
Abstract
Qualitative research on the experiences of those living with premenstrual dysphoric disorder (PMDD) is limited. Utilising the material–discursive–intrapsychic (MDI) framework, the purpose of the study was to privilege the voices present within individuals who have moved into a space of recovery, management, or transformation of PMDD, and explore these narratives. The study involved seven, in-depth narrative interviews. The data were then analysed using the Listening Guide, a feminist, poststructural method used to capture the polyphony of perspectives surrounding PMDD experiences. The analysis generated two broad narrative themes, with four subsequent voices under each: (a) “within abjection”—the voice toward the Other, the voice silenced, the voice of anger, the voice of agency; and (b) “beyond abjection”—the voice of action, the voice of surrender, the voice of resistance, the voice of reembodiment. Significant findings from the research involved identifying the movement toward a space of recovery, management, or transformation of PMDD as attainable, with PMDD being a negotiable and therefore plastic experience for participants. Further, the participant accounts of dismissive, uninformed, and harmful treatment from medical providers were heard; experiences which led participants toward self-help options for PMDD management.
Keywords
There is limited research exemplifying the voices of people who have previously experienced premenstrual dysphoric disorder (PMDD): biomedically positioned as a cyclical, hormone-based mood disorder arising during the luteal phase of the menstrual cycle—the time postovulation, before menstruation (American Psychiatric Association, 2013). PMDD is often defined as a severe and debilitating form of premenstrual syndrome (PMS), despite research suggesting PMDD is a separate, underlying condition that is triggered during the luteal phase (International Association For Premenstrual Disorders, 2019; Romans et al., 2012). While PMDD shares emotional and physical symptoms with PMS such as mood swings, anger, anxiety, depressed mood, sleep disturbance, and physical symptoms, such experiences are considered to be more debilitating to the point of severely impacting daily life (Kuehner & Nayman, 2021).
Whilst the reification, categorisation, aetiology, and treatment of PMDD have been heavily contested in medical, psychotherapeutic, and feminist spheres (Browne, 2015; Craner et al., 2014; Hantsoo & Epperson, 2015; Hartlage et al., 2013; Zachar & Kendler, 2014), two aspects of PMDD are still often overlooked: first, the qualitative, individual experiences of those living with PMDD; and second, the idea of PMDD as plastic: the ability for symptoms to change, increase, lessen, or disappear. Literature highlighting the combination of the two—qualitative studies investigating PMDD plasticity—appears to be further limited. Accordingly, my research allows a deeper understanding of the lived experiences of PMDD that encapsulates an arch of recovery, management, or transformation in entirety. The research raises questions regarding what were thought of as “settled certainties” (White, 1995, p. 15) in the understanding and experience of PMDD, giving agency to a voice not yet heard within the body of literature. My research explores whether the movement toward a space of recovery, management, or transformation of PMDD is attainable: whether PMDD is a negotiable and plastic experience.
Scholars taking a critical discursive perspective have highlighted how much research on negative premenstrual change, such as PMDD, often describes the experience as “pathology that must be eradicated” (Ussher, 2003, p. 136), a time that seems “alien” to the female subject (Winslow, 2019, p. 3), with the “sufferer as split” (Ussher, 2008, p. 33) between herself and the symptoms. For participants in these studies, premenstrual change could be considered as a process of abjection from the self: an experience as neither subject nor object, that which cannot be assimilated, that which is “opposed to I” (Kristeva, 1941/1982, p. 14). Here, discourse on the female experience is sustained as a process of interpellation where dominant viewpoints of the menstrual cycle become internalised (Browne, 2015; Chrisler et al., 2014; Maji & Dixit, 2019; Ussher, 2002, 2008). Further, the female reproductive body at large is “positioned as abject, as other, the site of deficiency and disease, the epitome of the ‘monstrous feminine’” (Ussher & Perz, 2020, p. 215).
In contrast to discursive critiques of the medical classification of severe premenstrual symptoms as a distinct disorder as positivist reification, the diagnostic label has been welcomed by many as validation of their experiences and opening an avenue for support (Osborn et al., 2020). Some studies have highlighted participants’ alliance toward the medical model of PMDD, alongside acknowledging its promotion of community and shared understanding (Winslow, 2019). Views on PMDD's aetiology and the purpose of the diagnostic label remain contested both among researchers and experiencers. These contestations surrounding PMDD seep into support and care options.
From a biomedical perspective, options for treatment are diverse and controversial. Common treatment options include cognitive–behavioural therapy (CBT), pharmacological treatment (such as selective serotonin reuptake inhibitors and hormonal contraception), and surgery (hysterectomy and oophorectomy; Hantsoo & Epperson, 2015). All treatment options present mixed results in terms of efficacy, with treatment guides for PMDD highlighting multiple research area gaps (International Association for Premenstrual Disorders, 2020; Kleinstäuber et al., 2012; Lustyk et al., 2009; Pearlstein & Steiner, 2012; Steiner, 2000).
