
Abstract
Objective: The objective of the present study was to determine oxidant and antioxidant status in infants with hyperbilirubinemia and/or kernicterus and to find whether there is a relationship between bilirubin level and oxidant/antioxidant status. Patients: The study includes 69 full-term newborns (neonates with hyperbilirubinemia needing phototherapy [Group 1, n = 36] and neonates with kernicterus [Group 2, n = 33]) and 25 age-matched healthy newborn. Results: Plasma total antioxidant capacity (TAC) and serum total oxidant status (TOS) were significantly higher in Groups 1 and 2 than the control group. There was a significant difference between Group 1 and control cases for malondialdehyde (MDA; p < 0.001). Total free sulfhydryl group (TTHI) values were significantly elevated in Group 1 compared to Group 2 and control cases. Correlation analysis showed that the correlation between total bilirubin (TB) and TAC, TOS, MDA and oxidative stress index may be expressed by a quadratic curve. After phototherapy, a statistically significant increase in nitrite level was observed. Conclusion: We demonstrated that the relationship between serum TB and antioxidants and oxidative stress could be expressed by a quadratic correlation curve.
Introduction
Apparent hyperbilirubinemia is a common complication in approximately 60% of healthy full-term newborns. 1 The total bilirubin (TB) level does not exceed the physiological limits in the majority of cases. However, it may rarely rise to very high levels and cause kernicterus. 1 This is the situation with irreversible neurological damage. Kernicterus was not a very rare condition before 1970s. The underlying cause in the majority of cases was hemolysis due to rhesus (Rh) isoimmunization. 1 This frequency decreased to very low levels with modern treatment modalities including exchange transfusion, phototherapy and intravenous immunoglobulin (IVIG). 1 The mortality rate in kernicterus has been reported to be 4.3%. However, the rate of serious sequelae has been reported as high as 84%. 1 Infants with kernicterus are exposed to important cytotoxic effects with increased protein oxidation related to high levels of bilirubin, decreased glucose-6-phosphate dehydrogenase and ATPase enzyme activity. 2 Therefore, these cases are thought to be related to higher oxidant stress. However, when the contribution of bilirubin to the total antioxidant capacity and antioxidant characteristic are assessed together, it is seen that there are many studies in the literature assessing the relationship between bilirubin and total antioxidant capacity (TAC), total oxidant status (TOS) and oxidative stress index (OSI). 2 Besides, phototherapy and exchange transfusion in infants with hyperbilirubinemia have positive or negative effects on these systems. However, no study was found in the literature about antioxidant system and oxidative stress in infants with kernicterus.
In this study, oxidant and antioxidant status were evaluated in infants with hyperbilirubinemia and kernicterus. Our aim was to determine oxidant and antioxidant status in these infants and to find whether there is a relationship between phototherapy and oxidant/antioxidant status.
Materials and methods
Patients and controls
The study included 69 full-term newborns (body weights of >2500 g) with hyperbilirubinemia and/or kernicterus who were hospitalized at Department of Neonatology, Faculty of Medicine, Yuzuncu Yil University, and 25 age-matched healthy newborn. Patients had no disorders other than hyperbilirubinemia. Infants in the patient group were divided into two groups: Group 1 included 36 infants with hyperbilirubinemia exceeding phototherapy limits and Group 2 included 33 infants with kernicterus. Latest guidelines from the American Academy of Pediatrics (AAP) for management of jaundice in a normal term newborn have been used to define phototherapy and exchange transfusion limits. The diagnosis of kernicterus was made by using clinical and physical examination findings (such as lethargy, decreased feeding and hypotonia, hypertonia, high-pitched cry, retrocollis, opisthotonus, impairment of upward gaze (setting sun sign), fever and seizures) and laboratory studies (high bilirubin level and absent auditory brainstem responses). 3
In blood samples, the following parameters were studied before therapy: blood group, complete blood count, liver and renal function tests, TB, direct bilirubin, indirect bilirubin, prothrombin time, partial thromboplastin time, serum electrolytes, direct Coombs, glucose-6-phosphate dehydrogenase (G6PD), thyroid hormones, urinary culture, TAC, TOS, OSI, malondialdehyde (MDA), total free sulfhydryl groups (TTHI), nitrate, nitrite and nitric oxide (NO) levels. These tests were re-performed in all infants included in the study groups before discharge from the hospital. For studies of oxidative enzymes and antioxidant capacity, obtained blood samples were stored at –28°C after centrifugation. The mentioned tests were also studied only once in the control group.
Patients with any predisposing condition for bilirubin neurotoxicity including sepsis, urinary tract infection, respiratory distress, major congenital malformations, congenital heart disease, asphyxia, metabolic acidosis, low birth weight and small for gestational age were excluded from the study. Infants with prematurity, G6PD deficiency or TORCH (Toxoplasma gondii, Rubella, Cytomegalovirus and Herpes simplex) infections, hepatitis and hypothyroidism were also not included in the study.
Complete blood count and biochemical parameters
Complete blood count was measured by using the Coulter STKS complete blood device, Scatter Pac, Lyse III and Isoton-III solutions. Electrolytes, renal and liver function tests were analyzed in Biochemistry Laboratory in our hospital using Bayer Opera Autoanalizer and Biotrol kits.
TAC
Plasma TAC levels were determined using a novel automated colorimetric measurement method developed by Erel. 4 The results are expressed as mmol Trolox equivalent/L.
