
Abstract
This article contributes to the theoretical understanding of institutions as fundamental in shaping the demand for migrant labour by investigating labour market regulation as possible explanation for cross-country differences in labour market segmentation and the presence of migrant workers. It compares the adult social care sector in England and the Netherlands with important cross-country differences in the reliance on migrant labour amid similar cost saving policies and marketization drives. The analysis draws on data collected between 2009 and 2019 and consisting of sectoral survey data, policy documents, interviews with relevant actors, and the observations of trade union and care workers’ meetings. The findings highlight the importance of path-dependent features of the national industrial relations systems in explaining observed differences but also how the specific nature of the regulatory outcomes depends on unions’ strategies and power.
Introduction
Recent literature has underlined the centrality of employers’ preferences for migrant workers in explaining the concomitant increase of low-paid labour migration and the deterioration of terms and conditions of employment through ‘flexibilization’ and ‘segmentation’ (e.g. Raess and Burgoon, 2015; Ruhs and Anderson, 2010). While empirical analyses confirm this correlation within and across countries in Europe (e.g. Alsos and Eldring, 2008; McCollum and Findlay, 2015; Raess and Burgoon, 2015), they have not clearly identified ‘how immigration’s effects for flexibility might be mediated by institutional conditions at the level of the enterprise, industry or country’ (Raess and Burgoon, 2015: 107). This gap in the literature has contributed to an implicit and distorting notion of ‘social dumping’, informing policy debate and academic analyses, which considers the deterioration of host countries labour standards as a direct effect of increasing low-paid migration.
This article contributes to this debate by arguing that labour market regulation poses a fundamental constraint on employers’ preferences and, therefore, influences the relationship between the concomitant increase of labour migration and flexibilization. Regulation is here defined as a ‘multiplicity of sites, spaces and actors – both formal and informal’ whose relationships determine its pattern and efficacy (MacKenzie and Martínez Lucio, 2005: 500). This extends beyond statutory legislation to include the social regulation by industrial relation actors and practices, which are fundamental components of regulatory systems and support higher levels of monitoring and enforcement of labour laws and agreements (Jaehrling and Méhaut, 2013).
This argument is developed by comparing the adult social care sector across two countries with different regulatory frameworks, England and the Netherlands. 1 Under the concomitant pressures of increasing demand for services and costs reduction policies, the sector has seen a widespread marketization and a greater reliance on migrant workers across countries which have inspired a debate about a ‘convergence’ across Europe (Simonazzi, 2009; Williams, 2012). However, important differences exist in the nature and extent of migrant employment as illustrated by a greater reliance on migrants in England than the Netherlands. The article analyses these differences by drawing on qualitative data collected between 2009 and 2019 and focussing on residential care which is less investigated than care in private households (Da Roit and Weicht, 2013). The data consists of public survey data, policy documents, interviews with key actors, and observations of meetings involving care workers and representatives of the biggest unions in the care sector, namely, UNISON and GMB in England and FNV Zorg en Welzijn (from here on FNV) in the Netherlands.
The findings are in line with the discussion of ‘virtuous’ and ‘vicious’ circles of institutional interactions in determining the extent of precarious work (Doellgast et al., 2018). They highlight the impact of social regulation and unions’ role and position in shaping the demand for migrant labour and the conditions of (migrant) workers. In the Netherlands, these factors not only support the recruitment and retention of local workers but also directly constrain employers’ use of flexible contractual arrangements. In England, unions struggle to perform a similar role and sectoral conditions are largely shaped by statutory regulation. This has provided employers with greater leeway to lower employment conditions with a subsequent increasing demand for migrant labour. These findings contribute to the literature on the impact of labour market institutions on the demand for migrant labour (e.g. Devitt, 2010; Menz, 2009; Wright, 2012). They also expand our understanding of the increasing relevance of migrant labour in the social care sector, which has been predominantly explained by the intersections of care, migration and employment regimes (e.g. Van Hooren, 2012; Simonazzi, 2009). While recognising the importance of these aspects, as well as factors such as language and colonial heritage, this article points to labour market regulation as an important yet largely overlooked factor within existing analyses. From a policy point of view, this paper challenges the view of social regulation and trade unions as forces of exclusion of migrant or precarious workers (Lindbeck and Snower, 2001) by sustaining the view that effective inclusion cannot stem from exploitative conditions but requires fair treatment and social justice for migrant and local workers alike.
The next two sections examine the relevant literature. A further section provides background information on the sector and the selected countries. This informs a comparative account on the migrant presence in the sector and the specific conditions of employment before the paper ends with discussion and conclusions.
