
Abstract
Clinical psychology is characterized by persistent disagreement about fundamental aspects of the discipline ranging from what mental disorders are to what constitutes effective treatment. Attempts to address the problem of epistemic disagreement have been frequently based on establishing the correct answer by fiat without identifying and addressing the sources of the disagreement. We argue that this strategy has not worked very well and the result is frequently ongoing and intractable disagreement, with each side in an argument convinced they are correct. In this paper, we outline an epistemic disagreement procedural model intended to assist researchers and clinicians in the field of clinical psychology to identify, explore, and develop inquiry strategies that capitalize on situations where competing knowledge claims are made. The result is a flexible conceptual framework committed to a defensible epistemic pluralism, fallibilism, and contextualism, across the various research tasks constituting the field of clinical psychology.
Keywords
Clinical psychology is an applied discipline committed to the delivery of effective methods of assessment and treatment of psychological problems by trained and competent clinicians. A pressing question concerns the best way to identify these methods: clinical authority, tradition, or systematic research? Each putative source of psychological knowledge has been endorsed at different times by groups of practitioners. In recent years a consensus about what constitutes best practice has gradually emerged in the curricula of clinical psychology programs throughout the world and is evident in the accreditation standards of professional organizations such as the American Psychological Association. In essence, the aim is to teach students how to implement treatments based on the translation of methodologically sound psychological research into clinical practice. More specifically, “evidence-based practice in psychology (EBPP) is the integration of the best available research with clinical expertise in the context of patient characteristics, culture, and preferences” (APA Presidential Task Force on Evidence-Based Practice, 2006, p. 271).
The concept of evidence-based practice (EBP) crucially depends on the production of knowledge 1 about the nature of psychological problems, their classification, causes, explanation, and treatment. Without such knowledge, it is hard to see how the symptoms of serious disorders such as major depression, schizophrenia, or posttraumatic stress disorder could be effectively managed (Krueger & Blaney, 2023). Understanding the composition and causes of symptoms enables clinicians to predict, intervene, and alter the course of a disorder in ways that either restore a person to their previous level of functioning or, at the very least, enhance their level of well-being and social functioning. Yet, putting forward knowledge claims leaves one vulnerable to the possibility of disagreement and the threat of being challenged and being wrong; facing error or ignorance head-on is what the knowledge game is all about (Ballantyne, 2019; Lougheed, 2020; Matheson, 2015). Epistemic disagreements about whether empirical claims are true or justified are frequent in clinical psychology and their persistence is recognized as undesirable given the discipline’s explanatory and therapeutic aims. 2 The trouble is that, in both research and clinical contexts, disagreement is always present and cannot be easily avoided. The interesting and important question, then, is: How can clinical psychology make progress despite widespread epistemic disagreement?
In this paper, we argue that adopting a metatheoretical perspective in the face of epistemic disagreements affords a valuable opportunity for the parties involved to deepen their understanding of psychological problems, their causes, and how best to treat them (Ballantyne, 2019; Ward et al., 2022). By epistemic disagreement, we mean situations when two or more reasonable individuals make competing knowledge claims, and at first glance appear to have access to equally good relevant epistemic considerations, and are equally competent to interpret empirical evidence or justify the reasons given. We will outline the core concept of epistemic disagreement later in the paper. As we aim to show, adopting a metatheoretical perspective allows light to be shed on the epistemic and ontological assumptions that underlie epistemic disagreements in clinical psychology. Although such disagreements frequently cannot be resolved at the local level (e.g., establishing that a specific theory is best supported by the relevant evidence), they are amenable to analysis from a more general and abstract point of view. We propose that the philosophical literature on epistemic disagreement provides resources that have the potential to move clinical psychology and psychiatry beyond pervasive and arguably fruitless disagreement (e.g., Lougheed, 2020). These resources include procedures for identifying and understanding the sources of epistemic disagreement concerning knowledge claims in a systematic way. It is important to stress that we are presenting the procedural model for resolving epistemic disagreements as only one possible way of addressing conflicting knowledge claims.
Epistemic disagreement in clinical psychology
Pervasive and ongoing disagreement between researchers concerning the nature, clinical features, causes, and treatment of different types of psychopathologies is characteristic of the field of clinical psychology, as in all sciences (Ballantyne, 2019; McCain & Kampourakis, 2020). Unfortunately, these debates occur primarily in local domains or contexts and typically fail to give rise to theoretical discussions that could provide a deeper “understanding of such arguments by making available for critical scrutiny their unacknowledged theoretical preconceptions” (Williams, 2001, p. 146). In other words, within each domain of scientific investigation we consider below, researchers are primarily preoccupied with the models and issues in that domain and confine critical remarks to their competitors rather than collaboratively engaging in an exercise to determine points of agreement and sources of disagreement in ways that may propel inquiry forward. 3 In our view, this is a mistake and may explain in part why there has been relatively little progress in the search for the causes and mechanisms constituting mental disorders or the discovery of strongly effective treatments (Hawkins-Elder & Ward, 2021a).
As illustrated in Table 1, there are a number of substantive domains in clinical psychology where disagreement occurs. These include—but are not limited to—conceptions of mental disorder, classification, theory construction, and therapeutic models. For example, there is an ongoing debate concerning the classification of mental disorders: whereas an underlying assumption of the DSM-5 is that mental disorders are real and discoverable and can be captured through a set of diagnostic criteria, others argue that they lack validity and core symptoms of psychopathology should be empirically derived to generate symptom clusters (e.g., Kotov et al., 2017). Similarly, there is substantive disagreement concerning the appropriate choice of therapy models. Given the efficacy of a diverse range of treatments with very different claims concerning the mechanisms of change (Prochaska & Norcross, 2018; Wampold, 2015), it is unclear what should guide the choice of therapeutic intervention. Similarly, there is disagreement concerning how treatment approaches should be combined or integrated (Bailey & Ogles, 2023; Norcross & Goldfried, 2018). In order to provide a bit more depth on the nature of these epistemic disagreements in clinical psychology, we focus in more detail on two areas of ongoing debate: the conception of mental disorders and theory construction strategies.
Examples of Epistemic Disagreement in Clinical Psychology.