Total free sulfhydryl groups
Free sulfhydryl groups of serum samples were assayed according to the method of Ellman 5 as modified by Hu et al. 6 The concentration of sulfhydryl groups was calculated using reduced glutathione as free sulfhydryl group standard and the result was expressed as millimolars.
TOS
Serum TOS was determined using a novel automated measurement method, developed by Erel. 7 The results are expressed in terms of micromolar hydrogen peroxide equivalent per liter (mmol H2O2 equiv./L).
MDA
Plasma lipid peroxides were evaluated by the fluorometric method based on the reaction between MDA and thiobarbituric acid (TBA).8,9 The values were presented as µmol/L.
OSI
The percentage ratio of TOS to TAC yields the OSI, an indicator of the degree of oxidative stress. 10 OSI (arbitrary unit) ¼ TOS (mmol H2O2 equiv./L)/TAC (mmol Trolox equiv./L).
Nitrate, nitrite and NO measurements
NO reacts with molecular oxygen and accumulates in the plasma as nitrite (NO2) and nitrate (NO3) ions. Thus, the stable oxidation end products of NO, NO2 and NO3 can be readily measured in biological fluids and used in vitro and in vivo as indicators of NO production. Plasma nitrite levels were measured with Griess reaction. 11 Briefly, samples were initially deproteinized with Somogyi reagent. 12 Total nitrite (nitrite + nitrate) was measured after the conversion of nitrate to nitrite by copporized cadmium granules by a spectrophotometer at 545 nm (Ultraspect Plus, Pharmacia LKB Biochrom Ltd., UK). Results were expressed as micromoles (µM) per liter plasma.
Ceruloplasmin measurement
Enzymatic activity of ceruloplasmin was measured according to Erel’s method. 13 In this method, ferrous ion is oxidized to ferric ions via ceruloplasmin ferroxidase activity. The results were expressed as unit per liter (U/L). 13
Statistical analyses
Statistical analyses were performed using the commercial program SPSS 17. Conformity of continuous variables to normal distribution was assessed using the one-sample Kolmogrov-Simirnov test. For descriptive statistics, the mean was used for the variables with normal distribution, and the median was used for the variables without normal distribution. The chi-square test was used for comparison between the groups of parameters such as the female/male ratio, delivery method, ABO or Rh incompatability and presence or absence of exchange transfusion.
Other parameters with normal distribution were compared using the one-way variance analysis. When there was a significant difference between the groups, the one-way ANOVA post-hoc Tamhanes' T2 test was used to find difference between the groups. Results were confirmed using Student’s t test (independent samples t test) for each group separately. The values before and after treatment were compared using Student’s t test (paired samples t test). Results were given as mean ± standard deviation. Level of significance was set as p < 0.05 except one-way ANOVA post-hoc Tamhones'T2 test for which it was accepted as p < 0.015.
Non-parametric variance analysis methods: Kruskal-Vallis one-way variance analysis and Mann-Whitney U test were used for variables without a normal distribution. Wilcoxon signed-rank test was used for the analysis of dependent parameters. Pearson correlation analysis and regression analysis were used to assess the relationship between the parameters. Correlation between variables without a normal distribution was analyzed using the Kendall's tau-b or the Spearman correlation analysis.
An informed consent was received from the parents. The study was approved by the Local Ethics Committee of Yuzuncu Yil University, Faculty of Medicine and the study was conducted in accordance with the Helsinki Declaration.
Results
The study group consisted of two subgroups: neonates with hyperbilirubinemia exceeding the phototherapy limit (Group 1, n = 36) and neonates with kernicterus (Group 2, n = 33). The control group consisted of 25 cases. Of the 36 cases in Group 1, 23 (63.9%) were males and 13 (36.1%) were females. In Group 2, 19 (57.6%) patients were males and 14 (42.2%) were females. In control group, 14 (56%) infants were males and 11 (44%) were females. The mean age was 4.5 ± 1.8 days (range 2–7 days) in Group 1, 5.61 ± 2.33 days (range 2–10 days) in Group 2 and 4.64 ± 1.934 days (range 2–10 days) in controls. While, in Group 1 the mean weight was 3119 ± 480 g (range 2470–4000), in Group 2 and control group this value was found to be 2965 ± 499 g (range 2300–3950 g), 3190 ± 521 g (range 2500–4300 g), respectively. The mean duration of jaundice was 2.8 ± 2.0 days (range 1–10 days) in Group 1 and 3.4 ± 2.6 days (range 1–10 days) in Group 2. There was no significant difference in Group 1, Group 2 and control groups for gender, age, weight and in Groups 1 and 2 for duration of jaundice (p > 0.05).
ABO and Rh incompatibilities were found in three (8.3%) infants and three (8.3%) patients in Group 1, eight (24.2%) and 7 (21.2%) patients in Group 2, respectively. While no patient had concurrent ABO and Rh incompatibility in Group 1, five patients (15.1%) in Group 2 had concurrent ABO and Rh incompatibility. All patients in Groups 1 and 2 underwent phototherapy. Additionally, exchange transfusion was performed in only 2 (5.6%) patients in Group 1 and in 16 patients (48.4%) in Group 2. While all patients in Group 1 were discharged with recovery, three patients (9.1%) died in Group 2. ABO and Rh incompatibilities were found to be significantly more common in the group with kernicterus compared to the other groups (p < 0.001). The rate of exchange transfusion was more common in the group with kernicterus and this was significant (p < 0.001).
