
Abstract
Persisting post-concussion symptoms (PPCS) refers to a heterogenous cluster of difficulties experienced by a significant proportion of individuals following mild traumatic brain injury (mTBI). Innovative developments by Kenzie et al. suggest that PPCS may be understood as a complex dynamical system, with persisting symptoms being maintained by interacting factors across the brain, experience, and social environment. This paper offers a conceptual and theoretical evaluation of Kenzie et al.’s model, based on a broad set of appraisal criteria drawn from the philosophy of science. Kenzie et al.’s model is found to have several strengths. Areas for improvement highlighted include recognising the role of bodily factors outside the brain, improving the specificity and perceived importance of psychological and contextual factors, and managing the complexity of the model. Four suggestions are then made for continued development of a complex systems approach to PPCS. These include drawing on an enactive understanding of human functioning, utilising the notion of a “scientific phenomenon” to improve specificity, making riskier psycho-social hypotheses, and developing component models targeted at clinical phenomena.
Keywords
Persisting post-concussion symptoms (PPCS), historically referred to as post-concussion syndrome (PCS), is a heterogenous cluster of difficulties experienced by a proportion of individuals following mild traumatic brain injury (mTBI). Common complaints include fatigue, headache, nausea, difficulties with concentration and attention, disruptions to vision and balance, depressed mood, and others (Ontario Neurotrauma Foundation, 2018; Silverberg et al., 2023). A recent expert consensus defined PPCS as the continued experience of at least one concussion-related symptom on a daily basis, occurring more than three months post injury (Lagacé-Legendre et al., 2021). A recent meta-analysis estimated that 16.1% of individuals experience PPCS following mTBI (Cancelliere et al., 2023). Given the high rates of mTBI in the general population, PPCS can affect the lives of a significant number of people (Brazinova et al., 2021; Langer et al., 2020; Lefevre-Dognin et al., 2021). PPCS can have significant negative implications on quality of life, functioning, and community and vocational participation (van der Vlegel et al., 2021; Voormolen et al., 2018). Some patients continue to experience difficulties that they attribute to concussion for many years (Brett et al., 2023; King & Kirwilliam, 2011, 2013; Theadom et al., 2016; Wäljas et al., 2015).
Researchers have been attempting to explain and predict the development of PPCS. Historically, there was a focus on mTBI as being an underlying cause of this condition. A view that mTBI was the primary cause drove the conceptualisation of “post-concussion syndrome” (PCS), a diagnostic term used to define the persistence of symptoms. Modern perspectives, however, have taken a biopsychosocial approach to modelling, focusing on incorporating empirically derived predictive and explanatory factors further to the initial injury to the brain. These biopsychosocial models vary significantly in their approach but can be clustered into three general groupings.
Many prominent PPCS models take a prognostic approach, which focuses on identifying empirically derived risk factors for delayed recovery from concussion. Frameworks by Rickards et al. (2022) and Polinder et al. (2018), for example, list evidence-based risk factors for PPCS, breaking these down into groupings based on when they occur relative to the concussion injury (e.g., predisposing factors, injury-related factors, perpetuating factors). While often understood as explanatory, this approach is best understood as trying to predict PPCS as these models do not specify how the listed factors contribute to PPCS or its maintenance. Alternatively, a subtyping approach to modelling is also common, where PPCS is broken down into recognisable symptom profiles. While these symptom profiles frequently overlap significantly, the hope is that different profiles may index different pathological mechanisms across the biopsychosocial spectrum (Ellis et al., 2015; Haider & Bezherano, 2019; Kontos et al., 2019; Lumba-Brown et al., 2020; Maruta et al., 2018). Finally, approaches such as the Fear–Avoidance model take a focused mechanistic approach, where one particular mechanism—in this case fear of symptoms and resulting behavioural avoidance—is hypothesised to play a causal role in the perpetuation of PPCS (Faulkner et al., 2022; Wijenberg et al., 2017). Notably, none of these three approaches really seek to explain how diverse factors across the biopsychosocial continuum work together in a way that contributes to the onset and maintenance of PPCS; there is a lack of models that present an integrated explanatory account of biopsychosocial pathology in PPCS.
One key exception to this is a recent model developed by Kenzie et al. (2017, 2018) and the symptoms network models that have arisen from it (Iverson, 2019). Kenzie et al. (2017, 2018) propose that PPCS can be understood as a complex dynamical system, with persisting symptoms arising from complex and dynamical interactions across cellular, brain network, experiential, and social levels of analysis. While their model follows the recent trend towards a biopsychosocial understanding, it stands out from others in the field in its attempt to articulate how relevant biopsychosocial factors may be interacting to maintain PPCS—that is, it is an attempt at an integrated explanatory account.
In our view, Kenzie et al.’s (2017, 2018) model represents a significant theoretical advance in the field of PPCS, and we think it is timely to review it from a purely conceptual and theoretical basis (rather than in terms of its empirical adequacy). Our aim is to provide a primarily conceptual commentary on Kenzie et al.’s important model based on a broad set of evaluative criteria. This commentary is intended in constructive support of both Kenzie et al.’s model and a complex systems approach to PPCS more broadly. To be clear, we do not seek to review the wider field of PPCS, nor to review Kenzie et al.’s proposal based on a thorough analysis of its empirical validity. It is also important to acknowledge that theoretical and empirical understandings of PPCS have continued to develop since Kenzie et al.’s model was presented. In this paper we are evaluating the model from a contemporary perspective, and at times will draw on knowledge that was not available at the time of development.
In this paper, we will first list some of the qualities that good scientific theories/models typically display. These features have been drawn from work in the philosophy of science and will serve as theory appraisal criteria for our commentary. We will then overview Kenzie et al.’s (2017, 2018) model before making some evaluative comments in light of our theory appraisal criteria. We then make some suggestions for the continued development of a complex systems approach to PPCS.
Appraisal criteria
A selection of qualities that good scientific theories or models display are summarised in Table 1. The qualities listed are summarised from a range of works in the philosophy of science (Haig, 2014; Keas, 2018; Kuhn, 1977; Lipton, 2017; Potochnik, 2016, 2017; Thagard, 2019). It is useful to consider that such qualities are often in tension with each other. These qualities will serve to structure our evaluation in the next section by serving as theory appraisal criteria. In selecting them, we have not attempted to list all appraisal criteria discussed in the rich literature on theory evaluation, but rather have sought to gather a broad but manageable range of fairly uncontroversial criteria. We have also chosen to not include qualities about which we had little to comment on. To help explain these appraisal criteria we have included an analogy of a map and its relationship to the landscape it represents. In a sense, a scientific model can be understood as an attempt to map the target phenomenon. This analogy is far from perfect, but we find it helpful in demonstrating the different kinds of positive qualities that scientific theories can have.
