
Abstract
Lead is very common in the environment, and it is therefore important to characterize its possible adverse health effects. The aim of this study was to evaluate the impact of lead exposure on selected functions of the liver and bile ducts in people who are chronically exposed to the metal because of their occupations. To provide this information, the activity of specific enzymes and the bilirubin concentration were determined in blood serum, and morphological parameters of the liver and bile ducts were evaluated using the ultrasonic imaging method. Healthy male employees of a lead–zinc processing facility (n = 145) who were occupationally exposed to lead were divided into two subgroups as a function of the lead concentrations in blood (PbB): low lead exposure (PbB = 20–35 μg/dl; n = 57) and high lead exposure (PbB = 35–60 μg/dl; n = 88). Human exposure to lead compounds was found to cause liver enlargement and to activate inflammatory reactions with the characteristics of moderate cholestasis within the bile ducts, while no characteristics of necrotic damage of hepatic cells were noted. It seems that lipid peroxidation can be one of the toxic mechanisms of lead which induce moderate cholestasis. The effects depend on the extent of the lead exposure and were greater in subjects with higher exposure levels, particularly subjects with PbB values greater than 35 μg/dl.
Introduction
Lead is a metal that is toxic to the living organisms even in low concentrations. 1 This element is very common in nature, and it is therefore important to characterize its possible adverse health effects. Human exposure occurs through inhalation or through the consumption of contaminated food or water.
The amount of lead absorbed from the environment by a human depends on its chemical form, the absorption route, and the sex, age, and genetic predispositions of the subject. 2 Lead absorbed from the stomach and the small intestine following ingestion enters the liver and the circulatory system through the portal vein. In erythrocytes, 99% of the lead is bound in the form of the soluble dibasic orthophosphate.
In cases of occupational exposure to lead (e.g., in metallurgists), inorganic compounds of the metal enter the body mainly through the respiratory tract. The following parameters are determined in evaluating lead toxicity and estimating the extent of lead exposure: zinc protoporphyrin (ZPP), delta-aminolevulinic acid (ALA) and lead concentration in whole blood. An early indication of Pb exposure is the accumulation of protoporphyrin IX in erythrocytes as a result of Pb interference in the process of heme synthesis. To assess the effect of Pb on this process, the total free erythrocyte zinc protoporphyrins (ZPP) was measured. Protoporphyrins remain in erythrocytes throughout their life span and are therefore a good indicator of chronic exposure. ALA is a substrate for aminolevulinic dehydratase (ALAD), an enzyme in the porphobilinogen synthesis pathway. Suppression of the ALAD activity by Pb leads to an accumulation of ALA. ALA in turn has a prooxidative effect and is associated with increased production of reactive oxygen species (ROS) . 3
The liver has detoxifying and exocrine functions. Toxic compounds in the liver may be bound to proteins, undergo biotransformation or be excreted unchanged in bile. 4 The biotransformation of xenobiotics is mediated by hepatic microsomal enzymes that may oxidize or reduce the compounds or produce conjugates. The mitochondrial, cytoplasmic and nuclear enzymes of the liver also participate in the chemical transformations of foreign substances. The cytoplasm constitutes the largest part of the hepatocyte and contains enzymes including aspartate transaminase (AST), alanine transaminase (ALT) and isoenzyme 5 of lactate dehydrogenase (LDH5). These enzymes appear in the blood when the hepatocyte membrane is damaged.
The presence of mitochondrial or lysosomal enzymes in the serum is consistent with severe hepatic damage, including necrosis. The hepatic capillaries are easily permeable and enable the transport of foreign substances from the blood to the hepatocytes, which surround the biliary canaliculi, through passive diffusion or transporter-mediated (active) transport. For heavy metals, active transport occurs. Thus, intracellular lead concentrations may be as much as several hundred times higher than lead concentrations in bile or blood plasma.
Ultrasonic imaging is a key method for diagnosing chronic illnesses of the liver. It is a noninvasive imaging method, enabling multiple evaluations. The main criterion for the diagnosis of parenchymal illness is an increase in hepatic echogeneity. The organ enlargement, change of shape and rounded edges objectively define parenchymal hepatic illnesses.