Antioxidant and oxidant system levels are presented in Table 1. Plasma TAC and serum TOS were significantly higher in Groups 1 and 2 than the control group. The p value for the difference between Groups 1 and 2 for TAC levels was 0.07. While, there was no significant difference between Groups 1 and 2 and between Group 2 and control group for MDA values, there was a significant difference between Group 1 and control cases (p < 0.001). TTHI values were significantly elevated in Group 1 compared to Group 2 and control cases. No difference was found between Group 2 and control cases. Ceruloplasmin, OSI, nitrite and NO levels were not significantly different among the three groups. Plasma nitrate level was highest in Group 1 and lowest in the Group 2. While there was a significant difference between Group 1 and Group 2, no significant difference was found between Group 2 and control group.
Comparison of all groups according to serum bilirubin, oxidant and antioxidant levels on admission
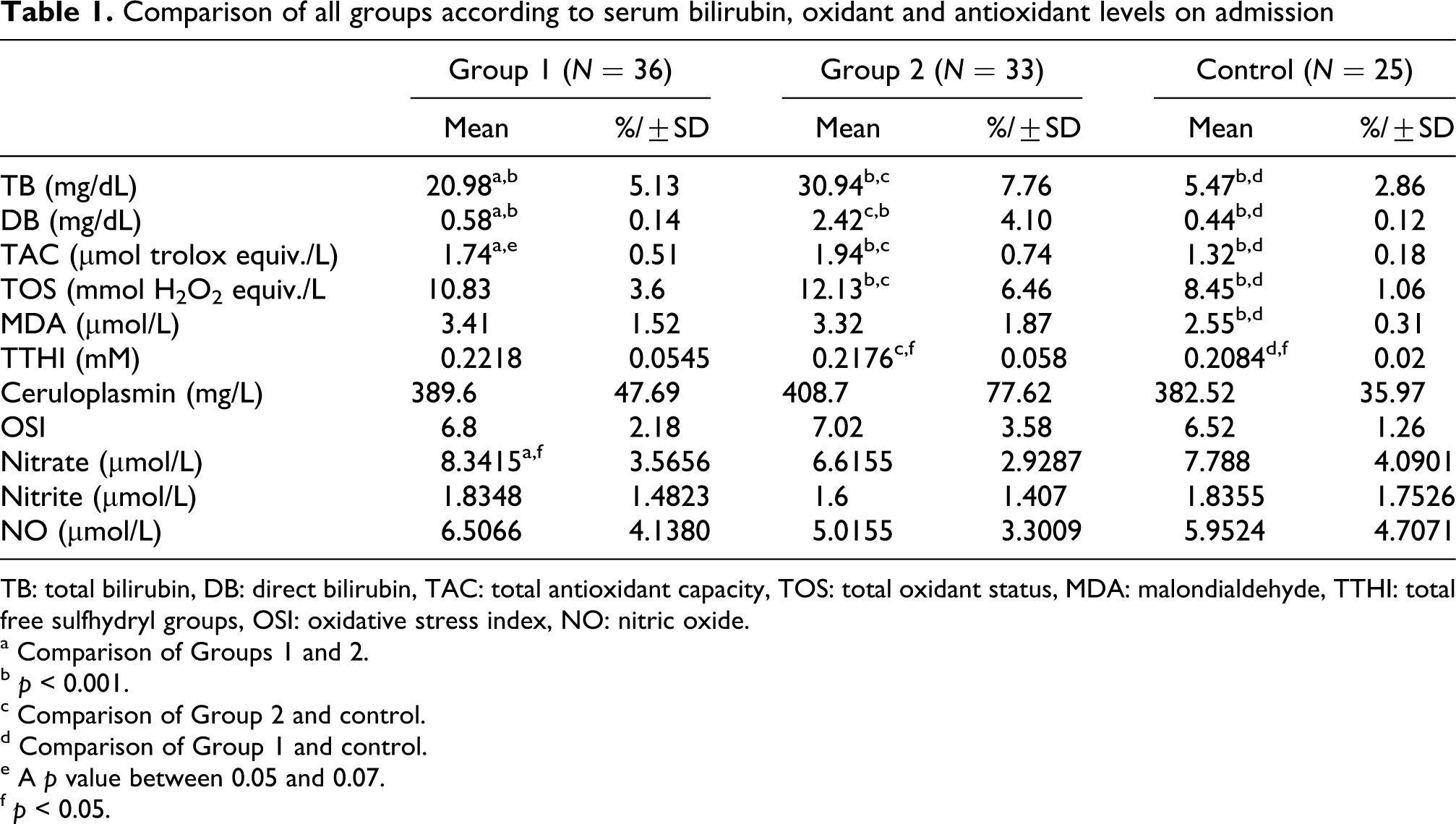
TB: total bilirubin, DB: direct bilirubin, TAC: total antioxidant capacity, TOS: total oxidant status, MDA: malondialdehyde, TTHI: total free sulfhydryl groups, OSI: oxidative stress index, NO: nitric oxide.
a Comparison of Groups 1 and 2.
b p < 0.001.
c Comparison of Group 2 and control.
d Comparison of Group 1 and control.
e A p value between 0.05 and 0.07.
f p < 0.05.