Valued Qualities of Scientific Theories.

Kenzie et al.’s complex systems approach
Grounded in the science of complex systems, Kenzie et al. (2017) outline a conceptual framework for understanding PPCS, which is then further developed into a more specified explanatory model in Kenzie et al. (2018). We take these papers to be contributions towards the development of the same model, with Kenzie et al. (2017) focused on the conceptual framework underlying model development, and Kenzie et al. (2018) focused on presenting a more complete explanatory model. In this section we overview the model.
The core idea of Kenzie et al.’s model is that PPCS is an emergent and heterogenous set of symptoms occurring after an mTBI, maintained by complex interactions across multiple scales of the human system. The central figure representing the conceptual framework from Kenzie et al. (2017) is presented in Figure 1. This conceptual framework features four nested and emergent scales: the cellular scale, the network scale, the experiential scale, and the social scale. Each scale is itself seen as emergent from the scale beneath it, with factors at each scale free to influence “downward” to the scale beneath it. That is, there is both “downwards” and “upwards” causality. The notion of emergence utilised is one articulated by Goldstein: “the arising of novel and coherent structures, patterns and properties during the process of self-organization in complex systems” (as cited in Kenzie et al., 2017, p. 10). It is also recognised that elements in the environment can impact factors at any of these scales.
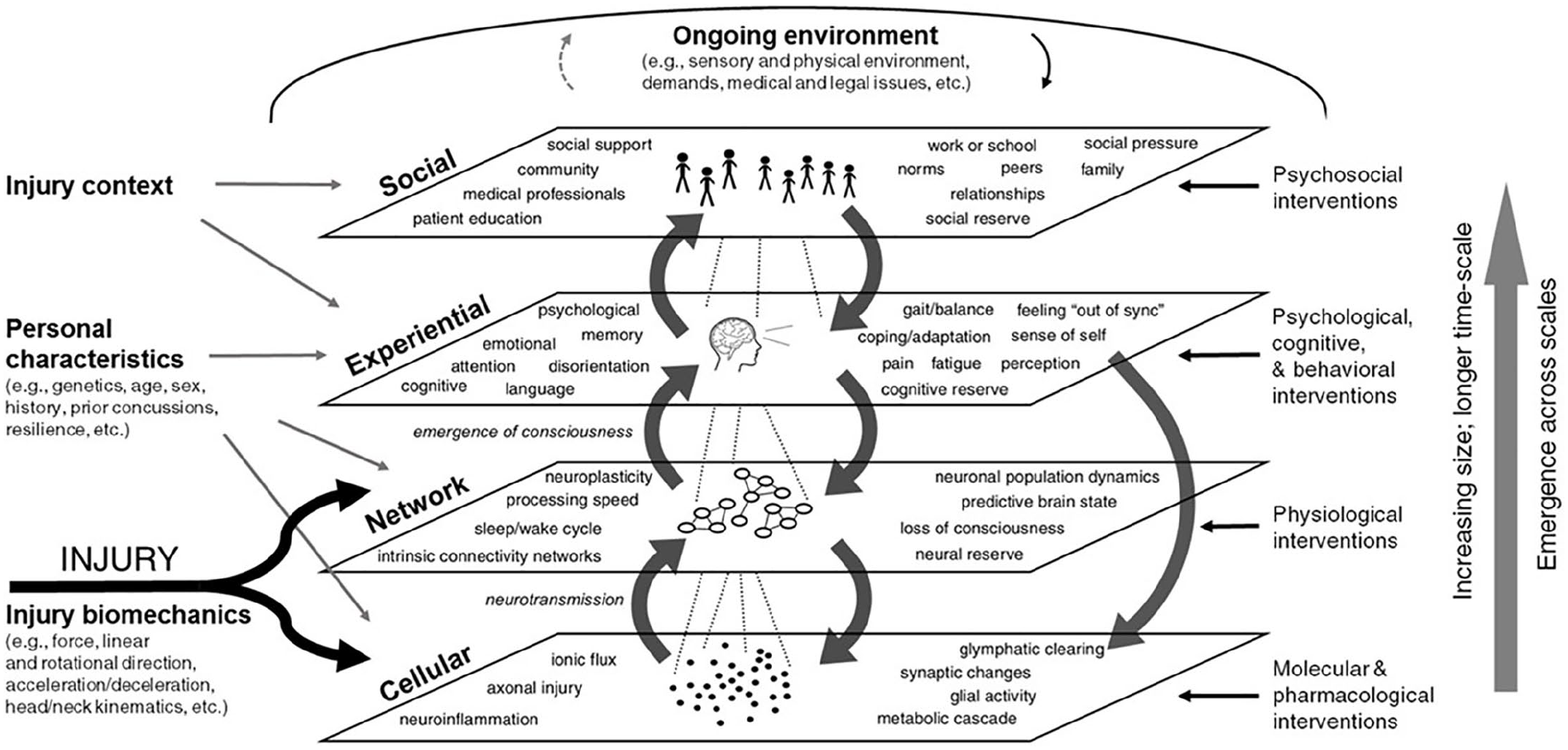
A Diagram of the “Mental Model” or Conceptual Framework Underlying Kenzie et al.’s Complex Systems Approach. Originally Presented in Kenzie et al. (2017). © 2017 Kenzie, Parks, Bigler, Lim, Chesnutt and Wakeland.
As can also be seen in Figure 1, Kenzie et al.’s (2017) conceptual framework includes some noted influences from outside these four scales. These include (a) the biomechanics of the initial injury, (b) the personal characteristics of the injured individual, and (c) the injury context. To reiterate, the central idea of this framework is that following initial perturbation by mTBI, factors across these four scales interact in complex nonlinear ways that facilitate or delay recovery. Kenzie et al. also highlight that subtypes of PPCS may emerge as we begin to understand the wider landscape of these complex dynamics.