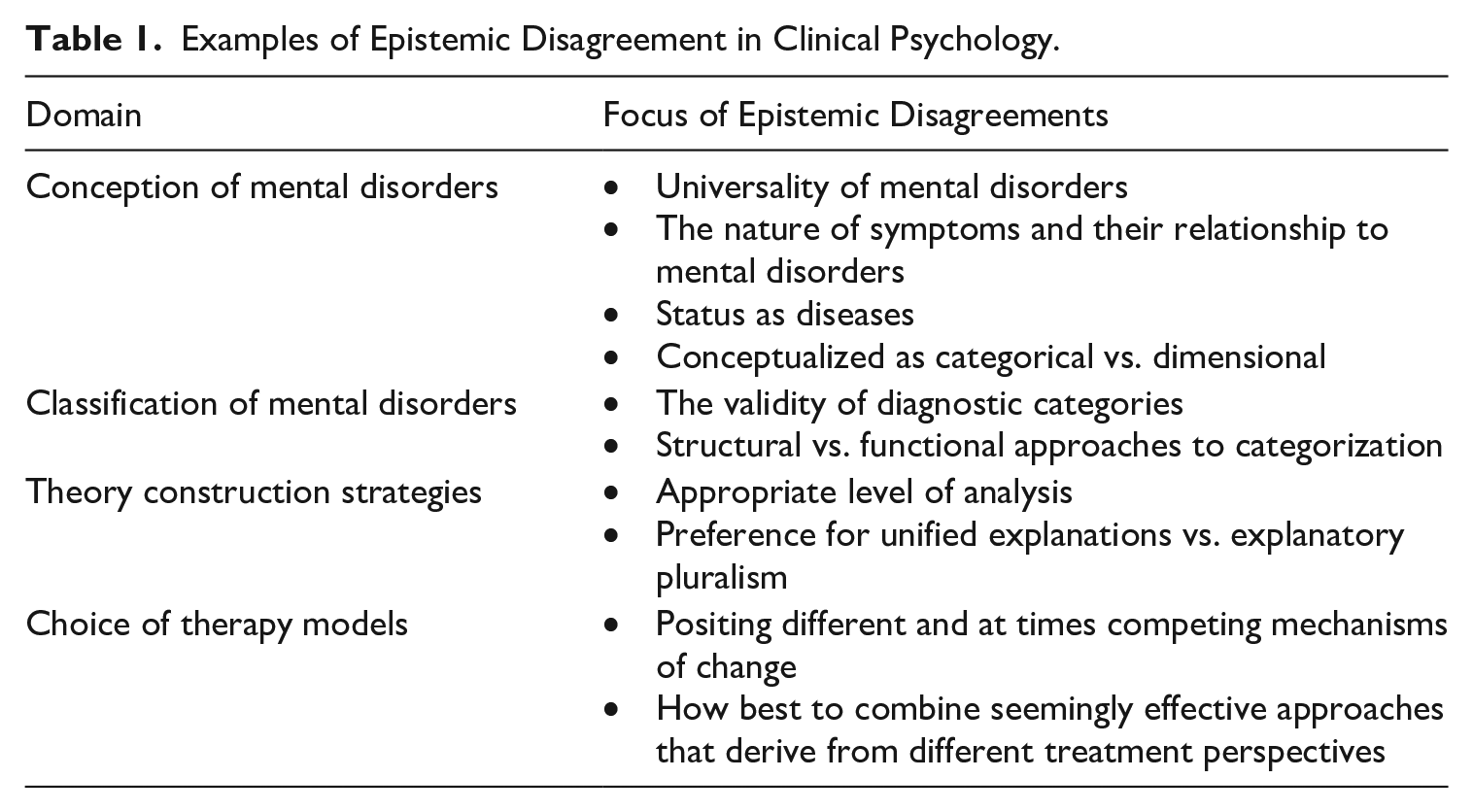
Conceptions of mental disorders
According to the DSM-5:
A mental disorder is a syndrome characterized by clinically significant disturbance in an individual’s cognition, emotion regulation, or behavior that reflects a dysfunction in the psychological, biological, or developmental processes underlying mental functioning. Mental disorders are usually associated with significant distress or disability in social, occupational, or other important activities. (American Psychiatric Association [APA], 2013, p. 20)
The implicit assumption is that mental disorders are mostly universal, their symptoms are caused by underlying dysfunctional psychological and/or biological mechanisms, and they are best understood in categorical rather than dimensional terms (Hucklenbroich, 2017; Solomon & Kendler, 2021; Zachar & Kendler, 2017). As we will demonstrate, all these knowledge claims are currently areas of vigorous dispute.
A common claim by psychopathology researchers is that many mental disorders are universal in nature and have the same underlying psychogenesis irrespective of cultural differences in clinical manifestation. For example, major mental disorders such as schizophrenia or bipolar disorder have been found in every culture that has been the subject of rigorous epidemiological research (e.g., Azis et al., 2019; Jablensky et al., 1992). By way of contrast, other researchers argue that mental disorders do not exist in any meaningful universal form, in part because the mind is hypothesized to be socially constructed and symptoms are so heavily culturally saturated that they are semantic interpretations of simple biological signals (e.g., Kirmayer et al., 2017; Marková & Berrios, 2009). This a conceptual and empirical disagreement.
A second, related area of ongoing epistemic (conceptual) disagreement concerns the nature of symptoms and their relationship to mental disorders (Wilshire et al., 2021). The DSM-5 and its supporting literature views symptoms as relatively simple, fact-like entities which are caused by dysfunctional psychological and biological systems. While there is ongoing discussion concerning the best way to classify mental disorders and how best to detect the relevant underlying psychological dysfunction, there is little debate about their relatively simple structure and their status as clinical manifestations of underlying disorders (APA, 2013; Easton et al., 2023). By way of contrast, according to the symptom network model of mental disorders developed by Borsboom et al. there is no underlying mental disorder—no latent factor—that causes individual symptoms. Rather, once a certain threshold is reached, a symptom emerges and causes the onset of other symptoms in an ongoing pathological cascade. A mental disorder is essentially a dynamic system of mutually maintaining symptoms (Borsboom, 2017; Borsboom et al., 2019).
