
Abstract
Objective: The aim of this study was to analyse the caustic and household detergent exposure cases were admitted to the Department of Emergency Medicine at Dokuz Eylul University Hospital (EMDEU) between 1993 and 2008. Methods: Age, sex, reason of exposure, clinical signs, rate of endoscopy in oral exposures, treatment attempts, length of hospital stay and outcome were evaluated. A chi-square test was used to analyse statistical differences. Results: Caustic exposures accounted for 8.5% (1160 cases) and 4.1% (1988 cases) of all poisonings in children and adults, respectively. Female/male ratio of caustic exposure poisonings was 0.8. Most of the exposures were unintentional (158, 86.8%). Intentional exposures were common in cases between 19 and 29 years old (χ2 = 25.685, p < 0.001). The most common caustic substance was alkaline (106, 58.3%) followed by acidic (47, 25.8%) and other household detergents (28, 15.4%). Vomiting (35.7%), nausea (14.8%) and sore throat (13.1%) were the most common clinical signs. The patients who had endoscopy, the most frequent finding was first-degree damage (58.7%). A 48-year-old man died from intentional hydrochloric acid ingestion. Conclusion: Because of the large number of unintentional caustic exposures, parent education is very important to decrease the caustic exposures in children.
Introduction
Caustic exposure is an important problem in developing countries. Children younger than 6 years are at particularly high risk of caustic poisoning at home. According to the data from poison information centers, the exposures to household cleaning substance are on the higher side of the poisonings. 1,2 Caustics are classified into acidic, alkaline substances and disinfectants. Although household detergents are generally of anionic or nonionic nature and they are known to be non-toxic, they can cause nausea and vomiting. Some of them such as laundry powders and dishwasher detergents which contain phosphate and carbonate may cause caustic burns. 3
Caustic exposures can cause serious health effects such as esophageal perforation, stricture formation and necrotic extension to the tracheobronchial tree. 4 Depending on the exposure routes, caustics can be the cause of gastrointestinal, dermal and ocular burns. The severity of the damage depends on the type, quantity and concentration of the ingested substance. Acidic and alkaline substances have high toxic effects. Alkaline substances generally cause more severe injuries than acidic substances in the esophagus by rapidly penetrating and producing liquefaction necrosis. Although vomiting, hypersalivation and abdominal pain indicate serious esophageal damage, the presence or absence of oral lesions is a poor indicator of esophageal injury. 5,6 The treatment is supportive and emesis and gastric lavage are contraindicated because of the perforation risk. 6 Activated charcoal has not been found to provide any benefit in caustic exposures. 6
In this retrospective descriptive study, we analysed the caustic and household detergent exposures with demographics, requirement of performing endoscopy in oral exposures and endoscopy findings in patients admitted to our emergency service in a 16-year period. We have also presented a lethal case of hydrochloric acid ingestion.
Methods
This study was approved by the Institutional Ethics Committee of the School of Medicine at Dokuz Eylul University (15.11.2009 no:123/2009). In this retrospective study, we scanned the patients’ charts with caustic and household detergents exposures, who were admitted to the Department of Emergency Medicine at Dokuz Eylul University (EMDEU) between 1993 and 2008. The patients admitted to EMDEU were categorized into three groups depending on whether they had acidic, alkaline or detergent exposures. Data about the demographics, type of exposed substance, distribution according to route and reason of the exposure (unintentional or intentional), endoscopy findings in oral exposures, length of hospital stay and the outcome of the patients were analysed retrospectively from the patient charts.
Performing endoscopy was decided depending on the exposed substance and the reason of exposure. Endoscopic gradings are provided in Table 1 . 7 All data were entered into the Statistical Package for Social Sciences for Windows 15.0 (SPSS 15.0). While children were defined as ≤18 years old (<6 years, 7–12 and 13–18), adults were defined as >18 years old (19–29, 30–39, 40–49, 50–59, 60–69 and >69 years). Statistical analysis was performed using the chi-square test. Results were considered statistically significant when p < 0.05.
Classification of endoscopic grading of esophageal injuries

Results
Over a 16-year period, although 290 caustic and household detergent exposure cases were admitted to EMDEU, only 182 of them could be evaluated from the patients’ charts, retrospectively. In our emergency room, 9.2% of the poisoning cases were caustic exposures among all of the poisoning cases (100.0%, n = 3148) admitted to EMDEU. Of the 182 cases admitted to EMDEU, 81 (55.5%) of them were male (54.5% and 56.6% children and adults, respectively). Female:male ratio of the 182 cases admitted to EMDEU was 0.8. Mean age of children and adults was 4.1 ± 0.5 and 38.7 ± 1.9 years, respectively. The age of children and adults ranged from 0.8 through 86 years (Table 2 ). The rate of caustic exposures in all poisonings were 8.5% in children (n = 1160) and 4.1% in adults (n = 1988).
