
Abstract
Background: A recent report showed increased frequency of apparent life-threatening events (ALTEs) in infants treated with the homeopathic medication GaliCol-Baby (GCB). The premise was that the ALTEs resulted from toxic effects of the drug’s components. We examine an alternative explanation. Method: The toxicological literature was searched for known reactions to the various GCB components, noting doses and reported symptoms. Dosage quantities and severity of reaction to the GCB were ranked independently by two groups of physicians, and a dose–response curve was generated. Reported toxic doses and symptoms were compared with those of the GCB series. The homeopathic literature was searched as well to determine the propensity of the GCB components to cause ALTE symptoms, when given in homeopathic doses to healthy volunteers (proving). Results: Doses ingested in the GCB series were 10–13 orders of magnitude smaller than those reported to cause toxic reactions in humans. There was poor correlation between symptoms with GCB and toxic profiles of the components. A nonsignificant, inverse relationship between dose and severity of reaction was observed. Conversely, four GCB components (in homeopathic doses) had a high propensity to produce at least one of five symptoms which define ALTE, two of which had intermediate to high propensity to produce three symptoms. Conclusions: It is unlikely that the ALTE following ingestion of GCB was a toxic reaction to any of the drug’s component. Homeopathic theory may explain this linkage, though further research is needed to understand the pathogenic effects of highly diluted homeopathic compounds.
Introduction
In all biological systems there are a number of reactions that produce varying degrees of stress, either internally (e.g. allergic or immune-mediated responses) or externally, such as toxic reactions. Often, when observing an externally induced reaction—especially when not described elsewhere in the scientific literature—there is a tendency to assume that the reaction is a toxic one, even if symptoms are unlike those described in the past with the offending agent. One example of such an assumption is a recently published study, which found a high frequency of apparent life-threatening events (ALTEs) in infants treated with the complex homeopathic medication GaliCol-Baby (GCB), a commonly used remedy for the treatment of infantile colic. 1 The premise of the authors of this study was that the ALTEs were the result of toxic effects of the components of the medication.
An ALTE was originally defined in 1986 by the National Institutes of Health (NIH) as ‘an episode that is frightening to the observer and that is characterized by some combination of apnea (central or occasionally obstructive), color change (usually cyanotic or pallid but occasionally erythematous or plethoric), a marked change in muscle tone (usually marked limpness), choking or gagging. 2 The ALTE is not an infrequent phenomenon among infants, with a rate of 1.5 per 1,000 live births reported in the Netherlands. 3 The ALTE has been attributed to a number of etiologies, though only rarely it is due to the ingestion of an identifiable drug or toxin.4–9 Medications implicated in ALTE include ephedrine, barbiturate, phenytoin, nicotine, dihydroergotamine, oxybenzone, and drugs of abuse such as cocaine. 9
The GCB (Unda SA, Brussels, Belgium) is a popular over-the-counter complex homeopathic medication, frequently used for infantile colic, though no scientific evidence exists to support this practice. Unlike classic homeopathy, in which remedies are individualized, based on intrinsic traits of the patient, complex homeopathy incorporates the use of standard mixtures, which are based on the patient’s symptoms. In a recent publication, Aviner et al. present a case–control study linking ALTE with ingestion of GCB. 1 The authors attribute the symptoms to ‘toxic’ effects of three of the GCB compounds: Veratrum album (false helleborine), Citrullus colocynthis (bitter apple) and Strychnos nux vomica (strychnine tree). These herbs exhibit significant toxicity when taken in large doses and were thus assumed to cause the ALTE symptoms in infants.
Highly diluted compounds have been in use by the homeopathic community for over 200 years. Homeopathy maintains that these preparations cause symptoms in healthy individuals, and can paradoxically cure sick individuals presenting with those same symptoms (Law of Similars). Homeopathic pathogenetic trials (provings from the German word for test) entail the process of administering various highly diluted compounds to healthy consenting volunteers and observing the symptoms induced. From the collective expression of symptoms, it is possible to speak of the ‘propensity’ of induction of a given symptom by a certain substance. Symptoms experienced weakly, or by a single ‘prover,’ are listed as Grade 1; symptoms experienced in a pronounced manner by many provers are considered Grade 3, with Grade 2 indicating an intermediate propensity to produce symptoms This information is typically used in selecting the appropriate single remedy in classic homeopathy for a given patient based on his or her symptomatology, according to the Law of Similars. 10 The possibility that these dilutions may be bioactive is vehemently contested. This article will examine the feasibility of this explanation for the effects of the GCB, offering a novel explanation, which can explain the ALTE symptoms based on the principles of homeopathic medicine.