In order to assess the effect of bilirubin on the antioxidant system, cases with blood group incompatibilities were excluded from the three groups (kernicterus, control and hyperbilirubinemia) and a new group was formed. Correlation and regression analyses were performed and the antioxidant effect of bilirubin was assessed. With this choice, the confounding effect of any oxidative damage that may have occurred after the hemolytic process on the results was avoided. There were 53 cases after exclusion of those with blood group incompatibility. Correlation analysis for TB, DB (direct bilirubin), IB (indirect bilirubin), TAC, TOS, OSI, MDA, TTHI, ceruloplasmin, nitrate, nitrite and NO values was performed in this new group.
The increase in bilirubin and the increase in TAC were parallel. However, the increase in TOS, MDA and OSI were not parallel because the mean MDA values in the group with kernicterus which had the highest TB levels were lower than those of Group 1. Therefore, the relationship between TB and antioxidant and oxidant system parameters may not be linear. The cases in this new group were divided into two new groups: cases with TB of ≤20 mg/dL and cases with TB of >20 mg/dL. The medical history, physical examination and laboratory values of the newly formed groups have been presented in Table 2. When these two groups were compared for the antioxidant panels; there was a significant difference for TAC and OSI. TAC was higher in the group with serum TB of >20 mg/dL and OSI was higher in the group with serum TB of ≤20 mg/dL (Table 2).
The comparison of cases with TB of >20 mg/dL and cases with TB of ≤20 mg/dL according to hematologic, biochemical, oxidant and antioxidant system parameters
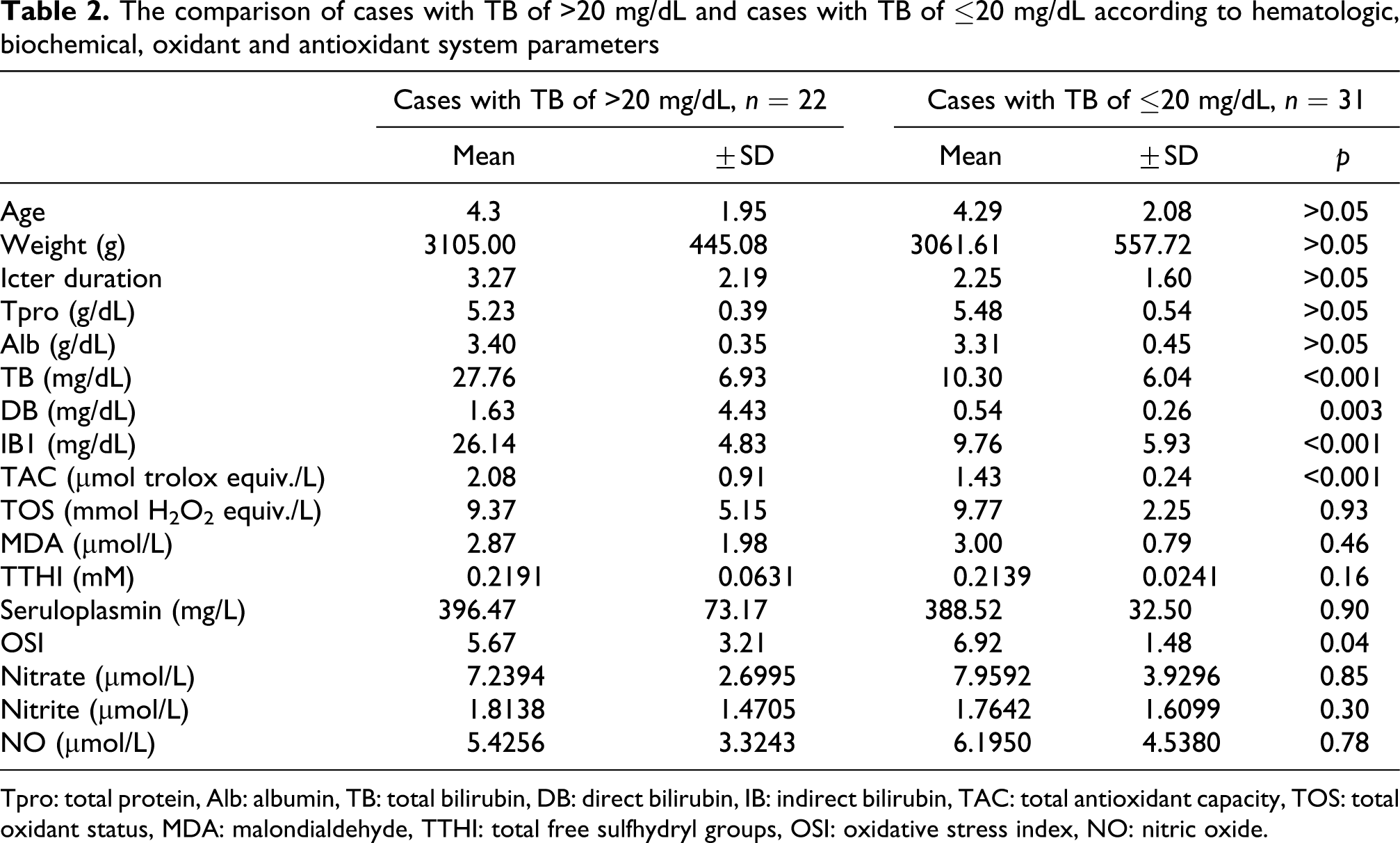
Tpro: total protein, Alb: albumin, TB: total bilirubin, DB: direct bilirubin, IB: indirect bilirubin, TAC: total antioxidant capacity, TOS: total oxidant status, MDA: malondialdehyde, TTHI: total free sulfhydryl groups, OSI: oxidative stress index, NO: nitric oxide.