Experiments carried out on animals exposed to lead show liver enlargement associated with increased proliferation of hepatocytes 5 and mitogenic processes. 6 These observations suggest that similar lesions might occur in humans. Thus, imaging assessment of the liver could provide valuable information. However, there are no previously published data from imaging tests of the liver in Pb-exposed humans.
Damage caused by lead primarily involves enzymatic inhibition caused by this metal. Numerous enzymes are inhibited by Pb, including Na+/K+ ATPase, ATP phosphohydrolase, NAD synthetase and 5′pyrimidine nucleosidase. 7 In contrast, Pb may increase the activities of alkaline phosphatase (FA), γ-glutamyltransferase (γ-GT), alanine and aspartic aminotransferases, LDH5 isoenzyme and cholinesterase (CHE). CHE are two genetically conditioned enzymes that catalyze acetylcholine degradation. Determining the activity of these enzymes is useful in assessing liver function and diagnosing the toxicity of chemical substances. 8
The purpose of this study was to evaluate the impact of lead exposure on the selected functions of the liver and bile ducts in people who are chronically exposed to the metal in an occupational setting through a determination of the activity of selected enzymes and the bilirubin concentration in serum and morphological parameters of the liver and bile ducts by the ultrasonic imaging method.
Methods
The tests were performed in 145 healthy men who were employees of a lead–zinc processing facility and who were occupationally exposed to lead. The subjects were divided into two subgroups. The following indicators were used for determination of the lead exposure extent: lead concentration in blood (PbB), ZPP concentration in blood, deltaaminolevulinic acid (ALA) concentration in urine. The tests were based on current PbB, ZPP and ALA concentrations and their averages of the last 3 years. The group tested was divided into two subgroups, depending on the PbB concentration in blood: low exposure to lead PbB = 20–35 μg/dl (LePb group) (n = 57) and high exposure to lead PbB = 35–60 μg/dl (HePb group) (n = 88).
The control group (C) (n = 36) were the people not occupationally exposed to lead compounds, healthy men in whom no increased PbB and ZPP concentrations in blood and ALA in urine were found.
The blood to be tested was sampled in the morning, on empty stomach, from the basilic vein, in the amount of 10 ml. Upon addition of EDTA as anticoagulant to 5 ml of blood, the plasma was obtained, while the serum was obtained from the remaining blood volume. Mid-Stream Specimens (MSU), 2 ml, were taken. All participants received vitamin C in doses of 300 mg/day. The study was approved by the Bioethical Commission No L. dz. NN-013-156/I/03 and was financed as a research project with funds assigned for science in 2005/2006.
Determination of lead concentration (PbB) in blood
Lead concentration in blood was determined with the use of atomic absorption spectrophotometry. Spectrophotometer was obtained from Unicam-SOLAR 939 QZ with deuteric alteration, graphite furnace from Unicam GF 90 and automatic feeder FS 90. The calibration curve was prepared on the templates from Nycomed, Norway. The calibration was carried out at the beginning and at the end of the determination series. Two certified standards from Nycomed with lead concentrations of 4.2 μg/dl and 38.0 μg/dl were used as internal control. The absorbance was read at wavelength 283 nm. The values were expressed in micrograms per deciliter of whole blood. Such method is specific for estimation of lead.
Determination of ZPP concentration in blood
The concentration of ZPP in blood was determined by a direct fluorometric method using hematofluorometer, model 206. The apparatus measures the ratio between the fluorizing substance (ZPP) and the concentration of hemoglobin—the light absorbing substance. The values were expressed in micrograms per grams Hb.
Determination of delta ALA concentration in urine
The concentration of ALA in urine was determined by Grabecki’s method.
9
The principle of this method is that ALA reacts with acetylacetone and that the resulting pyrrole compound subsequently reacts with p
Determination of the activity of the liver form of LDH5 in blood serum (EC 1.1.2.3)
Krawczyński’s spectrophotometric method 10 was used to determine the total enzyme activity. The LDH activity is measured as the decrease in optical density at 340 nm within 1 min. The liver isoenzyme (LDH5) is totally inactivated within 30 min of heating at 57°C. Thus, the liver isoenzyme activity, LDH5, was calculated on the basis of the difference between the total activity and the activity of other isoenzymes that remained following incubation for 30 min at 57°C. The enzyme activity was expressed in IU/l.