Labour migration, segmentation and the regulation of the labour market
Employers’ preferences for migrant labour, as an attempt to minimise labour costs, have been considered central in a causal circular relationship between (intra-European) labour migration and labour market segmentation (e.g. Ciupijus, 2011; McCollum and Findlay, 2015; Ruhs, 2006). These analyses provide the scope for reflections on labour market regulation as constraint on or opportunity for employers’ behaviours and therefore on the extent of low-paid labour migration. Several contributions have highlighted how the interplay of regulatory processes and institutions (Peck, 1996) or ‘systems effects’, also including factors such as job status and the gendered nature of work (Ruhs and Anderson, 2010), shape employers’ choices towards local or migrant labour. Other scholars have underlined the relevance of employment and recruitment regimes, and especially the ways in which state and non-state institutions influence skill formation (e.g. Devitt, 2010). Some authors (Menz, 2009; Wright 2012) have linked varieties of capitalism to employers’ preferences which explain the variation of migration policies across countries, thus creating different ‘patterns of interaction between market institutions and labour supply and demand’ (Wright, 2012: 131). However, while referring to or hinting at its relevance, these analyses do not systematically address the ways through which labour market regulation, actors and processes influence the demand for migrant labour.
To advance such an analysis, we draw on literature about the role of regulation in reducing labour market segmentation and counteracting the rise in precarious jobs (e.g. Benassi and Dorigatti, 2015; Doellgast et al., 2009; Rubery et al., 2018). Doellgast et al. (2018) have argued that precarious work could be contained through the ‘virtuous’ interaction of inclusive institutions, union strategies, workers solidarity and voice-oriented employers’ practices. The interdependence between employment law, national industrial relations systems and union power at the sectoral level is considered necessary to maintain collective protection (Doellgast et al., 2009). Unions’ power, in turn, partly reflects their level of institutional embeddedness (e.g. Arnholtz and Refslund, 2019; Marino, 2012) but also results from a variegated sets of resources and ‘strategies’ used to leverage them (Doellgast et al., 2009; Frege and Kelly, 2004). Particular attention has been paid to the organising of new groups including migrant workers (Arnholtz and Refslund, 2019), with reflections on the synergies between different power resources in contexts of embedded industrial relations (Martínez Lucio et al., 2017).
This article draws on these analyses to investigate how (social) regulation and union power operate to provide inclusive security within an otherwise non equilibrating labour market where there is the constant potential of a (migrant) reserve army (Rubery, 1987). By constituting a major constraint on employment practices, these factors can be considered as fundamental determinants of the overall demand for labour migrants and their conditions in the labour market.
Adult social care and migrant labour
Strong similarities exist in adult social care employment across Europe. It mostly concerns women, generally older than the workforce average, and is characterised by low standards in terms of pay, hours, training and status, in particular in the private segment of the sector and in home care (Simonazzi, 2009). The poor standards are based on implicit assumptions that these jobs replicate domestic unpaid work and require no or limited formal qualifications (Hebson et al., 2015). While research has shown high levels of job satisfaction (Atkinson and Lucas, 2013), studies also highlight how the acceptance of poor working conditions can be explained by gendered social norms reinforcing the image of women as natural carers or lack of better opportunities due to the combination of economic, family, educational and labour market circumstances (Hebson et al., 2015).
Labour shortages and recruitment problems became significant in the early 2000s as result of women opting for less stressful jobs, higher investments in education, and the implementation of work-life balance and active labour market policies (Williams, 2012). While the recruitment problems highlighted the need to upgrade practices and employment conditions to appeal to a wider workforce (Rubery and Urwin, 2011), they were accentuated by attempts to reduce costs through the commodification and marketisation of care provision (Simonazzi, 2009; Williams, 2012). Outsourcing of services to the private sector by local authorities, which has been pronounced in England, exacerbated the extent of low pay and facilitated the evasion of unsocial hours premia and sick pay (Rubery and Urwin, 2011), further lowering the public perception of the low status of these jobs.
In this context, the recruitment of migrant labour has become increasingly significant and has inspired an idea of convergence as ‘European welfare states reduce their increasing social expenditure costs through strategies that involve, directly or indirectly, migrant health and care labour’ (Williams 2012: 373). Increasing intra-EU mobility, following the different phases of EU enlargement, has been important in this process since it has provided a wide supply of ‘cheap’ labour (Simonazzi, 2009). Cross-country differences in the extent of migrant labour, however, are still significant and have been investigated considering the intersection between care and migration regimes (e.g. Van Hooren, 2012). Some analyses have also considered the role of employment systems and the relevance of working conditions as resulting from the segmented nature of the labour market (Da Roit and Weicht, 2013; Williams, 2012). Simonazzi (2009) has argued how national employment models, combined with the nature of the care markets (formal/informal, regulated/unregulated), shape the characteristics of elderly care regimes including the use of migrant workers to cope with labour shortages. For example, the differences in employment regimes explain why the UK has increasingly shifted to migrant labour while Sweden has been ‘determined to prevent the onset of a low-skilled, low-paid market for irregular eldercare workers’ and has aimed at improving employment and working conditions to recruit and sustain a stable long-term care workforce (Simonazzi, 2009: 227). A more recent analysis of Sweden reports an increasing presence of migrant care labour concentrated in large cities, but also underlines how this has not come at the expenses of working conditions in the sector (Jönson and Giertz, 2013). These analyses acknowledge the link between employment regulation and migration but remain mostly limited to general references to path-dependent institutional features with scarce consideration of the role of the actors within the regulatory context and their relative power.