Building upon the conceptual framework presented in Kenzie et al. (2017), Kenzie et al. (2018) utilise causal-loop diagramming to develop the framework into a more specified explanatory model. To do so, they draw on a broad range of literature, interviews with experts, and direct expert involvement. Kenzie et al. (2018) also features a summary image of the model, which is reproduced in Figure 2. As can be seen, this model seeks to capture in greater detail the hypothesised network of causal factors and nonlinear interactions that occur across the various scales. Despite its complexity, Kenzie et al. (2018) emphasise that this model “is intended as a preliminary demonstration of this method and only captures a portion of the immense complexity of concussion recovery” (p. 3). Thus, it is important to note that Kenzie et al. see their model as still under development.
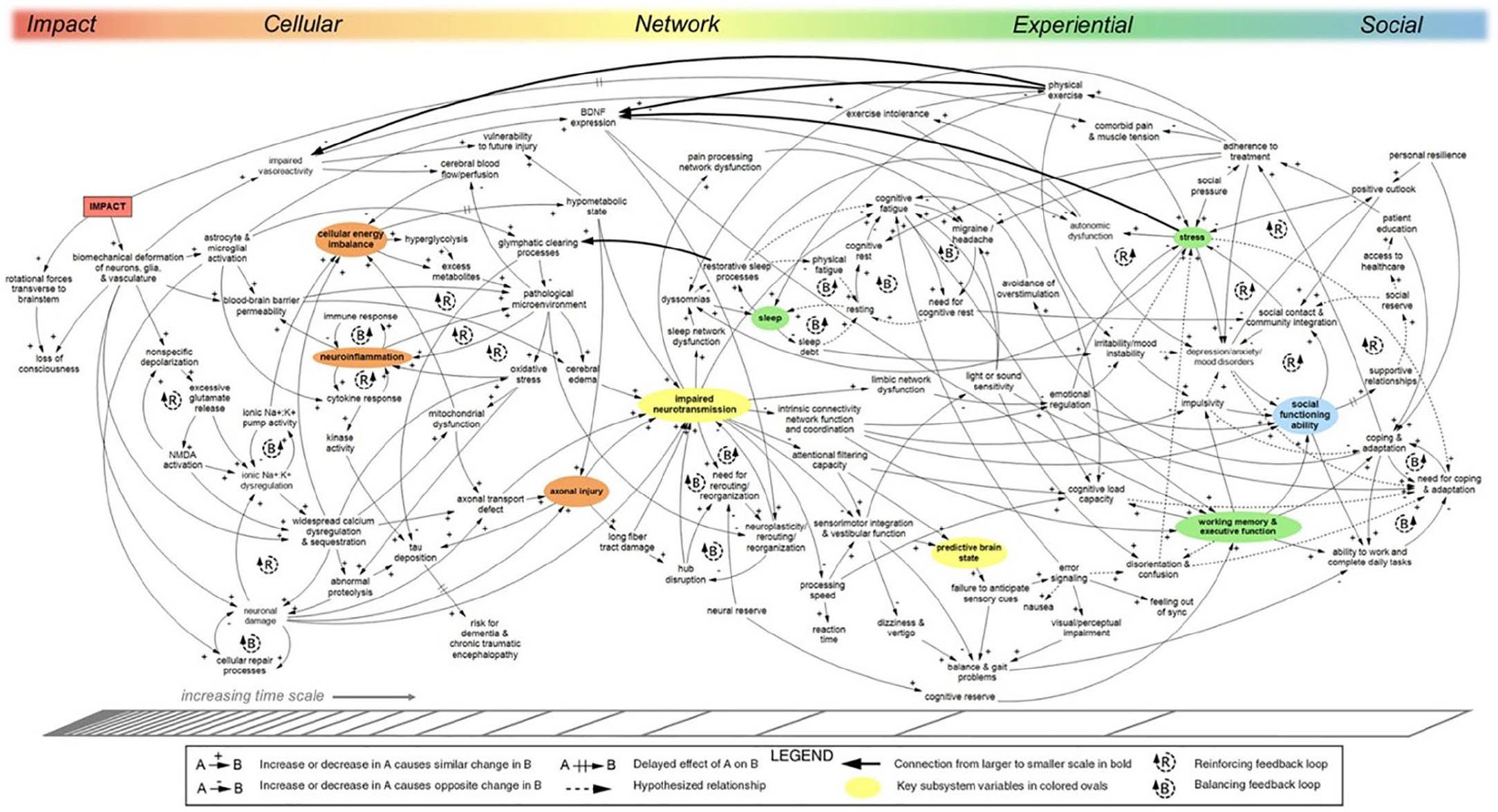
A Causal Loop Diagram of mTBI. Originally Presented in Kenzie et al. (2018). © 2018 Kenzie, Parks, Bigler, Wright, Lim, Chesnutt, Hawryluk, Gordon and Wakeland.
To parse some of the noted complexity of the model, Kenzie et al. (2018) highlight “key indicator variables” at each scale (p. 4). These include: cellular energy imbalance, neuroinflammation, and axonal injury at the cellular scale; impaired neurotransmission and disrupted prediction of sensory input at the network scale; sleep disruption, stress, and working memory / executive difficulties at the experiential scale; and disruption to social functioning abilities at the social scale. It is unclear if these “key indicator variables” are understood to be of particular explanatorily relevance, or if they are picked out for some other reason. It is also notable that in this image the scales are represented in a way that implies continuity between them rather than clear separation as implied in Kenzie et al. (2017).
As another way of breaking down the complexity of the model, Kenzie et al. (2018) also present more targeted causal loop diagrams highlighting particular feedback loops at and across the various scales (Figures 5–8). We have chosen to not present these diagrams here. These smaller scale causal loop diagrams, abstracted from the wider model, appear to be focused on positive and negative feedback loops of apparent relevance to the maintenance of PPCS, such as how stress and physical exercise both impact elements of the network at “lower” scales. This feeds into one of the core ideas presented by Kenzie et al. (2018): that interventions in mTBI may be understood to support recovery by shifting the balance within the wider network of interactions, toning down “reinforcing” feedback loops that maintain PPCS, and activating “balancing” feedback loops that encourage a return to allostasis.
Before moving on, it is worth mentioning a related proposal by Iverson (2019). Based on Kenzie et al.’s (2017, 2018) conceptual model, Iverson (2019) argues for the utility of symptom network modelling in the study of PPCS. Symptom network modelling is a particular methodology for capturing correlations between symptoms, ideally in a longitudinal fashion, to infer a network structure that may account for the persistence of symptoms over time without reference to a latent cause. While this is an exciting development, on our reading, Iverson appears to be presenting a methodological approach rather than novel explanatory model and does not appear to develop substantially on Kenzie et al.’s core ideas. For this reason we have here focused our analysis on Kenzie et al. (2017, 2018).