Determination of FA activity in blood serum (EC 3.1.3.1)
This assay was carried out using a biochemical analyzer from Roche/Hitachi. In the presence of magnesium and zinc ions, p-nitrophenyl phosphate is hydrolyzed by the enzyme to phosphate and p-nitrophenol. The amount of p-nitrophenol is directly proportional to alkaline phosphatase (FA) activity and can be determined photometrically. The enzyme’s activity was expressed in IU/l.
Determination of γ-GT in blood serum (EC 2.3.2.1)
This assay was carried out using a biochemical analyzer from Roche/Hitachi. γ-GT transfers γ-glutamyl groups from
Determination of AST activity in blood serum (EC 2.6.1.1)
This assay was carried out using a biochemical analyzer from Roche/Hitachi. AST catalyzes the transamination reaction in both the directions. The oxaloacetate product is in turn a substrate in the indicator reaction, in which malate dehydrogenase (MDH) causes the oxidation of NADH to NAD. The decrease in the optical density of NADH measured photometrically is directly proportional to the oxaloacetate concentration and thus to the AST activity. The enzyme’s activity was expressed in IU/l.
Determination of ALT activity in blood serum (EC 2.6.1.2)
This assay was carried out using a biochemical analyzer from Roche/Hitachi. ALT catalyzes the transamination reaction in both the directions. The pyruvate product in turn becomes a substrate for lactate dehydrogenase (LDH) in the indicator reaction in which NADH is oxidized to NAD. The decrease in the optical density of NADH measured photometrically is directly proportional to the pyruvate concentration and thus to the ALT activity. The enzyme’s activity was expressed in IU/l.
Determination of cholinesterase (CHE) activity in blood serum (EC 3.1.1.7)
The cholinesterase activity in blood serum was determined by the means of a spectrophotometric kinetic test based on the hydrolysis of butyryl thiocholine iodide catalyzed by the enzyme contained in the specimen. The thiocholine produced in turn reacts with dinitrobenzoic acid, producing a yellow-colored disulfide. The determination was made at 37°C using reagent sets from Gilford and a Technicon RA-XT analyzer to record the increased absorbance at 405 nm. The enzyme’s activity was expressed in IU/l.
Determination of malondialdehyde concentration in blood plasma
Malondialdehyde (MDA) was measured fluorometrically as 2-thiobarbituric acid reactive substance in blood plasma, according to Ohkawa. 11 Plasma were mixed with 8.1% sodium dodecyl sulfate, 20% acetic acid and 0.8% 2-thiobarbituric acid. After vortexing, samples were incubated for 1 h at 95°C and butanol pyridine 15:1 (v/v) was added. The mixture was shaken for 10 min and then centrifuged. Butanol pyridine layer was measured fluorometrically at 552 nm (515 nm excitation). Tetraethoxypropane was used as the standard. Data were shown as µmol/l plasma.
Ultrasonic imaging
The ultrasonic imaging of the liver was carried out using a Scanner 250 Plus at 3.5 MHz. A series of cross-sectional images in the sagittal, horizontal and inclined planes were taken. The liver size was assessed in the cross-section, using the medioclavicular dimension a-p and the Harbin index (relative proportion of the caudate lobe to the right lobe of the liver) in the cross-section and the thickness index (caudate lobe a-p/left lobe a-p). The portal system, gall bladder and bile ducts; the size and echogeneity of the liver; and the course and size of major vascular trunks, common hepatic duct and common bile duct were evaluated. The dimensions, limits and echogeneity of all the irregular lesions, including the diffused lesions, and focal lengths of the liver parenchyma were described, and their location was provided; the diameters of intra- and extrahepatic bile ducts were determined, and their clearance was evaluated; irregular structures were described; the size and shape of the gall bladder were evaluated; and the thickness and regularity of the gall bladder wall and its lumen were evaluated. 12,13
Statistical analysis
The database was created in the MS Excel 2003. Statistica 6.0 PL software was used for the statistical analysis. For each parameter descriptive statistical indexes were defined (average, standard deviation (SD) or percentage). The distribution regularity was checked with the W Shapiro-Wilk test, while the variance homogeneity was measured with the Levene test. To compare the changes between the specific groups, Kruskal–Wallis one-way analysis of variance by ranks was used. To compare the exposed groups to the control group, t test for independent trials or t test with independent variance estimation or Mann–Whitney U test was used. For quality variables (smoking habits), the chi-quadrate test was used. To assess the correlation, the Pearson or Spearman test was used. Changes with significance level p < 0.05 were assumed as statistically significant.
