
Abstract
Dental amalgams are a commonly used dental restorative material. Amalgams are about 50% mercury (Hg), and Hg is known to significantly accumulate in the kidney. It was hypothesized that because Hg accumulates in the proximal tubules (PTs), glutathione-S-transferases (GST)-α (suggestive of kidney damage at the level of PT) would be expected to be more related to Hg exposure than GST-π (suggestive of kidney damage at the level of the distal tubules). Urinary biomarkers of kidney integrity were examined in children of 8–18 years old, with and without dental amalgam fillings, from a completed clinical trial (parent study). Our study determined whether there was a significant dose-dependent correlation between increasing Hg exposure from dental amalgams and GST-α and GST-π as biomarkers of kidney integrity. Overall, the present study, using a different and more sensitive statistical model than the parent study, revealed a statistically significant dose-dependent correlation between cumulative exposure to Hg from dental amalgams and urinary levels of GST-α, after covariate adjustment; where as, a nonsignificant relationship was observed with urinary levels of GST-π. Furthermore, it was observed that urinary GST-α levels increased by about 10% over the 8-year course of the study among individuals with an average exposure to amalgams among the study subjects from the amalgam group, in comparison with study subjects with no exposure to dental amalgams. The results of our study suggest that dental amalgams contribute to ongoing kidney damage at the level of the PTs in a dose-dependent fashion.
Introduction
Dental amalgams are a commonly used dental restorative material. Amalgams are sometimes referred to as ‘silver fillings’ because of the silver color and its use as a ‘filling’ for dental cavities; however, amalgams are about 50% mercury (Hg) with the remainder composed of silver as well as tin, copper, and zinc. Amalgams were shown to significantly contribute to Hg body burden. 1,2
One issue of amalgam safety is the effect of Hg exposure on kidney integrity. Studies show that Hg selectively accumulates in the proximal tubules (PT) of the kidney, 3,4 and Hg affects the PT of the kidneys more than the distal tubules (DT). 5 The distribution of inorganic Hg into PT cells in the rat increased with increasing concentrations of Hg; however, little correlation was found between Hg and dose in DT cells. 3 Why PT cells are more vulnerable is not completely understood; however, it is postulated to be due, in part, to the distribution of enzymes and transport proteins important for the uptake of Hg into PT cells. 6
Investigators hypothesized that because PTs are more vulnerable to Hg than DTs, kidney stress markers specific to the PTs and DTs could be used to determine kidney injury. 7 These investigators examined urinary glutathione-S-tranferases (GSTs), both GST-α and GST-π. GST-α is localized in the PT and GST-π is found in the DT. 8,9 Elevated urinary GST-α level suggests PT damage and elevated urinary GST-π level is suggestive of DT damage. 10,11
Investigators examined both GST-α and -π in children with and without amalgams (amalgams versus resin composites) over an 8-year-period as a part of the Casa Pia children’s amalgam trial (the parent study). 7 The parent study showed no significant difference between the two groups on GST-α and -π levels; however, the dose-dependent relationship between cumulative Hg and GST-α and -π levels was not examined.
Our study further examines the Casa Pia children’s amalgam data and specifically examines the potential dose-dependent relationship between cumulative Hg exposure from dental amalgam fillings and urinary GST-α and -π levels. Our hypothesis is that the levels of GST-α should be more related to Hg exposure from amalgams than the levels of GST-π.
Subjects and methods
The parent study protocol for collecting the raw data examined in our study was approved by the institutional review boards at the University of Washington and the University of Lisbon. All parents or guardians gave written consent, and all children provided signed assent. Principal design and analytical issues involved in this trial as well as principal outcome measures were previously reported. 7,12 We reanalyzed datasets provided to us from the parent study.