Finally, a persistent topic of disagreement concerning the nature of mental disorders revolves around whether they are best conceptualized in categorical or dimensional terms. A common understanding of mental disorders is that they are discrete disease-like processes whose validity is centered around their etiology—or causes—and the underlying processes constituting the symptoms (Hucklenbroich, 2017; Hyman, 2010). Ideally, each distinct disorder possesses the same set of clinical features, follows a similar course, shares the same causal factors, and has distinct boundaries that distinguish them from other mental disorders (Robins & Guze, 1970). In addition, it is claimed that giving a diagnosis involves placing individuals into categories, where a person likely has the disorder or they do not. In contrast to this categorial conception of mental disorders, Lahey (2021) argues that symptoms and the disorders they cluster into exist as continuous factors, and that they are best viewed as problems rather than categorical mental diseases. He claims that this perspective is supported by empirical research into the nature of symptom presentations and allows for more effective treatment. Specifically, he states that “Psychological problems are simply aspects of behavior—broadly defined . . . to include ways of thinking, perceiving, feeling, and acting—that cause us distress. Or interfere with functioning in important areas of our lives” (Lahey, 2021, p. 1). In short, epistemic disagreement about the best way to conceptualize mental disorders is ongoing and shows no sign of abating (for a recent review, see Nielsen, 2023).
Theory construction strategies
We will now turn to disagreement over the correct way to develop and evaluate scientific theories, focusing on two areas of ongoing epistemic disagreement: arguments about the appropriate levels of analysis to adopt in explaining and treating psychological problems, and a stated preference for seeking unified explanations versus explanatory pluralism.
Theories are formulated in a variety of scientific disciplines to explain the occurrence of specific states and outcomes, such as diseases, mental disorders, chemical reactions, and species evolution and survival. Theories vary in their form but in essence are conceptual structures developed to explain why certain phenomena exist and persist or behave as they do. In the sciences, sometimes these explanations are mechanistic in nature (i.e., they seek to decompose systems into their various components and processes to grasp how they work) and at times they are formulated in the language of agency and intentions (i.e., identifying the reasons why a person acted as they did). 4 For example, from a mechanistic viewpoint, theories of disease in medicine attempt to discover the impact of an etiological agent (e.g., exposure to a toxin) on the production of a suite of symptoms through the operation of underlying causal mechanisms (i.e., pathogenesis; Kendler et al., 2011). Alternatively, an interpretative, meaning-centered explanation of depression might inquire into the way individuals make sense of adverse experiences and look for alterations in core beliefs or attitudes (Beck, 2008). Or again, an explanation pitched at the genetic, molecular, or neurological level of explanation could be preferred. For example, molecular models of anhedonia, a core symptom of depression, largely focus on the role of dopamine due to the large body of evidence indicating its importance in the brain’s reward system (e.g., Wise, 2008). In the area of psychopathology there is little agreement on the nature of the causal mechanisms generating mental disorders and on which level of analysis, if any, should be regarded as the primary one.
A related issue is the degree to which researchers seek integrative as opposed to pluralistic explanations of psychological problems. An example of integrative interlevel theoretical work is Kendler et al.’s (2006) model of the etiology of major depressive disorder (MDD). Based on an extensive examination of data from multiple levels of human functioning, Kendler et al. (2006) hypothesized that MDD is a complex disorder that is the outcome of several causal factors from different levels or domains interacting over time. The major causal factors included developmental adversity (e.g., early loss, childhood sexual abuse, and low parental warmth), genetic vulnerability (e.g., temperament, serotonin-functioning defects), and psychological variables such as low self-esteem. All these factors are required to explain and predict depression, and understandings across different levels of human functioning are all understood to have explanatory utility.
By way of contrast, epistemic pluralism is a theory creation strategy that endorses the creation of multiple, distinct models of phenomena (or their causes), accepting that each has a unique explanatory focus (Hochstein, 2016). For example, Hawkins-Elder and Ward (2021b) propose that the prevailing approach to theory construction in psychological science is problematic because of the quest for what they call “the one best model.” In their view, this is a forlorn hope because modelling requires both (a) idealization, where there is a deliberate distortion of certain parameters of the target system (e.g., assuming perfectly rational actors, which is strictly incorrect), and (b) simplification, leaving out nonsalient features of a phenomenon for modelling purposes (e.g., ignoring anxiety symptoms when modeling psychosis). Thus, for explanatory purposes, the aim is to create a network of loosely allied models:
In our view, the [one best model] perspective should be set aside in favor of a more collaborative and pluralistic approach. Model pluralism involves the representation of target phenomena (e.g., specific mental disorders) by a collection of models at different scales and levels of analysis that together form an overarching explanation or “explanatory network.” (Hawkins-Elder & Ward, 2021b, p. 830)
From the perspective of epistemic pluralism, it is a scientific mistake to seek to create integrated or unified theories as encouraged by researchers such as Kendler (2008) and Thomas and Sharp (2019)—one that is likely to result in wasted efforts. The argument is that successful truly unified models are rare (or some would say nonexistent), mainly because of the epistemological challenges of building accurate models of phenomena in a complex, messy world. Furthermore, it is argued that scientists typically use models as heuristic devices to explore data patterns in order to identity phenomena and do not view them as representations of a preexisting reality (Massimi, 2022). According to this perspective, it makes sense to create a number of competing or complementary models when investigating patterns in the world. Wherever researchers are positioned with respect to this debate, it is apparent that there is ongoing disagreement about the epistemological, methodological, and metaphysical aspects of natural and social phenomena such as mental disorders, and how best to understand and explain them (Wilkinson, 2023).
Implications
There are a number of areas in clinical psychology in which there are currently competing conceptual and empirical knowledge claims. These disagreements are pervasive, persistent, and unresolved. Despite such ubiquitous epistemic disagreement within the knowledge base and practices of psychopathological science, evidence-based practice is an accepted requirement for most modern clinical psychology training programs and accreditation bodies. A key issue concerns how this requirement may be satisfied. If evidence-based practice is, as the name suggests, based on evidence, yet rival knowledge claims have not been subjected to critical scrutiny, then on what basis does one adjudicate between or among them?
Ongoing knowledge conflicts in clinical psychology at every phase of inquiry thus create difficulties for researchers and leave them pondering the following question: How do we know what is true or justified? The major challenges facing clinical practitioners concern the trustworthiness of their theoretical models of mental disorders as well as of their assessment and treatment protocols. In other words, what can clinicians really count on as psychological knowledge? Finally, a pressing issue for students of clinical psychology is knowing what knowledge is worth acquiring and what can safely be ignored: What should we learn? In each case, what is needed is a systematic way of addressing disagreement that can lead to reasonable decisions about what attitude to take with respect to competing knowledge claims: Change your mind, stand fast to your position, or withhold judgment.