Research context and design
England and the Netherlands differ in terms of their social care regimes. England is closer to a liberal care regime where social care is provided by the private market with public provision highly means- and needs-tested. The Netherlands resembles a Social Democratic care regime with universal access to social care for all those in need (Van Hooren, 2012), albeit care provision has become increasingly means-tested over the years. 2 However, important similarities also exist in the provision of adult social care. First, the responsibility and provision of care services are largely split. In England, local authorities are responsible for the provision but, since the 1990s, outsourcing has resulted in an increasing move of employment to the private sector (Rubery and Urwin, 2011), with private for-profit providers accounting for 78 per cent of jobs in 2018 (Skills for Care, 2019). In the Netherlands, local authorities are responsible for domiciliary care and mandatory collective insurance makes health insurers responsible for nursing and care homes (Alders and Schut, 2019). However, the actual care services are mostly provided by private non-profit organisations. Second, a policy of budget reductions in the context of rising service demand has created concerns about the quality of care as well as employment and working conditions in both countries. In England, the years of austerity resulted in £7.7 billion of savings despite the rising demand for care with 1.4 million older people not receiving the care and support they needed in 2018 (ADASS, 2019). In the Netherlands, public investments in the sector have been traditionally high and have sustained working conditions and service quality (Alders and Schut, 2019). However, interventions to reduce costs have been introduced since 2012, including a 32 percent reduction to the budgets for domestic help (Alders and Schut, 2019). Some of these cuts pre-empted the 2015 Law on Long-Term Care which promoted care of elderly people in their private home. This caused a strong decline in employment in both domestic and residential care between 2012 and 2017 (UWV, 2015). However, as analysed later, public initiatives promoted a policy shift resulting in a rise of public investment of €2.1 billion per year between 2017 and 2021.
The two countries differ in the regulation of employment with ‘liberal pluralism’ in England and ‘social partnership’ in the Netherlands (Visser, 2009). In the Netherlands, unions have long enjoyed strong institutional support and remain fundamental actors in the national regulatory framework. Despite a decline in union density from around 40 percent in the 1960s to 15.4 per cent in 2019, collective bargaining coverage has long been stable around 80 per cent. In England, the decline in union density has started later and density continues to be slightly higher at 22.2 per cent in 2019. 3 However, the lack of institutional underpinning to social regulation has accentuated the effect of membership decline in weakening unions’ role and position. These differences also shape the relationship between statutory legislation and social regulation. In the Netherlands, this relationship can be defined as ‘embedded’ since social partners are influential in national level policy making and standards are set and enforced by collective agreements which achieve full coverage through the extension mechanisms. In England, statutory legislation has become more and more a unilateral regulatory tool and is nowadays considered as a counterweight for the absence of collective agreements at the sectoral level (Grimshaw et al., 2016). The situation in the adult social care sector reflects these general patterns. Actual unionisation rates in residential care are slightly higher in the UK (19.2% in 2019) than in the Netherlands (estimated by interviewees to be about 15%). 4 However, collective bargaining plays a very limited role in England while there is full coverage in the Netherlands.
This paper draws on a range of data referring to the period between 2009 and 2019. This includes 19 interviews with workers and representatives of UNISON and GMB in England and the FNV in the Netherlands. In England, interviews involved 12 individuals: five workers and seven union officers. Three workers were female migrants (of Polish, Greek and Filipino nationalities) and the other two were British men (1 of ethnic minority background). Union representatives included four female officers (2 Filipinos, 1 Polish, 1 British of ethnic minority background) and three male officers (2 of ethnic minority background). In the Netherlands, interviews involved seven Dutch nationals: two female workers (1 of ethnic minority background), and five union officers (3 males and 2 females, 1 man and 1 woman of ethnic minority background). Most interviews in England took place between 2013 and 2015 while interviews in the Netherlands were held in 2017. We also participated in two meetings involving care workers and union representatives, followed by short exchanges with participants. In England, this concerned a meeting in 2015 organised in a residential care home in south London by UNISON. Participants to this meeting mostly included female migrant workers. In the Netherlands, it concerned a union meeting organised in Utrecht in 2017 with a large group of mostly female workers, including a small number of ethnic minority workers. The notes collected during these events provided important information on workers’ grievances and experiences as well as union position and responses during particularly turbulent years characterised by the austerity policies in England and major budget reductions in the Netherlands. We complemented this data with available statistics on migration, sectoral survey data and policy documents by relevant organisations such as Skills for Care in England and the UWV in the Netherlands, and collective agreements. The subsequent two sections draw on this data to consider the differences in migrant labour and the regulation of employment in the sector across the two countries.