Study population
The cohort of children examined in our study came from the Casa Pia clinical trial on the health effects of amalgams. 7,12 As described previously, 7,12 the children examined in our study were the residents of the Casa Pia school system in Lisbon, Portugal, and were of 8–12 years old at the study inception. Eligibility requirements excluded children with preexisting neurological or developmental disabilities. Subjects were initially randomized to amalgam (treatment) or composite resin (control) dental care groups. Children were evaluated at baseline and at seven subsequent annual intervals after the initial dental treatment. An extensive battery of neurobehavioral, neurological, renal function, urinary Hg, and urinary porphyrin assessments were used in each evaluation. In addition, detailed information was collected regarding the composition, number, size, and positioning of dental fillings in each child’s mouth. Table 1 summarizes the baseline measurements recorded on the cohort of children examined in our study. In our analyses, we did not modify the original dataset provided to us from the parent study.
A summary of the baseline measurements for subjects examined in our study.
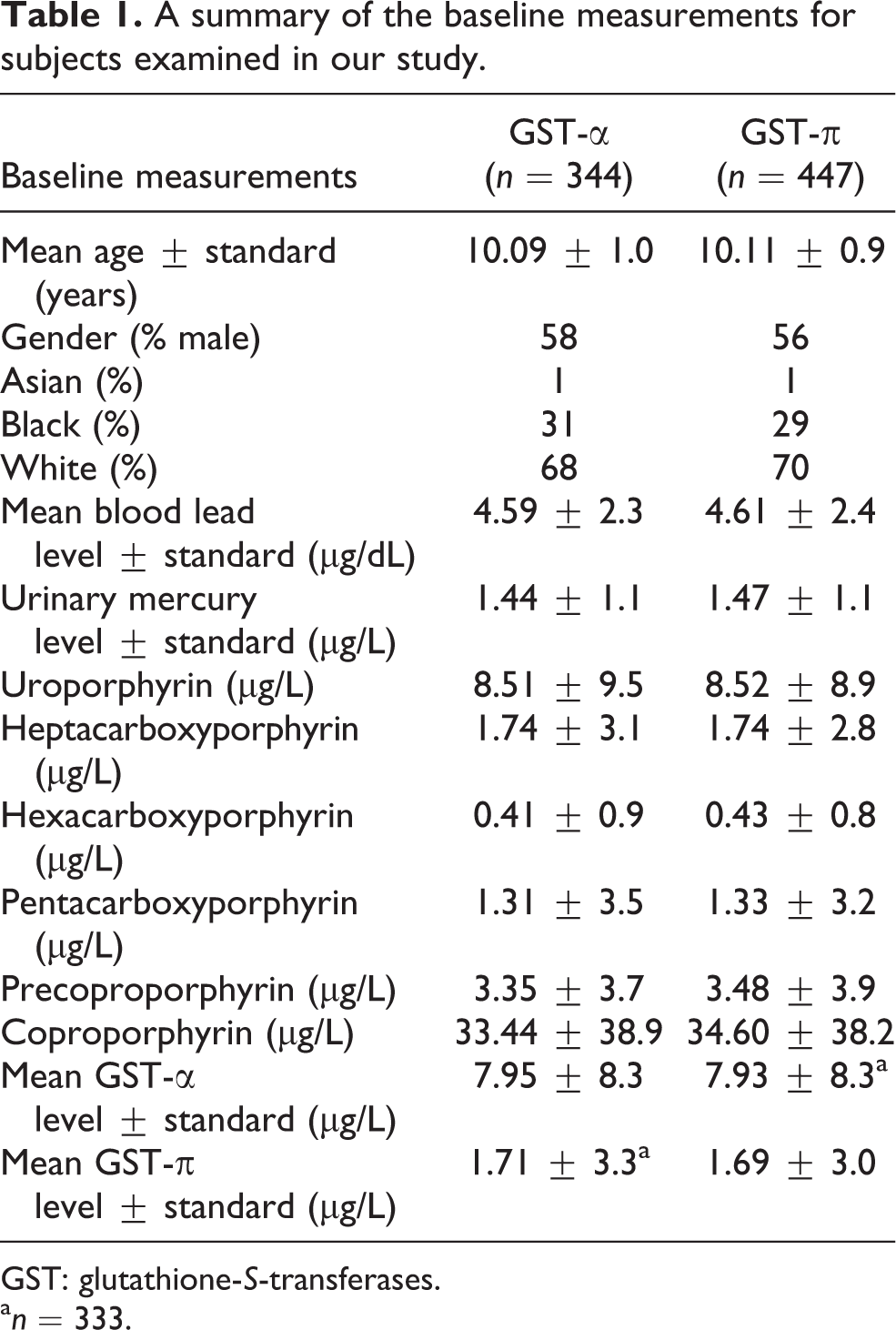
GST: glutathione-S-transferases.