On the other hand, as stated in the beginning of this paper, disagreement is a crucial engine of scientific progress, and the existence of competing conceptual analyses or models can result in a deeper and more accurate understanding of the world (Kornblith, 2021; McCain & Kampourakis, 2020). The problem is that the way epistemic disagreement is currently dealt with in psychology tends to be characterized by biased thinking and often partisan debates where opponents talk past each other or simply change the subject. The development of a method that cuts across what are thought to be distinct disputes and provides a way to frame these local problems as ones of more general epistemic disagreement while capitalizing on the dynamic and often constructive nature of intellectual conflict is arguably needed. A second-order method for identifying and systematically responding to conflicting knowledge claims can provide a constructive way of addressing such disagreements; one that neither retreats into intellectual silos and ignores alternative perspectives nor dismisses its scientific competitors out of hand. In what follows, we first outline the nature of epistemic disagreement and introduce some key concepts. We then introduce an epistemic disagreement model that can assist researchers and practitioners in clinical psychology to address situations in which competing knowledge claims are made.
Epistemic disagreement
Epistemic disagreement, 5 as we are understanding it here, occurs when two or more reasonable individuals make competing knowledge claims and at first glance appear to have access to equally good relevant epistemic considerations and are equally competent to interpret evidence or justify the reasons given (Matheson, 2015). For the purposes of this paper, we have replaced the concept of evidence with the less restrictive term “relevant epistemic considerations.” This makes it easier to employ different types of argument structures and evidence in research and clinical reasoning. Evidence in this broader sense also encompasses conceptual analysis and theoretical reasoning that is employed to justify a set of hypotheses or claims. We do not include ethical claims in our definition but note that some theorists argue ethical claims are also knowledge claims (see Zimmerman et al., 2018).
The difficulty for a knowledge seeker is that something cannot be both true/justified and false/unjustified at the same time; someone or something must give way. 6 The disagreement itself could take slightly different forms: (a) one individual asserts p (e.g., autism is a mental disorder) while another denies the truth of p (not-p: autism is not a mental disorder ) or (b) the dissenting person asserts q which by implication entails the falsehood of p (autism is simply a normal variation of psychological traits; it is a question of neurodiversity).
In the philosophical literature, we encounter different ways of conceptualizing epistemic disagreements at a theoretical level that offer analytic tools by which to evaluate current debates in clinical psychology. We are particularly sympathetic to accounts that recognize that (a) challenges to knowledge claims are issued and subject to challenges in specific contexts and one’s informational situation across contexts is subject to change (contextualism), (b) knowledge claims that survive challenges may later be subject to revision in light of new evidence (fallibilism), and (c) knowledge claims that have been subject to critical scrutiny from a variety of different perspectives have a greater probability of being on firmer epistemic footing than those that have not.
Williams (2001), for example, provides a contextualist picture of knowledge and epistemic justification that is in the spirit of the kind of theoretical work we believe could ground effective strategies for responding to epistemic disagreements in clinical psychology. Approaching epistemic debates from this theoretical perspective, Williams emphasizes that within contexts in which one individual issues a knowledge claim and another individual challenges it, five main factors are at play. First, it is important to recognize that two people engaged in a debate allow each other certain default entitlements that cannot be called into question. They take each other’s rationality, access to, and experience of the world for granted (i.e., intelligibility or semantic constraints), and without this starting point, the debate could not get off the ground. Second, there are methodological constraints that shape the direction of inquiry insofar as some claims are simply not up for grabs. For example, the parties involved do not push inquiry to the point of questioning their own existences or whether they are both on Earth. Third, there are also dialectical constraints; certain claims may at first enjoy default status but later be subject to critical scrutiny depending upon how the disagreement unfolds. Fourth, there are costs and benefits to engaging in epistemic disagreements; so-called “economic constraints.” There may be limited time to invest in resolving a disagreement and the disputants opt for efficiency. Alternatively, if their aim is error reduction, they may decide to invest considerable time in coming to a resolution. Finally, knowledge claims are always issued in specific contexts in time and space and situational factors external to the epistemic agents engaged in debate dictate whether the evidence put forward in support of a given knowledge claim constitutes adequate grounds. Williams indicates that whereas the first four constraints—intelligibility/semantic, methodological, dialectical, and economic—all have to do with individual agents being epistemically responsible (i.e., internal factors), situational constraints are external and beyond their control, though equally as important to evaluating the outcome of the debate. Thus, even within different epistemological perspectives there can be norms held in common.
While Williams (2001) offers beneficial metatheoretical resources for understanding some of the general dynamics of epistemic disagreement, other authors have sought to understand the contours of specific types of epistemic disagreements. This work is important for our aims in this paper. For example, Lougheed (2020) asks us to consider the following scenario:
Suppose that after an agent comes to believe proposition P she finds out that there is an epistemic peer—someone of equal intelligence and ability—who has evaluated the same body of evidence and come to believe not-P. What should her reaction be upon discovering peer disagreement? Does the existence of peer disagreement constitute a (partial) defeater to her original belief that P? Or is she rationally permitted to maintain her belief that P even in the face of peer disagreement? (p. 3)
There are several ideas in this quote that we want to clarify, synthesize with the conceptual tools put forward by Williams (2001), and adapt as a basis for developing a model aimed at helping psychopathology researchers and clinicians 7 navigate epistemic disagreements more fruitfully and effectively.
Epistemic peers
As Lougheed (2020) explains, epistemic peers are persons of equal intelligence and ability, who may, in some cases, arrive at opposite conclusions when faced with the very same body of relevant epistemic considerations. Epistemic disagreements in which two or more individuals have access to the equally good relevant epistemic considerations and possess roughly the same level of expertise to evaluate them can and do occur in clinical psychology. For example, psychotherapy researchers might have access to the same set of studies on the effectiveness of CBT for personality disorders—and have the same level of relevant competence—but disagree over what the mechanisms of change are; in part, this is a conceptual disagreement.
Epistemic action
In such cases of epistemic disagreement, as Lougheed (2020) indicates, one is faced with the question of how to react. If a peer rejects a belief that you hold, should you maintain your belief, subject it to further scrutiny given this fact, or reject it? For example, if you are a psychotherapy researcher who believes that CBT works by changing maladaptive core beliefs but one of your peers disagrees and argues that it works by exposure mechanisms, this situation affords an occasion to engage in the kind of theoretical reflection Williams (2001) encourages, before determining an appropriate course of action. Does the disagreement concern the quality of the evidence concerning the change mechanism or problems with the theoretical assumptions? Are different standards of evaluation being applied? For example, if a researcher is an expert in quantitative statistical methods in psychopathology research but ignorant about qualitative methods, they will not be as competent to evaluate knowledge claims about possible change mechanisms based entirely on a qualitative method such as discourse analysis as someone with that specific expertise. The aim of such reflection is to get clear on each other’s theoretical presuppositions and their potential sources in order to locate the source of the disagreement. Engaging in such reflection will inform which course of action to take in response to the disagreement: (a) Should you stick to your original claim, (b) change your mind, (c) suspend belief, or (d) engage in further evidence gathering and/or conceptual evaluation before you decide on the best course of action? Episodes of epistemic disagreement are dynamic, and positions may change over time in response to new information, but given constraints of time and resources, an individual must choose one of these four options.
