
Abstract
Introductory psychology courses have a broad reach; their textbooks are instrumental in disseminating information about mental distress. In this study, we present the theoretical implications of a Foucauldian discourse analysis of constructions of schizophrenia in six introductory psychology textbooks assigned in Aotearoa/New Zealand and Australia. We identify three interconnected discursive constructions within the textbooks: object-for-study, social problem, and unrecoverable illness. These constructions converge to position people with a diagnosis of schizophrenia (PWDS) as sites for biomedical intervention and generate biomedical treatment as necessary but non-curative. Notably, the voices of PWDS are absent from the texts. We contend that amplifying counter discourses and the voices of PWDS is essential to provide the context, meaning, and hope that is missing from these textbooks, and broader society. We work with Mad Studies to present potential ways of theorising otherwise around these experiences—and leveraging this theory in textbook writing.
Keywords
Introductory psychology (IP) courses, the most widely taught courses in the discipline (Griggs, 2014), are typically students’ first engagement with the field of psychology (Ferguson et al., 2018). They can play a significant role in shaping the values and attitudes of students, who often find the content relevant to their lives and influential on their views of social issues (Whitbourne & Hulicka, 1990). Students studying various subjects (law, business, medicine, etc.) may take IP courses as electives, increasing the reach of these courses (Warne et al., 2018). Such courses are commonly structured around psychiatric diagnoses (Harper et al., 2007) and teaching staff often “teach the textbook” (Griggs & Bates, 2014).
Textbooks are not neutral purveyors of knowledge; they (re)produce certain (usually “mainstream” or dominant) versions of the world, shaping the knowledge and values of readers (Thoma, 2017). Textbooks carry perceived authority due to their endorsement by educational institutions and are seen as holding the official version of a society’s knowledge (Smith & Sheyholislami, 2022). They are used in 98% of IP courses in the United States, and are often the only assigned reading (Griggs & Bates, 2014). Whissell (1997) described IP textbooks as “flagships of the discipline” (p. 115), able to define and present to the world what psychology is. Textbooks are also central for professional training, considered a resource for both knowledge and professional identity (Fredwall & Larsen, 2019). The limited literature on IP textbooks indicates they can contain information that is outdated (Wahl, 1989), inconsistent with current research (Arrigo & Pezdek, 1998; Wilgus et al., 2016), and incomplete or factually inaccurate (Bartels, 2019; Ferguson et al., 2018; Gleaves, 2007; Griggs, 2014; Steuer & Ham, 2008; Zucchero, 2011). Over time, alterations to IP textbooks have addressed some of their limitations, including correcting inaccuracies in well-known narratives (e.g., Griggs, 2014).
Textbooks used in psychology courses typically have an uncritical psychiatric and diagnostic focus (Cromby et al., 2008). Some have argued that many abnormal psychology textbooks do not transparently express the controversies in psychology or the tenuousness of the facts they present (Simon, 2006). Textbooks may align with a primarily biomedical, individualising perspective of mental distress common in undergraduate psychology curriculums more generally (Simon, 2006; Snyder et al., 2019).
Given the reach and impact of IP courses, their content and its dissemination stand to shape how people experiencing distress are understood and treated, impacting their lives and livelihoods. In this article, we explore (a) how people with a diagnosis of schizophrenia (PWDS) are constructed in IP textbooks and (b) how a Mad Studies (MS) theoretical framework might imagine otherwise. While MS is relevant for constructions of various experiences of mental distress and engagement with these in textbooks, we focused on constructions of schizophrenia. This diagnosis is often associated with problematic and limiting stereotypes and misinformation that may be replicated in psychology textbooks (Hunter, 2013; Joseph, 2000). Psychosis refers to a category of experiences often associated with schizophrenia, including sensory experiences and/or beliefs that others do not share and appearing out of touch with consensus reality (Cooke, 2017). Psychosis is rarely presented “from within” (i.e., from the perspectives of people experiencing it), missing layers of understanding that stem from lived experience (Fredwall & Larsen, 2019; Jones & Shattell, 2016). Textbooks typically portray psychosis, schizophrenia, and associated symptoms through a biomedical lens (Cromby et al., 2008; Halter et al., 1992; Hunter, 2013; Joseph, 2000; Simon, 2006); thus, there may be disconnection between how people are described and how they feel, and between what they want and what they receive.
Mad studies
MS is a body of scholarship stemming from lived experience/consumer movements (Beresford, 2020). Key principles of MS include prioritising the voices and knowledge of those with lived experience over “experts,” favouring social over biomedical approaches, taking a critical lens on psychological constructions, and focusing on the meanings behind madness (Sweeney, 2016). MS highlights the role of power in psy professions and education, where professional knowledge dominates experiential knowledge, and professionals hold power over those diagnosed (Faulkner, 2017). Psy professionals and the “psy-complex” refer to a “dense web of theories and practices” where control over meaning and “solutions” to mental distress is primarily held by psychiatrists and psychologists (Parker, 2007, p. 10).
Both authors of this paper have lived experience of mental health service use and aim to honour lived experiences throughout our scholarship. We approached this topic with a focus on where the voices of those with lived experience are—or are not—in depictions of mental distress. Accordingly, we focused on how traditional and biomedical constructions of madness often exclude the knowledge and perspectives of mad people (Sweeney, 2016). MS invites a consideration of truth and legitimacy regimes as (re)produced through expert discourse (LeBlanc & Kinsella, 2016; Russo & Beresford, 2015). Critically analysing discourse within IP textbooks offers an opportunity to examine what discursive constructions exist around PWDS—and what and who these constructions open, close, portray, and exclude.