Evaluating Kenzie et al.’s model
In this section, we will evaluate Kenzie et al.’s (2017, 2018) model, using the theory appraisal criteria presented in Table 1. We will first comment on strengths before moving on to more critical comments.
Strengths
Kenzie et al.’s (2017, 2018) model represents a significant step forward in the conceptual understanding of PPCS. Biopsychosocial understandings are now a mainstay within the field; however, these have tended to feature relatively linear formulations and ultimately fall short of capturing the complex network of factors often seen with mTBI. Kenzie et al.’s model thus aligns with and furthers a field-wide move beyond a simple hunt for underlying neurological causes. Vitally, Kenzie et al.’s model suggests a more dynamic and thoroughly biopsychosocial approach where psycho-social factors not only “shape the outcome” but drive symptoms themselves—resulting in the emergence of symptom-reinforcing feedback loops within the system. The flow of causality within Kenzie et al.’s model does not simply come “from below” while being constrained by psychosocial factors “above,” but instead causality is seen to flow in all directions, including “downward” and “around and around.” Acknowledging such causal complexity helps to account for key features of PPCS that other models struggle to explain, such as the heterogeneity of symptoms, the variability in duration of symptoms, and the nonlinear nature of recovery. This thereby lends Kenzie et al.’s model a particular strength in terms of empirical fit and explanatory breadth relative to other models in the field.
Another key feature of Kenzie et al.’s (2017, 2018) model is the breadth of explanatory mechanisms featured. While the model is complex, it manages to capture a very wide range of biopsychosocial phenomena and causal links hypothesised to play a role in PPCS. The interactions between these features are reasonably well specified for a dynamically focused model—at least at the cellular and network scales—thus highlighting clear avenues for continued empirical investigation of causal links within the model. A review of how well available empirical evidence supports this model is out of scope, however it is noteworthy that model design involved collaboration with experts, suggesting reasonable empirical fit.
Considering the large range of causal relationships featured, the model over all can be considered relatively parsimonious. This may strike some readers as odd given the clear complexity of the model. It is important to remember that parsimony is not equal to simplicity, but also considers the breadth of features accounted for. Given the noted symptomatic heterogeneity and nonlinear recovery course of PPCS, it is very plausible that it is simply a complex phenomenon by nature. To capture such a phenomenon, our models may therefore have to acknowledge and work with this complexity.
A range of other strengths are also apparent. By summarizing such a broad range of knowledge about PPCS into a unified model, Kenzie et al.’s (2017, 2018) proposal offers a unifying account of current understanding. This brings utility for researchers. While the idea that PPCS may be an emergent multiscale phenomenon will be hard to empirically assess using current methods, it is fair to say that the model is novel and ambitious. We would argue that this, along with the way the model acknowledges complexity, is inspirational—encouraging curiosity and further exploration. Considering this, and the model’s role in the emergence of network modelling in the field, the model can also be said to be fairly fruitful (although fuller evaluation will require observation of how the model impacts the field over time). All in all, Kenzie et al.’s model is a major step forward in efforts to understand PPCS. The contributions of the current paper are intended in support of this exciting approach.
Critical observations
In this section, we reference our appraisal criteria to make some critical observations of Kenzie et al. (2017, 2018), highlighting four key areas for further development for a complex systems approach to PPCS. Our first area for improvement concerns the omission of the body from the model. As discussed earlier and as represented in Figure 1, Kenzie et al.’s underlying conceptual model is based on four nested and emergent scales: cellular, network, experiential, and social. It is relevant here that Kenzie et al.’s (2017, 2018) discussion of the cellular and network scales is entirely focused on the brain. Considering this, the wider body outside the brain is not represented in the conceptual structure of the model. As we will show, this negatively impacts the external coherence and explanatory breadth of the model.
This omission of the wider body is relevant to the appraisal criteria for two reasons. The first reason is more conceptual and concerns the appraisal criterion of external coherence. Consider that the four scales and other structural elements within Kenzie et al.’s (2017, 2018) model essentially represent assumptions about human functioning. While the brain is of obvious importance when talking about the effects of a brain injury, it is well recognised that the brain is intimately and bidirectionally connected to the wider body in terms of both physiology and function (Freund et al., 2016; Pessoa, 2023). This is an empirical finding gaining more and more recognition within science more broadly, but given particular emphasis within the field of embodied cognition (Fuchs, 2017; Shapiro & Spaulding, 2021; Thompson & Cosmelli, 2011). By not including the wider body, the model conflicts with accepted understandings of how the human body and brain work, negatively impacting external coherence. To return to our map analogy, by representing human functioning without leaving space for the role of the body, the map being presented is conflicting with other maps that cover the same landscape.
The second reason that the omission of the body is relevant to the considered appraisal criteria is that not having a place for the body in the conceptual model diverts explanatory attention away from mechanisms that involve the body. This negatively impacts the explanatory breadth and empirical fit of the model. PPCS concerns broad aspects of the human experience, including pain, cognition, sleep, balance, vision, endocrine function, and so forth, and these aspects all thoroughly involve the wider body. In line with this, factors within the body but outside the brain are recognised within the literature as likely mechanisms that may support PPCS. Consider, for example, that c-spine dysfunctions commonly contribute to the experience of cervicogenic headache and balance difficulties in PPCS (Marshall et al., 2015). This mechanism, of clear importance to understanding PPCS, is not referenced in Kenzie et al.’s (2017, 2018) model. Other factors situated within the wider body include peripheral pain sensitization (Blumenfeld et al., 2022; Gold & Gebhart, 2010), and disruptions to the gut-brain axis (Celorrio & Friess, 2022; Soriano et al., 2022). These mechanisms are also not included in Kenzie et al.’s (2017, 2018) model. We suggest that such omissions may be secondary to the conceptual omission of the body within the underlying framework. Not including the wider body seems to have placed limitations on the breadth of mechanisms captured within Kenzie et al.’s model and reduced recognition of recognised features of PPCS. Returning to our map analogy, because of decisions made about what areas of the landscape are relevant, the map is missing some important and task-relevant landmarks.