Results
The Pb-exposed population evaluated did not differ by age, body mass index or employment period, concentration of hemoglobin, smoking and drinking habits from the control group. However, statistically significant differences in the concentration of Pb, ALA and ZPP between the control group and the groups tested were detected. The PbB concentration in the LePb group was more than 3 times that of the controls, and the PbB concentration in the HePb group was nearly 5 times as high as that of the controls. Similarly, the ZPP levels in the LePb and HePb groups were 2 and nearly 4 times as high as those of the controls, respectively. Relative to the control group, the concentration of ALA in the urine of the subjects in the LePb group was 39% higher and that of the HePb group was 45% higher (Table 1).
Age, BMI, time of employment at the company within the group, % of smokers, number of drinks per weekend, measurements of exposure to lead compounds (lead concentration in blood (PbB), ZPP concentration in blood, concentration of ALA) and concentration of Hb in the control group and in the groups exposed to leada

a Values are presented as mean ± SD and range.
BMI: body mass index; ZPP: zinc protoporphyrin; ALA: delta-aminolevulinic acid; Hb: hemoglobin
The numbers of leukocytes in blood were 23% higher in the exposed subjects than in the controls: 27% higher levels were observed for the HePb group and the concentration of MDA was 32% and 45%, respectively. Many of the enzymes were also elevated in the exposed population (combined HePb and LePb