Methods
Literature Search
An in-depth search of the toxicological literature for the components of GCB was conducted. The terms Veratrum album, Citrullus colocynthis, Strychnos nux vomica, Cuprum metallicum, Bryonia, Matricaria chamomilla and Magnesium phosphoricum (magnesium phosphate dibasic trihydrate) were entered into the MEDLINE, Toxline, Clinical Evidence, The Cochrane Library, Embase, IBID, IPA, Mayoclinic, Medscape, MEDLINE Plus, Natural Medicines Comprehensive Database and other search engines to identify any case reports, clinical research (controlled and uncontrolled trials) or any other relevant publication on the subject, in both English and German. The compounds, their doses and symptoms produced were noted. A computer-based homeopathic database (Radar Homeopathic Software—www.archibel.com) was searched to determine the propensity of the various GCB components to cause the symptoms seen in the Aviner series, as presented in Table 1 .
Reported cases of apnea following GaliCol-Baby ingestion a

NA: not available, GCB: GaliCol-Baby.
aBased on Aviner et al. 1
Dose–Response Analysis
Concentrations of the components in GCB were calculated based upon the Homeopathic Pharmacopoeia Convention of the United States (HPUS) 1981. 11 Because it was not possible to ascertain from Aviner’s data the exact amounts of GCB ingested, a ranked approach was adopted. Two internists, blinded mutually as well as to patient outcome, were asked to rank the GCB dosages given to infants in Aviner’s series from lowest to highest. Correlation was examined and, if found, dosage ranks were averaged. A pediatric intensive care physician and the director of a pediatric emergency department, also blinded to the dosage and to each other’s response, were independently asked to rank the severity of disease of the 11 cases presented in Aviner’s study. The correlation was then tested between the average dosage rank and severity, as determined by each of the two sets of physicians. Neither national nor international marketing data on GCB could be obtained. The association between ordinate variables was performed using Pearson’s correlation (PASW, version 18, 2009). Calculations did not take into consideration the conversion from liquid to dry weight. Comparisons are on a broad measure of order of magnitude.
Results
Toxicological symptoms
Poisoning with Veratrum album, is rare, with the Swiss Toxicology Information Center collecting national data on poisonings—reported only eight severe cases between 1966 and 1994. 12 Symptoms of toxicity include vomiting, nausea and abdominal pain, followed by bradycardia, hypotension and, in severe cases, cardiac conduction abnormalities and even death.13,14 The fatal dose of dried Veratrum powder in adults is estimated at 1–2 g (about 15–30 mg/kg body weight). 15 The quantity of Veratrum album in one dose of GCB is less than 0.3 × 10–10 mg, the equivalent of or less than about 0.1 × 10–10 mg/kg per body weight in an average infant, resulting in a difference of at least 13 orders of magnitude in dosage. Poisoning with Citrullus colocynthis is exceedingly rare as well. Three cases of acute colitis were reported in 1989, 16 and no fatalities have been reported in humans. Symptoms gleaned from animal studies include decreased protein synthesis, renal failure and hemoconcentration, with lethal doses at 2.5–10 g/kg/day. 17 One dose of GCB contains less than 10–9 g of colocynthis (less than 3 × 10–10 g/kg per body weight in an average infant), 10 orders of magnitude below the lethal dose.
The most toxic component of Strychnos nux vomica is strychnine. Brucine, also present in this plant, is 50–100 times less toxic. The first signs of strychnine intoxication are anxiety, nausea and vomiting, followed by twitching of facial muscles, generalized muscular rigidity and increased sensitivity to noise, touch and any stimulus. Symmetric cramps of the skeletal muscles, with opisthotonus and apnea may occur. In severe cases, muscular response may be provoked by slight external stimuli. Death may occur within 20–30 minutes after the ingestion of a large dose of this herb. The estimated toxic dose for this herb in humans is 0.4 mg/kg, with a lethal dose of 5 mg/kg. 18 One dose of GCB contains less than 10–10 mg/kg of Strychnos nux vomica extract or less than 3 × 10–11 mg/kg in an average infant, for a difference of at least 11 orders of magnitude in dosage.