Taking a discursive perspective, there is limited research on support options for PMDD specifically, and no accounts of positive PMDD change. One exception is the role that narrative therapy—a poststructural and social justice-led modality—can play in recontextualising PMDD and its symptoms (Dolman, 2015; Ussher et al., 2002). Similarly, a small body of research presents symptoms of premenstrual change as negotiable, albeit focusing primarily on PMS rather than PMDD. In this work, Ussher (2004, 2008) identifies participants’ ability to change their perceptions of negative premenstrual change, which, in turn, changes the severity of their symptoms. In this vein, the effects of recalling positive experiences of premenstrual change have also been investigated. King and Ussher's (2012) participants were able to organically recollect positive premenstrual experiences such as “legitimacy of self-care,” “release of tension,” “attractiveness,” “positive emotional outcomes,” “creativity,” and “energy.” Ussher et al. (2014) expanded on these findings, investigating how challenging pathologisation and viewing premenstrual change from a “feminist perspective” as a “source of power” (p. 340) allowed for an increase in positive symptoms. Similarly, Kues et al. (2018) investigated women's self-reported symptoms before and after reading texts associated with period positivity. They found that after reading such texts, participants reported increased positive premenstrual experiences in subsequent cycles. Nordlander (2018) reports on participants’ shared feelings of “renewed agency,” “sisterhood,” and “empowerment” associated with premenstrual symptoms, with many participants resisting the label of PMS and PMDD as being associated with cultural “baggage” (p. 8). Each of these studies supports the idea of premenstrual change not existing solely as a “fixed unitary syndrome” (Ussher & Perz, 2013, p. 909), but rather a malleable experience, as dominant discourses on the menstrual cycle, alongside individual symptoms, are able to be negotiated.
Building on this insight, my study highlights overlooked aspects of PMDD through an interpretive analysis of the narratives of those who have moved into a space of recovery, management, or transformation of PMDD. The aim of the study was to privilege and explore participants’ stories of transformation. I chose to use the words “recovery,” “management,” and “transformation” as they mirror the lived experiences and language used by my participants; however, each term can also represent the experience of positive change. The research was guided by two questions. First, what has the transition into recovery, management, or transformation of PMDD looked like for participants? Second, how have participants understood this transition?
Methodology
Aligning with the research aims, my chosen methodology privileges the individual person's voice, stories, and ownership of their body and experience. My work takes a material–discursive–intrapsychic (MDI) approach, as proposed by Ussher (1996, 1997, 2000), who argues that when conceptualising premenstrual experiences, equal importance should be placed on the tangible factors of premenstrual change, gender discourse, and the individual person's experience, including their perceptions of their experience. The epistemological shift toward a MDI approach allows for subjective experience, critical perspectives, and clinical knowledge to be held together (Ussher, 1997).
Aligning with this model, I drew on the Listening Guide as a data collection method, which makes tangible the argument of the importance of polysemy (the coexistence of multiple possible meanings; Gilligan & Eddy, 2021; Gilligan et al., 2003). The Listening Guide is based on the view that the “self” is not monotonic but rather contrapuntal, as such, the psyche contains multiple perspectives about any given experience. The Listening Guide seeks to capture each individual “voice” as a way to present the narrated subject as authentically as possible. The Listening Guide locates a person as a protagonist of their world and redefines the relationship between the scientific observer and the subject to one of coproduction, where the subject becomes the privileged author (Gilligan & Eddy, 2021; Gilligan et al., 2003). As a feminist methodology, the Listening Guide places participant voices at the forefront and upholds the feminist argument that knowledge-making practices are an inseparable and constitutive part of the realities they help create, which was upheld throughout the research, acknowledging that research methods are themselves discursive and representational (Doucet & Mauthner, 2008; Mauthner, 2017).
Data collection and analysis
The study entailed in-depth narrative interviews with people who have previously experienced PMDD. Participants were recruited through social media pages and online support groups involving PMDD. Participation was completely voluntary and self-selective. Inclusion criteria for participants were as follows: (a) participants must be over the age of 18, (b) hold a sound understanding of the English language, (c) have experienced PMDD, either diagnosed by a medical professional or self-diagnosed, though (d) feel they have moved into a space of recovery, management, or transformation of PMDD. Seven participants were selected to participate. The small number of participants was justified by the wish to capture the vivid, idiographic accounts from participants surrounding their personal experiences of and post-PMDD. Table 1 below provides an overview of the participant characteristics.
Participant demographics.