In keeping with MS convention, we use the (not universally embraced) terms mad/ness and lived experience (of mental distress) to describe what is traditionally called “mental illness.” We use “person/people with a diagnosis of schizophrenia”—abbreviated to PWDS—rather than “schizophrenics” or “people with schizophrenia.” While the existing literature often focusses on psychosis, the textbooks we examined rarely mentioned psychosis outside of the diagnosis of schizophrenia, so our findings and discussion refer primarily to schizophrenia specifically. Diagnostic language itself is a contentious issue, particularly within MS, where many find such language reductive. Our focus is not on adjustments to diagnostic language but on exploring how this language—and other discursive constructions—works to close or open opportunities to engage with complex and nuanced lived experiences.
Constructions of schizophrenia
Negative representations of people with mental distress are consequential; they can increase negative attitudes and stigma towards those with psychiatric diagnoses, impede help-seeking, and generate a sense of pessimism about recovery (Stuart, 2006). There are numerous problematic representations of people experiencing psychosis, who are often presented as unpredictable, dangerous, and unable to recover (Kassam et al., 2011; Magliano et al., 2014). These perceptions can result in discrimination from family, friends, and community members, as well as within housing, social services, and employment (Thornicroft et al., 2009).
Metzl (2009) outlined how constructions of schizophrenia have shifted over time and been tethered to gendered and racialised stereotypes. From the 1920s to 1950s, schizophrenia was constructed as a disorder primarily affecting people who were white and who were viewed as generally harmless, if somewhat infantile, and in need of nurturing. Following the civil rights movement, schizophrenia was reconstructed as a disorder impacting men, particularly Black men, and became associated with aggression, volatility, and hostility. As Metzl described, this enabled a construction of civil rights activism as itself delusional and psychotic. These constructions shifted the proposed management of schizophrenia from a nurturing stance to a more restrictive and controlling one. This intersection of racism and negative stereotypes associated with psychosis has persisted and spread, with harmful consequences. In Aotearoa/New Zealand, for instance, Māori adolescents experiencing “early psychosis” are often labelled within mental health services as violent and high-risk, which can lead to increased coercion and poorer outcomes (Manuel et al., 2023).
Today, a construction of schizophrenia characterised by biomedical and diagnostic discourses prevails. Schizophrenia is presented as a genetic disorder and a disease or dysfunction of the brain, despite limited empirical evidence (Cromby, 2016; Magliano et al., 2014). Biogenetic constructions can increase the negative stereotypes associated with schizophrenia (incompetence, unpredictability, dangerousness, and inability to recover) and create the desire for social distancing from PWDS (Magliano et al., 2014; Zimmerman et al., 2020). In response, clinicians may prioritise long-term neuroleptic medication at the expense of psychosocial interventions (Magliano et al., 2014).
Many people who experience psychosis or who are prescribed antipsychotic medication endorse psychosocial explanations for their experience over biomedical explanations (Carter et al., 2018; Read, 2020). These explanations include trauma, abuse and neglect, social stressors, bereavement and loss, psychological characteristics, and spiritual or existential experiences (Read, 2020). People with lived experience may frame psychosis as a normal (i.e., meaningful, understandable) response to abnormal (traumatic or distressing) life circumstances (Corstens et al., 2014). These ways of framing psychosis differ markedly from many mainstream psychiatric/biomedical perspectives on psychosis. Exploring these varied perspectives through the lens of discourse affords us an opportunity to further unpack the operation of multiple and conflicting lenses on experiences. In this study, we explored these representations as they play out in IP textbooks.
Methodology
We used Foucauldian discourse analysis (FDA), a type of critical discourse analysis (Wodak & Meyer, 2016) to explore how people with a schizophrenia diagnosis (PWDS) were constructed in IP textbooks. In a discourse analytic frame, language not only conveys meaning but is itself meaningful; it makes certain ways of doing, being, and understanding possible (Foucault, 1982; Willig, 2013). Discourse does not objectively describe reality, but instead creates and sustains reality. By exploring discourse as regulatory and constructive, we can unpack common, taken-for-granted, “expert”-endorsed, and alternative or resistant ways of discussing people and things that materially and ideologically influence how those people and things are understood (Arribas-Ayllon & Walkerdine, 2008; Foucault, 1982). People, and texts produced by people, reinforce and/or resist certain possibilities for how someone or something might be understood (Davies & Harré, 1999). This is not necessarily a delimitation that authors actively choose, but works through everyday interactions and structures (Lazar, 2005). This methodological approach aligned with our theoretical framework, Mad Studies, in a shared acknowledgment of and attention to power.