Migrant care labour in England and the Netherlands
While the gender composition of the social care workforce is similar across the two countries, the migrant presence differs with twice as many migrant workers (defined here as foreign-born) in England than the Netherlands (Skills for Care, 2019; UVW, 2020).
‘Hard to fill’ vacancies (Cangiano et al., 2009: 26) have pushed previous UK governments to recruit workers from overseas, as in the case of 20,000 senior care workers recruited from the Philippines following increased investments in the NHS by the Labour government in the 2000s. In this decade, the share of migrant workers more than doubled to around 18 per cent of total workforce in the UK as a whole and more than half in London (Cangiano et al., 2009). Although it has not increased further in recent years, the composition has changed due to the increase of Eastern European migrants after the EU enlargements in 2004 and 2007. The share of EU and non-EU migrants has, respectively, increased and declined by about 3 per cent of the workforce since 2012/13. In 2018, around 17 per cent of the workforce was not British, almost equally divided between EU (8%) and non-EU nationals (9%). This was higher than their overall share in the population (14%). 5 Since 2014, Romanians have become the largest group of foreign workers in adult social care, representing 13 per cent of all foreign workers in 2018, followed by Polish workers (11%) and migrants from various non-European countries (Skills for Care, 2019). This changing composition reflects the preferences of providers and employers for EU migrants due to, for instance, the simplification of bureaucratic procedures, economic savings, and the fact that these workers are ‘white’ and therefore less likely to encounter hostility from patients (ENG7_Unison National Officer, 2014). This also helps explaining the introduction of stricter requirements for non-EU workers, which pushed many providers to ‘make them redundant and send them home because we can’t afford to follow the requirements of the Home Office’ (ENG7_Unison National Officer, 2014).
The interviewees (e.g. ENG7_Unison National Officer, 2014; ENG4_Workplace union representative, 2015) often highlighted how migrant workers had higher levels of education and experience than required for the job. High wages than in the country of origin were an important motivator and the idea of the job as a ‘temporary step’ emerged during the interviews, suggesting that the level of commitment to the job itself (but not to the well-being of the patients) was lower than the literature attributes to local workers (Atkinson and Lucas, 2013). Younger workers, especially those who had less family commitments, considered it as a transition to better opportunities (ENG3_Team supervisor, 2015; ENG4_Workplace union representative, 2015). However, more economically vulnerable individuals showed a higher dependency on the job and reported how its precarious and exploitative nature contributed to make them feel unsecure and ‘scared’ (ENG6_migrant worker, 2015). It is too early to appreciate the full impact of Brexit and the new points-based immigration system implemented in January 2021 on the migrant labour presence in the sector. However, Skills for Care data show a drop in the number of filled posts for care workers in residential and nursing homes by 4.9 percent between March and October 2021 and a corresponding increase in vacancies. 6
In the Netherlands, reference to the need for migrant labour has remained limited and mainly concerns nursing rather than social care, although some unionists reported an increase of migrant workers at the lowest qualification levels (NL2_FNV Workplace Representative, 2017). The percentage of migrant workers in residential care is substantially lower than the share of ethnic minority workers (respectively, 12.4% and 19.7%) and both rates are lower than the shares among the total workforce (respectively, 14.2% and 24%). 7 Some care providers have tried to recruit migrant workers for nursing positions, but these initiatives have been limited in number and impact. Recruiting initiatives focus on workers from other sectors or further education to those employed at lower qualification levels. The ‘Working in care’ action programme by the Ministry of Health, Welfare and Sport in 2018, in response to the increasing shortages in the sector, did not focus on migrant workers but supported regional action plans involving care providers, educational institutions, local governments, care buyers and employees with a focus on recruitment and retention, work reorganisation and better remuneration.
The regulation of employment in care
The regulation of employment in the sector differs between the two countries in accordance with their national characteristics, being primarily based on statutory provisions in England and collective bargaining in the Netherlands.
In England, the progressive erosion of institutional and organisational power over time has resulted in a high fragmentation of union strategies. Unions rely on a diverse set of power resources depending on factors such as union identity, sectors in which the union operates, and size and type of the covered workforce. In elderly care, weak union presence and the inability to mobilise members for collective action pushed trade unions to adopt a partnership-oriented strategy (ENG7_Unison National Officer, 2014) but from a position of relative weakness. An example is the 2013 recognition agreement by Unison, the GMB and the RCN (Royal College of Nursing) with Four Seasons Health Care, at the time the biggest care provider with about 500 homes and 30,000 care home staff. This agreement allowed the unions to conduct joint pay negotiations at national level and allocated company level representation to the union with the highest local membership. The agreement attempted to ‘get more systematic in the way in which employees are treated in terms of pay and working conditions’ across care homes (ENG7_Unison National Officer, 2014). The increased union presence in workplaces also provided support with health and safety issues, discrimination, bullying and harassment, lack of training and task allocations (ENG8_Assistant Unison National Officer, 2014). However, union activists recognised the limited reach of collective gains and the low efficacy in guaranteeing a decent wage rise. Another initiative, the UNISON Ethical Care Charter pressures local authorities to take responsibility for securing decent working conditions throughout their externally contracted workforce. 8 While initially applying to domiciliary care workers, UNISON also produced a Residential Care Charter in 2017, covering the quality of care for residents, training and support for employees, working conditions (pay, working hours, contract status) and union recognition. 9 Both charters stress how poor terms and conditions for workers negatively affect standards of care. Despite the improvements achieved when implemented, the number of signatory local authorities has remained rather limited, resulting in a low and fragmented efficacy across the country and highlighting the weaknesses of voluntary approaches (Johnson et al., 2021).