groups) relative to the controls: cholinesterase activity was 56% higher, FA was 17% higher and γ-GT was 47% higher. The 19% greater level of activity of AST in the HePb group was a significant increase. In contrast, the concentrations of bilirubin, LDH5 and ALT were not different from the controls in either group of exposed subjects (Table 2).
The quantity of leucocytes in blood, bilirubin concentration, CHE, AST, ALT, LDH5, FA, γ-GT and concentration of MDA in serum in the control group and in the groups of people exposed to leada
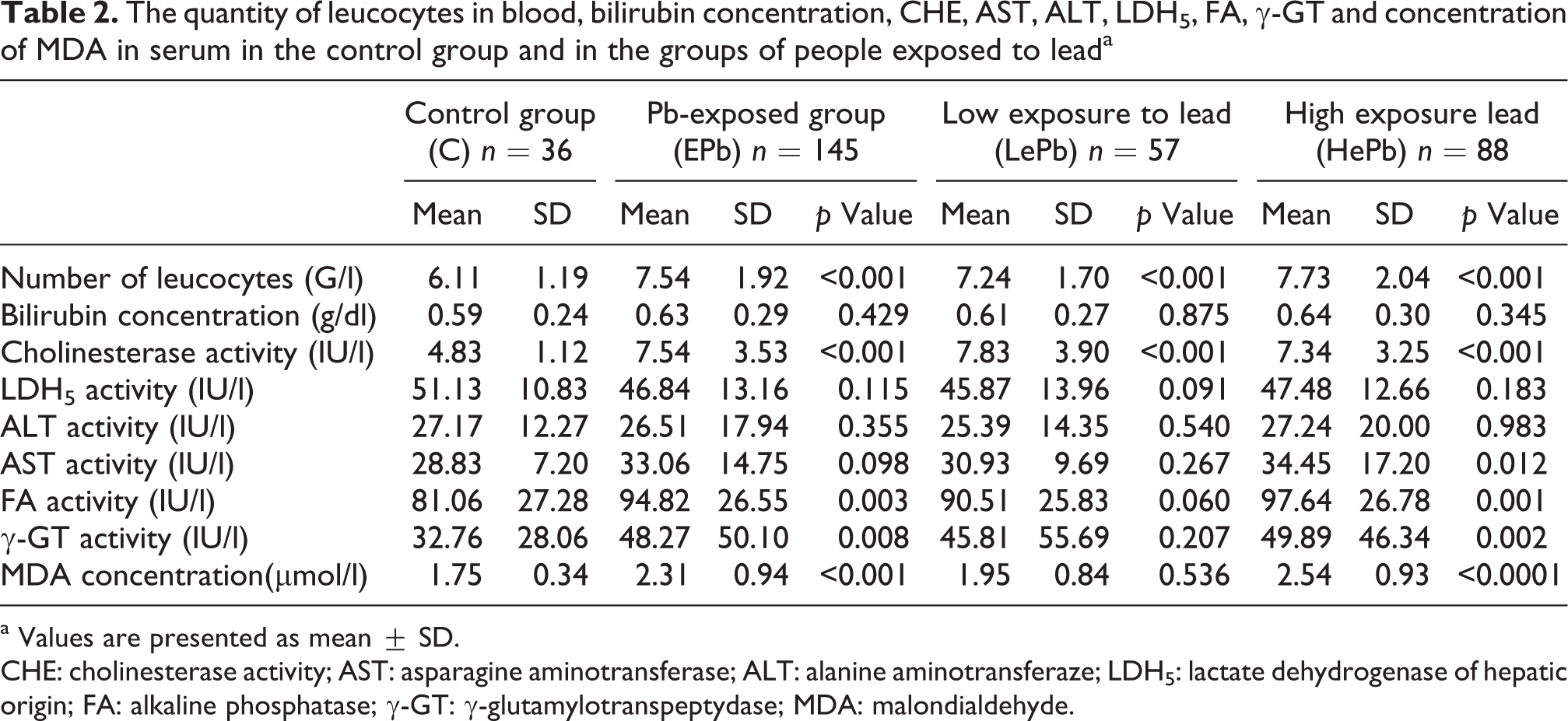
a Values are presented as mean ± SD.
CHE: cholinesterase activity; AST: asparagine aminotransferase; ALT: alanine aminotransferaze; LDH5: lactate dehydrogenase of hepatic origin; FA: alkaline phosphatase; γ-GT: γ-glutamylotranspeptydase; MDA: malondialdehyde.
The size of the liver was larger in the Pb-exposed groups than in the control group. The ultrasonic imaging showed that all the dimensions (Table 3) were between 1% and 8% higher than the values in the control subjects, with approximately half of the measured differences being significantly different from the controls. Moreover, the gall bladder wall was found to be 9% thicker in the exposed subjects than in the control group (Table 4). No differences in hepatic echogeneity or homogeneity between the exposed subjects and the control group were observed.
Dimensions of the liver assessed using ultrasonic imaging for the control and lead-exposed groupsa
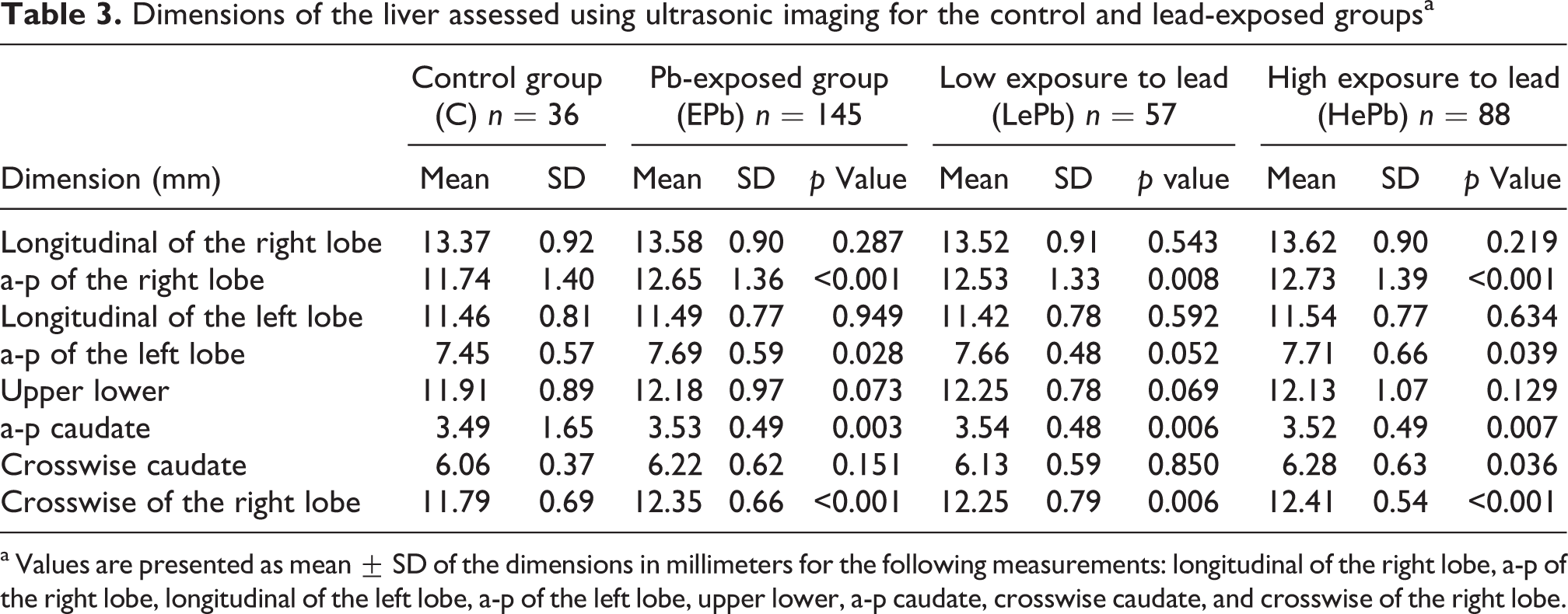
