
Abstract
Borderline personality disorder (BPD) is a serious psychiatric condition, especially stigmatized in women. Stigma is a social injustice, as it discredits and reduces the wholeness of a person to one of taint and discount. Psychological scientists play a uniquely powerful role in the stigmatization and destigmatization of BPD by constructing the meaning of BPD at each step of the research process. We discuss this powerful role and how to destigmatize BPD by incorporating an intersectionality framework that includes disability as a category of difference (as with gender, race, and sexuality). This framework centers the role of systems and structures in creating and maintaining stigma, while emphasizing the close interactions between interpersonal and structural stigma. This article illustrates researchers’ power to assign meaning to BPD in research and highlights the importance of considering individuals as embedded in intersectional social categories, which are multidimensional and dynamic in nature. We propose that intersectional cultural humility, with its social justice aim and feminist origins, can guide BPD researchers to conduct nonstigmatizing and rigorous research on BPD. To inform clinical practice and advance social justice, we offer action steps for researchers to destigmatize BPD with intersectional cultural humility at multiple steps in the research process.
Keywords
Borderline personality disorder (BPD) is a serious and heavily stigmatized mental health condition characterized by four domains of instability: in relationships (e.g., alternating between extremes of idealization and devaluation of a relationship), behaviors (e.g., recurrent suicidal behaviors or self-harm), emotions (e.g., intense and shifting mood episodes), and sense of self (e.g., markedly and persistently unstable self-image; American Psychiatric Association [APA], 2022). BPD diagnoses in clinical settings show a 3:1 female-to-male ratio, despite gender similarities in prevalence in community-based samples (Gunderson et al., 2018). Individuals meeting the diagnostic criteria have high rates of suicide (Zanarini et al., 2016) and die up to 40 years prematurely (Gunderson et al., 2018). However, like all psychopathology, BPD is a social construct imbued with meanings that reflect cultural values and beliefs negotiated among individuals holding different power positions in a societal structure at a given historical time (Cosgrove, 2000; Maddux et al., 2019). As psychologists, we are conferred with the power to assert which behaviors are normative, who is to blame for deviance from the norm, and who is worthy of “remediation” or “treatment.” Psychologists have long constructed BPD as an individual's inborn problems, falsely decontextualized and deemed untreatable (Masland et al., 2023; Pickard, 2011; Rodriguez-Seijas et al., 2023; Schwarz, 2018). This social meaning-making, in turn, impacts individuals’ behaviors and mental health outcomes. For example, the term “borderline” at its origination was merely descriptive of psychological states between psychosis and neurosis; this term soon acquired pejorative connotations and was used to label individuals—especially women—as difficult and irremediable (Masland & Null, 2022). Consequently, although BPD can be highly responsive to evidence-based psychotherapeutic treatments (Choi-Kain et al., 2017), when working with individuals with BPD compared to other conditions, health professionals are less likely to engage in helping behaviors or to express empathy and optimism (Dickens et al., 2016; Forsyth, 2007; for comprehensive reviews on the contentious history of BPD and its associated challenges in healthcare settings, see Aviram et al., 2006; Dickens et al., 2016; McKenzie et al., 2022). The academic literature perpetuates biases against BPD with pejorative language and research processes founded on stigmatizing assumptions (Masland et al., 2023). This article focuses on deconstructing BPD stigma in research practices to inform clinical care and promote social justice.
Discussions within health disciplines about eliminating BPD stigma have often taken a public health approach, highlighting the impact of self-stigma, label avoidance, and blocked service resources and life opportunities such as employment (Juurlink et al., 2019; Masland et al., 2023). That approach, however, fails to examine psychiatric disability stigma as a problem of social justice (Corrigan, 2016; Corrigan et al., 2005). Stigma is an attribute (e.g., physical illness, a mental health condition, or social category like gender or race) that discredits or reduces the wholeness of a person to “a less desirable kind,” or one of taint and discount (Goffman, 1963). As Goffman (1963) emphasized, stigma is relational, as stigmatization of one confirms the “usualness” of others. As such, stigmatization is, arguably, entirely dependent on power (Link & Phelan, 2001). Social justice involves a process of remedying oppression and marginalization associated with power imbalance at stigma's backbone, aiming “to decrease human suffering and to promote human values of equality and justice” (Vasquez, 2012, p. 337). Therefore, public health approaches alone, without integrating social justice perspectives, are limited for understanding and eliminating stigma (Corrigan et al., 2005).
