated to be highly effective in reducing the local pain as well as the degree of tissue damage in our cases and previous report. 2
Prophylactic removal of fingernail and excision of the affected skin were not recommended in our cases due to increasing of patient’s suffering. Fingernail removal has been suggested when there is a severe subungual pain and discoloration. 2 Surgery is considered seriously only in cases with tissue damage.
Cardiac dysrhythmia and death following severe HF burn or ingestion of HF have been reported. In our study, one patient died 6 hours following an accidental dermal exposure (6.5% TBSA) to pure HF. Another patient died 11 h following an intentional ingestion of 80 mL of anti-rust solution. These two fatalities had presentations of hypocalcemia, hypokalemia, ventricular tachycardia, seizure, and intractable shock.
Numerous published reports described that death may occur as a result of electrolyte imbalance in HF poisoning such as hyperkalemia, hypocalcemia, and hypomagnesemia. 1,2,9 –11 Profound hypocalcemia is a purported culprit in HF toxicity, and hyperkalemia has also been suggested as an etiology of fluoride-associated dysrhythmias. Hyperkalemia is postulated to result from direct actions of fluoride anion or second to resuscitative effect or tissue injury. 8,12 The observation of hyperkalemia in HF poisoning has been first challenged by Vohra et al. 12 They reviewed reports of 26 cases with life-threatening toxicity associated with exposure to fluoride compounds (including HF) and noticed that hyperkalemia had been conclusively demonstrated only in cases of poisoning with sodium fluoride or sodium silicofluoride and in those cases who received resuscitative procedures. However, hyperkalemia was not observed in patients of HF poisoning who have not received resuscitation. Comparing with sodium fluoride, HF is a week acid that does not readily dissociate; therefore, fluoride ion associated hyperkalemia may be not an important mechanism of dysrhythmias in cases of poisoning with HF. In our series of 324 cases, there was no hyperkalemia case, which is consistent with the scarcity of published cases of hyperkalemia with HF poisoning. However, hypokalemia tends to occur in cases of severe HF poisoning.
Limitations
This study is a retrospective analysis of prospectively collected information in a PCC-Taiwan database and suffers from the weaknesses of all retrospective studies, including reporting bias, recall bias, selection bias, and possible confounders that cannot be controlled for in retrospect. This study uses PCC-Taiwan data that do not reflect all HF exposure in Taiwan because reporting to PCCs is voluntary.
Conclusion
HF cause significant symptomatology, and most calls of HF required hospital evaluation. Delayed toxicity, systemic involvement, and insufficient knowledge of patients or physicians pose clinical diagnostic and therapeutic challenges. Both inadequate and over-treatment should be avoided. Based on our observation, hyperkalemia should not be overemphasized as a common finding in HF exposure, and hypokalemia tends to occur in cases of severe HF poisoning. Further studies will be needed to elucidate mechanism of electrolyte abnormalities as well as optimal management following HF poisoning.
Footnotes
Funding
The authors acknowledge the financial support from the Department of Health designated for The National Taiwan Poison Control Center in Taipei Veterans General Hospital, Taipei, Taiwan, 2011.