Cuprum metallicum, or metallic copper, dissolves with great difficulty and thus, for practical purposes, does not cause acute toxic effects. 19 Some reports exist of chronic toxicity and even a fatal outcome in a psychotic patient who swallowed 275 copper coins, a metal which can cause ‘metal fever’ when inhaled as dust. 20 Bryonia alba root is a caustic agent and irritant, though far less toxic than Strychnos nux vomica. 21 Symptoms include severe diarrhea and vomiting, abdominal pain, dizziness, hypothermia, dilated pupils, perspiration and cardiopulmonary collapse. Sublethal doses may cause bronchial irritation, hepatomegaly, diuresis with urinary tenesmus and cardiac depression. 22 In case reports of human Bryonia alba intoxication, the doses used were not mentioned. However, it is likely that if the more toxic Strychnos nux vomica is considered safe in those concentrations present in the GCB medication, then it can be assumed that the less toxic Bryonia alba, present in the same concentration, should be at least as safe.
Matricaria chamomilla is a familiar herb in Western nations, and it has been granted food status in the Unites States. 23 Rare case reports of allergic reactions to this herb can be found. The lethal dose 50% (LD50) of chamomile oil exceeds 5 g/kg for oral toxicity in rats and acute dermal toxicity in rabbits. 24 The content of chamomilla in one dose of GCB is 1.34 × 10–9 g (about 0.5 × 10–9 g/kg body weight in an average infant), 10 orders of magnitude below the LD50 in rats. Magnesium phosphoricum is considered, in large doses, to be a contact-irritant of skin and eye. Oral administration induces vomiting and is not known to produce serious toxic effects. 25 No case reports of toxicity in humans were found nor data concerning LD50.