Social justice is at the core of feminism (e.g., Lafrance & Wigginton, 2019). Feminists have long asserted that many descriptors of BPD (e.g., emotionality) are female-stereotyped and that the diagnosis pathologizes women by decontextualizing their mental health from adverse life experiences (e.g., gendered violence; Aitken & Logan, 2004; Cermele et al., 2001; Miller, 2008; Shaw & Proctor, 2005; Ussher, 2013). However, many feminist critiques of BPD are criticized as “neurotypical feminism” (M. L. Johnson, 2021) that risks “theorizing away” the suffering of the lived experience of BPD (Hornstein, 2013; Marecek & Gavey, 2013). Such feminist critiques reject BPD stigma for women yet still uphold the oppressive meaning of BPD, thus failing to protect any group with the diagnosis. Instead of distancing women from a BPD label, neuroqueer feminism attends to both the distress described in BPD and its unjust stigmatization, shifting “from concerns about sexism to concerns about gendered and racialized psychiatric ableism” (M. L. Johnson, 2021, p. 647). By integrating intersectional and neuroqueer feminist analyses of BPD, we seek to advance feminism's interconnected social justice goals to better understand and empower those with BPD without either embracing a female deficit perspective or distancing any group from BPD.
We acknowledge complex associations between trauma and BPD symptomatology that warrant more extensive analysis than space permits, potentially involving closer examination of the definition of trauma and healthcare implications. Briefly, BPD and trauma-related disorders (as currently defined; APA, 2022) can have significant overlap in symptomatology. While it may be possible to fully recognize BPD as trauma-based (Fonagy et al., 2017), inclusive of individuals who identify as having BPD without a self-identifiable traumatic life event, such recognition may require a revised definition of trauma. Moreover, even if clinicians recognize BPD symptomatology as trauma sequela, effective intervention still requires their competency in working with unique interpersonal dynamics associated with personality disorders (PDs; Wright et al., 2022) and selecting treatments. Such attempts to reframe or reconceptualize BPD with trauma may reflect stigma recognition but cannot eliminate BPD stigma from its root. With these complexities in mind, our approach to BPD destigmatization acknowledges both disability and other social problems such as patriarchy and colonial psychiatry, which may perpetuate or even define disability.
We take a social justice approach inclusive of BPD as a disability and focus on destigmatizing it in research, highlighting scientists’ own power to construct BPD and its stigma. Our approach to BPD research offers additional perspectives for both feminist scholars and PD researchers to understand the stigma and means to its reduction. For feminist scholars, awareness of BPD stigma as constructed in mental health research offers means to directly confront the stigma, taking an increasingly intersectional approach that attends particularly to the vectors of gender and neurodiversity. PD researchers hold powerful positions in the mental health system that afford them privileges in assigning meaning to BPD. Although contemporary PD researchers may not consciously intend to stigmatize BPD, being socialized in and unaware of the unjust assumptions embedded in the BPD literature can lead researchers to perpetuate stigma through scholarship and scientific communication. We describe how PD researchers can assign meaning to BPD at each stage of investigation and highlight the importance of considering intersectionality in BPD destigmatization. We propose that intersectional cultural humility, including the practice of reflexivity and the process of ongoing learning with attention to the intersectionality of power and social justice (Buchanan et al., 2020), can guide scholarship that is destigmatizing, beneficent, and rigorous. Finally, we provide recommendations for PD researchers to incorporate social justice perspectives in research practice.
Constructing BPD and stigma through language
Researchers assign meaning to constructs through choice of language. In the BPD literature, stigmatizing language can be overt; for example, labeling individuals as “manipulative” and “attention seeking,” phrases that convey moralistic judgement but lack empirical evidence (Masland et al., 2023). In addition, language reflecting assumptions of inferiority is ubiquitous. For example, characteristics of BPD, such as interpersonal hypersensitivity (Gunderson & Lyons-Ruth, 2008), are often assumed to be a biological “vulnerability,” even though sensitivity can be developmentally neutral, leading to different outcomes depending on the environment (Ellis et al., 2011). Characterizing behavior in terms of “risks,” “deficits,” and “impairments” is also common, even when neutral descriptors are appropriate in the context. As Rodriguez-Seijas et al. (2023) reviewed, although the current Diagnostic and Statistical Manual of Mental Disorders Fifth Edition Text Revision (DSM-5-TR) no longer describes PDs as developmental “defects” as in earlier editions (e.g., APA, 1952), PDs continue to be described as primarily attributable to an individual's “inner experience,” with less emphasis on contextual etiologies relative to other conditions (APA, 2022). Left unaware of the potentially dehumanizing assumptions about BPD reflected in such language, researchers may unconsciously incorporate concepts such as “vulnerability” and “deficit” into the meaning of BPD. If such language and associated meaning are left unchallenged, discussions and research on BPD are grounded in biased descriptions with questionable empirical support.