The gender and age distribution of caustic exposures

Most of the exposures were unintentional (158, 86.8%) in patients, both in children (95.9%, n = 95) and in adults (75.9%, n = 63). Intentional exposures were observed between 13 and 18 years in children and between 19 and 49 years in adults. Intentional exposures were significantly high between 19 and 29 years in adults (χ2 = 25.685, p < 0.001). There was no sexual dominance in children or adults among intentional exposure attempts (Figure 1). The most common caustic substances were alkaline (58.3%, n = 106) followed by acidic (25.8%, n = 47) and detergents (15.4%, n = 28). Frequently exposed acidic and alkaline substances were hydrochloric acid (55.3%, n = 26) in acidic exposures and sodium hypochlorite in alkaline exposures (66.9%, n = 71).

Distribution of causes for caustic and detergent exposures by gender in children and adults.
Alkaline caustic exposures were higher than that of acidic and detergent exposures both in intentional and unintentional exposures (62.5%, n = 15 for intentional and 57.5%, n = 91 for unintentional; Figure 2). Most of the exposed caustics were labeled (87.9%, n = 160). The sources of the caustics were bleach (40.6%, n = 74), dishwasher detergents (8.8%, n = 16), lime solvents (8.2%, n = 15), oil solvents (6.9%, n = 12) and the others.

Distribution of caustic substances.
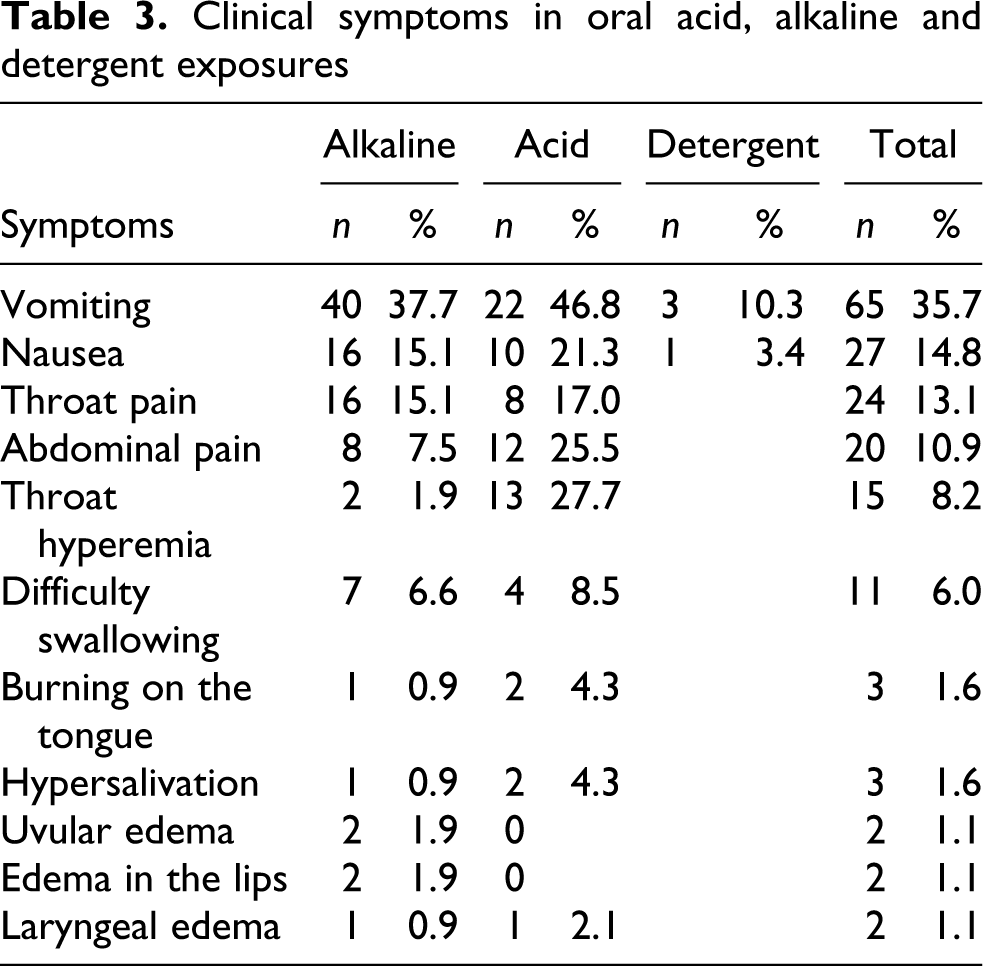
Oral ingestion (93.4%, n = 170) was the main route of exposure. According to history, 9.9% of the patients (n = 18) had already eaten yoghurt and drunk milk. On presentation, 41.2% of the patients were asymptomatic in the emergency room. The most common findings in the exposed patients were vomiting (35.7%) followed by nausea (14.8%) and sore throat (13.1%) in oral exposures (Table 3 ). Withhold all oral feedings, providing fluid and electrolyte balance was recommended in all patients. Endoscopy was performed in 27.0% (n = 46) of the oral exposures consisting of acidic (42.5%) and alkaline ingestions (24.5%). Endoscopy was not required in alkaline caustic ingestions significantly (76.1%, n = 83, χ2 = 4.177, p < 0.05). The frequent findings in endoscopy were first-degree damage (58.7%) followed by no damage (26.1%), second- (8.7%), third- (4.3%) and fourth-degree (2.2%) damages. First-degree damage was common in acidic (65%) and alkaline (53.9%) exposures. Second-degree damage was found in 15% of the acidic exposures (Figure 3). The rate of symptomatic patients were 62.9% (n = 107). Endoscopy was performed only for a small portion of symptomatic patients (38.3%, n = 38). The rate of performing endoscopy in asymptomatic patients were 10.6% (n = 8), and 9.3% (n = 7) of them had endoscopic findings lower than third-degree damage.