Conditions in the Netherlands are fundamentally shaped by collective bargaining with full coverage. These agreements extend beyond pay to include provisions on employment duration, working hours, holidays, sickness pay, pensions, travel allowances, voice including the role of works councils, and conditions for reorganisations. The level, scope and extent of these agreements reflect the unions’ institutional embeddedness which has been considered influential in lowering the political and organisation incentives for union recruitment (Marino, 2012). However, the FNV has shown the ability to engage in organising new groups of workers to leverage membership power resources (Connolly et al., 2017) and keep ‘their position of strength’ in engaging with counterparties (Frege and Kelly, 2004). Between 2012 and 2018, for instance, it rejected the sector-wide agreements, signed by the other main unions, since it considered the envisioned protections inadequate. Instead, the FNV engaged in organising campaigns to ‘stop the race to the bottom’ and managed to improve on sectoral conditions through several local collective agreements with major care and nursing home providers. This showed an ability to depart from traditional, institutionally embedded, practices and rely on alternative power resources to achieve ‘fair’ collective gains for workers. Alliances with other stakeholders were also central in the union’s actions concerning elderly care. An example is the admittedly ‘very political’ campaign ‘Save the Care’ (NL3_FNV Organizer, 2017) which challenged the 2015 legislative change by demanding an end to the cutbacks, no ‘excessive’ profits or rewards, a clear and compulsory staffing norm, and decent employment. A petition, organised together with CNV Zorg en Welzijn and receiving almost 1 million signatories, drew wide political support and contributed to the mentioned rise in public investment.
Comparative overview employment conditions.
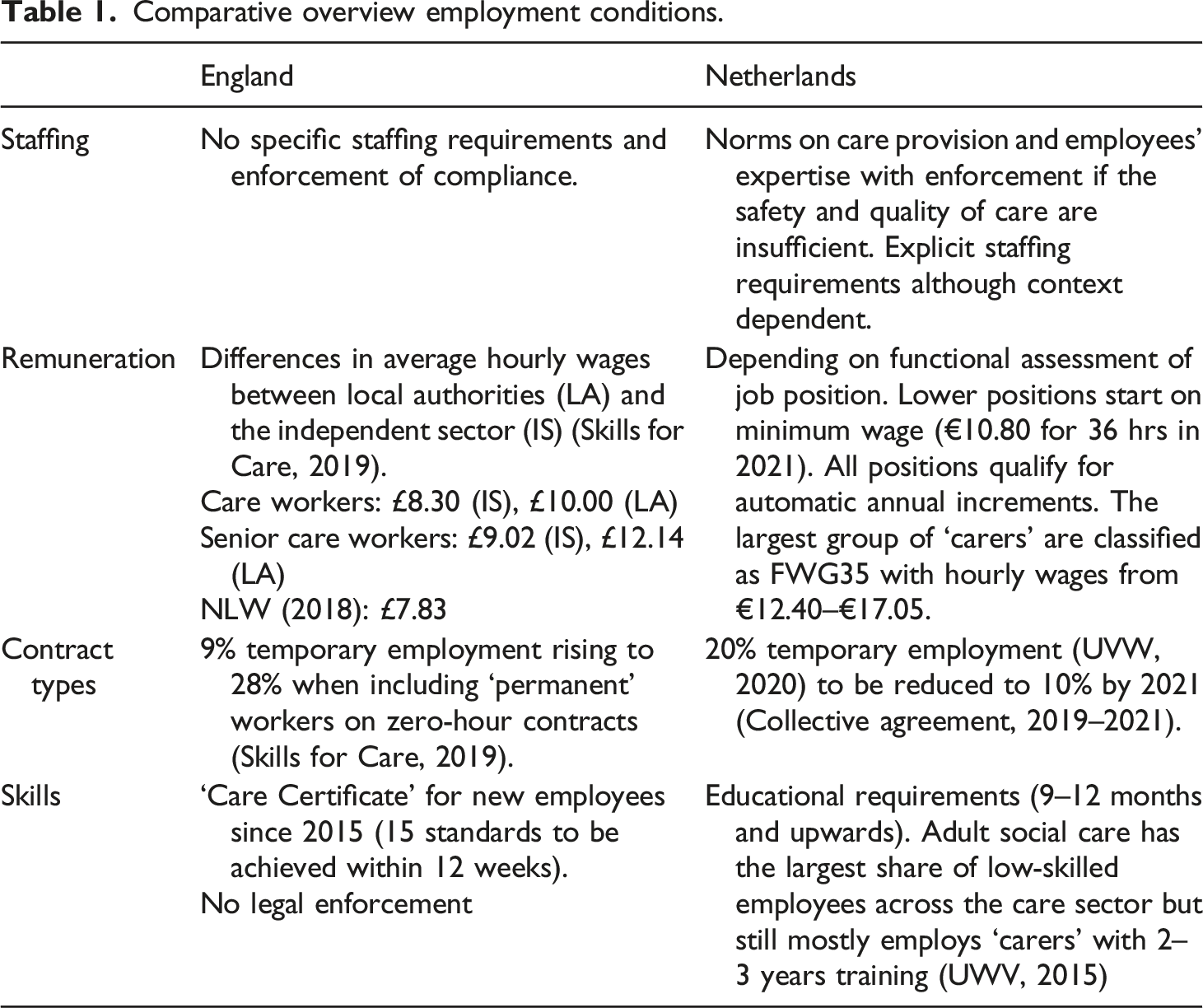
Staffing requirements
Trade unions consider staffing norms crucial to the quality of care, especially in the context of outsourced services: ‘The homes that are difficult to fill staff tend to be the homes of the poorer standard, that don’t have a good management, that offer less money than their neighbours’ (ENG1_Unison National Officer, 2015). These homes are also those in which migrant workers presence is higher (ENG1_Unison National Officer, 2015). However, quantitative staffing norms have been considered difficult to implement due to the diversity of care needs across the sector.
Organisations in England are asked to employ ‘enough staff’ to satisfy an agreed set of standards and provide ‘appropriate support, training professional development, supervision and appraisal’ (Health and Social Care Act 2008 (Regulated Activities) Regulations 2014). 10 However, the lack of a compliance regime or compulsion for providers has resulted in a diminishing number of staff (UNISON, 2013) and a progressive process of job intensification, which has been directly linked to the increase of the migrant workforce in the care homes (ENG7_Unison National Officers, 2014).