A second area for improvement concerns the way that psychological and social factors are incorporated into Kenzie et al.’s (2017, 2018) model. By psychological, we refer to many of the experiential, emotional, and behavioural factors, as well as broader elements such as history, context, and personal agency. As it is currently presented, Kenzie et al.’s model lacks specificity regarding the psychological and contextual aspects of PPCS, negatively affecting the model in several ways. To return to our map analogy, one large and important area of the map is effectively blurry.
To evidence this claim, consider the model as presented in both papers (Kenzie et al., 2017, 2018). Many key psycho-behavioural factors central to the maintenance of and/or recovery from mTBI are not represented, including: overall activity level, engagement with symptom-aggravating activities, beliefs about one’s symptoms, and behavioural avoidance. In the more detailed explanatory model in Kenzie et al. (2018), some psychological factors of recovery such as “personal resilience,” “coping and adaption,” and “emotional regulation” are included. However, these factors are very abstract in nature. They refer to complex phenomena or capacities and are not unpacked or discussed further. Indeed, given just how abstract and outcome-focused these notions are, it is not exactly clear what they refer to. For example, there are many ways that individuals can be said to regulate their emotions and many ways this ability can be compromised (Gross, 2015). In other words, emotional regulation is a multirealisable capacity, not a specific phenomenon that may appropriately serve to specify a maintenance mechanism in a model such as this. Similarly, an experiential factor “headaches/migraine” is included in the model as a single object with the same causes and influences (see Figure 2), but headaches within PPCS are diverse phenomena with a similar experiential quality—for example, tension vs. migraine headache (Blumenfeld et al., 2022). As another example, “depression/anxiety/mood disorders” is included as a single factor despite these each being complex conditions in their own right—arguably just as heterogenous as PPCS is (Contractor et al., 2017; Olbert et al., 2014). Articulating these aspects of the model in such general terms limits the ability of the model to represent empirically testable and specific psychological mechanisms that maintain PPCS.
One key consequence of the lack of specificity in the psychological domain is reduced clinical utility. Using this model, a clinician would be offered very little guidance as to how to understand the psychological aspects of a patient’s difficulties, other than to identify that a patient isn’t very “resilient” or that they are having difficulties with “coping and adaption.” Much greater specificity is required before the psychological aspects of the model could meaningfully offer useful treatment guidance.
A third area for improvement concerns the implied importance of psychological and social factors in PPCS. With the role of psychological agency underspecified in the model, one gets the impression those experiencing PPCS are somewhat passive in the recovery process and psychological factors are not of central importance. By analogy, if one area in the corner of a map is blurred out it implies nothing important happens there. This impression is also reinforced by the structure of the model. For example, explicit room is made within the conceptual model for “interventions” at the various scales, through which relevant clinicians can be understood to shape recovery. However, there is little explicit room made for the efforts of the affected individual to shape their own recovery, either positively or negatively. As discussed above, factors such as “coping and adaption” are included but are very underspecified. Importantly, this impression appears unintentional, and may well reflect the state of knowledge and conceptualisation at the time of model development. Kenzie et al. (2017) state: “to understand the heterogeneity, uncertainty, and complexity in the conscious, felt experience of concussion, we must understand how these variables appear, disappear, and are modulated by personal characteristics, history, and context” (p. 9).
This impression, that psychological factors are not centrally important to PPCS, is relevant to our appraisal criteria for two reasons. The first is that the explanatory role of psychological factors is widely recognised by the field (Broshek et al., 2015; Faulkner & Snell, 2023; Polinder et al., 2018; Rickards et al., 2022). A failure to emphasise the role of psychological factors therefore arguably impacts the empirical fit and explanatory breadth of the model. The second reason is based upon our own clinical observations and is therefore proposed more tentatively. As psychologists working with those experiencing PPCS, recovery often stalls when there is conflict between the requirements of recovery and the person’s mode of functioning in the world. “Mode of functioning” is a concept borrowed from Nielsen (2023) that refers to the ways in which—based on their evolutionary, cultural, and developmental history—a person understands themselves, the world, and goes about achieving important functional objectives. For example, factors that made a person “resilient” in the face of previous adversity or a high-level vocational demand (e.g., an ability to tolerate pain and focus on what they are working on) may now, in the context of PPCS, support a pattern of pushing through symptoms until they are exhausted, ultimately slowing recovery. Psychological input for PPCS often involves development of psychological and behavioural flexibility, learning to let go of previously helpful strategies and adapt to the challenges of recovery (Faulkner et al., 2022). This requires active engagement from patients as agents in their recovery. Supporting patients with making such changes requires an understanding of the person’s history, how they have learned to live their lives, and their current goals. Without this understanding, it can be very difficult to understand why someone may act in a way that ultimately perpetuates their symptoms. Failing to sufficiently capture the psychological aspects of PPCS and highlight their importance is therefore likely to negatively affect the clinical utility of the model.
Our final area for improvement concerns the management of complexity. Models in science are both representations of the world and tools for use by scientists (and in this case clinicians). As such, scientific models are subject not only to epistemological values—that is, how well they represent the topic of study—but also to pragmatic values—that is, what we have here labelled the quality of utility (Potochnik, 2016, 2017). For a model of a clinical problem this means that, all else the same, structuring models in a way that is accessible to clinicians is a genuine theoretical virtue. Improvements in the management of complexity are likely to improve the utility of the model, encouraging use by researchers and clinicians.
mTBI and the challenge of persisting symptoms appears to be an extremely complex phenomenon. Kenzie et al. (2018) highlight this well and the complexity of their model underpins many of the strengths we have here overviewed. However, this complexity may still be seen as overwhelming, and we worry this may discourage both scientists and clinicians from using this model. This is a tension Kenzie et al. appear to have recognised, as they make several efforts to parse the complexity of the multiscale network they are articulating—that is, highlighting key indicators and presenting more focused causal loop diagrams. The online version of their model also offers useful interactive ways to manage complexity. Despite these efforts, the presentation of the model is still very complex. This likely limits the utility of the model for both researchers and clinicians. To return to our map analogy, the map is trying to capture very complicated terrain, but we can still acknowledge the map is hard to use and try to improve on this.
In summary, our conceptual and theoretical analysis of Kenzie et al.’s (2017, 2018) model has suggested four areas where further development is most required. These are: (a) recognition of the wider body, (b) the specificity of the psycho-behavioural aspects of the model, (c) recognition of the importance of psychological factors/patient agency, and (d) the management of complexity. We have here shown how these four areas are relevant to our listed theory appraisal criteria.