Clinical symptoms in oral acid, alkaline and detergent exposures

Endoscopy findings of the acid and alkalis in oral exposures.
In children (n = 91), endoscopy was performed in 16.5% (n = 15) for oral ingestions. First-degree damage was common in acidic and alkaline ingestions (50%, n = 4 and 42.8%, n = 3) followed by no damage and second- and third-degree damages.
Duration of hospital stay were 4.8 ± 1.0 hours for detergent exposures, 17.9 ± 4.9 hours for alkaline exposures and 24.4 ± 5.9 hours for acidic exposures. More than half of the patients (60.4%) were observed in the emergency service and 18.1% of them were referred to the outpatient clinics for further evaluation. There were no records about the outcomes of the 20.8% patients in the charts (Figure 4). A 48-year-old man admitted to the intensive care unit (ICU) died because of the intentional exposure of hydrochloric acid.

Outcomes of exposures to acid, alkalis and detergents.
Case report
A 48-year-old man was admitted to EMDEU 2 hours after ingestion of nearly 500 ml of hydrochloric acid. The patient vomited and his clothes were whitened. According to medical history, the patient was in depression. On admission, agitation, tachypnea, difficulty in swallowing and copious amount of secretion were the main signs and symptoms. His Glasgow Coma Scale (GCS) was E4M5V6. Vital signs were arterial blood pressure (ABP) 139/74 mmHg, pulse 48/min and respiratory rate 16/min. There was a compensatory metabolic acidosis on admission. Because of the perforation risk, endoscopy was not planned. In the observation period, the patient was intubated because of deteriorated respiration. Repeated arterial blood gas analysis showed a deep metabolic acidosis (pH 7.15). Bicarbonate was given intravenously and the patient was transferred to the ICU. The GCS was E1M1V1. Laboratory examinations revealed the following: glucose 186 mg/dL, BUN 20.8 mg/dL, creatinine 2.0 mg/dL, Na+ 139 mEq/L, Ca++ 10 mEq/L, Cl– 135 mEq/L, Hb 16.2 mg/dL, WBC 29.4, Plt 202.000, AST 53 IU/L and ALT 20 IU/L. In the following 4 days, the patient was given ciprofloxacin, metronidazole, vancomycin and imipenem/cilastatin. Because of the hemodynamic instability, a supportive inotropic therapy was performed. Fresh frozen plasma (4 units) and erythrocyte suspension (2 units) were also administered by transfusion. Because of the free air in the abdominal radiography, he was operated in the fourth day of admission to the ICU. Total gastrectomy, vagotomy, esophagiectomy, tube duodenostomy, jejunostomy, splenectomy and bilateral tube thoracostomy were performed. The patient was dialysed 2 days after operation. ABP decreased during the hemodialysis. The patient died on the sixth day of the hospitalization because of the failure of supportive treatment for cardiopulmonary arrest.