Data collection
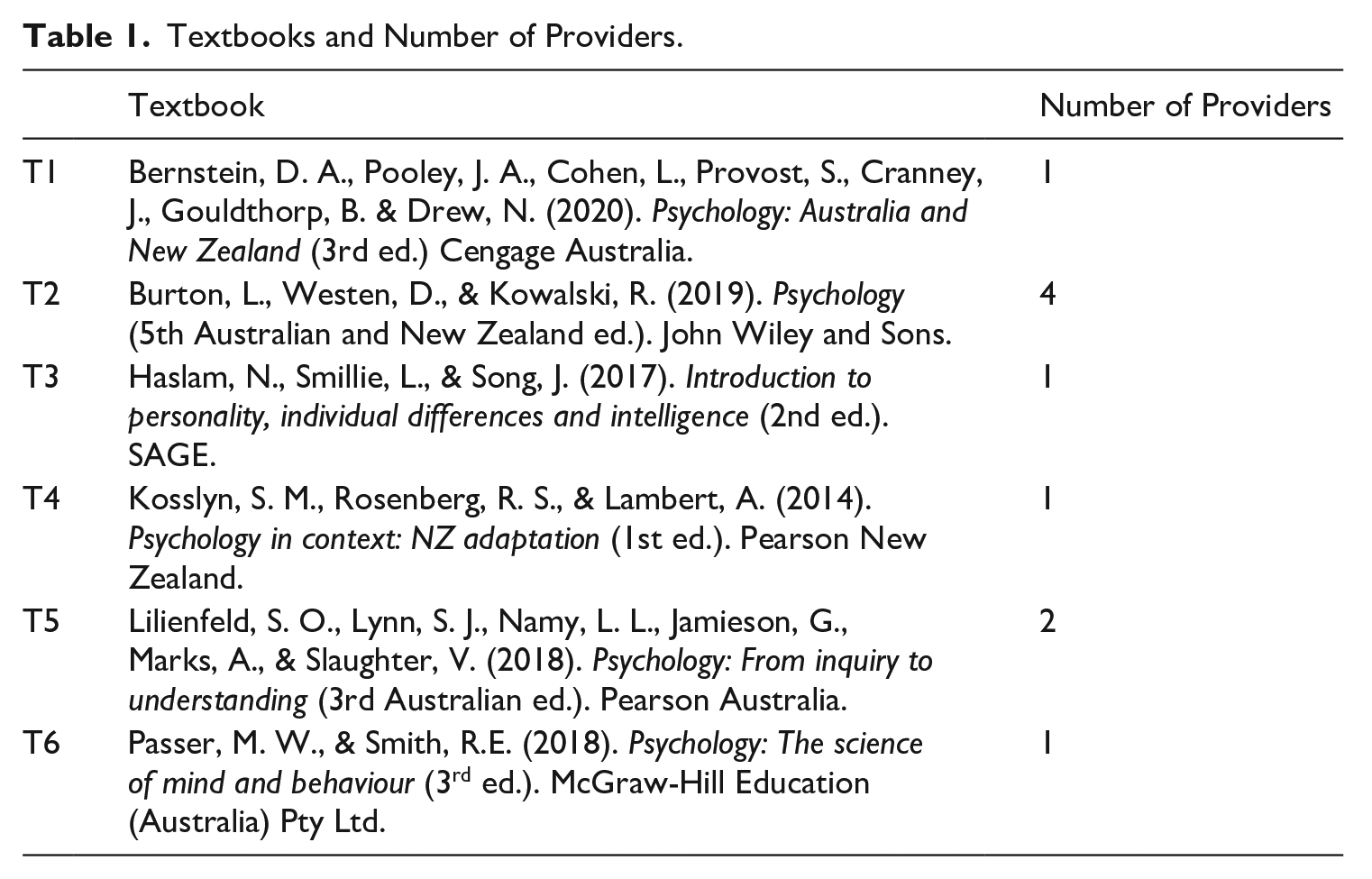
As this project analysed publicly available data (published textbooks), we followed a low-risk ethics protocol through Massey University. We intended to analyse the current assigned textbooks for IP courses at the six largest tertiary providers in Aotearoa/New Zealand. Due to textbook overlap across courses and courses without assigned textbooks, this approach yielded only three textbooks. We thus examined the 10 largest tertiary providers in Australia from which we identified a further three textbooks, resulting in a total of six textbooks assigned across 10 IP courses (see Table 1 for textbooks and the number of providers that assigned each textbook). It appeared that two textbooks were written for an Australasian audience and four were adapted from US textbooks.
Textbooks and Number of Providers.
Data analysis
We identified all relevant material in each textbook: chapters (e.g., “abnormal psychology,” “psychological disorders”), sections (e.g., “schizophrenia spectrum disorders”) and references within the index outside of these chapters (e.g., hallucinations, psychosis). We examined this material and the broader chapters containing information about psychosis/schizophrenia for contextual and comparative information. The first author, in consultation with the second author, followed the six stages of FDA as outlined by Willig (2013). We identified all constructions (implicit and explicit) of the discursive object (PWDS) in the text and considered how PWDS were located within wider societal discourses. We then explored action orientation: how discourses function and what they invite, justify, negotiate, or prevent. Then we examined the subject positions made possible by constructions of PWDS and the opportunities for action enabled and prevented by these constructions and subject positions. Finally, we examined the consequences of the subject positions on the experiences of those involved, particularly those who experience psychosis. Throughout, we considered what the writing was doing—and how broader ways of describing, constructing, and formulating were made possible/impossible in relation to PWDS. In the discussion section, we explored potential MS “responses” to these constructions, exploring differences in how PWDS might be engaged with in psychology textbooks. In so doing, we orient to the ways in which a MS theoretical lens invites alternative ways of constructing PWDS, which might provoke new pedagogical openings in psychology.
Analyses
We identified three interconnected discursive constructions of PWDS: object-for-study, social problem, and unrecoverable illness. Broader biomedical and diagnostic discourse appeared throughout these discursive constructions. Consequently, these constructions produced a particular outcome for PWDS: requiring treatment, primarily biomedical treatment within the psy-complex. While each textbook is quoted in our analysis, we have not identified in-situ which textbook each quote is sourced from or the specific page number on which the quote appears (see also Hunter, 2013). 1
Object-for-study
The textbooks construct PWDS as objects for study and expert intervention. Ultimately, through this construction, the subjectivity of PWDS is absented, with little reference to the personhood of the PWDS evident in the textbooks. One core aspect of this construction is the power of the biomedical gaze, which presents schizophrenia as a (scientifically) understandable entity, inviting assessment and measurement of pathology. This separates the body—and the “pathology”— from the person, and positions doctor/expert/researcher as powerful and knowledgeable (Foucault, 1973). Another formulation related to this construction is the working up of “novelty”. Here, PWDS are constructed as oddities for observation by expert observers. This is related to the biomedical gaze, insofar as the reader is invited to marvel at the difference of schizophrenia as observable entity. In parsing out schizophrenia from the person, textbooks work up assessment, measurement, and study as natural next steps. In so doing, the subjectivity of PWDS is absented, reduced to statistics, and defined based on their prevalence, genetic predispositions, and likelihood of chronicity and suicide.