Correlation analysis showed that TB >20 mg/dL was negatively correlated with TOS, MDA and OSI and that TB ≤20 mg/dL was positively correlated with TAC, TOS, MDA and OSI (Table 3). Thus, the increase in serum TB values and the increase in TAC, TOS and MDA were not linear. It was found that the correlation between TB and TAC, TOS, MDA and OSI may be expressed by a quadratic curve (Figure 1).
Correlation analysis of TB, DB, IB, oxidant and antioxidant system parameters in cases with TB of >20 mg/dL and in cases with TB of ≤20 mg/dL
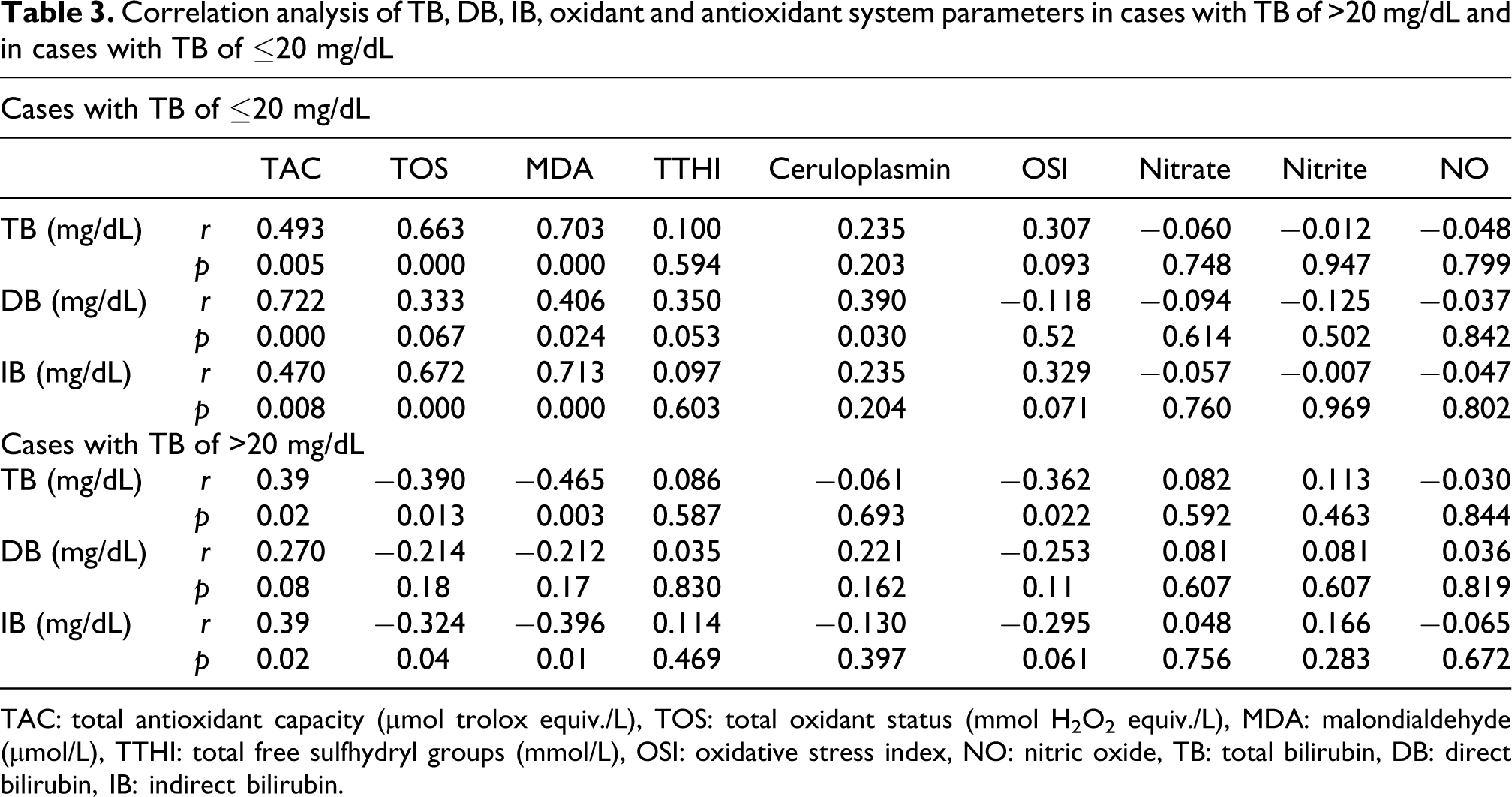
TAC: total antioxidant capacity (μmol trolox equiv./L), TOS: total oxidant status (mmol H2O2 equiv./L), MDA: malondialdehyde (μmol/L), TTHI: total free sulfhydryl groups (mmol/L), OSI: oxidative stress index, NO: nitric oxide, TB: total bilirubin, DB: direct bilirubin, IB: indirect bilirubin.