Epistemically weaker and stronger positions
In some cases of epistemic disagreement (e.g., the CBT case above) where another researcher does not have access to equally good relevant epistemic considerations (e.g., bodies of evidence), or possesses other sets of evidence or reasons that are equally relevant, and/or lacks the same level of competence as you to adequately assess the relevant epistemic considerations (e.g., empirical evidence concerning a propositions truth), they are in an epistemically weaker position. That is, their claims are not as well supported as yours. In this situation, it would be reasonable for you to reject their set of knowledge claims and stick with your original claim. An example of this would be if your argument for the claim that CBT works by the modification of thinking processes and core beliefs is better justified than a claim by a Gestalt researcher that it works by emotional disclosure. In this case, they would be in a weaker position, and therefore it would be reasonable for you to remain steadfast. An epistemically stronger position is the reverse of this situation. The individuals or groups who disagree with you about the truth of a belief (or model) have better access to the relevant epistemic considerations and/or possess superior competencies than you with which to adequately assess the evidence and reasons. In this situation, the rational action would be to reject your own knowledge claim.
Epistemic defeaters
These are reasons to reject previously accepted knowledge claims because they undermine or rebut some aspect of your argument. That is, they may indicate that (a) the ideas guiding the relevant research studies are problematic in some respect, (b) methods used to collect and analyze evidence are unreliable, and (c) competence required to interpret and present theory and evidence is missing (Ballantyne, 2019). Examples of common defeaters include researcher bias, counterfactual interlocuters (logical possibilities you had not considered and should have—for example, who has gotten to play a role in the gathering/constructing of “evidence”?), unpossessed evidence (relevant evidence you have unjustifiably overlooked), requisite expertise (do you have the required competence to perform or interpret the research or are you a relative novice?), and epistemic trespassing (where an expert on one domain of science makes knowledge claims in an area in which they are novices). Defeaters can be partial or complete in nature.
Epistemic election
The final core concept we would like to clarify is that of an epistemic election. This is a metaphor for the process of evaluating the quality of the evidence and theory underlying competing knowledge claims and reaching a decision about what stance you should adopt with respect to the disagreement. For example, stick with your knowledge claim, change your views, suspend belief, or refuse to take a position until you have instigated some kind of additional critical inquiry process. This might include searching for or gathering additional evidence, exploring other possible positions (i.e., knowledge claims), evaluating theory, reanalyzing data, reaching out to experts to consult, and so on. As de Cruz and de Smedt (2013) argued in their analysis of epistemic disagreement over the taxonomic status of Homo floresiensis, peer disagreement can promote the active searching for additional evidence, sources of bias, and re-evaluation of existing evidence. Once you are satisfied you have enough evidence (or better theory) and the necessary competence to decide on a course of action, a winner, loser, or a tie is announced. It is important to stress that not everyone gets a “vote” in deciding what position is stronger and so on. In science, as in most domains of knowledge, there are explicit and implicit criteria outlining what level of expertise is required to participate in the process (possessing a PhD, having relevant training, adhering to certain methodological standards, etc.), and what norms are relevant when making decisions about the epistemic merits of each set of knowledge claims.
Epistemic disagreement model
Recapping our argument so far, clinical psychological science is characterized by persistent disagreement concerning the nature of mental disorders (or if you prefer, psychological problems), their classification, explanation, and treatment. These disagreements center on two key areas: (a) conflicting theoretical claims and (b) disputes about the quality of evidence and reliability of methods producing this evidence. To date, efforts to resolve these disagreements have typically focused on the specific assertions being made within a scientific perspective and researchers have not engaged with second-order questions such as how competing knowledge claims should in general be addressed. One advantage in formulating epistemic disagreement at an abstract and general level is that it cuts across disputes within different domains and offers a set of conceptual tools to refine and direct the process of responding to disagreement. We propose that ideas from the philosophical literature regarding epistemic disagreement can be recruited to complement current strategies for managing entrenched disagreement. It is important to stress that we do not see them as replacements for clinical psychology’s existing epistemological and methodological tools but rather as additional cognitive resources. We will now outline a procedural model based on ideas from the epistemic disagreement literature and recent work on the evidence-based practice model (Ward et al., 2022). 8
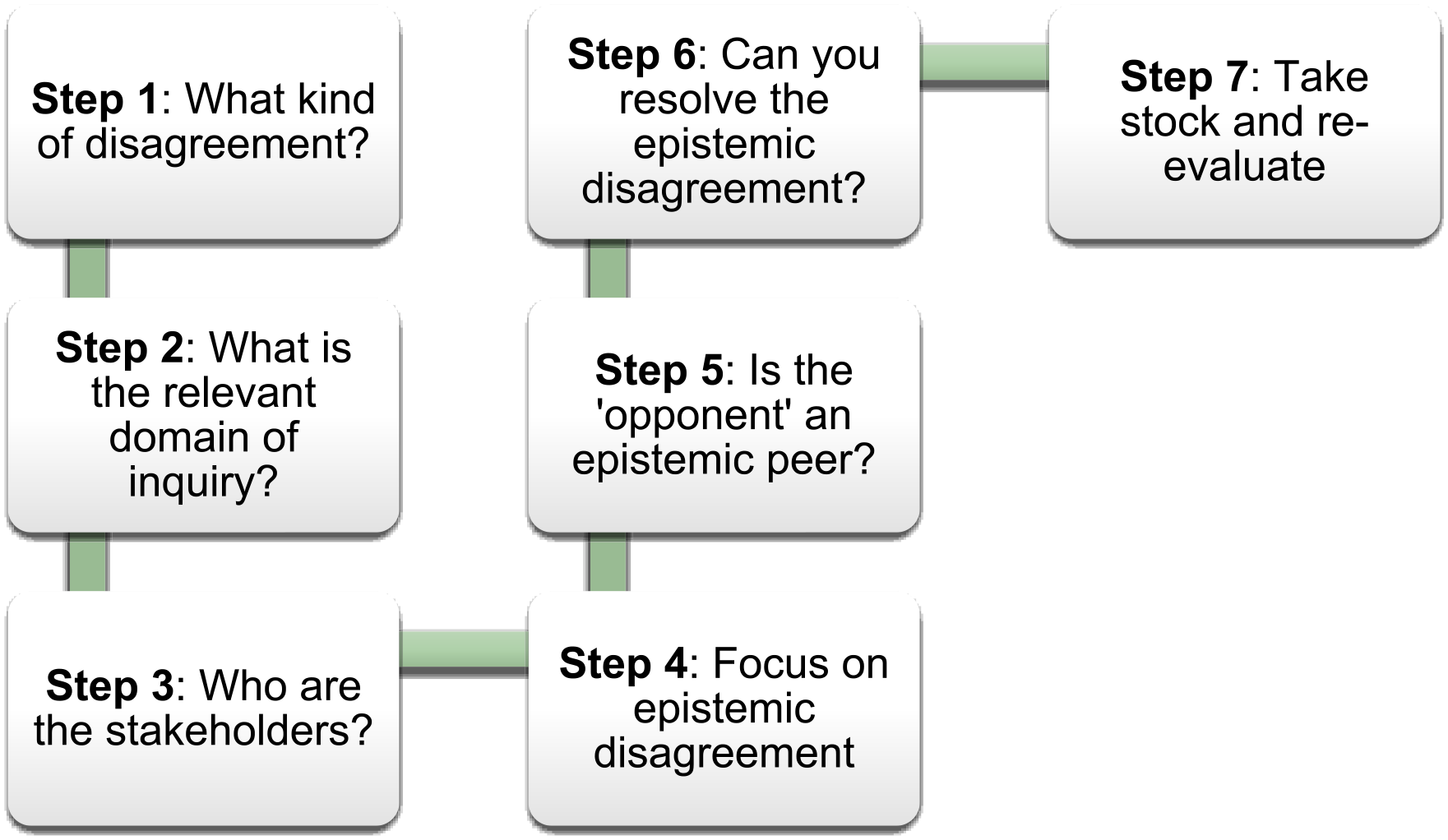