In places, an explicitly expert or teaching tone reinforces this construction; for example, “we can see that this patient skips from topic to topic” (T5); here, both reader and writer are positioned (“we can see”) as scientists studying a perplexing phenomenon from a professional distance. The reader, who the text implicitly presents as not being a PWDS, is at times invited into the expert position, for instance with the use of a rhetorical question: A challenging question for evolutionary psychologists is how to explain the presence, over several generations, of a stable percentage of the population that has a debilitating mental disorder. How, for example, can an evolutionary theorist explain the worldwide presence of schizophrenia, a disease that clearly diminishes an individual’s capacity for both survival and reproduction? (T2)
Here, the phenomenon of schizophrenia takes over from a meaningful engagement with the subject position of the person at the centre of the experiences described. Then, schizophrenia is constructed as a phenomenon that fascinates scientists. The focus on survival and reproduction constructs schizophrenia as a biological anomaly. This evolutionary focus reinforces a medicalisation of schizophrenia that enables a focus on the characteristics of schizophrenia as biological entities, rather than exploring the subject positioning of PWDS in relation to biographical and social contexts.
Where PWDS are discussed (versus schizophrenia as diagnosis), they are referred to as “cases” and “patients,” positioning them in relationship to professionals, as objects for clinical intervention. At times, this construction also elides an explicit construction of the person themselves, instead confirming the subject positioning of the diagnosis itself: “the heterogeneity of this condition makes it difficult to arrive at a reliable diagnosis in many cases” (T4). Here, PWDS are absented, while schizophrenia as “condition” is discussed as “difficult” for professionals to diagnose, due to its heterogeneity. Contrastingly, the following quote takes an expert diagnostic tone, constructing schizophrenia as a homogenous diagnosis: Psychiatric diagnoses serve at least two crucial functions. First, they help us pinpoint the psychological problem a person is experiencing. Once we’ve identified this problem, it’s often easier to select a treatment. Second, psychiatric diagnoses make it easier for mental health professionals to communicate. When a psychologist diagnoses a patient with schizophrenia, [they] can be reasonably certain that other psychologists know the patient’s principal symptoms. Diagnoses operate as forms of mental shorthand, simplifying complex descriptions of problematic behaviors into convenient summary phrases. (T5)
Mental distress is formulated as a “problem” for professionals to solve. Diagnosis is then positioned as crucial for easing treatment selection, presenting this as necessary and as facilitating communication. While the PWDS is more “present” in this instance (first as “a person” and then—once the “problem” is isolated—as “a patient”), they are distilled into a diagnosis, resolving the constructed issue of a complex problem by enabling shorthand. Here, diagnosis exists solely to benefit professionals, rather than also considering its effects on the people being diagnosed, who may find diagnosis either, or both, helpful and harmful; the nuances and complexities of a collaborative diagnostic discussion are not presented.
At times, “symptoms” of schizophrenia are explored in relation to different (i.e., nondiagnostic) ways of understanding. For instance, hallucinations are positioned as potentially relevant in non-Western contexts: Some non-Western cultures . . . value hallucinations as gifts of wisdom from the gods . . . These cultures possessed terms for disorders that are strikingly similar to schizophrenia. (T4)
Positioning hallucinations as “gifts” is made possible by positioning this as other (“non-Western”). This opens potentially different readings of schizophrenia, but constructs other cultures as misreading entities that should be clinically diagnosed. The phrasing “strikingly similar to schizophrenia” brings this alternate reading back into a diagnostic frame, as does the assertion of these being alternative terms for “disorders.”
Elsewhere, “symptoms” are constructed as problematic or “bizarre.” Every textbook uses terms such as “bizarre,” “abnormal,” “oddities,” “inappropriate,” “peculiar,” and “different” to refer to people and their behaviour. In using these kinds of terms, an oblique subject positioning enables a particular working up of how one might orient to PWDS: While in a stuporous state, they may exhibit waxy flexibility, in which their limbs can be moulded by another person into grotesque positions that they will then maintain for hours. (T6)
Here, the subject position open to the PWDS is passivity; neither being moulded into “grotesque positions” nor doing so to a vulnerable person are problematised. Meanwhile, the PWDS is only present as “they” in this passage. While this construction appears across textbooks, overtly voyeuristic behaviour is discursively positioned as a relic of the past, as in this quote about Bedlam: “in those days, people could buy tickets to tour the cells and gawk at the patients” (T1). In positioning this as past behaviour (“in those days”), the textbook can maintain its status as modern and beyond such constructions, while simultaneously reinforcing voyeurism in maintaining an “object-for-study” discursive construction.
Social problem
In this discursive construction, PWDS are formulated as socially problematic, burdensome, and undesirable. A core aspect of this discursive construction is the positioning of PWDS as detached from sociocultural context (particularly the sociocultural factors that make sense of their madness), out of contact with “reality” and “normality,” and to be avoided by nonexperts. Secondly, this discursive construction positions PWDS as undesirable, dangerous, and burdensome. As in the prior discursive construction, both of these formulations rely on the absenting of the subjectivity of PWDS in favour of constructions of the diagnosis of schizophrenia.
While this construction involves a similar gaze-like positioning for the textbook writer and reader vis-à-vis the PWDS, here the observed behaviours or characteristics described relate to socially (un)desirable traits or actions. For instance: Lack of motivation and poor social skills, deteriorating personal hygiene and an inability to function in everyday situations are other common characteristics of schizophrenia. (T1)
Here, the PWDS is once again largely missing—this passage constructs schizophrenia itself as object, describing how its characteristics include lacking motivation and social skills. The PWDS is present in their absence, with schizophrenia itself operating as a force that generates an inability to function or be hygienic. Arguably, this could be understood as a nonblaming stance, where the person is absented in order to foreground the (externalised) force of the diagnosis. However, in absenting the PWDS, there is also a risk of the diagnosis coming to represent, for the reader, the totality of the person’s subjectivity and experiencing. Elsewhere, PWDS are described as “commonly odd, eccentric, or peculiar in their mannerisms” (T3). This positioning can “other” the PWDS, generating distance between them and the reader, who is positioned alongside the author as an observer and expert. For instance, one textbook suggests that “they may strike us as ‘odd ducks,’” (T5) referring to PWDS as striking “us” (the textbook writer and reader). This positioning also negates the possibility that the reader might themselves have been diagnosed with schizophrenia.