Language used in studies of impulsivity in BPD illustrates this stigmatizing framing. Impulsivity is a diagnostic criterion for BPD (APA, 2022), referring to behaviors that often lack foresight and are incongruent with the individual's social goals or well-being (Crowell et al., 2009; Oas, 1984). However, reference to impulsivity in the BPD literature often takes on a colloquial meaning and deviates from that operational definition, even when the definition is explicitly stated. For example, impulsive behaviors are widely referenced using phrases such as “impulse control” or “self-control” (Beauchaine et al., 2009; Crowell et al., 2009), without operationalizing the construct of control. Although “control” can be related to impulsive behaviors (Nigg, 2017), lack of control is popularly and colloquially associated with undesirable personal characteristics (e.g., lacking willpower, being “out of control”). Associating impulsive behaviors with deficient or poor character, however, is neither helpful nor necessary. For example, in eating disorders, binge eating refers to consuming an objectively large amount of food in a short period of time, often accompanied by a sense of loss of control (APA, 2022). Despite the explicit description of feeling a loss of control, researchers often recognize that associating binge eating with negative personal characteristics of lacking control is false and stigmatizing (Hollett & Carter, 2021; Ma et al., 2021; Ma, Capobianco, et al., 2019; O’Connor et al., 2016).
Moreover, in the BPD literature, references to impulsivity in conjunction with control tend to accompany theoretical descriptions of biological “vulnerabilities” or “deficits” (see e.g., Beauchaine et al., 2009; Crowell et al., 2009). Colloquial connotations of the research language, combined with theories of biological dispositions which did not originally intend to stigmatize (Linehan, 1993, 2020), have generated and perpetuated an impression—even within the PD research field—that impulsivity in BPD reflects an “inherent biological deficit” (Rodriguez-Seijas et al., 2023). By contrast, researchers can describe binge eating unambiguously with no moralistic assumptions or framing, including when biological and genetic factors are the research focus (Ma et al., 2020; Ma, Mikhail, et al., 2019; Racine et al., 2009). This clarity can be achieved, for example, by adhering to behavioral descriptions without referencing “control” and by using neutral descriptors such as biological “factors” instead of “deficits.” In BPD research, when researchers routinely discuss impulsivity with a colloquial reference to control, the description communicates assumptions of inferiority about individuals with BPD and hampers the creation of research programs that may elucidate other potential influences on impulsivity and impulsivity's potential adaptivity (Ellis et al., 2011; Ligneul, 2021).
Structural power in the meaning of BPD
Power shapes individuals’ behaviors and psychological processes as well as mental health outcomes (Hatzenbuehler et al., 2013; Pieterse et al., 2012). As feminist scholars have pointed out, power is particularly relevant to BPD symptomatology (Aitken & Logan, 2004; Cermele et al., 2001; Miller, 2008; Shaw & Proctor, 2005; Ussher, 2013). For example, chronic suicidality can reflect coping with the effects of structural stigma (for a recent analysis on BPD symptomatology in groups with minoritized sexual/gender identities, see Rodriguez-Seijas et al., 2023). Recent advancement in BPD theories also explicitly challenged the traditionally dominant intrapsychic views of BPD and discussed how considering broader structural inequalities may enrich existing theories of BPD (Fonagy et al., 2017). Ignoring power and its dynamic nature can lead to construction and examination of BPD in ways that unjustifiably blame the individual.