a Values are presented as mean ± SD of the dimensions in millimeters for the following measurements: longitudinal of the right lobe, a-p of the right lobe, longitudinal of the left lobe, a-p of the left lobe, upper lower, a-p caudate, crosswise caudate, and crosswise of the right lobe.
Measurements of liver morphology, PV dimensions, CBD and dimensions and GB wall thickness assessed using ultrasonic imaging in the control and lead-exposed groups

PV: portal vein; CBD: common bile duct; GB: gall bladder.
The AST activity was positively correlated with the PbB concentration (R = 0.15 p = 0.048), ZPP (R = 0.15 p = 0.043) and ALA (R = 0.19 p = 0.012). The FA activity was positively correlated with the concentration of PbB (R = 0.25 p = 0.002) and ALA (R = 0.19 p = 0.012). The activity of γ-GT positively correlated with the concentration of PbB (R = 0.23 p = 0.002) and ALA (R = 0.16 p = 0.030). Besides, there are positive correlations between the a-p dimension of the right liver lobe and concentration of PbB (R = 0.27 p < 0.001), ZPP (R = 0.25 p < 0.001) and ALA (R = 0.19 p = 0.010); the anterior dimension of the right lobe and the concentration of PbB (R = 0.24 p = 0.001), ZPP (R = 0.23 p = 0.002) and ALA (R = 0.20 p = 0.007); the anterior dimension of the caudal lobe and the concentration of PbB (R = 0.15 p = 0.045) and ZPP (R = 0.15 p = 0.046), as well as the gall bladder thickness and the concentration of PbB (R = 0.15 p = 0.045). The concentration of MDA positively correlated with PbB (R = 0,37 p < 0.001), ZPP (R = 24 p = 0.001), FA (R = 0.34 p < 0.001) and γ-GT (R = 0.14 p = 0.05).