We observed instances of counter discourses, where experiencing mental distress is constructed as normal or at least common; this often refers to mental distress more broadly and/or symptoms of schizophrenia, such as hallucinations. As one textbook notes: experiencing a mental disorder at some stage in life was the “norm,” rather than the exception, with only 17 percent of the population reaching mid-life free of any mental health problems. (T2)
While mental disorders are explicitly positioned as the norm here, they are still problems, with “reaching mid-life free of any mental health problems” (T2) a desirable, if uncommon, achievement. Elsewhere, textbooks refer to hallucinations as relatively common, noting that: between 10 and 14 percent . . . to as many as 39 percent . . . of college students and people in the general population report having hallucinated during the day at least once—even when not taking drugs or experiencing psychological problems. (T5)
Here, the textbook normalises the experience of hearing voices, positioning mental distress—and schizophrenia symptoms—within the realm of human experience. The use of statistics and references reinforces the expert positioning here. Despite the reported commonality of hallucinations amongst the general population, the construction of psychosis as abnormal remains dominant.
Despite counter discourses, the construction of PWDS as social problems and abnormal largely position them as unpredictable and potentially dangerous and violent. Textbooks describe unpredictable or violent behaviour, stating that PWDS might “fly into a rage” (T1), experience “unpredictable agitation” (T4) or “bouts of frenzied, purposeless motor activity” (T5). Some textbooks feature explicit statements that PWDS “can be dangerous to others” (T6), not distinguishing between potential risk to oneself versus others. At times, famous examples are used to support this discourse, such as speculation that Vincent van Gogh may have had schizophrenia, and this drove violent behaviour including cutting off his own ear. Elsewhere, this danger is linked to both the normality and unpredictability of schizophrenia; for instance, schizophrenia “strikes about 1% of people” (T3). This phrasing constructs schizophrenia as something that occurs suddenly and randomly, like a lightning bolt from the sky.
Unrecoverable illness
Within this discourse, the subjectivity of PWDS is once again largely elided, with a reduction instead to the diagnosis of schizophrenia. In turn, schizophrenia is constructed as a catastrophic illness without cure or potential for recovery. A core feature of this discursive construction is chronicity. Despite this chronicity, a second core feature is the working up of the necessity of (primarily pharmaceutical) treatment. With regard to the former, five textbooks, strongly suggest that people cannot recover from schizophrenia, using terms like “chronic,” “enduring,” “recurring,” “long-term,” “permanently,” and “relapse,” and phrases such as “many years of anguish and incapacitation” (T6). One textbook states: [family members] also tend to believe their schizophrenic relatives could fight their symptoms if they just exercised more willpower. . . Believing that people can control their destiny may be destructive when it is not true. (T2)
While this may be an attempt to absolve PWDS of blame for their symptoms, it constructs them as being powerless over their experience, having no hope of recovery, and having no influence over their symptoms or future. The distinction between PWDS and family (framed as nonexpert) and biomedical (expert) opinion is reinforced in the statement “it is not true.”
Where recovery features in the textbooks, it is undefined and/or constructed as an impossibility, with the most desirable outcome deemed to be “function[ing] reasonably well”: About 40 per cent of people with schizophrenia improve with treatment and are able to function reasonably well. The rest show continuous or intermittent symptoms that permanently disrupt their functioning . . . and, especially for those with a drug abuse problem, may lead to homelessness. (T6)
While the 40 % figure may initially invite some hope, this positions the best possible outcome for PWDS as to “function reasonably well”—not to recover or live a full life. The 60%, then, apparently have permanently disrupted functioning, with drug abuse and homelessness framed as looming possibilities. These figures further lend credence to the expert opinion and tone present throughout the textbooks.
Elsewhere, a more optimistic alternative was presented: Researchers found that 20 high-functioning people with schizophrenia—including doctors, an attorney, and a chief executive—used such strategies as taking medication, getting exercise and adequate sleep, avoiding alcohol and crowds, and seeking social support to manage their illness successfully. (T5)
Here, PWDS may use intensive practices to “manage their illness” by being effective bio-citizens (see Rose, 2007). The naming of professions with high social status emphasises that the promise of these practices is not to only “function,” but to be powerful members of society, as defined within a capitalist frame of reference. In all instances, recovery is presented as occurring only with treatment within the psy-complex.
While people may, in this construction, reach a “reasonable” or even (rarely) high level of function, schizophrenia is still constructed as destructive. Using terms like “severe,” “profound,” and “disturbed,” PWDS are described as “sufferers of schizophrenia” and “severely disordered people” (T6), positioning them as victims of schizophrenia; a terrible affliction which is “especially tragic” (T3). They are described as having a “shattered mind” and “one personality that’s shattered” (T5), suggesting that schizophrenia has the power to destroy the things that make them who they are. For instance: [a psychiatrist] has called schizophrenia the “cancer” of mental illness: It’s perhaps the most severe of all disorders—and the most mysterious . . . . As we’ll discover, it’s a devastating disorder of thought and emotion associated with a loss of contact with reality. (T5)
The comparison with cancer, a medical disease which invokes fear for many people, discursively ties schizophrenia to suffering, premature death, and debilitating and often unsuccessful treatment. The association further tethers schizophrenia to a biomedical discourse inviting medical intervention. Despite the construction of recovery as impossible, biomedical treatment is constructed as essential. The kind of treatment constructed as required is linked to the construction of schizophrenia itself as a biological illness or disorder caused primarily by genes and faulty brains. While textbooks present psychosocial discourses, these are given significantly less space and often dismissed as theories in favour of biomedically focussed constructions. Psychosocial factors are described as “important,” but then given minimal, if any, further description. For example: Although a biological vulnerability appears to be essential for most or all cases of schizophrenia, environmental variables play an important role in both the onset and course of the disorder. (T2)
Environmental variables are constructed as “important,” but positioned as secondary to biological factors, which are “essential.” Despite their purported “importance” they received a fraction of the word count given to biological factors. Another text (T6) likewise deems the search for parent/family causal factors “largely unsuccessful,” constructing a failed attempt without future potential, while simultaneously describing the specific genes and their role in schizophrenia aetiology as “still unknown.” This frames genetic research as a worthwhile endeavour within a discourse of faith for imminent discoveries that promise more fulsome “solutions.”