a n = 333.
Urine sample collection procedures and measures of urinary GSTs
As described previously, a urine sample (∼50 ml) was collected from each child at baseline and at each subsequently scheduled annual visit to the University of Lisbon School of Dental Medicine for dental, neurological, and neurobehavioral evaluations. 7,12 It was not possible to correct for dilution of urine samples by normalizing with urinary creatinine levels because this information was not provided to us by the investigators involved with the parent study. Concentrations of GSTS-α and -π in urine samples were measured by enzyme immunoassay employing kits purchased from Biotrin USA (Cedarknolls, New Jersey, USA). 7 The assay procedure is based on the sequential addition of sample, enzyme conjugate, and substrate to microtiter wells coated with anti-α and anti-π GST immunoglobulin G. A Molecular Devices UV-Max microplate reader capable of 96 simultaneous ultraviolet absorbance determinations was employed for GST quantization.
Estimating the Hg exposure variable
The number of amalgam restorations of the buccal, distal, lingual, and occlusal surfaces (no amalgam restorations were recorded for medial or incisal surfaces) was counted and the level of exposure was computed by applying scores of 1.0, 2.0, or 3.0 for small, medium, or large restorations, respectively, then adding these scores for each restoration of each tooth for each year. Other weighting schemes for large, medium, and small sizes were also considered (i.e. 1.0, 4.0, 9.0; 1.0, 8.0, 27; 1.0, 1.0, 1.0; and ln(1.0), ln(2.0), ln(3.0)). However, the weighting scheme that best correlated with urinary Hg levels (using only amalgam subjects who were 12 years or older to avoid any issues with baby teeth) was 1.0, 2.0, 3.0. Thus, this weighting scheme was used to create the yearly exposure scores used in all of our subsequent analyses. In addition, since baby teeth (which comprised 22% of restorations) are smaller than adult teeth, the exposure for baby teeth was taken to be one half the exposure for adult teeth (i.e. with scaling factors of 0.5, 1.0, and 1.5 for small, medium, and large restorations, respectively). Furthermore, as subject weights were not available, each yearly exposure score was divided by the subjects estimated body mass index (BMI) based on the subject’s age and gender. The estimated BMI scores for age and gender utilized were obtained from the Centers for Disease Control and Prevention (CDC)’s BMI 50th percentile clinical growth charts (http://www.cdc.gov/growthcharts/clinical_charts.htm#Summary). The BMI-normalized yearly exposure scores were accumulated from year to year. Thus, a restoration contributed to exposure for the year it was placed and each subsequent year, unless a tooth had been lost in a given year, in which case its exposure contribution was set to zero for that year and all subsequent years. This procedure was applied to both baby teeth and adult teeth. The exposure score for each year was assumed to affect the outcome measure for the same year. The assumption that exposure in a year affected outcomes in the next year was also considered. However, the first assumption produced a better fitting model.