There are seven steps in the epistemic disagreement model, each conceptually dependent on the one prior to it (see Figure 1). We have chosen to present the key decisions at each step as they relate to an epistemic agent rather than in a more impersonal manner. The reason for this is that, in our view, science consists in a set of interlinked practices and is always historically and culturally situated within a specific community, comprised of researchers and a set of social, material, and cognitive resources (Massimi, 2022). Therefore, it makes more sense to stress the role of researchers’ epistemic responsibilities (which is also articulated in Williams’ 2001 framework) rather than speak in a detached way about theories, models, justification, and so on. An important point to stress is that we assume that researchers involved in a dispute concerning competing knowledge claims share a set of basic assumptions (e.g., what constitutes evidence, criteria for evaluating knowledge claims, etc.) about the domain in question which make it possible for them to engage in reasonable dialogue.
Phases of the epistemic disagreement model.
Step 1: What kind of disagreement is at stake?
The first step is to discern whether or not the apparent disagreement is real or merely a misunderstanding where researchers are speaking at cross purposes. For example, it is arguable that functional approaches to classifying mental disorders are not necessarily in competition and can coexist quite comfortably with structural models such as the DSM-5. In part, this is because they are focusing on different tasks, that is, description of symptom patterns (DSM-5) versus explanation of problems by referring to goals and maladaptive behavioral strategies for achieving them. Once the nature and sources of the disagreement have been formulated, the nature and level of conflict will become more evident. Identifying cases of epistemic conflict is sometimes easy; for example, when there is a dispute between research groups in the literature or in research forums, such as conferences. Otherwise, we propose that the existence of disagreement should be assumed and that researchers look at the possible defeaters for clues; for example, considering counterfactual scenarios, checking unpossessed evidence, and scrutinizing work for cognitive and motivational biases.
Following a decision that the disagreement is real, it is crucial to formulate it in concrete terms and to clarify exactly what kind of disagreement it is. A significant decision is whether the disagreement is an epistemic one in which knowledge claims about some aspect of psychopathology and its treatment directly conflict (i.e., p versus not-p); for example, whether CBT exerts its therapeutic effects by modifying problematic core schema or by encouraging exposure to feared situations. It is important to distinguish knowledge claims from ethical, political, and spiritual claims; for example, that it is always wrong for clinicians to physically but nonsexually comfort their clients (e.g., to place a hand on their shoulder) versus the idea that such actions are sometimes acceptable in unique circumstances and do not necessarily breech professional boundaries. Epistemic and nonepistemic disagreements rely on different argument structures and have different aims. In the case of scientific claims, the goal is to explain something causally while normative arguments are intended to persuade individuals to act differently (Walton, 2008), although we note that some theorists argue that ethical or social normative claims are epistemic in nature (see Zimmerman et al., 2018). Currently, our procedural model does not address these important types of disagreement.
Step 2: What is the epistemic task?
If it is decided that the disagreement is an epistemic one, then the next step is to identify the domain of inquiry and associated task. There are a variety of distinct tasks in clinical research, each requiring the utilization of different types of knowledge. These tasks include risk prediction, problem detection, classification, compositional explanation (i.e., providing a rich description of a symptom at different levels of analysis), causal explanation, evaluating therapeutic effectiveness, maintenance of treatment gains, and ongoing risk management. The relevant epistemic considerations for these tasks will vary and range from the evaluation of statistical evidence and models, to the appraisal of theoretical claims. For example, the knowledge required for risk prediction will include nominating a distinct outcome variable such as hospital readmission, psychometric criteria for constructing good risk measures including reliability and validity norms, and normative data gathered on relevant client populations. As another example, relevant methods for clinical phenomena (symptom) detection will include use of multiple data sources, statistical techniques for identifying patterns in data, and background knowledge of psychopathology symptoms and disorders. Failure to identify the task clearly may result in researchers arguing at cross purposes.
Step 3: Who are the stakeholders within the context of psychological inquiry?
It is important to locate and identify the key stakeholders in the disagreement. Is the disagreement between researchers who have the same general scientific perspective or is it between researchers from different epistemic communities who hold sharply conflicting views? The latter may include researchers working within an indigenous knowledge tradition, who have quite different assumptions about the composition of the mind and its relationship to the natural world. A related question concerns the subjects of the investigation: What are the relevant and critical demographic features that should be considered when seeking to understand the specific details of the disagreement? This will include ethnic, cultural, gender, class, sexual, social, and relevant psychological factors such as the presence of cognitive or physical disabilities. Each of these factors may result in different epistemic perspectives on mental health issues. Describing the salient features of key stakeholders provides a frame within which the contrasting knowledge claims can be understood. For example, appreciating that certain cultural groups believe it is possible to converse with beings from other dimensions may cast a different light on what is considered to be psychotic versus spiritual phenomena.