Suggestions for continued development
Our analysis highlights several ways in which Kenzie et al.’s (2017, 2018) model is a significant step forward for the field. It also highlights four key areas for potential continued development for a complex systems approach to PPCS, as summarized above. In this section, we offer a series of suggestions for making improvements in these areas.
Suggestion 1: Embodiment, embedment, and enactivism
Given the physiological and functional embedment of the brain within the body, there needs to be allocated space for the wider body within any conceptual framework of brain injury. We strongly suggest that future iterations of a complex systems approach to PPCS make explicit conceptual space within the underlying framework for the role of the wider body. Doing so will immediately improve external coherence and make room for embodied mechanisms currently excluded from Kenzie et al.’s (2017, 2018) model, such as c-spine and gut–brain axis dysfunctions—thus improving explanatory breadth. Such a move will also leave the model open to incorporating any future discoveries concerning the role of the wider body in PPCS.
Regarding how to achieve this inclusion of the body, this will likely require moving away from the notion of “emergent and nested scales” as utilised in Kenzie et al.’s (2017) framework. It is hard to imagine how one would make sense of the relationship between brain and body using this hierarchical structure. The network structures of the brain are, after all, not emergent from the body but are rather embedded within it. To include the body, an alternative set of assumptions about human functioning would therefore be required. Keeping with the strengths of Kenzie et al.’s current approach, any candidate replacement framework would have to allow for biopsychosocial interactions and “downward causality.” Based on our analysis it should also offer greater recognition of the wider body, and not dismiss psychological factors as epiphenomenal or otherwise less explanatorily important. One plausible framework to fill such a role is enactivism.
Enactivism refers to a particular set of philosophical and neuroscientific assumptions about how the mind works that has overlapping roots with dynamical symptoms theory (Fuchs, 2017; Gallagher, 2017; Thompson, 2010). Recent developments in the philosophy of psychiatry have suggested enactivism represents a fruitful platform from which to understand the complex causal structures of psychopathology (de Haan, 2020; Fuchs, 2017; Gallagher, 2024; Maiese, 2021; Nielsen, 2023; Stein et al., 2024). It is emphasised how these ideas offer a means though which to integrate an understanding of the various biopsychosocial factors known to be at play in mental illnesses. For example, the framework of “3e Psychopathology” conceptualises mental disorders as complex process structures spanning the brain–body–environment system, keeping people stuck in patterns of making-sense-of and acting-in the world that work against their functioning (Nielsen, 2023). Drawing inspiration from this enactive turn within the study of psychopathology seems appropriate because of the overlapping conceptual needs shared by the study of PPCS and the study of mental disorder. Both PPCS and mental disorders (e.g., depression) appear to be complex and heterogenous conditions that sit at the crossroads of mind and body. These similarities bring with them a shared need for conceptual tools to grapple with this complexity and to navigate the apparent mind–body divide. It therefore seems potentially fruitful to “cross-pollinate” ideas between these two areas of study.
To briefly overview, enactivism is a naturalistic perspective on the mind and human functioning. It recognises that human behaviour and experience is influenced by factors across the brain, body, and environment. Central to our purposes, under an enactive view, the mind does not emerge from the brain as a separable thing but is instead understood as an ongoing process constituted by the brain–body system as it navigates and makes sense of its environment. The three most important concepts to understand within this view are that the mind is “embodied,” “embedded,” and “enactive.” Embodied refers most centrally to the idea that the mind is not separate to the brain and body, rather the mind is constituted by the entire body acting in context, and that the brain needs to be understood in the context of the body (Shapiro & Spaulding, 2021; Thompson, 2010). Embedded refers to the idea that virtually all aspects of human functioning involve constant interplay between individuals and their environments over multiple timescales—that is, that we both shape and are shaped by our environments over time (Fuchs, 2017). An embedded perspective holds, for example, that understanding a patient’s context and history is always going to be vital for a full understanding of behavioural and medical difficulties. Finally, enactive refers to the idea that the mind, and our ability to experience meaning, has evolved primarily to facilitate adaptive action in context. The mind, to an enactivist, is primarily an ongoing process of sensorimotor exchange between organism and environment, with more complex or internalised cognitive processes having evolved in a way that builds upon this structure. Under an enactive view, this process constitutes the enaction of meaning for the organism in question, thus cognition is understood as “sense-making,” an ongoing and body-involving process of making sense of and engaging with the world (Thompson, 2010). Enactivism assumes both an embodied and an embedded view, hence why the term enactivism is used here to refer to this collection of ideas.
We suggest that grounding future developments of a complex systems approach to PPCS within an enactive understanding of human functioning may be fruitful. Congruent with both Kenzie et al.’s (2017, 2018) model and 3e Psychopathology, an enactive understanding would construe PPCS as a complex and distributed process structure extending across the brain–body–environment system, inhibiting a person’s attempts to go about their normal day. Developing upon Kenzie et al.’s model, however, an approach grounded in an enactive perspective would make space for the wider body. Clinically speaking, doing so would arguably encourage clinicians to look beyond PPCS as their unit of analysis and intervention, to deeply consider the patient’s context and the way PPCS is interwoven with the patient’s history and psychological life. It would also recognise that, while a medical condition, PPCS is interwoven with the individual’s processes of meaning-making. We offer the development of an enactive perspective as one plausible avenue for continued conceptual development of a complex systems approach to PPCS.
Suggestion 2: The notion of “phenomena”
Our next suggestion for future iterations of a complex systems approach to PPCS is that factors included in the model should be restricted to genuine or at least putative scientific phenomena. Doing so should help to improve the specificity of the model, especially within the psychological and social domains. Phenomena is here used as a technical term referring to evidenced regularities/occurrences inferred from data about the world (Bogen & Woodward, 1988). Under this definition, then, a scientific phenomenon refers to a relevant regularity in the world; a meaningful object, process, or capacity, fit to play a role within or be the subject of a scientific explanation (Haig, 2014). Clinical phenomena, meanwhile, similarly refers to phenomena of clinical relevance (Ward & Clack, 2019). This notion of a scientific phenomenon is useful as it restricts what factors can be included in an explanation to those suited for this role, thus maintaining specificity. Of particular interest in this case is that this notion discourages use of multiply realisable factors in our explanations—that is, factors that look similar, but on closer inspection turn out to be better conceptualised as multiple different things with separate causes and consequences. To use an example from psychopathology, the notion of anhedonia, a common symptom of depression, has been argued to likely represent multiple phenomena with similar experiential qualities (Clack & Ward, 2020).