The correlation between total bilirubin and total antioxidant capacity (TAC; p < 0.001), total oxidant status (TOS; p = 0.002), malondialdehyde (MDA; p = 0.004) and oxidative stress index (OSI; p = 0.008).
The infants who underwent exchange transfusion were excluded from those who underwent phototherapy in this new group. The effect of phototherapy on the antioxidant system was studied by comparing the pre- and post-treatment data. Pre-treatment and post-treatment laboratory values have been presented in Table 4. It was found that post-treatment TAC and nitrite levels increased compared to pre-treatment levels; however, the difference of TAC levels was not significant. It was thought that the increase in nitrite which is a form of oxide NO may be related to the oxidant stress effect of phototherapy (Table 4).
The effect phototherapy on biochemical, antioxidant and oxidant system parameters
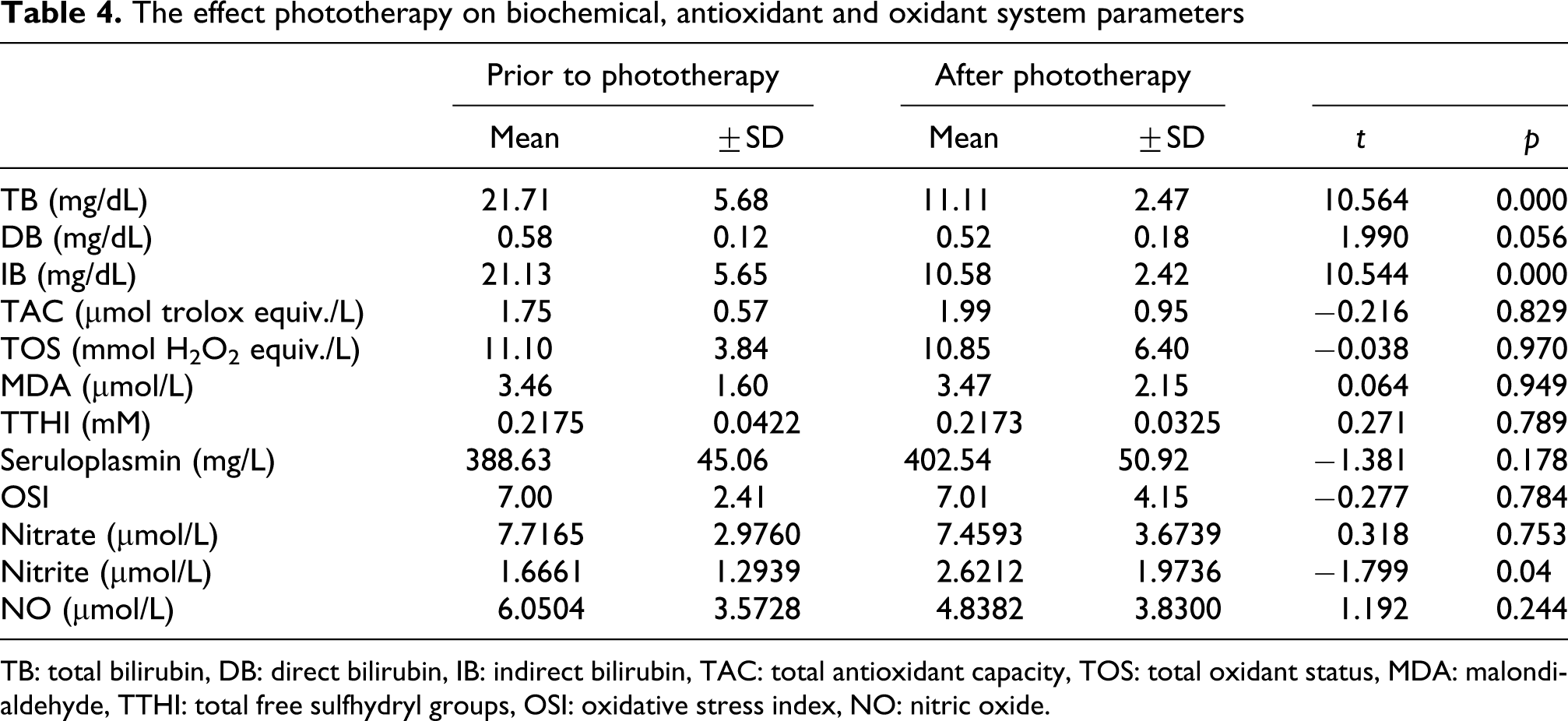
TB: total bilirubin, DB: direct bilirubin, IB: indirect bilirubin, TAC: total antioxidant capacity, TOS: total oxidant status, MDA: malondialdehyde, TTHI: total free sulfhydryl groups, OSI: oxidative stress index, NO: nitric oxide.