For example, recent longitudinal studies found that stressful life events did not prospectively predict BPD symptoms, but having BPD was related to subsequent dependent stressors (Allen et al., 2022; Conway et al., 2018). Dependent stressors are stressful events influenced to some degree by individuals’ actions, in contrast with independent stressors, which are unrelated to individuals’ behaviors and attitudes (Hammen, 2006; Paykel, 1987). The occurrence of dependent stressors was attributed to the individual and therefore deemed potentially avoidable (Conway et al., 2018). However, closer examination of the events classified as dependent stressors revealed that structural power may have received little consideration in the classification; such events included unemployment, being fired from a job, financial difficulties, and legal problems. Although individuals often contribute to the context in which they find themselves, privilege and oppression are factors that can shape a stressful situation and one's subsequent psychological outcomes. An individual's privilege and power, for example, can contribute to the behavioral norms they may follow in a situation, their autonomy in the unfolding of the situation, how the situation is subsequently narrated or characterized, and what resources are available as they navigate it. Further, the heavy stigma attached to BPD can compound existing disadvantages, in that one could experience bias and marginalization by merely being associated with the concept of BPD (Masland et al., 2023). Despite potential implications of structural power in the events classified as dependent, findings from these studies on associations between having BPD and experiencing dependent stressors (Allen et al., 2022; Conway et al., 2018) were discussed as supporting the theory that individuals with BPD create or select into stressful environments, known as a stress generation phenomenon (Hopwood et al., 2010; Wilson et al., 2017). Such conclusions, without discussing the potential influence of structural power and possibilities of structural support, are incomplete and assign characterological blame to individuals with BPD for placing themselves in stressful situations.
In addition to shaping such individual events, power is implicated in each person's life as it relates to sociocultural norms. These norms express the values and power structure of a culture at a given time, such that privileges become invisible to individuals whose way of life aligns with the dominant culture, and those whose behaviors deviate from the cultural norm are often pathologized and even criminalized. BPD has been linked specifically to such deviations using descriptions of domain disorganization, which refers to noncompliance with the rules, demands, and expectations of social domains (e.g., work, love relationships, friendships), especially in the appropriateness of expressing emotions and interpersonal closeness (Hill et al., 2008). Behaviors that do not comply or follow these rules are considered domain disorganized. Such noncompliance has been framed as manifesting early risks for BPD, if overt BPD symptoms had not already developed (Hill et al., 2008). Although difficulties with sense of self and psychological boundaries with others are important struggles for individuals with BPD and often manifest in interpersonal behaviors (APA, 2022; Bender & Skodol, 2007; De Meulemeester et al., 2021), the definition of domain disorganization dilutes BPD symptomatology as simply not complying with defined social rules. This framing does not recognize or acknowledge that domain boundaries and social rules reflect the values of the powerful. For PD researchers, omitting such consideration of structural power can lead to imprecise or inaccurate conclusions about risks for BPD and can overpathologize differences; it creates barriers to healthcare accessibility for individuals encompassing diverse statuses and identities (Gunderson et al., 2018; Masland et al., 2023; Rodriguez-Seijas et al., 2023), while failing to encourage scholarship that elucidates the real difficulties and mechanisms involved in the condition.
Importantly, identifying the power embedded in structural norms and acknowledging individual differences does not mean attempting to construct BPD symptoms as normative (i.e., pretending that related experiences are shared by everyone). Even though psychometric studies support a dimensional view of BPD (Ruggero et al., 2019), BPD at the individual level can impact people's lives in ways that create qualitatively different experiences. Focusing on similarities without acknowledging differences invalidates not only the suffering experienced by individuals who have BPD (Fonagy et al., 2011; Zanarini & Frankenburg, 2007), but also the stigma and marginalization associated with the diagnosis (Masland et al., 2023). Similarly, just as racism cannot be resolved by color-blindness (Brown et al., 2003) and sexism is not dismantled by denying gender difference (Hare-Mustin & Marecek, 1988), BPD cannot be destigmatized by normalizing its symptoms or erasing the diagnosis. Attempts to normalize symptoms of psychiatric disability imply an inherent superiority in being normative, thus exacerbating stigma and further blaming individuals for not hiding their symptoms (Corrigan et al., 2005). In short, a social justice framework inclusive of BPD neither denies the suffering of those with its symptoms nor objects to effective treatment for BPD, but instead advocates compassion and space for its unapologetic and fearless disclosure (M. L. Johnson, 2021).