Statistical analyses
In all statistical analyses, a two-tailed p < 0.05 was considered statistically significant. Both amalgam and composite groups were included in the analysis but all participants in the composite group had an amalgam exposure level of zero except for two subjects who received amalgam restorations in error. Since repeated measures were collected for each subject, a mixed-effects repeated-measures model was used to estimate the relationship between exposure and outcome. This type of model takes account of the correlation between repeated observations of the same subject and allows for the inclusion of subjects with missing data. Each model included terms for subject, including the repeated measurement factor, exposure, and the following covariates: gender, race, baseline level (i.e. study year 1) of urinary Hg, baseline measurements of each urinary porphyrin measures (uroporphyrin, heptacarboxyporphyrin, hexacarboxyporphyrin, pentacarboxyporphyrin, precopropophyrin, and coproporphyrin), and the baseline level of lead in each subject’s blood. Interaction terms were added if they contributed significantly to the model. Ordinarily, one would use study year as the repeated factor because it measures time from the beginning of the intervention. Since, the present analysis is not comparing intervention groups, it is more reasonable to use age as the repeated factor. For both outcomes, a log transformation was used to satisfy the normality requirement for the statistical procedure. This model can be specified as follows:

where yia is the log of urinary GST level for the ith subject at age a, Eia is the amalgam exposure level for the ith subject at age a, ci 1 to ci 11 represent the 11 covariates described above for the ith subject, vi and uia are subject and age random effects, respectively. The coefficient b 1 represents the effect of amalgam exposure level on GST-α or -π levels. Table 2 summarizes mean Hg exposure from dental amalgams by the age of the study subjects.
A summary of mean mercury exposure from dental amalgamsa by age of study subjects.b
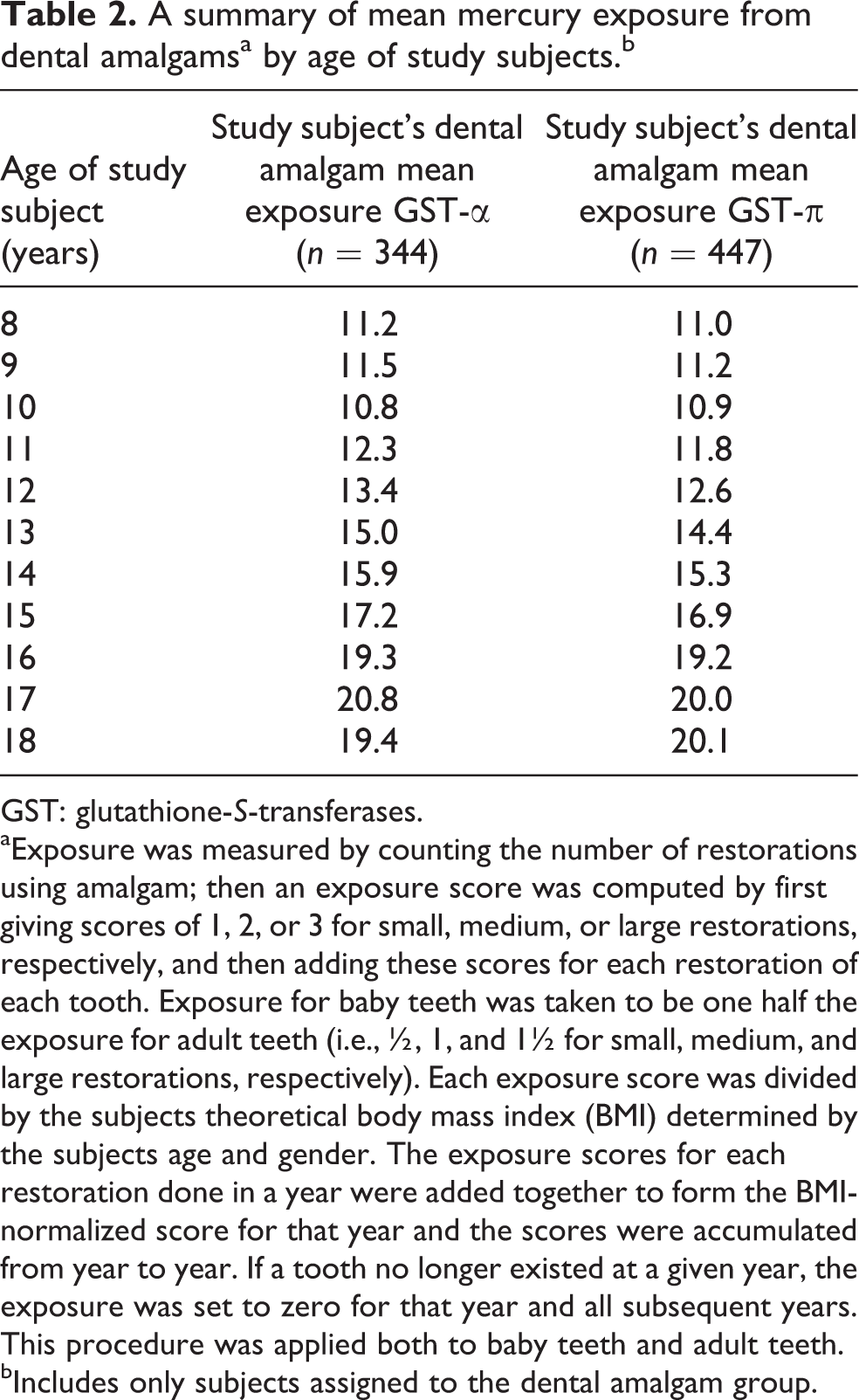
GST: glutathione-S-transferases.
aExposure was measured by counting the number of restorations using amalgam; then an exposure score was computed by first giving scores of 1, 2, or 3 for small, medium, or large restorations, respectively, and then adding these scores for each restoration of each tooth. Exposure for baby teeth was taken to be one half the exposure for adult teeth (i.e., ½, 1, and 1½ for small, medium, and large restorations, respectively). Each exposure score was divided by the subjects theoretical body mass index (BMI) determined by the subjects age and gender. The exposure scores for each restoration done in a year were added together to form the BMI-normalized score for that year and the scores were accumulated from year to year. If a tooth no longer existed at a given year, the exposure was set to zero for that year and all subsequent years. This procedure was applied both to baby teeth and adult teeth.