In the Netherlands, compliance with law and quality requirements is monitored with possible fines against care providers. Still, references to employment conditions are limited to the general requirement of ‘sufficient care employees’ to match the clients’ care needs. Following the ‘Save the Care’ campaign, a temporary staffing norm requiring a minimum of two carers during crucial tasks was introduced in 2017, and despite some resistance, has been fully implemented in 2019. 11
Remuneration
In England, the national minimum wage (NMW) and, from 2016, the national living wage (NLW) have contributed to pay increases since the 2000s. In 2021, the NLW was raised to £8.91 and extended to those aged 23 and over. However, the NLW might not always apply as illustrated by a recent Supreme Court decision which established that workers who sleep on site are only entitled to the NLW for the time during which they provide care (Webber, 2021). Pay rates in social care are substantially higher among local authorities than in the independent sector with the full-time equivalent average annual pay for care workers and senior care workers being, respectively, £19,500 and £23,700 in local authorities and £16,200 and £17,600 in the independent sector (Skills for Care, 2019). Recognition agreements with individual employers have played a minor role. For instance, the national level negotiations between the unions and Four Season resulted in wage increases substantially in line with the increase in the NMW and lower for employees above the NMW (ENG8_Assistant Unison National Officer, 2014). UNISON’s Residential Care Charter calls for pay on or above the Real Living Wage, to be differentiated from the NLW, and extra pay for unsocial hours but, as mentioned, remains a voluntary tool which has received limited support.
In the Netherlands, the rise in the NMW has been more limited in recent years with gradual bi-annual increases from €9.27 per hour in 2012 to €10.80 per hour in 2021 (for those 22 years and older). However, the sectoral collective agreements include pay scales based on different job grades with an automatic annual progression. For example, in the most recent agreement, 5 years’ experience in the one of the lower job grades, FWG15, offers €12.83 compared to a €11.34 starting salary, an increase of about 13 per cent. This percentage rises at higher functional levels. 12 Salary increases since 2010 have been limited but recent collective agreements (2018–19, 2019–21) offered annual pay raises around three per cent. Additional pay is achieved through one-off payments, end-of-year payments (currently 8.33% of the annual gross salary) and holiday allowances (8% of the annual gross salary with a guaranteed minimum of €2002.50 from 2021).