Table 2 summarizes the toxic symptoms of the GCB components as found in the toxicological literature. Of the known symptoms of the GCB components, only vomiting, rigidity and apnea were observed in the infants described in the report by Aviner et al. Table 3 presents the quantity of GCB components present in a single dose of the medication, along with the reported toxic dose reported elsewhere in the literature and finally, the order of magnitude difference between the two.
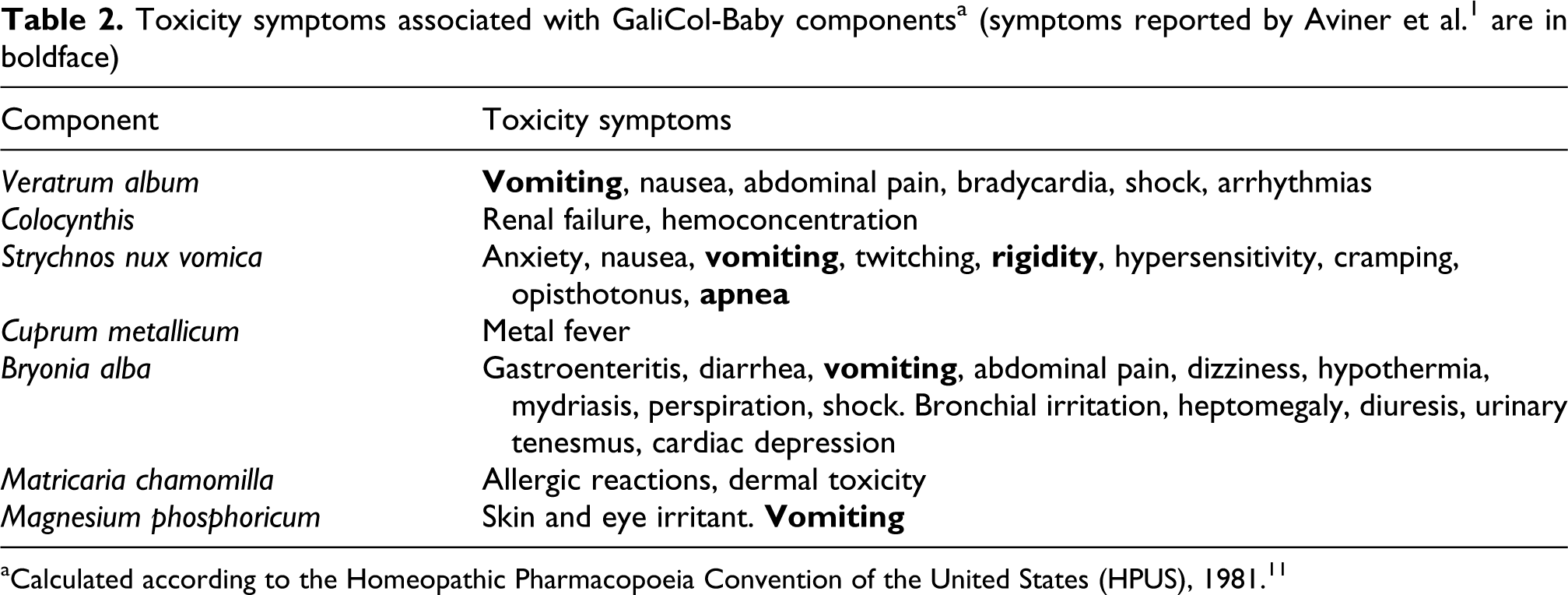
aCalculated according to the Homeopathic Pharmacopoeia Convention of the United States (HPUS), 1981. 11
Quantity of components in GCB and recognized toxic doses

LD50: 50% lethal dose, GCB: GaliCol-Baby.
aAll homeopathic components were homeopathically prepared and diluted to the indicated degree. To this solution was added inert diluent to a volume of 1.0 ml, and 0.143 ml of each solution was added to 99 ml diluent to create 100 ml of GCB.
Homeopathic symptoms
Table 4 summarizes the propensity of the seven active components of GCB to cause the ALTE and non-ALTE symptoms observed in the Aviner series. Four components (Veratrum album, Cuprum metalicum, Bryonia and Chamomilla) have an intermediate to high propensity to produce at least one of the five symptoms that define ALTE, when given in homeopathic dilutions. Two of these (Veratrum album and Cuprum metalicum) have an intermediate-to-high propensity to produce three of the four possible ALTE symptoms. The term ‘sudden death’ does not appear in the homeopathic literature and thus could not be evaluated. The GCB components also show an intermediate-to-high propensity to cause all but one of the non-ALTE symptoms presented in Aviner’s series.
Propensity of homeopathic remedies to produce symptoms of ALTE a
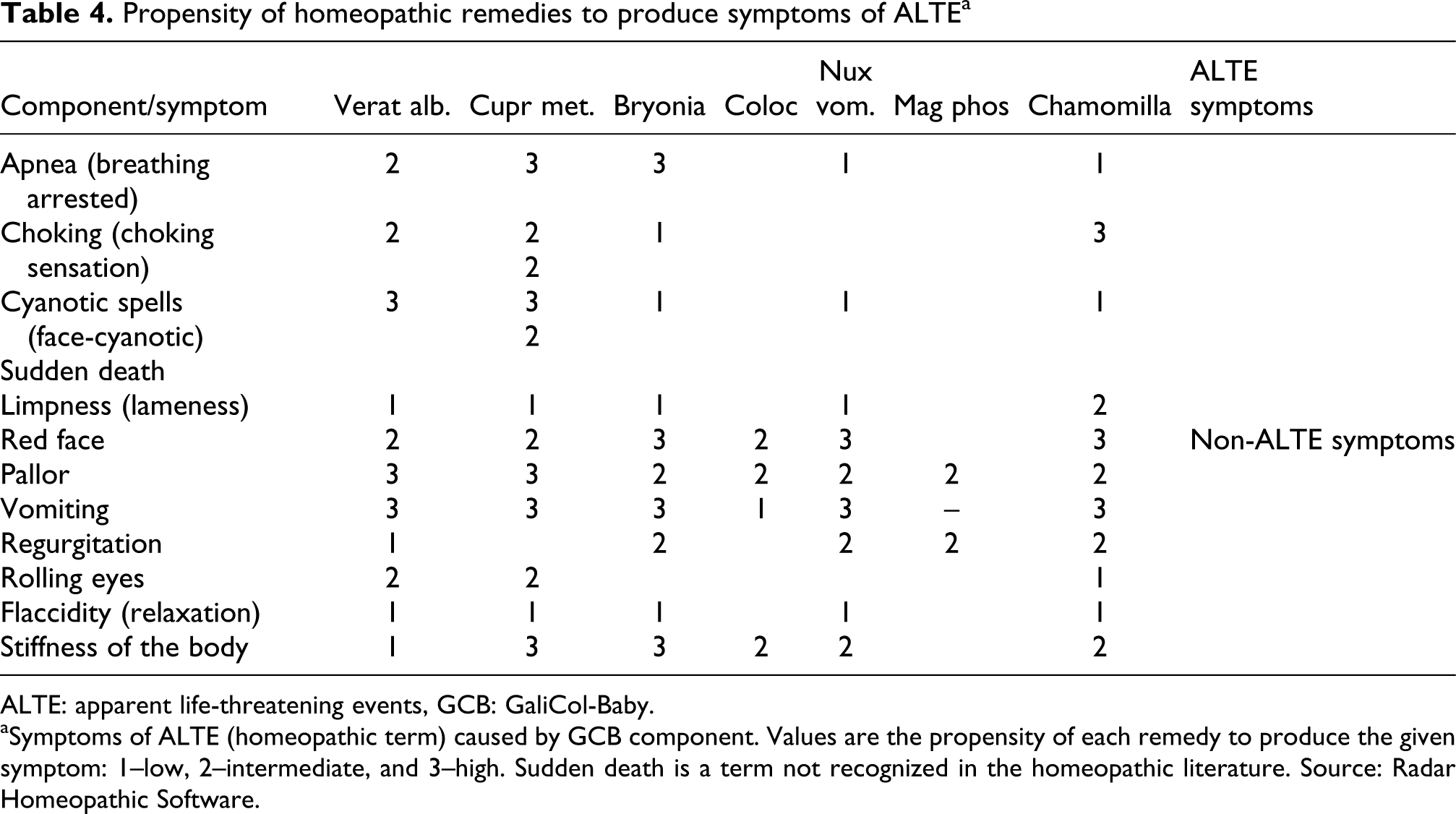
ALTE: apparent life-threatening events, GCB: GaliCol-Baby.
aSymptoms of ALTE (homeopathic term) caused by GCB component. Values are the propensity of each remedy to produce the given symptom: 1–low, 2–intermediate, and 3–high. Sudden death is a term not recognized in the homeopathic literature. Source: Radar Homeopathic Software.