Intersectional awareness in constructing BPD and BPD stigma
Beyond recognizing the role of structural oppression in the etiology and disability experience of BPD, it is imperative to incorporate intersectional approaches into BPD research and its destigmatization. Rooted in Black feminist activism and scholarship, intersectionality refers to the connection and overlap among multiple social categories (e.g., gender, disability) embedded within and constructed by interlocking systems of oppression (Collins & Bilge, 2016; Crenshaw, 1989; Rosenthal, 2016). The emphasis on how systems create and maintain privilege and oppression makes social justice a central focus of intersectionality (Buchanan & Wiklund, 2021; Cole, 2009; Collins & Bilge, 2016; Crenshaw, 1989). Essential to any intersectional approach is the analysis of power conferred by social categories and systems, linking the micro, meso, and macro levels (Else-Quest & Hyde, 2016). By recognizing the unique meaning and impact of multiple social categories, intersectionality considers each individual as inseparable from their context and does not rank oppressions (Buchanan et al., 2020; Moraga, 1981). As such, intersectionality emphasizes that social justice serves everyone and that oppression of any group cannot be solved alone or in isolation (Bell, 2016; Case, 2016; Else-Quest et al., 2023).
Despite increasing discussions about the conceptualization, assessment, and treatment of BPD in the context of social systems and oppression (e.g., Becker et al., 2022), recognizing the impact of marginalization on BPD symptomatology without fully incorporating an intersectional approach and its social justice imperative could further stigmatize BPD and those with the diagnosis, as well as clinical practitioners and researchers. Moreover, failing to fully incorporate intersectionality limits the validity and utility of research findings.
We illustrate the importance of including disability as a category of difference in intersectional consideration using a recent critique of diagnosing BPD in sexual/gender minority (SGM) groups. Rodriguez-Seijas et al. (2023) criticized the traditional exclusion of SGM individuals in BPD research and posited, “if presenting psychosocial difficulties can be understood in relation to psychosocial stress like that propagated by cisnormative/heterosexist society [as for SGM individuals], then the diagnosis of a personality disorder might be inappropriate” (p. 24). The statement points to concerning problems of generalizability of existing BPD research, yet it risks further stigmatizing BPD by perpetuating its decontextualization. On the one hand, most BPD studies have been conducted exclusively with White women (Cristea et al., 2017; Masland et al., 2023), despite a lack of evidence for elevated community prevalence among women (Gunderson et al., 2018) and comparable odds for receiving a BPD diagnosis across racialized groups (Becker et al., 2022). Further, people with BPD are more likely to identify as SGM than those without BPD (Reich & Zanarini, 2008; Rodriguez-Seijas et al., 2021), but research on relationship processes in BPD has focused almost exclusively on heterosexual cisgender women (Masland et al., 2023). These research design conventions perpetuate the myth that BPD is a “women's disorder” and inevitably raise skepticism about the generalizability of findings (Masland et al., 2023).
On the other hand, Rodriguez-Seijas et al.'s (2023) suggestion to exclude SGM persons from BPD diagnoses uniquely distances SGM individuals—but no one else—from the construction of BPD as an intrapersonal, inborn disorder without fundamentally challenging this construction and its associated stigma. They argue that when SGM individuals’ behaviors resemble BPD symptoms, the behaviors may be more appropriately attributed to environmental circumstances, rather than to the “intraindividual deficit” framing that is embedded within a BPD diagnosis. Yet, excluding SGM persons from BPD diagnoses perpetuates the stigmatized construction of BPD that intersects with cisnormativity and heteronormativity. In contrast to intersectionality, the minority stress framework on which Rodriguez-Seijas et al.'s (2023) reasoning was based does not seek to elucidate the multidimensional and dynamic nature of individuals’ power positions (Buchanan & Wiklund, 2021). Without eradicating BPD stigma itself, any attempts to protect one group of people from it (e.g., by distancing them from the diagnosis) will only function to maintain and intensify BPD stigma. Ultimately, such attempts undermine destigmatization efforts and further harm those whom the distancing was initially meant to protect.