Employment contracts and working conditions
About nine out of every 10 workers in the English care sector have permanent contracts in accordance with the country’s comparatively limited share of flexible employment (Skills for Care, 2019). However, these data are deceptive as almost a quarter of the permanent workforce was on zero-hours contracts. Moreover, the prevalence of outsourcing to for-profit organisations has negatively affected both employment security and working conditions. The lack of sectoral collective agreements and the union weakness have allowed employers to reduce costs through the increase of flexible and precarious work and the labour intensification and deskilling of the existing labour force. Low-pay, unsocial working hours, job precarity, lack of training, and their consequent negative impact on the job-status explain to a large extent the shortage of domestic social care workers and the employers’ demand for migrant workers (ENG7_Unison National Officer, 2014). While going ‘an extra mile’ because of the commitment to the job and patients partly explains workers’ acceptance of poor working conditions (ENG8_Assistant Unison National Officer, 2014), the increasing exposure to intimidations and threat of being fired also plays an important role (ENG6_migrant worker, 2015). The impact of working conditions on recruitment and retention is confirmed by turnover differences between local authorities (14.1%) and the independent sector (32.1%), but also differences among the latter where employers with pay levels above the NLW, better working conditions, and investments in training record an annual turnover rate of less than 10 per cent (Skills for Care, 2019).
In the Netherlands, the sector has been characterised by rather high percentages of flexible employment, up to 30 per cent in 2014 (UWV, 2015). Workers also complained about work intensification and de-skilling. Some workers have been ‘forced to work less hours or otherwise be put in the flex pool’ while others work overtime with low or no additional pay and face an increase of management tasks through self-managing teams (FNV meeting1, 2017). A general lack of recognition of workers’ contributions makes them feel ‘like a washing machine’ and workers also reported cases of intimidation by employers, and the feeling of being easily replaceable (FNV meeting1, 2017). This increased after the legislative change in 2015 when many care providers did not renew temporary contracts, laid off personnel or closed their operations: ‘Everyone was afraid to lose their job, and they were pressured. The employer would say “I can get 10 others for you”’ (NL1_FNV Organizer, 2017). However, the new investments and the recent collective agreements have improved the situation. Action against rising flexibilization was central to the union bargaining agenda and a joint employer-union programme to reduce job pressure has been initiated. Recent collective agreements also reduce flexible employment, not only indirectly through ‘harder’ skills requirements but also directly by constraining employers’ use of precarious employment and particularly zero-hour and min-max contracts. This has increased permanent contracts to 80 per cent in 2018 (UVW, 2020) and the 2019–21 collective agreement states the ambition to raise the share further to 90 per cent by the end of its duration.
Skill requirements and training
The definition, enforcement and recognition of skill requirements has been a general challenge in the sector. In England, training has been historically low. Almost half of all care workers now have a relevant qualification at NVQ level 2 or higher after the government set this objective in 2003. New skill regulation for lower levels was introduced in 2015 in the form of the Care Certificate which defines a set of 15 standards, targets workers who are new to social care, and can be completed on-the-job within 12 weeks. 13 However, there is no legal enforcement. The low requirements make the sector easily accessible to workers independently by their qualifications and skills and gives employers wider discretion in recruiting and lowering conditions in the sector (ENG2_Unison National Officer, 2013). Differently from formerly recruited non-EU migrants with professional accreditations, EU mobile workers have entered England with more diverse set of skills and professional training. As such, the ‘substitution’ of non-EU workers has not necessarily been able to maintain the same level of skills guaranteed by previous policies of active recruitment.
In the Netherlands, most workers have a nursing, educational or care qualification and have access to paid on-the-job training as per the collective agreement. Over 80 per cent of direct care workers are ‘carers’, a position which requires 2–3 years of professional education (UWV, 2015). They are supported by a smaller group of assistants, with one or two years of education, for daily tasks in personal care, housekeeping and recreation. Their number has been reduced after the budget cuts in 2012 resulting in the deskilling of the more qualified carers who had to cover these daily tasks as ‘people still need to be washed and provided support while eating’ (NL2_FNV Workplace Representative). However, this trend has been partly reversed in recent years.
Discussion and conclusions
The scholarly debate on the determinants of labour migration has underlined the relevance of institutional frameworks and regulatory dynamics across several domains. This includes references to the role of national employment systems (Menz, 2009; Simonazzi, 2009) and specific aspects such as VET systems (Devitt, 2010) in determining the demand for migrant labour. These analyses highlight the centrality of the State in regulating market mechanisms, which the Covid19 epidemic has reaffirmed more drastically, against a mainstream economic discourse aimed at diminishing its intervention. However, references to the specific role of social regulation and its actors, which are fundamental in influencing the regulatory interventions of the State and in determining regulatory outcomes (MacKenzie and Martínez Lucio, 2005), have been limited.