Considering Kenzie et al.’s (2018) model (see Figure 2), we noted earlier that “headache/migraine” is included in the model as a singular factor with the same causes and consequences. The same is true of the factor “depression/anxiety/mood disorders.” Both factors each represent diverse phenomena, likely with diverse causes and influences within the PPCS network. As discussed earlier, lumping these phenomena together negatively impacts the specificity of the model. Requiring factors included within the model to meet the conceptual requirement of being a plausible scientific phenomenon (rather than many different things lumped together) will improve specificity. This is because it will require splitting such multirealisable factors into more specified and stable conceptual objects. This will then allow for more specified causal hypotheses to be drawn about the relations between these objects. For example, setting such a constraint on inclusion in the model would require that broad and multirealisable notions such as “resilience” or “coping and adaption” be decomposed into more specific and meaningful concepts (such as specific patterns of behaviour), thus affording the model greater specificity and utility. With improved specificity in this area of the model, psychological factors will also likely appear to be more explanatorily relevant.
Suggestion 3: Push the psychosocial boat out
While there is clear agreement across the field that psychological and social factors play key roles in PPCS, the understanding of how psychological and social mechanisms may contribute to genuine symptoms appears to be relatively underdeveloped and lacking in specificity (Broshek et al., 2015; Polinder et al., 2018; Silverberg & Iverson, 2011). Arguably, then, one reason the psychological and contextual aspects of Kenzie et al.’s (2017, 2018) model are somewhat underspecified is that the model is an attempt to summarize this available evidence at the time of model development. To be clear, some specific psychological mechanisms are recognised and evidenced in the field, including, for example, the misattribution of normal experiences/“symptoms” to the injury (Gunstad & Suhr, 2001; Yang et al., 2014), anxiety sensitivity leading to greater discomfort and therefore symptom reporting (Whittaker et al., 2007; Wood et al., 2011), and inflexible fear-avoidance leading to under-activity (Faulkner et al., 2022; Wijenberg et al., 2017). However, many psychological factors discussed in the literature appear much less specific. For example, comorbid psychiatric conditions are a frequently cited perpetuating factor in PPCS, yet discussion rarely goes beyond this to consider specific conditions and how these conditions may negatively impact recovery processes or otherwise act to maintain symptoms (Faulkner & Snell, 2023). Such underdevelopment appears to be recognised regarding social factors; for example, a recent multidimensional review states: “Community integration, social support, lifestyle, and family dynamics may contribute to the development and persistence of post-concussion symptoms . . . [h]owever, conclusive evidence has not yet been established” (Polinder et al., 2018, p. 5).
Given this state of the field, our third suggestion is that future iterations of a complex systems approach to PPCS seek to “push the boat out” and hypothesise just beyond the bounds of available evidence in the psychological and contextual domains. One of the evaluative criteria we have discussed is fruitfulness, that is, the degree to which a model inspires further scientific exploration and provides novel hypotheses. While we have here suggested that Kenzie et al.’s (2017, 2018) model is a relatively fruitful one for various reasons—and while it certainly provides a novel conceptual perspective on PPCS as a whole—it does not provide much in the way of novel and specific causal hypotheses to be tested. Given the thoroughly biopsychosocial conceptual underpinnings of this complex systems approach to PPCS, we suggest that future iterations of this approach will be ideal vehicles for novel psycho-social hypotheses. To return to our map analogy, we suggest that future iterations of this map “sketch in” some speculated detail in the blurry unknown regions. Doing so (while constrained by the ideal of utilising scientific phenomena as per suggestion two) will hopefully encourage exploration of these areas. This should help to address our concerns about the specificity of the psychological and social domains, improve the fruitfulness of the model, and encourage further developments in this area.
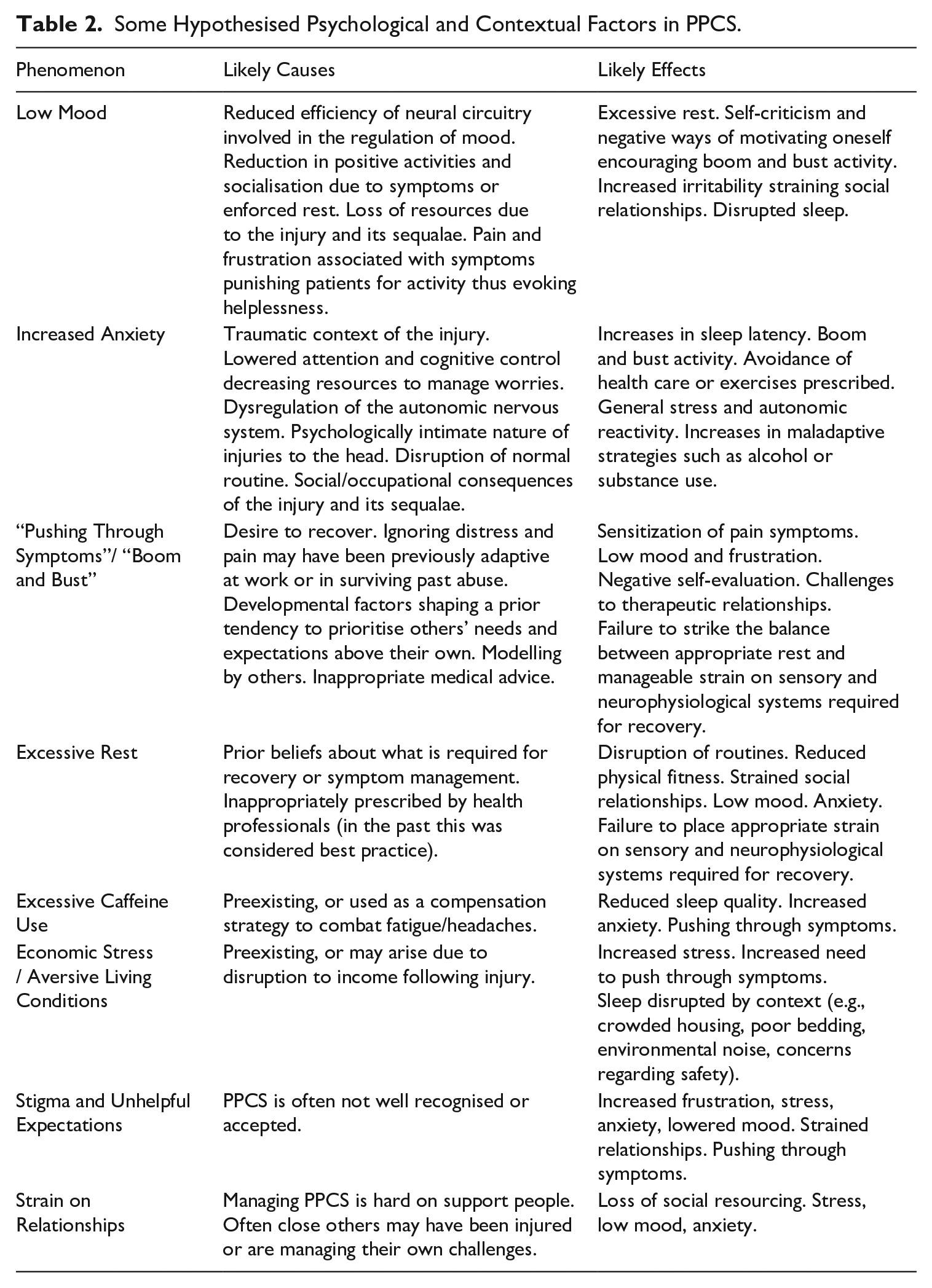
In support of this suggestion, Table 2 offers some psychological and contextual hypothesises. These are inspired by our own clinical observations as well as relevant review articles including Broshek et al. (2015), Lumba-Brown et al. (2018), and Silverberg and Iverson (2011). In proposing these factors, we suggest they may contribute to the wider PPCS process structure as per the complex systems approach. In line with suggestion 2, we have sought to include more specified phenomena than are currently included in Kenzie et al.’s (2018) model. For each factor we outline likely causes (i.e., why the phenomenon may be more likely to occur in PPCS), and likely effects (i.e., how the phenomenon may contribute to other elements in the PPCS network). Thus, we aim to articulate how these hypothesised factors may be contributing to the perpetuation of the wider PPCS system.