Historical events in mental health demonstrate this point. The removal of homosexuality from the DSM represented a powerful victory of gay and lesbian activists in resisting structural oppression. However, the liberating history has also been critiqued for creating ranks of oppressions (Kunzel, 2018). Specifically, gay activists solely focused on advocating for “nonpatient, nonprisoner homosexuals” (Hooker, 1993, p. 450) by aligning their own healthiness with the unspoken norms of “gender normativity, putative whiteness, economic stability, monogamy, and other forms of belonging” (Kunzel, 2018, p. 468). This alignment achieved respect for gay and lesbian persons who fit into the constructed norms of health. The simultaneous distancing from persons who did not fit into the defined ways of health and happiness (e.g., individuals with psychiatric disabilities), however, further devalued and minoritized these multiply marginalized individuals. Similarly, transgender individuals were often excluded during the gay liberation movement of the 1970s. While changes between the DSM-II and DSM-III-R rephrased and eventually removed “homosexuality,” DSM-III for the first time included “gender identity disorder” and “transsexualism” as psychiatric disorders (Drescher, 2010). Notably, the destigmatization of gay and lesbian individuals was done with conscious awareness of the oppression placed on individuals with psychiatric disabilities (Kunzel, 2018; Metzl, 2010). Yet, some have argued that pinning the shame of mental illness on someone else was strategic and thought to reduce the number of “battles to fight” (Kameny, 1965, pp. 16–17): If [homosexuality] is sickness or disease or illness, it becomes then a mental illness. Properly or improperly, people ARE prejudiced against the mentally ill. Rightly or wrongly, employers will NOT hire them. Morally or immorally, the mentally ill are NOT judged as individuals, but are made pariahs. If we allow the label of sickness to stand, we will then have two battles to fight—that to combat prejudice against homosexuals per se, and that to combat prejudice against the mentally ill—and we will be pariahs and outcasts twice over.
As Kunzel (2018) eloquently commented, when we juxtapose the familiar victory of the gay liberation movement in mental health history with rights of those with psychiatric disabilities, we are inspired to ponder the loss “in the effort to distance ourselves so vociferously from people positioned as “patients,” and in the name of claiming health” (p. 470). In this example, an intersectionality framework names the apparent tension between two social movements (e.g., gay liberation and mental illness destigmatization) as interconnected struggles for justice. That is, in identifying how both heterosexist and ableist systems of oppression cooperate to impose social norms and devalue the humanity of individuals living outside those norms, a coalition that challenges both systems is more powerful and prevents either group from contributing to the entrenchment of injustice more broadly.
Thus, without the guidance of intersectionality frameworks, attempts to protect one group from BPD stigma by distancing them from BPD create a ranking of oppressions that further stigmatizes it. As Rodriguez-Seijas et al.'s (2023) arguments imply, a BPD diagnosis would be appropriate for “heterosexual, cisgender, White, middle-class people,” who are well-represented in BPD research and for whom the intraindividual deficit models of BPD were developed. This strategy may distance SGM groups from BPD stigma, but because oppressions are interlocking and cannot be solved by destigmatizing any single group (Case, 2016), at best it only temporarily solves one problem while contributing to others. Most saliently, feminist scholars have fought for decades against diagnosing women with BPD using similar arguments of environmental oppression (Cermele et al., 2001; Cosgrove, 2000; Marecek & Gavey, 2013), in spite of, or because of, the unjustified oversampling of cisgender women in BPD research. Notably, Rodriguez-Seijas et al. (2023) also acknowledged the clinical utility of assigning diagnoses and provided recommendations for conducting assessment and intervention with SGM persons, such as carefully considering sociocultural factors that may be associated with their symptom presentation. However, competent clinical research and practice warrant consideration of social context for everyone, regardless of their social groups (APA, 2022). If researchers and clinicians fail to respect and contextualize the experiences of individuals with BPD in general, it is difficult to conceive that SGM individuals, women, or any marginalized groups with BPD symptoms would receive more respectful care. Intersectional frameworks guide us to consider everyone within their sociopolitical context, with a recognition that intersecting forms of privilege and oppression create complex and dynamic relationships among researchers, clinicians, and people with disabilities.
Intersectional cultural humility in research
As intersectionality and constructivist standpoints assert, power and structural inequality shape the lived experience of everyone, including scientists. It is essential to recognize how our own intersectional positions confer power in various contexts as well as how power dynamics manifest in our scholarly endeavors. Moreover, despite their valuable expertise, researchers are also constant learners, gathering evidence from empirical research in their fields and from interactions with individuals with lived experience of BPD. As they incorporate new knowledge, researchers may need to change course or develop new perspectives or approaches to BPD. This process is essential to scientific advancement and requires both critical thinking and humility.