Dose–response analysis
Physicians questioned on dosage ranking agreed in six of eight cases for which dosage data were available. The disagreement was of one degree of rank between two subjects (Pearson correlation coefficient r = 0.97, regression line slope ≈ 1). Physicians queried on severity indicated a nonsignificant inverse relationship between dose and severity (Pearson coefficient –0.398, p =0.328 for physician A and –0.489, p = 0.219 for physician B).
Discussion
The article by Aviner et al. leaves little doubt as to the association between GCB ingestion and ALTE. However, the doses ingested are between 10 and 13 orders of magnitude below that considered toxic. Furthermore, the symptoms observed among the infants correlate poorly with reported toxic symptoms attributed to the GCB components. Apnea, an important symptom of ALTE, is a final stage of Strychnos nux vomica intoxication. However, the infants in the GCB series showed none of the symptoms that typically precede apnea in Strychos nux vomica poisonings (Table 2). It should be noted that this compound is present in GCB at a concentration 11 orders of magnitude below that considered toxic. The other toxic components of GCB are similarly at infinitesimal concentrations, when compared with the toxic doses reported. Indeed, if there is any dose–response relationship it is an inverse one, albeit nonsignificant. The appearance of ALTE immediately following ingestion of GCB in four of the infants is not in keeping with a toxicological mechanism, but rather with the purported action of proving as described in homeopathy. Finally, though marketing data were unavailable, GCB is a widely sold over-the-counter pediatric preparation in Israel. Were this preparation indeed toxic, we would have expected a far larger number of cases of severe reactions, reflecting the toxicological profile of GCB components.