Discussion
We analysed the caustic exposure cases admitted to the Dokuz Eylul University Emergency Service, retrospectively, over a period of 16 years. The American Association of Poison Control Centers 8 reported over 200,000 telephone enquiries regarding caustics and household detergent exposures (8.6% of all poisonings) in 2008. The household cleaning substances are reported to constitute nearly 10% of the poisonings, according to data from poison information services. 1,2
There is limited data related to caustic and household detergent exposure rate in Turkey and some other developing countries. In some reports from emergency services, caustic exposure was found to be the second cause of poisonings in children; and it is suggested to be the back rank of the poisonings in adults among all poisonings. 9,10 Although a male dominance in childhood and female dominance in young adults were reported in overall poisonings, no sexual dominance was reported either in adults or in children in our study. In a study from Macedonia, a female dominance was reported in caustic exposures. 11
Reasons of caustic exposures are generally intentional in adults and unintentional in children, according to previous reports. Acids are the most encountered caustics in intentional ingestions. 12 –14 In our study, most of the poisoned patients were children under 6 years, with unintentional caustic exposures, and adults between 19 and 49 years with intentional caustic exposures. Adolescents between 13 and 18 years also had intentional caustic exposures. Although the intentional exposure rate was higher in patients between 13 and 49 years, a sexual dominance was not found in the age groups.
All over the world, the use of household cleaning agents such as sodium hypochlorite and sodium hydroxide is common. 15 In a study by Havanond, although acidic ingestions were found to be higher in intentional ingestions, alkaline ingestions were found to be higher in accidental ingestions. 16 In our study, alkaline caustic exposures were higher both in intentional and unintentional exposures. Additionally, alkaline substances, especially sodium hypochlorite was found to be the most encountered caustic agent. Common use of sodium hypochlorite for cleaning purpose in households in our country may be the reason of this finding.
The main clinical manifestations of caustic exposures are nausea, vomiting, abdominal pain, shock, irritation or burns of the oropharyngeal mucosa, esophagus, and stomach and acidosis in acid exposures. 3 In our study, approximately 40% of the patients were asymptomatic and the most common clinical findings were vomiting and nausea. Serious clinical findings such as uvular edema, burning on the tongue and lip edema were rare. Clinical findings were not found to be different in intentional or unintentional acidic or alkaline exposures. There was only one fatal caustic exposure caused by hydrochloric acid ingestion in our study. Intentional hydrochloric acid ingestions can cause massive gastric necrosis, coagulopathy, renal failure and metabolic acidosis. 17,18 A patient with severe hydrochloric acid ingestion complicated by myocardial infarction was also reported. 19 In our patient, metabolic acidosis was marked. Endoscopy could not be performed because of the perforation risk. Although urgent surgical operation was performed, the patient failed to respond to supportive treatment for cardiopulmonary arrest.
It was shown that the presence or absence of oral lesions is a poor indicator of caustic-induced esophageal injury. Although several studies recommend that early endoscopy should be performed with care in symptomatic patients, there are no strict guidelines for endoscopy in caustic ingestion patients. 5,14,16,20 In our study, endoscopy was required in a quarter of the patients who ingested a caustic agent. Endoscopy criteria were determined according to the severity of the poisoning rather than the presence or absence of the oral lesions. In our study, endoscopy requirement rate was found to be higher in acidic ingestions than that of alkaline ingestions. This finding is compatible with the previous reports related to simple household cleaning substances that caused insignificant esophageal injuries requiring no intervention. 21
Induced vomiting, neutralization with water or milk, activated charcoal and gastric lavage are not recommended in caustic exposures, except nasogastric aspiration, which can be performed during large quantities of acid ingestions to prevent metabolic acidosis. Supportive treatment such as withholding oral feeding and providing fluid–electrolyte balance are beneficial in caustic exposures. 22 In our study, all supportive treatment attempts were provided properly. Because of the retrospective nature of the study, there were some missing data about the results of the poisonings. However, unknown results could not be severe exposures because of the lack of endoscopy and ICU data registrations of the patients who had missing outcomes in our hospital.
Conclusion
In our retrospective study, more than half of the caustic exposure patients were children. While unintentional caustic exposures were common in children under 6 years, intentional exposures were common in adolescents. There was one deadly acid caustic exposure in our retrospective data. Because of the large number of unintentional caustic exposures, parent education is very important to decrease the caustic exposures in childhood.
Footnotes
Acknowledgements
This study was presented as a poster in Turkish Pharmacology Society, 20th National Pharmacology Congress, 3rd Clinical Toxicology Symposium, p. 230, in Antalya, Turkey, 2009 and submitted for evaluation poster presentation in XXXI International Congress of the European Association of Poisons Centres and Clinical Toxicologists in Crotia 2011.
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.