The practice of intersectional cultural humility (Buchanan et al., 2020; Ortega & Faller, 2011) is central to integrating humility with the recognition of researchers’ positionality in conducting rigorous and nonstigmatizing research on BPD and other disabilities. Intersectional cultural humility calls for researchers’ reflexivity both personally and in their respective disciplines (Berger, 2015; Else-Quest et al., 2023; Hornstein, 2013), including deep and persistent self-reflection on one's own privileges, subjective perceptions, and power positions in relation to these cultural contexts. Notably, cultural humility differs from cultural competence, which does not involve a continuous growth mindset and assumes that cultural learning has a point of completion, achievable through training and practice (Buchanan et al., 2020). Both PD and feminist researchers are conferred with the power to determine how BPD is understood and discussed. Despite claims of objectively uncovering the truth of naturally existing phenomena, psychologists’ own experiences and positionality are reflected in our science (Buchanan et al., 2021; Hare-Mustin & Marecek, 1988; Roberts et al., 2020). When PD researchers start to recognize and acknowledge that we construct BPD through each study and discussion, we move closer to conducting more comprehensive and beneficent research (i.e., better science).
Recommendations for clinical research producers and consumers
To facilitate our goal of destigmatizing BPD with intersectional cultural humility in the BPD research process, we make several recommendations for clinical researchers, both as producers and consumers of PD research. Researchers, especially clinical scientists, occupy a uniquely powerful position in the cultures of the scientific field, mental health system, and community of individuals with lived experience of psychiatric disabilities. Even though the impact of power and privilege may not necessarily be the focus of each research study, scientists’ assumptions about the influence of these social justice factors are reflected throughout the research process: researchers decide what contextual data to collect or analyze, whether certain experiences can be solely attributed to an individual, and when discussing research findings, whether considerations of structural influence can be reasonably omitted. Through this process, scientists can shape how the concepts of health and pathology are constructed. BPD may be constructed, to varying degrees, as reflecting character deficiencies or as reflecting the influence of social contexts. Similarly, who is thought to have BPD and how they are treated, as well as the roles scientists play in BPD stigmatization and destigmatization, are expressions of the power researchers wield in constructing psychiatric disabilities.
Table 1 presents an overview of our recommendations. At each phase of the research process, researchers can practice reflexivity and intersectional humility to destigmatize BPD and other psychiatric disabilities. For example, at the study design phase, researchers can critically examine theories and hypotheses about BPD and other PDs with thorough consideration of system, culture, and power. At the data collection phase, researchers can ground their sample selection in robust empirical research and theory instead of stereotypes, and they can use appropriate methodology to collect data from samples with underrepresented groups. Moreover, researchers can further amplify the voices of individuals with BPD by deploying participatory methods that incorporate how they construct the meaning and experience of their own diagnoses.