We believe that a toxic reaction to the active components of GCB is unlikely. However, the possibility of a toxic reaction to one of the ‘inactive’ ingredients should be taken into consideration. Gas chromatography mass–spectrometry analysis of the medication has revealed ethanol, propanol, pentanol, glycerol and sugars. Ethanol is not a listed component of GCB, and, lacking quantative data, we conjecture that these alcohols are residual compounds left over from the homeopathic preparation process. The reported lethal dose of ethanol in children is 3 g/kg, and ethanol blood concentration of 100 mg/dL may result in severe toxicity. To avoid toxicity, the American Academy of Pediatrics has established 25 mg/dL as a maximal blood ethanol concentration not to be exceeded following a single dose of alcohol-containing medication. 26 To achieve this blood ethanol concentration, the upper limit of ethanol dose in a single dose of medication is 0.19 mL/kg or 0.15 g/kg. However, even if the total liquid component of GCB was alcohol, a single dose of GCB (3–5 drops) would contain only 0.5–0.8 × 10–4 g/kg of 30% alcohol, three orders of magnitude below that dose. For this to occur, the infants would have had to receive 1,000 doses to approach the level permitted by the American Academy of Pediatrics. Other inactive GCB components—xylitol 30%, sorbitol 10%, glycerin 10%, arome banane 0.3%, quinoleine yellow 0.0012%, methyl parahydroxybenzoate natrium 0.1% and propyl parahydroxybenzoate natrium 0.01%—are in frequent pharmacologic use and are not known to cause significant toxic effects. Thus, we believe it is unlikely that the inactive ingredients could explain the associated ALTE.
If the link between GCB and ALTE is unlikely to be due to a toxic reaction to either the active or inactive components of the medication, an alternative explanation should be sought. The infants treated with GCB were essentially healthy individuals given a combination of remedies in highly diluted, homeopathic preparation. In homeopathic pathogenetic trials, a proportion of healthy individuals treated with homeopathic remedies that are not homeopathically indicated will express symptoms typical to those remedies. Indeed, these ‘trials' form the foundation for the use of single homeopathic remedies. We believe that Aviner et al. have presented an extraordinary and compelling example of homeopathic proving on a population-based scale. This is supported by the extremely minute quantities of the GCB components—far below those anticipated to cause any toxic effect; by the inverse dose–response relationship observed; and by the strong correlation between the ALTE and non-ALTE symptoms reported by Aviner et al. and those reported in homeopathic provings of GCB components. In consenting adults, in whom homeopathic pathogenic trials are typically performed, these symptoms would have likely been trivial and unremarkable.
The implications of this approach, if validated, extend far beyond the need for the manufacturers of homeopathic products to provide warning labels on their products. Aviner and colleagues may have inadvertently demonstrated that highly diluted homeopathic remedies have true biological effects, in a case series of 11 infants—the first such revelation reported in the conventional medical literature. We believe it is likely that such phenomena have in fact occurred in the past, but these have most probably been overlooked, either due to the trivial impact anticipated on adults or older children or due to the relatively inaccurate collection of data which typifies clinical trials and postmarketing surveillance.
Other reports of toxic effects of homeopathic remedies have been reported in the literature as well. These reports invariably show a lack of understanding as to what constitutes ‘homeopathic’ medicines, making it extremely difficult to ascertain as to whether there is indeed a toxic effect at play or whether the resulting symptoms are due to the phenomenon of proving. For example, Kuenzli et al. describe a case of childhood bullous pemphigoid, which was purportedly caused by a homeopathic treatment. 27 The authors mention a long list of homeopathic compounds ingested by the patient, yet do not provide the exact dilutions administered. Others present the dilutions but exhibit ignorance as to the significance of such information.
The mechanism by which GCB could have caused these symptoms remains as yet unknown. As such, laws requiring the use of warning labels on homeopathic products are warranted, as are those regarding qualification of those practicing homeopathic, especially with the neonate and infant population. Further research into the pathogenic effects of highly diluted compounds is in order, and the clinical implications of this research should prove intriguing.
Footnotes
Acknowledgements
We are grateful to Dr Cornelius Gropp for his helpful and insightful comments on the manuscript; to Dr Moshe Puder and Mag Ruth Shiloh for their help in quantifying the components; and to Ms Yaffa Kleiner Brandwein for proofreading and corrections.
No conflict of interest exists for any of the authors.
No funding was provided for this study.