bIncludes only subjects assigned to the dental amalgam group.
Results
Table 3 summarizes the relationship between the BMI-normalized cumulative exposure to Hg from amalgams and kidney function parameters (GSTs-α and -π) in the model constructed. A significant exposure effect means that the outcome is significantly affected by the level of exposure after adjustment of covariates. A positive estimate means that higher levels of exposure are associated with higher levels of the outcome measured, while a negative estimate means that higher levels of exposure are associated with lower levels of the outcome measured. The results showed an adjusted significant dose-dependent correlation between increasing Hg exposure from amalgams and increasing urinary GST-α levels, whereas no significant adjusted correlation was found between increasing Hg exposure from amalgams and increasing urinary GST-π levels.
A summary of the relationship between cumulative exposure to mercury from dental amalgamsa and outcome urinary mercury measurements.

GST: glutathione-S-transferases.
aExposure was measured by counting the number of restorations using amalgam then an exposure score was computed by first giving scores of 1.0, 2.0, or 3.0 for small, medium, or large restorations, respectively, then adding these scores for each restoration of each tooth. Exposure for baby teeth was taken to be one half the exposure for adult teeth (i.e. 0.5, 1.0, and 1.5 for small, medium, and large restorations). Each exposure score was divided by the subjects estimated body mass index (BMI) determined by the subject’s age and gender. The exposure scores for each restoration done in a year were added together to form the BMI-normalized score for that year and the scores were accumulated from year to year. If a tooth no longer existed at a given year, the exposure was set to zero for that year and all subsequent years. This procedure was applied both to baby teeth and adult teeth.
bOutcome estimate was adjusted for the baseline level (i.e. study year 1) of urinary mercury, each porphyrin measure, gender, race, blood lead level, and GST-α level.
cOutcome estimate was adjusted for the baseline level (i.e. study year 1) of urinary mercury, each porphyrin measure, gender, race, blood lead level, and GST-π level.