Discussion
Lead-associated liver damage or metabolic functions’ disorder may be evaluated indirectly by analyzing the activity of the enzymes released to the blood from damaged hepatocytes, the serum levels of proteins synthesized in the liver, and the concentrations of bilirubin and other metabolic products excreted by hepatocytes to the blood or the bile ducts. 14
Few studies have examined the impact of lead on the livers of people exposed to this element. The tests carried out by Cooper et al. in 301 workers employed at a lead melting and refining facility indicated that the levels of AST were above 50 IU/l in 11.5% of people with PbB concentrations below 70 μg/dl, in 20% of people with PbB concentrations above 70 μg/dl and in 50% of people with PbB concentrations above 100 μg/dl. This study also indicated that there was a statistically significant correlation between the AST activity and the PbB concentration. 15 However, the available studies do not clearly define the chronic effects of Pb on the liver function. 16,17 One study examined the correlations between the PbB concentration and the liver condition in battery factory workers 17,18 during the period between 1988 and 1999. This study indicated a positive correlation between PbB concentrations and γ-GT, but there were no correlations among the other indicators. Other authors have shown that the AST and ALT activities were significantly increased in people occupationally exposed to lead. 19 In another study, the PbB and hepatic enzyme activities were examined over the course of 10 years in bus drivers living in Athens. These subjects were occupationally exposed to the organic lead compounds contained in gasoline. However, during the period of the study, a gradual decrease in the PbB concentration and normalization of the AST and ALT activities were observed, which could have been related to the extensive introduction of lead-free fuel and healthier lifestyle promotion. 20
In the present study, the AST activity was increased by 19%, and the γ-GT activity was increased by 52% in the serum of those exposed to high levels of lead relative to those in the control group. In contrast, no changes in ALT were observed in the exposed population. The literature suggests that increased activities of ALT and AST in the blood are most likely due to the disintegration of the mitochondria after the complete destruction of the hepatic cells. 21 However, since AST and ALT are also present in nonhepatic tissues, the organ or tissue source of the increased serum levels cannot be conclusively determined. Ultrastructural examination of the damaged parenchymal cells of animals experimentally exposed to lead might provide additional information.
The liver enzyme γ-GT is primarily expressed in hepatocyte cell membranes and in the epithelial cells of the intrahepatic bile ducts. The γ-GT activity in the blood serum is exclusively derived from the liver. 22 The increased levels of the plasma γ-GT activity without changes in the plasma ALT activity could suggest that Pb increases the catalytic efficiency of γ-GT rather than disrupting the permeability of the liver cells. The additional induction of the enzyme could have been caused by the long-term consumption of alcohol in the group of people highly exposed to lead.
These analyses showed that the FA activity was increased in the people exposed to lead. Specifically, in the LePb and HePb groups, the FA activity increased by 12% (p = 0.060) and 20% (p = 0.001), respectively, than that of the control group. Moreover, there was a statistically significant correlation between the activity of FA and the lead exposure indicators PbB and ALA. δ-ALA accumulated in lead intoxication can be suggested as a source of ROS, which is now accepted as being associated with the pathophysiology of lead toxicity. 23 Lead ions show a high affinity for sulfhydryl groups of proteins, which may lead to the inactivation of some intracellular enzymes, with phosphatase activity increasing simultaneously. 24 The numbers of free ribosomes and polyribosomes in cellular cytoplasm, where the enzyme is synthesized, are likely decreased by exposure to heavy metals. 25 The statistically significant increases in the activities of FA and γ-GT described herein in the subjects chronically exposed to lead relative to the control group may be explained by the ongoing process of liver adaptation to harmful factors, including the heavy metals.
A few epidemiological and clinical studies have suggested that chronic exposure to Pb may cause deficiencies in the function of the immune system. 26 In the current study, statistically significant increases in the numbers of leukocytes were observed in the groups of people exposed to Pb relative to the control group. Specifically, the number of leukocytes increased by 19% (p = 0.001) and by 27% (p = 0.000) in the LePb and HePb groups, respectively, relative to the control group. These results may suggest a lead-associated inflammatory response. The metal may also modify the cellular and humoral immunological responses, which are associated with the occurrence of inflammatory, allergic and neoplastic diseases. 27 Pb may also regulate human immunological responses at various stages, modifying inflammatory reactions of early and late types, including the number of circulating T and B lymphocytes, natural killer (NK) cells and immunological memory cells. 28
Numerous diseases lead to the diffusion of liver damage with uncharacteristic ultrasonic symptoms, including damage caused by alcohol, in which various levels of adipose degeneration are observed, and damage is associated with a history of exposure to toxins, including environmental toxicants such as heavy metals, and acute and chronic liver inflammation. Ultrasonic imaging is a very sensitive test. Unfortunately, it is relatively nonspecific for diagnosing diffuse lesions. On the basis of the ultrasonic imaging results, we cannot draw any conclusions concerning the etiology and type of the histological lesions. Liver enlargement is the most frequent symptom of a diffuse disease of this organ. 29 At the same time, along with enlargement, the form and structure of the liver change, namely, the edges become rounded. The diagnoses based on the ultrasonic imaging and histopathological examination results are frequently associated with adipose degeneration and cirrhosis of the liver. 30,31
In this study, liver enlargement was observed in the group of people exposed to lead. The evaluation of the liver using ultrasonic imaging showed a statistically significant increase in the size of the right and left liver lobes in the a-p and cross-section, compared with the people not exposed to Pb. The a-p dimension of the left lobe was larger in the groups of exposed people: by 7% in the LePb group (p = 0.008) and by 8% in the HePb group (p = 0.000) compared with the control group. Similarly, the transverse dimension of the right lobe was larger in the groups of exposed people, with increases of 4% (p = 0.006) and 5% (p = 0.000) for the LePb group and the HePb group, respectively, relative to the control group. The a-p dimension of the caudate lobe was 2% larger in the LePb group (p = 0.006) and in the HePb group by 1% (p = 0,007). The Pb-exposed subjects in this study were healthy people, none of whom had previously suffered from known liver inflammation due to infection or from hematological or metabolic diseases. Furthermore, none of the subjects were obese or diabetic, nor were any of them taking any medicines or abusing alcohol. Lead was the only harmful factor.