Discussion
Free radical reactions are important reactions, having a role in the appearance of aerobic life forms and having efficient functions in the evolution process. Besides the contributions of these reactions to life, their feature of being harmful to living organisms has been the focus of interest for the scientists. In contrast with the intrauterine life, the relationship between antioxidants and oxidative damage has been studied for life after birth, which has higher oxygen concentrations. In conclusion, in the newborns,in conditions such as premature retinopathy, lung damage due to hyperoxic ventilation (bronchopulmonary dysplasia), intracranial hemorrhage, periventricular leucomalacia, sepsis, necrotizing enterocolitis, hypoxic ischemic encephalopathy, the increase in free radical and reactive oxygen species have been thought to be responsible in the pathogenesis.14–16
It was first suggested in 1937 that bilirubin has a preventive effect for infections. The antioxidant feature of bilirubin was then demonstrated in numerous studies.17–20 Wiedemann et al. 21 found that plasma was better protected against oxidative stress in newborns than in adults, owing to its higher content of antioxidants like bilirubin and its lower content of oxidizable lipids. Additionally, in another study, low molecular weight antioxidants' concentrations (urate, bilirubin, albumin and sulfhydryl groups) and lipid peroxidation levels were examined in pair-matched maternal and cord blood plasma. The authors were determined that urate, bilirubin and sulphydryls were in significantly higher concentrations in cord blood than in maternal blood and finally they suggest that the increased levels of these antioxidants in cord blood may contribute to the increased resistance of cord plasma to Cu+2-induced lipid peroxidation. 22 This difference supports the hypothesis that newborn tends to increase the antioxidant capacity to balance oxidative stress after birth. In contrast with these findings, Sullivan and Newton 23 measured antioxidant activity in cord sera and found that antioxidant activities of the newborn were lower than those of adults. In another study that was conducted by Mireles et al., 2 which was performed to examine the range in which bilirubin exerts its beneficial effect, the authors used erythrocytes derived from cord blood and incubated them with 0–60 mg/dL bilirubin combined with 3 g/dL bovine seum albumin (BSA; bilirubin/BSA) to mimic physiologic and pathologic conditions. In that study, oxidative stress was induced by incubating the erythrocytes with a solution of 0.6 mM H2O2 and 0.15 M CuSO4 to generate hydroxyl radical mediated injury. Finally, the authors concluded that bilirubin, at physiologic concentrations, protects neonatal red blood cells against oxidative stress in the presence of physiologic concentrations of BSA but that bilirubin concentrations of 30 mg/dL or higher and a bilirubin:BSA ratio of greater than one are associated with significant cytotoxicity. 2 In further studies, it was shown that membrane cholesterol and phospholipids were liberated under conditions where molar bilirubin/albumin ratio was >1 and where free bilirubin increased and they suggested that in newborns with severe hyperbilirubinemia, bilirubin may cause erythrocyte damage. 24 Therefore, it was suggested that cases in which the cytotoxic effects due to bilirubin are seen, as in kernicterus, may be related to higher oxidant stress. Hence, we compared plasma TAC, serum TOS, OSI, MDA, nitrate, nitrite, NO, ceruloplasmin and TTHI in infants with kernicterus with those in cases with hyperbilirubinemia exceeding phototherapy limits and controls to assess the oxidant stress and antioxidant capacity. In conclusion, it was found that the group with kernicterus had significantly higher antioxidant capacity. This situation was thought to be related to the contribution of increased bilirubin to the antioxidant capacity. However, it was found that while there was a significant increase in TOS compared to the control group, there was no significant difference when compared to Group 1. Mean MDA levels were lower than those of Group 1, whereas they were significantly different from those of the control group. The smiliar relationship was also seen in TTHI. It was suggested that increased TAC in the group with kernicterus may be related to antioxidant feature of bilirubin. Both onset of the direct toxic effect of bilirubin and the hemolytic process may be responsible for increased oxidative stress. Therefore, contribution of bilirubin to antioxidant capacity and the relationship with oxidant stress were studied after formation of a new group excluding the infants with blood group incompatibility, i.e. hemolytic process.
Kilic et al. 25 studied the relationship between serum bilirubin levels and plasma nitric oxide and activity of enzymes in erythrocyte such as superoxide dismutase (SOD), glutathione peroxidase (GSH-Px) and catalase (CAT) in premature infants. Their study included 20 premature infants with jaundice and 15 premature infants without jaundice as a control group. Plasma nitric oxide and serum bilirubin levels were found to be significantly higher in the study group than those in the control group. In addition, erythrocyte SOD, GSH-Px and CAT enzyme activities were found to be significantly lower in the study group than those in the control group. Finally, they concluded that in the etiology of hyperbilirubinemia, neonatal erythrocytes and nitric oxide reactions are affected differently and that erythrocyte hemolysis caused as a result of these effects may play a role in the etiopathogenesis of unconjugated hyperbilirubinemia. Hemolysis might also be seen because of the inadequacy of the protection by erythrocytes against the cytotoxic effects of free radicals resulting from the lack of antioxidant enzymes in these cells. In another study, Dani et al. 26 assessed the hypothesis that changes in plasma TB levels could influence the antioxidant system and oxidative stress in preterm infants. In that study, 22 healthy preterm infants who presented with visible non-hemolytic hyperbilirubinemia were studied. They found that TB did not correlate with plasma total hydroperoxide concentration (TH), TAC or TTHI concentration, but a significant correlation was found between TH and TAC, TH and TTHI, and TAC and TTHI concentrations, both at study entry and after 24 hours. They suggested that the decrease in plasma bilirubin was contemporary with an increase in