Some Hypothesised Psychological and Contextual Factors in PPCS.
Suggestion 4: Structure the use of “pop-out” models
Finally, regarding the practical management of complexity within a systems approach, we suggest building upon Kenzie et al.’s (2018) use of targeted diagrams abstracted from the wider model. However, we suggest developing further on this approach in a structured way, thus introducing an element of modularity to future models. Drawing on the Relational Analysis of Phenomena (RAP) approach (Nielsen & Ward, 2020), we suggest the development of smaller scale component models targeting individual clinical phenomena within PPCS and of their relations to other phenomena within the PPCS system. As component models, these would be understood to be artificially abstracted from the wider model of PPCS. In line with our map analogy, these would be the equivalent of “pop-out” sections of greater detail on a map. This builds upon the way that Kenzie et al. (2018) present smaller scale causal loop diagrams abstracted from the wider model, a feature they also utilise in their online version of the model. However, rather than being based on any feature of interest to the researcher, we would suggest producing these smaller scale models in an organised way. Specifically, we suggest targeting such “pop-out” models on recognised clinical phenomena (i.e., symptoms) in PPCS, thus supporting greater clinical utility.
There are clear advantages of incorporating component models focused on clinical phenomena into a complex systems understanding of PPCS. Firstly, adding an intermediate level of abstraction is likely to help with general comprehensibility of the model, as those engaging with it can clump/cluster the complex information being presented more readily. Secondly, orientating this middle level of complexity around clinical phenomena (i.e., “symptoms” that clinicians will recognise) is likely to facilitate clinical translation and utilisation of the model, as clinicians will be more able to integrate the model with their clinical understandings of PPCS. This is likely to improve clinical utility relative to the current focused causal loop diagrams which do not seem to be targeted in a structured way or align with clinical understanding. Lastly, as articulated in Nielsen and Ward (2020), introducing a set of explanatory targets (i.e., clinical phenomena or clusters thereof) at a middle scale of complexity within a conceptual model of a given complex pathology may allow dispersed researchers to better co-ordinate their efforts in producing coherent knowledge. They argue that introducing such co-ordinating epistemic structures is likely to result in a faster route to deeper understanding of that pathology at a field-wide level.
To explain this further, introducing component “pop-out” models of individual clinical phenomena (or small clusters thereof) within the wider model of the PPCS system would provide a co-ordinating structure for researchers studying PPCS around the world. Such a co-ordinating structure would then allow researchers to better consider and communicate how the knowledge they have produced fits into our wider understanding of the PPCS system. For example, imagine that a given research team working within this framework produces a detailed analysis of fatigue in mTBI. Conceptually, this component model of fatigue could then be “slotted in” to the wider model, supporting a structured understanding that is easier to comprehend and theorise about, and also easier for clinicians to access and apply to when formulating their patients’ difficulties and targeting treatments. With a similar process completed iteratively around the world, a complex systems approach to PPCS could conceivably evolve in a structured and accessible way.
Conclusions
PPCS is a serious and impairing set of difficulties experienced by many people after mTBI. Kenzie et al. (2017, 2018) have presented a very promising approach to conceptualising and modelling the dynamical constitution of PPCS. In support of this approach, we have evaluated the model against a broad series of theoretical qualities. Several strengths were highlighted, and it was concluded that this model is a significant conceptual and theoretical step forward for the field. Areas for continued improvement were also highlighted. We argued that there is room for improvement regarding recognition of the wider body, the specificity of psychological and social factors, the perceived explanatory importance of these factors, and the practical management of complexity. In response, we made four suggestions for the continued development of a complex systems approach to PPCS: the possibility of making conceptual space for the body by grounding future developments in an enactive understanding of human functioning, improving specificity by restricting factors included within the model to genuine scientific phenomena, including riskier hypotheses in the psychological and contextual domains, and utilising “pop-out” component models of clinical phenomena as a structured way to manage complexity and improve clinical utility. We hope this commentary will contribute to the continued efforts to map the PPCS landscape.
Footnotes
Acknowledgements
Thank you to Dr. Tony Ward and the two anonymous reviewers for valued feedback on earlier versions of this paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.