This comparative discussion of adult social care in England and the Netherlands has illustrated the importance of social regulation. The sectoral collective bargaining in the Netherlands, and the nature of the relationship it confirms between employers/providers and workers, raises the status of jobs and provides a means to put issues on the agenda as illustrated by provisions requiring firms to consult works councils (e.g. on reduction in temporary contracts, working hours, working times). This has not prevented strong pressure on working conditions and many union representatives and workers in the Netherlands would not recognise the situation as a ‘positive’ example, especially during the period of major cost and employment reductions. However, while not always successful in achieving better employment outcomes, this regulatory framework maintains the discussion on the interrelations between quality of care and employment and, as such, the need for satisfying terms and conditions of employment. It therefore constitutes an important constraint for employers’ opportunistic behaviour and guarantees minimum standards which contribute to sustain the supply of a local workforce. This has not only offered some defence of employment conditions in the context of budget reductions but has also supported improvements in recent years such as the reversal of the earlier cutbacks in funding, the introduction of a staffing norm and the improved conditions in the latest collective agreements.
This comparison allows for the recognition of potentially virtuous and vicious circles of institutional interaction similar to Doellgast et al. (2018). The lower union strength in the English care sector and the absence of sectoral bargaining have provided employers with the leeway to lower conditions without much opposition besides the statutory legislation. This not only lowers the status of work but also makes it hard to address issues such as, for example, the demand for the NLW during night shifts. In the Netherlands, the interaction between statutory and non-statutory institutions can be depicted as a virtuous circle which constrains opportunistic employers’ behaviour and in turn limits labour market segmentation and the demand for migrant workers. The sustainability of such virtuous interactions is partly due to the path-dependent nature of the national employment and industrial relation system. The well-established industry-level collective regulation has proven crucial to maintain decent standards in the face of existing budget pressures. At the same time, the findings show how the existence of such sectoral coordination cannot be taken for granted as it can come under pressure together with the working conditions it tries to improve. In this case, maintaining ‘fair’ regulatory outcomes depends on unions’ organisational strength as well as their willingness and capacity to mobilise alternative power resources. The FNV’s refusal to sign collective agreements and success in pushing individual employers back to the bargaining table were built on membership resources and relied on organising new members as a fundamental strategy to maintain union strength and bargaining power.
While acknowledging the importance of other factors such as care and migration policies but also historical, cultural, and especially linguistic ties (Lozano et al., 2015), the findings highlight the role of social regulation and union power in shaping the demand for migrant labour. This finds further confirmation in the fact that the employment of migrant labour in the Netherlands, even if still limited, has increased more in informal live-in domiciliary care (Da Roit and Van Bochove, 2017), than in formal (residential) care where trade union presence is stronger. The centrality of collective actors’ strategies and approach, which may deviate from well-established path-dependent solutions, also suggests that similar external pressures concerning the care sector may not necessarily lead to similar solutions in terms of migrant workers’ recruitment, challenging the idea of convergence in the sector (Williams, 2012).
The findings confirm the link between migrant labour and flexible labour markets but with an important difference, if compared to other secondary labour market segments, which highlights the relevance of an intersectional approach when further investigating this relationship. While increasing migrant labour in the care sector is a clear effect of flexibilization, it cannot be considered its ‘cause’. This questions the idea of a causal circular relationship (e.g. Raess and Burgoon, 2015) between the two phenomena in this specific context where the relatively poor conditions can be related to the gendered nature of the sector. In England, providers and employers have increasingly used migrant labour and this has alleviated the need to upgrade terms and conditions of employment to appeal to a broader local supply of labour. However, the poor conditions are antecedent to the raise of intra-European migration as they are originated from and retained by the low-paid homogeneous labour market for women in part-time jobs (Rubery and Fagan, 1993). In the Netherlands, migrant labour has occasionally been considered in a context of labour shortages 14 but a shift towards migration has not taken place as social regulation and the working conditions it shapes continue to attract local workers. However, it is important to acknowledge that this positive impact of regulation potentially allows for and may even accommodate negative employment conditions for migrant workers such as discrimination and poor skill recognition. This further supports the importance of studying migration within the broader patterns of regulation, combining sector specifics, institutional regulation, industrial relations and union influence.
The intra-EU migration within the framework of free movement constitutes the ideal context to analyse the relative weight of regulatory domains other than immigration controls in determining migration inflows, with the post-Brexit UK as an interesting inverse experiment. The arguments also deny the relevance of ‘protectionist’ views which do not recognise the need for and contribution of migrant labour in the host labour markets and perpetuate their exploitation. While providing good care services is expensive, their costs are increasingly bore by the (migrant) workforce trough low pay and job intensification and indirectly by the State which is increasingly called to face the social reproduction expenses which the market refuses to cover. These observations call for mechanisms which limit the marketization of the sector, such as an increasing reliance on non-for-profit organisations and collective regulations, and the need to raise labour standards for migrant and local workers alike.
Footnotes
Acknowledgements
Our thanks to Jill Rubery, Miguel Martínez Lucio and Valeria Pulignano for their detailed feedback during the writing process. We are also grateful to the editor and the two anonymous reviewers for their valuable feedback in developing the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A part of the primary research for this article was funded by the Economic and Social Research Council (grant number ES/K001752/1).