While evaluating the parenchymal echogeneity, no differences were found in the exposed groups and in the control group. A statistically significant difference, however, was found in the wall thickness of gall bladder, which was 8% larger in the LePb group (p = 0.033) and 9% larger in the HePb group (p = 0.020) compared with the control group. The causes of wall thickening of the gall bladder without its disease include cirrhosis of the liver (portal hypertension, hypoalbuminemia), liver inflammation and decompensated right ventricular heart failure. 32,33
It has previously been shown that the Pb concentration in the bile of people exposed to the metal is several hundred times higher than its concentration in serum. Approximately 8% of absorbed lead is excreted via the bile ducts. 4,34 Thus, long-term exposure to a high concentration of this element may contribute to the development of chronic inflammation of the bile ducts. An additional argument for the possibility that chronic cholestasis may lead to chronic inflammation of the gall bladder and bile ducts is that significant increases were observed in FA, γ-GT and cholinesterase activities (by 52% compared with the control group) in the people exposed to Pb.
One of the most important toxic mechanisms of lead is oxidative stress. Many mechanisms are involved in lead-induced pathologies. First, ALA that accumulates during lead exposition undergoes auto-oxidation and is a source of ROS, second lead induces the production of ROS, directly (effect on membrane lipids) and indirectly, enhancing the levels of superoxide, hydrogen peroxide and hydroxyl radicals. Lead interferes with antioxidant enzymes, such as superoxide dismutase, glutathione peroxidase, catalase.
35
–37
Additionally, lead has an influence not only on the activities of antioxidant enzymes but also on the dose-dependent expression in their gene.
38
Oxidative stress is observed in serum, erythrocytes, seminal plasma and organs as kidney, heart, brain and liver.
3,23,39
In experimental studies in liver concentration of product of lipid peroxidation – MDA increased about 39–80% and in one study over 100%
36
. In the present study, MDA in plasma was 45% larger in the LePb group compared with control and correlated positively with PbB, ZPP, FA and γ-GT. It seems that lipid peroxidation can be one of the toxic mechanisms of lead that may induce moderate cholestasis. Many studies are underway to determine the effect of antioxidant supplementation following lead exposure. N-acetylocysteine, alpha-lipolic acid, S-adenozyl-
The data obtained in this article indicate that the chronic exposure to high concentrations of lead disturbs some enzymatic functions of the liver. Moreover, chronic exposure probably stimulated mitosis in hepatocytes, leading to liver enlargement. This element may also contribute to the inflammatory and cholestatic reactions in the organ.
In conclusion, human exposure to lead compounds was found to cause liver enlargement, lipid peroxidation and to activate inflammatory reactions with the characteristics of moderate cholestasis within the bile ducts, while no characteristics of necrotic damage of hepatic cells were noted. The effects depend on the extent of the lead exposure, with stronger effects occurring at higher exposure levels, particularly for the subjects with PbB values greater than 35 μg/dl.
Footnotes
Conflict of interest
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.