Discussion
GST-α levels significantly correlated with exposure from amalgams in a dose-dependent fashion. Because GST-α is a means of assessing kidney injury, the results suggest accumulation of Hg at the levels of the PTs of the kidney and subsequent renal injury. The change in GST-π was nonsignificant. Hg accumulates in the PT, thus GST-α would be expected to be more related to Hg exposure, than GST-π.
Investigators previously examined markers of tubular damage and glomerular dysfunction and amalgam exposure in 101 healthy adults. It was observed that markers of tubular damage and glomerular dysfunction were both higher in the exposed than the unexposed group. These investigators concluded that the amalgams are unsuitable due to possible renal damage. 13
Several autopsy studies have shown that Hg levels in the kidneys can be related to amalgam exposure. 14 For example, investigators examined seven adults with 11–33 surfaces containing amalgams and controls containing no amalgams, and found that the amalgam group had kidney levels of 433 ng Hg/g of wet tissue while the controls had 49 ng/g. 15 Subsequently, examination of kidney Hg levels in dental workers found they had 5–10 times more Hg in their kidney than controls. 16 Other investigators studied total Hg levels in the kidney of 18 cadavers. 17 Total Hg levels were higher in subjects with a greater number of amalgams (>12) than subjects with fewer amalgams (0–3) in the kidney. Most studies that examine Hg levels in the kidney come from autopsy studies; however, one recent study examined Hg levels in 109 living donor kidneys combined with information about diet, amalgams, and other types of exposure. 18 Kidney Hg levels increased by 6% with every additional amalgam, and amalgam was the main determinant of kidney Hg.
GST-α levels significantly correlated with exposure from amalgams in a dose-dependent fashion. Because GST-α is a means of assessing kidney injury, the results suggest accumulation of Hg at the levels in the PTs of the kidney and subsequent renal injury. The change in GST-π was nonsignificant. Hg accumulates in the PT, thus GST-α would be expected to be more related to Hg exposure, than GST-π.
In considering our observations of an association between Hg exposure from dental amalgams and ongoing damage to the PTs of the kidney, investigators have reported that chronic damage to PTs resulted in maladaptive repair with interstitial capillary loss, fibrosis, and glomerulosclerosis. 19 These investigators concluded that the selective damage to the PTs can drive the formation of interstitial fibrosis, capillary rarefaction, and potentially glomerulosclerosis, substantiating a direct role for damaged PTs in the pathogenesis of chronic kidney disease. This is significant because chronic kidney disease remains one of the leading causes of death in the developed world, and hence the results of our study suggest that ongoing Hg exposure from dental amalgams may play a plausible role in the pathogenesis of human chronic kidney disease.
It is also noteworthy that our results are not consistent with those observed from the parent study. 7 Our study is differentiated from the parent study in that we constructed statistical models to specifically examine the relationship between dose-dependent dental amalgam exposure variables and kidney integrity biomarkers with the examination of multiple covariates. Furthermore, our study used a more sensitive statistical model than the parent study, and hence, our study may have been able to detect statistically significant effects of dental amalgam exposure variables on kidney integrity biomarkers that were not possible given the statistical model used in the parent study.
Strengths/limitations
In considering the strengths/limitations of our study, the design utilized was strong, and its strength helped to reduce any potential limitations. The overall design of our study was constructed a priori to the actual examination of any study subjects, and the study subjects examined were randomly assigned to dental amalgam or composite groups at baseline. As a result, potential biases regarding potential reasons for exposure to a specific treatment or regarding specific types of evaluations undertaken on study should not have adversely impacted the data analyzed. Furthermore, the randomization, helped to ensure that both exposure groups examined had similar baseline characteristics. In addition, both the amalgam and composite groups were of moderate size and not numerically weighted in a direction (i.e. there were several hundred study subjects in both the amalgam and composite groups), helping to reduce potential biases regarding the sample composition in the statistical modeling used.