Step 4: Focus on epistemic psychological disagreement: p versus not-p
Once it is clear that the disagreement is an epistemic one, the next step is to formulate more precisely what the disagreement is about. Is it about a specific symptom such as anhedonia, a mental disorder like major depression, an explanatory model, quality of evidence, methods for generating evidence, or treatment effectiveness? Sometimes at this point it becomes obvious that the disagreement was only apparent, and the procedural model can be exited. For example, two sets of researchers may disagree about the essential properties of anhedonia and then come to the realization that they are focusing on different levels of analysis and therefore do not really disagree; they are simply talking about different aspects of the phenomenon of anhedonia (see Wilshire et al., 2021).
Once it is apparent that there is a genuine (p versus not-p) 9 disagreement, the researcher needs to clearly state their reasons for the relevant knowledge claim and consider possible defeaters. This will include evaluating the quality of first order evidence and methods, and taking a critical look at the underlying epistemic norms that support their claims. It is crucial to clearly state the competing knowledge claims (going through the same process above) that are in opposition to their own. The researcher should actively search for “the other view or model,” accepting that there will always be competing viewpoints from within and beyond their epistemic community. Other considerations include identifying the depth of the disagreement (is it about core assumptions?) and whether a phenomenon is truly a psychopathological one or belongs to another type altogether. For example, what appears to be depressed mood could be more accurately described as sadness.
Step 5: Is the person or group making conflicting knowledge claims an epistemic peer?
Once a researcher’s own knowledge claim and the reasons supporting it have been precisely formulated, the next step is to inquire whether the researcher making a claim that conflicts with theirs is an epistemic peer. There are a number of important considerations that accompany this decision: What additional resources or information are required to make this judgment? Is their access to the relevant evidence, theories, training, and cognitive skills roughly the same as mine? If so, should they be granted epistemic equivalence status? If not, why not? It is essential to employ a principle of epistemic charity and grant peer status if in doubt. This is to offset the obvious problem of researcher bias and to accept that a diversity of views from qualified decision-makers is likely to improve the quality of a research decision (Ballantyne, 2019). If the competing claim comes from an epistemic community with significantly different norms and ontological assumptions, then the researcher should consult someone who possesses expertise in both traditions. An example would be disagreement about the causes of psychosis between researchers with different methodological expertise such as qualitative versus quantitative methods. The researcher with a preference for employing qualitative methods to explore patients’ experiences of psychosis could favor first-person accounts over biomarkers such as fMRI-generated data. Both have access to different but arguably equally good evidence. However, it should be noted that there can be contrasting epistemic norms concerning what constitutes good evidence. For example, a psychodynamic researcher may consider within-session therapist observations solid evidence while another researcher views it as biased. In this example they should look for guidance from individuals who have training in both sets of methods and look for common epistemic norms relating to establishing the reliability and validity of knowledge claims. Sometimes agreement may not be possible, but a good faith effort should be made. Another example is when adjudicating knowledge claims between therapeutic models—researchers should consult an expert from the competing methodology to make sure they have fully grasped the nature of the methods utilized, theoretical assumptions, quality of the evidence, analyses, and treatment techniques.
Step 6: Can the epistemic psychological disagreement be resolved?
In the next step, the researcher actively seeks to resolve the problem of epistemic disagreement. If the opposing researchers are granted the status of peers, they inquire into what epistemic norms they hold in common (e.g., regarding evidence, reasons, methods) which could help to clarify which is the correct claim(s). This will involve consulting Williams’ (2001, see above) five types of constraints: default entitlements, methodological, dialectical, economic, and external. If the opposing researcher is judged to be in a weaker position, then—just to be sure—the researcher should still reevaluate the evidence and reasons for their claims. This process will involve searching for defeaters they had not considered, such as unacknowledged evidence, bias, possible ideas not considered, or lack of competence. However, if following the reevaluation of reasons for making their knowledge claim the researcher remains confident that their position is stronger, they should reject the competing position. By way of contrast, if they decide the competing claim is stronger, they should revise or reject their claim, and make any revisions believed to be necessary to their model. In this scenario, the decision is to accept the opposing knowledge claim.
In science it is important to consider the pros and cons of each knowledge claim at the time the dispute is being addressed (synchronic) and in the longer term (diachronic). With respect to the latter evaluation process, a key issue is which claim in the long run is likely to be a stronger option (Lougheed, 2020). The epistemic criteria for appraising the merits and weaknesses of the various options will depend on the task that is the focus of disagreement. For example, theory appraisal criteria such as fertility, explanatory depth, simplicity, coherence, external consistency, and consilience should be applied when the research task is an explanatory one (Haig, 2014).
Importantly, if there is room for reasonable doubt concerning the epistemic status of the opposing knowledge claim, then research guided by both claims and their respective scientific perspectives should be encouraged to proceed in parallel. Epistemic pluralism makes sense in the short term at least, as it often takes considerable time for the strongest scientific position to emerge (Chang, 2022). It is a mistake to prematurely shut down competing options. In such a case, the researcher should suspend judgment about whether their belief is correct and engage in a search for additional evidence and/or better models to guide and interpret evidence. That is, the decision is to suspend the endorsement of either knowledge claim and to state that it is unclear whether p or not-p is correct.
It is important to factor in the cost of being incorrect in addressing epistemic disagreement. For example, in a situation of genuine disagreement between epistemic peers, one knowledge claim might lead to outcomes that cause less harm than another even though they both may be wrong (or right).
Step 7: Take stock and reevaluate as necessary
The final step involves the researcher at a later point taking a second look at the epistemic situation and asking whether any relevant new evidence or reason has emerged that weakens or strengthens the justification for their previous knowledge claim. For example, there may have been advances in technology that provide access to entirely new bodies of evidence or there may be better statistical methods available for collecting and analyzing evidence. Alternatively, a researcher might have increased their level of competence by acquiring knowledge of new techniques that provide a reasonable basis to revisit their earlier decision. The whole point of this step is to remind researchers that the acquisition of knowledge is a dynamic and evolving process and there is no end point to the process. Scientific perspectives provide windows to explore the world that over time result in improved understanding of clinical phenomena and their relationship with each other (see Massimi, 2022). For example, contemporary research into the core features of schizophrenia has found that what were once considered to be unique symptoms of schizophrenia such as auditory hallucinations and paranoid delusions are commonly found in other mental disorders like bipolar disorders and depression (Kring & Smith, 2021). The earlier knowledge claim that hallucinations and paranoid delusions were specific to schizophrenia initially “won” out over the competing claim that it was not. This is because the evidence and supporting reasons for this belief were judged to be stronger at that time. However, with the advance of classification technologies and statistical methods this judgment was reversed.