With schizophrenia constructed as a biomedical illness, treatment therefore must be biomedical; medication is constructed as “superior,” “effective,” and “essential” for treating schizophrenia. This superiority is reinforced by the construction of PWDS as incapable of communicating effectively: Thought disorganisation is often so extreme that it is difficult to communicate with these individuals. Their behaviour often appears silly and childlike and their emotional responses are highly inappropriate. (T6)
This construction of PWDS as having “highly inappropriate” emotional responses and as appearing “silly and childlike” positions their voices and processing as ineffective. PWDS are reduced to their diagnoses, thus rendered recipients of treatment, and as potentially unable to respond “as expected.” This severely limits collaborative and nonbiological treatment options; talking therapies, for example, rely on effective communication and coherent thinking, which are constructed as absent in PWDS. Meanwhile, medication is constructed as helpful and practically unlimited: “For virtually every psychological disorder treated with psychotherapy, there’s an available medication” (T5). The framing of virtually every disorder as having a potential medication formulates this option as the viable path for exploring treatment. Psychological, and especially psychosocial, therapies are positioned as adjunct to medication and as enabling acceptance rather than being first line: “therapy can play a role in helping them to accept the need to take medication on a lifelong or long-term basis” (T4). The lack of power and credibility of PWDS reappears in this discourse, where “patients” are treated, and doctors know best what patients “need to accept.”
Despite the construction of medication as an essential solution for schizophrenia, descriptions of its effectiveness, and the statistics used to reinforce the credibility of these claims, are inconsistent both within and across textbooks. The following quotes appear within one text: “Antipsychotic drugs have been used successfully for over 60 years,” “only a minority experience a good response, and successful treatment of the negative symptoms of schizophrenia is still a challenge.” (T6)
Despite the stated shortcomings, antipsychotic drugs are still constructed as “successful” in countering the “challenge” of schizophrenia. When describing antipsychotic medication, several texts note potential harms, including tardive dyskinesia caused by antipsychotic medication: Uncontrollable and grotesque movements of the face and tongue are especially prominent in this disorder, and sometimes the patient’s arms and legs flail uncontrollably. Tardive dyskinesia can be more debilitating than the psychotic symptoms that prompted the drug treatment, and it appears to be irreversible once it develops. Within 4 years of beginning antipsychotic medications, about 20 per cent of young adults and 30 per cent of those over 55 develop tardive dyskinesia symptoms. (T6)
Despite the severity of such side effects (“can be more debilitating . . . irreversible once it develops”), in every text that mentioned iatrogenic harms, they are downplayed as an acceptable risk—without explanation of how possible risks could be transparently explored with PWDS. This risk is constructed as being balanced out by the described risk associated with PWDS, as well as other measures that are framed as more problematic: Antipsychotic drugs have reduced the need for padded cells, straitjackets and other restraints that were formerly used to control the disordered behaviour of hospitalised patients. (T6)
Some kind of control is positioned, here, as needed in order to rein in “the disordered behaviour” of the PWDS. Medications are likewise positioned as replacing more invasive forms of treatment, without destabilising the shared goal of these approaches, for instance: Large numbers of lobotomies were also performed in Australia and New Zealand, though the number fell dramatically after the 1950s, as drugs became available, especially for schizophrenia. (T2)
Medication is thus positioned as a powerful tool that enables PWDS to be “released” from hospitals, a term suggestive of the release of prisoners. In positioning lobotomies and restraints as tools of the past, current treatments are discursively distanced from practices now seen as restrictive or inhumane. One text references non-Western treatment methods, constructing these as inferior to Western methods through terming them “nonclinical” and stating “however, the efficacy of such treatments is unknown,” (T2).
Counter discourse appears in two texts which reference psychosocial support, framing this as efficacious, and, with reservation (“appears to”) as playing an important role in recovery (notably, from an episode rather than schizophrenia): “family interventions are efficacious” and “social support appears to play an important role in recovery from a schizophrenic episode.” (T4)
Still, medication maintains its position as superior: “medication . . . is clearly superior to the use of therapy, although CBT can help decrease psychotic symptoms.” (T4)
Once again, recovery remains elusive, with therapy framed as potentially helpful to decrease symptoms.
Discussion
Through a Foucauldian discourse analysis of the textbooks, we have demonstrated how PWDS are constructed through a biomedical lens as objects-for-study, social problems, and unrecoverable illnesses. These discursive constructions position PWDS as passive recipients of biomedical treatment who require control and containment: interventions that must be undertaken by particular kinds of experts. These discourses (re)produce and reinforce themselves and each other; together, they present biomedical treatment as a logical response to an unsolvable, but manageable, problem. Our analyses highlight tensions between lived experience perspectives prioritised in MS and traditional psy-expert perspectives reinforced through textbook discourse.