Action steps for researchers to destigmatize BPD with social justice and intersectional cultural humility.
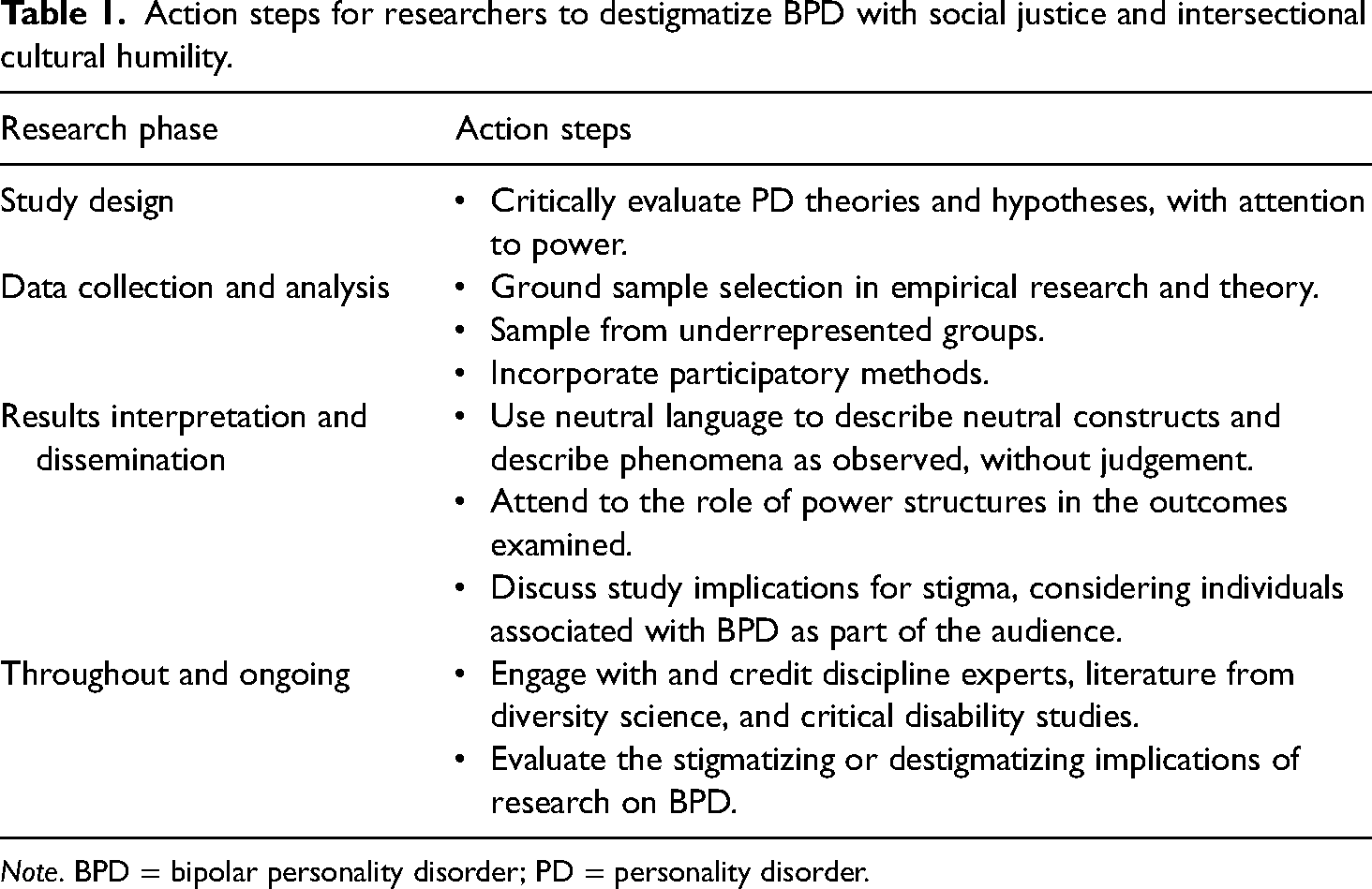
Note. BPD = bipolar personality disorder; PD = personality disorder.
At the phase of interpreting results and disseminating findings, researchers should, at a minimum, use neutral language to describe neutral constructs, seeking to avoid stereotypes and characterological judgement of individuals with BPD. Similarly, researchers should aim to describe a phenomenon in its observed or measured forms, instead of an assumed personal character trait or deficit. When we consider and discuss the role of systems or structures in the outcomes examined, rather than as an isolated intrapersonal phenomenon, we further contextualize BPD-related phenomena and deepen our understanding. Likewise, it is important that researchers discuss their study’s implications for stigma, with the assumption that individuals with BPD and others associated with the diagnosis are among the audience.
Throughout the research process, there is a need for researchers’ ongoing, iterative growth and refinement of their methods and practices. That work can only happen with the intersectional humility we advocate here. For example, PD researchers can consult and incorporate literature from diversity science, including research from critical disability studies, as well as other discipline experts. Moreover, to enhance their ability to work within social justice frameworks, we recommend researchers integrate readings on social justice in clinical science and relevant research methods while also being mindful of appropriately crediting those contributions. Finally, all of us must critically evaluate the stigmatizing or destigmatizing implications of our research on BPD and other psychiatric disabilities. We offer these recommendations as the floor, not the ceiling, for promoting social justice frameworks in clinical science.
Conclusion
A social justice perspective to destigmatizing BPD reminds us that “we are, each of us, part of the problem, because, in one way or another, and for all our differences, we have in common the fact of our participation in a society we did not create” (A. G. Johnson, 2018, p. ix). Social injustice impacts everyone, albeit in different ways. Destigmatization does not entail expressing sympathy or pity for the “othered,” but rather recognizing the inherent connections among all of us and the power in alleviating human suffering without leaving anyone behind. Researchers’ self-reflection, guided by intersectional cultural humility, involves remaining open to learning about our own inevitable subjectivity while recognizing that privilege, power, and difference shape each individual's lived experience and ways of knowing. As scientists, we portray and construct the “other” through our study design, data analysis and interpretation, and communication of science. We recognize our own responsibilities in addressing the long-standing BPD stigma, as intersectional cultural humility guides us to transform destigmatization into compassionate, beneficent, and rigorous science.
Footnotes
Acknowledgements
We thank NiCole T. Buchanan, Sherah J. Faulkner, and Kellyann M. Navarre for helpful discussions on drafts of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Canadian Institutes of Health Research (CIHR) provided essential support to RM (Grant No. DFD-175795) when preparing the manuscript.