Brief example
It would help to demonstrate the utility of the epistemic procedural model by presenting a historical example where researchers held competing views and, through the application of the epistemic disagreement model, arrived at a resolution that both sides were happy with. Unfortunately, given the newness of our model, this is not possible. A brief example of one ongoing dispute over the most valid way of classifying mental disorders provides some indication of how this process could unfold.
Clinical phenomena can be classified in different ways, depending on the goals and theoretical allegiances of researchers. Thus, for example, classification can be based on structural aspects of disorders such as in signs and symptoms or in terms of their functional impacts, such as an inability to meet specific types of need. The DSM-5 is a structural model because disorders are operationalized in terms of lists of symptoms and a specified time frame in which they have been present. Critics of the DSM have argued that its symptoms are often nonspecific and shared across different disorders (e.g., depression and anxiety; schizophrenia and bipolar disorder) and there is a problem of disorder heterogeneity: there are hundreds of ways one can meet some diagnostic criteria (Lilienfeld & Treadway, 2016). An alternative approach to classifying mental disorders turns from a focus on lists of symptoms to motivational systems (goal directed behavior). According to Del Giudice (2018):
motivational systems set the goals of behavior and monitor causes of success and failure in the pursuit of those goals. Motivational systems affect behavior indirectly by triggering emotions, which in turn coordinate adaptive suites of physiological, cognitive, and behavioral response. (p. 37)
The use of the epistemic disagreement model would reveal that there is no fundamental conflict between the two approaches because they provide different information and serve quite different roles in research and practice. The DSM-5 is useful for highlighting clusters of related symptoms, while a functional approach based on core needs and goals more clearly specifies the relationship between persons and their environment and the degree to which important needs have been blocked by both environmental and psychological constraints. The epistemic dispute could be resolved at phases two or three once researchers realize that they have different foci of inquiry.
Conclusions
A default assumption of the epistemic disagreement model outlined in this paper is that reasonable competing knowledge claims are always present, even if they go unnoticed. The presented model helps to pinpoint these loci of disagreement and creates options for resolution. By doing so it avoids fruitless disputes where researchers are speaking at cross purposes and therefore inquiry has become bogged down and valuable resources are being misdirected and wasted. A related point is that the epistemic disagreement model keeps researchers and clinicians humble as it encourages them to assume initially that those with whom you disagree are likely to be epistemic peers. Therefore, researchers need to work hard to reject a competing knowledge claim rather than the reverse being the case.
Researchers employing the epistemic procedural model outlined in this paper are less likely to overlook the potential value of marginalized psychological models. For example, with respect to cultural models of psychological problems, we argue that framing disagreement between indigenous researchers and traditional science as cultural in nature is a mistake. It implies that science is not itself a cultural product and that non-Western cultures do not have a cognitive system like science—or other rigorous empirical inquiry traditions/institutions. Neither assertion is true in our view (see Gaukroger, 2020). In comparing knowledge claims from different traditions or cultures, it is essential to ask: What kind of knowledge is best suited to address this problem? The source of the knowledge is not as relevant. Rather the question should be: Does this model provide the best explanation we have, according to our preferred epistemic tools and evaluative criteria (or does it best address the task in question)? This way of thinking about knowledge application will help researchers and clinicians to avoid the trap of thinking that one set of knowledge claims can explain any problem in any domain and that models from other cultures (sources) should be automatically disqualified from consideration.
From a critical perspective, there are three obvious criticisms of our approach. The first is that the epistemic disagreement model is too complex and will be difficult for psychopathology researchers to use. In response, we doubt if this is the case. Scientists routinely utilize a range of complex, specialized techniques to formulate and evaluate models and analytical methods. Searching for alternative viewpoints in the different phases of inquiry is likely to reduce the chances of prematurely rejecting nonmainstream perspectives, thereby conserving rather than wasting precious cognitive resources. Second, it could be argued that what matters for scientific progress is diversity at a scientific institutional level not openness to alternative perspectives at the level of the epistemic agent, whether that is a research group or individual scientist. Thus, it does not really matter if specific research groups are inflexible and dogmatic as long as there is critical exchange at the broader institutional level. By way of reply, research on decision-making suggests that including individuals with diverse views within a group is likely to improve its overall problem-solving ability beyond that of simply having groups with diverse views (Ballantyne & Dunning, 2022). There is no reason to believe that this finding is not applicable to researchers. In addition, we think the well-documented cognitive and motivational biases evident in human beings provide a good reason to give researchers the skills to offset them as much as possible (Howard, 2019). Third, researchers could complain that there is little new in our approach and that everything we propose is already integral to their practice. Certainly, the idea of seeking to falsify hypotheses is a central part of scientific investigation, and that is a feature of the epistemic disagreement model. However, our focus goes beyond the testing of hypotheses, and encompasses the full array of tasks evident in scientific practice. In addition, the epistemic disagreement model provides a general method for dealing with disagreement across different scientific perspectives, and in this respect is novel.
In conclusion, science thrives on intellectual competition and critical exchanges between research groups. Part of the critical culture of science is the willingness to take risks and be prepared to fail. As Popper argued a long time ago, bold conjectures and attempts to refute them have the potential to light up problem areas and reveal solutions to problems no one had previously thought of (Popper, 1963/2002). Set against the willingness to take epistemic risks is the human tendency to stay within current understandings and to resist the revision of beliefs (Ballantyne & Dunning, 2022). A combination of motivational and cognitive biases can blind researchers to other possibilities and result in a stubborn adherence to cherished theories. The result of these biases can be ongoing and intractable disagreement, with each side in an argument convinced they are correct. While scientific methods and institutions can mitigate this rigidity to some degree, they are imperfect. The fact that epistemic disagreement in clinical psychology is pervasive and often counterproductive suggests it might be time to consider additional options. In our view, the epistemic disagreement procedural model outlined in this paper offers another way of building cognitive diversity into psychological science while avoiding fruitless partisan conflict.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.