After initial random assignment of study subjects to amalgam/composite groups, detailed information was collected regarding specific biological parameters at baseline. Subsequently, detailed information was collected regarding exposure to dental amalgams (i.e. size, number, location, etc.) and repeated measurements of specific biological parameters. As a result, the repeated measurements examined were collected in a controlled fashion, so that potential limitations, such as changes in sample collection techniques or analysis over the course of multiyear study of study subjects, should have minimally impacted the data. Unlike the parent study, 6 our examination of the data utilizes detailed statistical models to evaluate multiple covariables and detailed analyses of exposure variables in the data, which helped to strengthen our analyses. Furthermore, analyses undertaken on actual collected data helped to confirm the validity of the assumptions made in the statistical models employed.
In considering the limitations of our study, our study had minimal information regarding past exposure to Hg or other sources of Hg exposure during the study among the study subjects. As a result, it is possible that these unaccounted for sources of Hg may have created confounding in the data examined, helping to reduce the significance of the findings observed. Despite this potential, our study found significant correlations. In addition, our study has the limitation that only individuals that were healthy at initial presentation were allowed entry into the study. As a result, the biological effects observed from amalgam exposure may be specific to healthy individuals, and not necessarily the consequences of Hg exposure from amalgams in less-than-healthy individuals. Another potential limitation is study subjects were only followed for 8 years. Hence, it was not possible to evaluate the potential long-term consequences of amalgam exposure over the course of decades to these individuals. Despite this fact, over the course of 8 years of our study, Hg exposure from amalgams did significantly impact the biological parameters examined. In addition, a further potential limitation of our study was the moderate size of the sample examined.
Another limitation of our study was that CDC’s BMI 50th percentile clinical growth charts were utilized on the subjects examined. It is possible that there may be differences in the BMIs between children in the United States and Portugal, but given that the BMI data was applied equally to subjects regardless of their dental status, this should not have impacted the overall direction of the results observed. Other limitations include that we were unable to quantitatively measure certain factors such as smoking, chewing of solid foods, chewing gum, drinking hot drinks, and so on, that may increase the release of Hg from amalgams. Similarly, we were not able to account for position and/or removal of amalgams, which can significantly increase Hg exposure. As a result, our study may underestimate the full extent of amalgam’s contribution to the kidney integrity biomarkers. Finally, a limitation of our study was that Portugal is known as a high-seafood consumption culture, as a result of this higher baseline exposure to Hg probably somewhat reduced the significance of the results observed, and in cultures with less seafood consumption the effects of Hg exposure from dental amalgams may be more striking.
Conclusion
The results observed were compatible with our hypothesis that because Hg accumulates in the PTs, urinary GST-α (suggestive of kidney damage at the level of PTs) levels would be expected to be more related to Hg exposure than urinary GST-π (suggestive of kidney damage at the level of the DTs) levels. Overall, the present study using a different and more sensitive statistical model than the parent study, revealed a statistically significant dose-dependent correlation between cumulative exposure to Hg from amalgams and urinary GST-α level, after covariate adjustment, where there was no significant relationship between urinary GST-π levels. Furthermore, urinary GST-α levels increased by about 10% over the 8-year course of the study among individuals with an average exposure to amalgams among the study subjects from the amalgam group, in comparison with study subjects with no exposure to dental amalgams as shown in Table 4. Future studies should extend our results in order to determine whether Hg exposure from amalgams significantly contributes to overt, medically diagnosed kidney disease at the level of the PT.
Estimated urinary GST-α and GST-π levels (µg/L of urine) by age and level of exposure.

GST: glutathione-S-transferases.
Footnotes
Funding
This study received funding from the nonprofit International Academy of Oral Medicine and Toxicology (IAOMT), nonprofit Institute of Chronic Illnesses, Inc., and the nonprofit CoMeD, Inc.
Conflict of interest
The authors declared no conflicts of interest