The dominance of biomedicine within the discursive constructions we explore above, which constructs schizophrenia as a biological disorder caused by genes and faulty brains, is consistent with findings across the literature (Cromby et al., 2008; Halter et al., 1992; Hunter, 2013; Joseph, 2000; Simon, 2006). Undergraduate students are not exposed to discourses that confront biomedical discourse (Snyder et al., 2019)—even the counter discourses we have identified above do not wholly dislodge the dominance of this frame. The texts position biological vulnerabilities as the ultimate cause of psychosis, and psychosocial factors as simply activating these underlying vulnerabilities (Boyle, 2013), despite a lack of empirical evidence to conclusively support biological vulnerability theories (see Bentall, 2004; Dillon & Read, 2013). Research on psychosocial causes of mental distress is largely overlooked or dismissed (Hunter, 2013), despite psychosocial explanations often being favoured by mad people (Carter et al., 2018; Read, 2020). We similarly found that the texts extensively covered psychotropic medications and inpatient hospitalisation, with less coverage of psychosocial treatments and community-based services. Recovery, or at least a degree of “functioning,” is presented as possible only with biomedical (and perhaps some adjunct psychological) treatment, within the psy-complex, overlooking evidence to the contrary and the benefits of nonpsy support (see Cooke, 2017). None of the texts feature established or emerging approaches that seek to enhance autonomy and make sense of “psychosis,” which can be effective and favoured by many PWDS. Such approaches include hearing voices peer support groups (Longden et al., 2018), Open Dialogue (Bergström et al., 2022), and Soteria houses (Leendertse et al., 2023). Non-Western and nonbiomedical approaches to treatment differences are either disputed or constructed as unusual cultural practices, inferior to scientific Western treatment (see also Hunter, 2013). Engaging with Mad Studies theories calls textbook writers and lecturers to open new conversations with students that encourage them to explore tensions in these constructions—and to prioritise the voices of mad people in storying their experiences (Pagdon & Jones, 2023).
In general, constructions of non-Western cultures in the texts are contradictory, downplaying cultural differences while positioning non-Western cultures as strange and inferior with their “unscientific” ways, and conversely, as unusual and positive. This incorrectly implies that only non-Western communities normalise experiences that could be constructed as psychosis (Larøi et al., 2014) and reflects the problematic imposition of Western psychological perspectives onto non-Western cultures (Ranzjin et al., 2007). This overlooks strengths that non-Western cultures hold in responding to such experiences, which may be culturally normative and seen as gifts or spiritual and/or cultural experiences (Taitimu et al., 2018), as well as the benefits of culturally specific approaches for responding to psychosis for Western and non-Western people. Notably, the texts acknowledge the role of psychosocial adversity in exacerbating schizophrenia. Mad Studies frameworks would encourage a contextualisation of experiences versus a focus on pathology, extending this focus to how people are constituted within psychosocial milieu, opening space for meaningful cross-cultural analyses (Dhar, 2020).
Schizophrenia is consistently constructed as an object for study and intervention by experts and professionals. This expert, professional framing is discursively bolstered by assertive, statistically reinforced statements which often invite the reader to adopt an “expert observer” role. These statements position PWDS as having faulty genes and brains, and as biological oddities requiring expert study and/or patients requiring professional intervention. PWDS are also positioned as objects to be gawked at for fascination. Mad Studies scholars note how professionals dominate conversations about mental distress (Snyder et al., 2019); this is prominent in the texts. Perhaps the most remarkable discursive feature across descriptions of PWDS is the absence of PWDS voices. Thus, the “perspective from above” (the professional perspective) prevails throughout the texts, while the “perspective from within” (the person’s own description) is absent (Fredwall & Larsen, 2019). Including the “perspective from within” could advance a more whole-person perspective of psychosis in IP textbooks. Those developing and delivering IP resources could draw on projects that centre first-person accounts of madness, such as Rethink Psychosis (https://rethinkpsychosis.weebly.com), Hearing the Voice (https://hearingthevoice.org), videos from PWDS such as Pat Deegan (https://www.youtube.com/@patdeegan), and Aotearoa/New Zealand’s Like Minds, Like Mine (https://www.likeminds.org.nz).
PWDS are also constructed as social problems—as outcasts, dangerous, and burdens, consistent with mainstream constructions of psychosis that have become associated with incompetence, unpredictability, and violence (Magliano et al., 2014) and of schizophrenia as linked to dangerous, volatile, and hostile traits (Manuel et al., 2023; Metzl, 2009). Here, there is another relationship between discursive constructions; the unrecoverable illness discursive construction, which formulates schizophrenia as a disease with no hope for recovery, feeds into a discursive construction of PWDS as social problem. Together, these constructions work to position PWDS as unable to recover or work and therefore as burdens to society. In this way, recovery—where constructed at all—is constructed through a Western, capitalist lens where effective bio-citizens work and produce (LaMarre et al., 2019). Mad Studies frameworks would promote normalising experiences classified as psychosis, countering myths and negative stereotypes, and highlighting examples of PWDS who are living well, according to lived-experience definitions of recovery (see Andresen et al., 2003).
A diagnosis of a psychotic disorder can be deeply distressing for those diagnosed (Linscott & Cross, 2009; Pitt et al., 2009; Thomas et al., 2013). The stigma, social distancing, and discrimination that have been reported towards PWDS (Pitt et al., 2009; Stuart, 2006; Thomas et al., 2013; Thornicroft et al., 2009; Zimmerman et al., 2020) can be at least partly explained by their portrayals as strange, smelly, antisocial, unproductive, and potentially violent. These constructions may create a self-fulfilling prophecy: when a person is labelled and positioned as an outcast for their assumed traits based on a diagnostic label, they may in turn be dismissed or cast out (Scheff, 1970).
In reducing PWDS to their diagnoses and emphasising the importance of biomedical treatment to manage, PWDS are constructed as unable to recover. Here the self-fulfilling prophecy appears again: when PWDS are constructed as unable to recover, despite evidence to the contrary (Cromby, 2016; Magliano et al., 2014), they are treated as hopeless cases. They are told to give up hope (Pitt et al., 2009; Thomas et al., 2013) and impeded from accessing psychosocial support (Magliano et al., 2014), thus facing additional barriers to recovery, which reproduce the discourse that PWDS cannot recover. The constructions of schizophrenia symptoms as meaningless and wholly negative conflicts with the experiences of PWDS, many of whom report that their experiences are deeply meaningful and personal (Fredwall & Larsen, 2019), contextualised within their life experiences, and not wholly negative (Jones & Shattell, 2016).