plasma antioxidant capacity and decrease in oxidative stress in preterm infants. Bélanger et al. 27 found a positive correlation between bilirubin concentration and TAC and the increase in TAC level was found to be related to bilirubin level. Kumar et al. 28 investigated the role of bilirubin as an antioxidant in neonatal hyperbilirubinemia by measuring MDA levels, a marker of oxidative stress and key antioxidant enzymes, superoxide dismutase (SOD), catalase and glutathione peroxidase (GPx) in otherwise healthy 70 term newborns with neonatal hyperbilirubinemia and 20 control newborns without jaundice. They found that jaundiced newborns had significantly lower MDA but higher SOD, catalase and GPx levels. Furthermore, plasma bilirubin showed significant negative correlation with MDA but positive correlation with antioxidant enzyme activities. It was concluded that neonatal hyperbilirubinemia is associated with lower oxidative stress. Yiğit et al. 29 compared 58 cases with manifest hyperbilirubinemia (>12.8 mg/dL) and 24 control cases without jaundice for MDA values was an index of free radical-induced lipid peroxidation. They showed that serum MDA concentrations were higher in infants with hyperbilirubinemia than in controls and a positive correlation was found between MDA and bilirubin concentrations in cases with manifest hyperbilirubinemia. When the study group was categorized according to the presence of hemolysis, a significant correlation was found between MDA and bilirubin concentrations in those infants with hyperbilirubinemia due to haemolysis. There was no such correlation in those without hemolysis. In another study, plasma MDA levels and serum bilirubin concentrations, in blood samples taken from healthy, term neonates with non-hemolytic hyperbilirubinemia were compared with those taken from healthy neonates without hyperbilirubinemia. Plasma MDA concentrations in neonates with jaundice were found to be significantly higher than those of the healthy infants. However, no significant correlation was found between plasma MDA and serum bilirubin concentrations. 30 Oğuz et al. 31 reported that TB values of ≤10 mg/dL were beneficial in the newborns and contributed to TAC, and that higher TB levels (>15 mg/dL) caused an increase in the lipid peroxidation even if it did not cause a risk for the central nervous system.
In our study, the mean TB value was 30.94 ± 7.76 mg/dL in Group 2 and 20.98 ± 5.13 mg/dL in Group 1. The mean TB value was measured as 5.47 ± 2.86 mg/dL in the control group. Although total oxidant level and oxidative stress index were significantly higher in Group 2 than those of the control group, no significant difference was found between the Groups 1 and 2. However, it was found that TAC was significantly higher in Group 2 compared to the other two groups. In our study, increase in bilirubin was parallel with increase in TAC when all cases were taken into account. However, increase in TOS, MDA and OSI was not linear because mean MDA value in Group 2 which had the highest TB were lower than those of Group 1. In order to assess the effect of bilirubin on the antioxidant system, a new group was formed after excluding those with blood group incompatibility in the three groups (Group I, II and controls). With this choice, the confounding effect of oxidative damage—which may appear after the hemolytic process—on the results was avoided. In the end of the correlation analyses, a TB of >20 mg/dL was significantly negatively correlated to TOS, MDA and OSI, and it was significantly positively correlated to TAC (p = 0.05, p = 0.013, p = 0.003 and p = 0.022, respectively). In the group with TB ≤20 mg/dL, it was significantly positively correlated to TAC, TOS, MDA and OSI (p < 0.001, p < 0.001, p = 0.09, p = 0.005, respectively). Therefore, the increase in the serum TB values and the increase in TOS, MDA and OSI were not linear. It was found that the correlation between serum TB and TAC, TOS, MDA and OSI may be expressed by a quadratic curve.
Satar 32 reported that antioxidant enzyme levels decreased as the level of bilirubin increased in full-term newborns with hyperbilirubinemia. After bilirubin values decreased by the effect of phototherapy, an increase was found in these enzyme levels. In contrast, Gathwala and Sharma 33 showed that blue light phototherapy increased the oxidative stress in preterm infants. Additionally, Dahiya et al. 34 showed that MDA levels significantly increased after phototherapy compared to pre-phototherapy levels, whereas GSH, TTHI and vitamin C significantly decreased after phototherapy. In conclusion, they suggested that phototherapy increased oxidative stress and should be used with care. In our study in which the effects of phototherapy on oxidant and antioxidant parameters were assessed, only nitrite was found to be affected and it showed an increase compared to pre-treatment values. This can be interpreted as phototherapy increasing the oxidative stress which was consistent with the literature. However, we could not find any significant change in MDA and TTHI levels. Similarly, Akisü et al.35,36 did not find any significant change in the levels of MDA and antioxidant parameters after phototherapy in their study.
Conclusion
We demonstrated that the relationship between serum TB and the antioxidant panel and oxidative stress parameters was not a linear line and that it can be expressed by a quadratic correlation curve. Although, there have been several studies on the contribution of bilirubin to antioxidant capacity, there are still many unexplained issues. Besides, different results from various studies suggest that we are still at the beginning of the way. We found that the antioxidant effect of bilirubin increases in parallel to the concentration, without a limit. Although the contribution to the antioxidant capacity increases in correlation with the serum level, it was found that after a certain point, kernicterus occurs with the direct toxic effect on the cell. Thus, further studies are required to understand the point at which the toxic effect of bilirubin—which is increased excessively to support the antioxidant capacity—begins in the neonatal period and to clarify the timing of the exchange transfusion. In infants with a rapid bilirubin increase, the antioxidant capacity may be supported with other substances which have antioxidant features and that are as beneficial as bilirubin, but with no toxic effects.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not for-profit sectors.