Within the texts, entire sentences or paragraphs present schizophrenia without mentioning people; only the “illness,” “symptoms,” “treatment,” or “course.” There are no meaningful lived-experience voices of PWDS in the data, only brief “nonsensical” quotes or descriptions of symptoms in an objectifying manner. Two texts have meaningful lived experience perspectives from people with other diagnoses: one includes a first-person perspective for each of the other nine diagnoses in the chapter, with schizophrenia the only diagnosis to go voiceless. This (re)produces the epistemic injustice experienced by PWDS in psy-professions and academia, where their voices are seen as noncredible and are removed from conversations about themselves and their experiences (LeBlanc & Kinsella, 2016).
When PWDS and their perspectives are absented and psy-professionals and their textbooks positioned as experts, it becomes possible for practices that invalidate or harm PWDS to be justified (Eiroa-Orosa & Limiñana-Bravo, 2019; Hamilton & Manias, 2006). When PWDS are dehumanised, it becomes acceptable to apply potentially harmful medication as a treatment, instead of providing truly informed consent through transparent discussion of the relative benefits and risks with consideration of the person’s individual circumstances. When PWDS are constructed as dangerous and violent, forceful and coercive measures are presented as acceptable and necessary (Metzl, 2009). The harms inherent in such measures are minimised through favourable comparison with the inhumane treatments of the “bad old days.” When PWDS are constructed as out of touch with reality, unable to communicate or be understood, with random, meaningless experiences rather than traumatic and distressing lives and histories, coercive treatment that violates their rights and autonomy can be presented as justifiable. When schizophrenia is constructed as a biomedical disease, then biomedical treatment is presented as the logical and legitimate response. This rests on the unproven assumption that physiological differences singularly cause schizophrenia, when the relationship between psychosis and physiological differences is complex and multidirectional (Harrop et al., 1996). Psychological therapies and psychosocial support are rendered illogical in treating a biomedical disease that presents “patients” as incomprehensible and unable to recover. This representation persists despite contradicting experiences and perspectives of mad people.
Despite the dominance of expert, biomedical perspectives, there is also evidence of counter-discourses across all textbooks. This appears in various ways: humanising PWDS, creative “expert” approaches, normalising symptoms, countering the schizophrenia–violence myth, providing examples of recovery and success, outlining psychosocial aetiologies, and describing psychological interventions. These are powerful alternatives to the dominant discourses that construct PWDS in negative and hopeless ways. However, the dominance of traditional discourse can act as a barrier to stigma reduction in medical student training (Newton-Howes et al., 2021); similarly, here the impact of the counter-discourses may be undermined by the dominant discourses throughout the texts.
Limitations and future directions
Our positioning has inevitably shaped our analyses. However, this is the nature of qualitative research (Willig, 2013) and appropriate within a Mad Studies framework (Sweeney, 2016). Following processes for robust qualitative research (Willig, 2013), we specifically looked for counter-discourses and unexpected findings in the data. During analysis, we revisited the data repeatedly to ensure our findings were grounded in the data and that quotes were not misconstrued by editing. Throughout analysis, we engaged with the literature to ground our findings. We used reflexive practices including supervision and journaling throughout the project. Further research could provide alternative worldviews by considering constructions of family within psychology textbooks, and cultural expertise would provide a valuable lens that is missing from our analysis. As psychology textbooks are relatively understudied, constructions of other diagnoses and comparisons across diagnoses could be explored, as could constructions of broader concepts such as recovery. Shortcomings in accuracy, currency, and bias have been identified in psychology textbooks (e.g., Ferguson et al., 2018; Joseph, 2000; Steuer & Ham, 2008); a content analysis would also be warranted to provide currency to this literature.
Finally, the textbook constructions do not answer two important questions: what course content surrounds the textbook material, and what impact do the textbooks have on student beliefs and attitudes towards mad people? The textbooks may be the sole assigned reading for a course or embedded within material which offers alternative perspectives; further research could examine overall IP course content. As the textbook constructions largely resemble societal attitudes, they may not specifically have an impact on student attitudes. As noted earlier, many IP courses are structured around textbooks, creating a vicious cycle—IP course leaders struggle to find textbooks that support nonmedicalised teaching, while textbook authors may be reluctant to change their content for fear of losing sales. This status quo has been challenged by Cromby et al. (2013), who produced an IP textbook that deemphasises diagnostic categories and prioritises mad voices within a biopsychosocial paradigm.
Textbooks are an opportunity to acknowledge and explore the contested ideas and evidence about psychology beyond just the biomedical (Simon, 2006). Textbook authors and course leaders who assign textbooks might consider the mantra “nothing about us without us,” which calls for people to have ownership and authority on the topic of their own experience (Brewer, 2018). Those who write and assign textbooks could consider the constructions they are (re)producing and the potential impacts of these constructions on people who already face significant challenges and barriers. Importantly, the voices of mad people should be central, on their own terms, and in their own words. Epistemic justice means those with power—psy-professionals and academics—acknowledge and amplify the knowledge and wisdom that comes from lived experience (Snyder et al., 2019).
Conclusion
Overall, this research indicates that the dominant constructions of schizophrenia and PWDS within IP textbooks (re)produce dominant discourses of schizophrenia. In so doing, they may create self-fulfilling prophecies that sustain discursive practices and create real-world harms to PWDS. IP textbooks have an extensive reach and the potential to affect the attitudes and perceptions of many students, who may be family, friends, community members, colleagues, and mental health workers of PWDS, or PWDS themselves. By amplifying the voices of PWDS and mad people in IP courses, these counter discourses can provide the context, meaning, and hope that is missing from current dominant discourses.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.