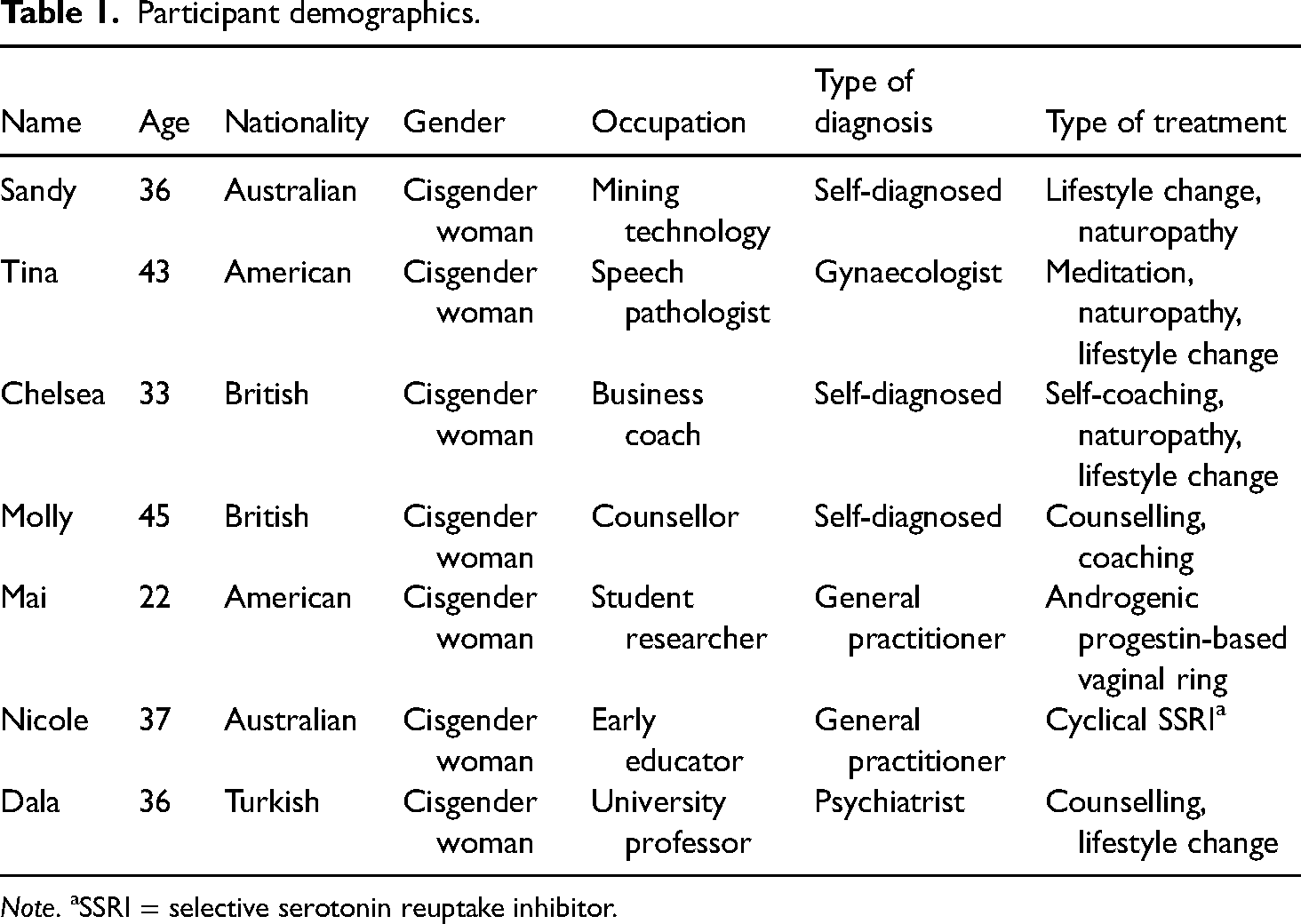
Note. aSSRI = selective serotonin reuptake inhibitor.
In-depth narrative interviews took place via Zoom, each lasting roughly 1 hour. Some of the questions I asked included: (a) what PMDD means for the participant, (b) their personal journey and history of PMDD, (c) what has influenced their journey out of PMDD, (d) where the participant is now in their relationship with PMDD, (e) how they view PMDD now, and (f) how they understand this transition. Interviews were recorded, transcribed, deidentified, and issued to participants for member-checking. The data were then analysed using the Listening Guide (Gilligan & Eddy, 2021; Gilligan et al., 2003). Each aspect of the method is outlined below.
The analytic procedure of the Listening Guide involves sequential readings of the transcripts, noted as “listenings.” The first listening is plot-focused—“attend[ing] to the landscape” (Gilligan et al., 2003, p. 160)—where details of each participant's story are distilled. The second listening is narrator-focused, where the first-person voice is found through the assembling of I Poems: the listing of each first-person word (“I”) and its subsequent verb, sequentially. The I Poem allows the variation of the first-person voice against the plot to be observed. The third and subsequent listenings involve attuning to a distinct voice if present within a single transcript, and following that voice through all other participant transcripts, and as guided by the research questions. Here, the contrapuntal voices are discovered, as each voice is found and followed. The final listening involves composing the analysis, where a “well-supported” (Tolman & Head, 2021, p. 158) interpretation of the narrator's experiences is presented. The researcher brings together all transcripts, illuminating similarities in voices that may have emerged across several interviews, yet also marking distinct differences between them (Gilligan et al., 2003).
Results
Participants’ experiences of PMDD recovery, management, or transformation, and their understanding of this journey, were heard through eight distinct voices grouped under two broad narrative themes, namely:
Within abjection: the voice toward the Other, the voice silenced, the voice of anger, and the voice of agency. Beyond abjection: the voice of action, the voice of surrender, the voice of resistance, and the voice of reembodiment.
Within abjection
The first narrative theme surrounds participants’ initial experiences with PMDD as those of confusion and desperation, alongside anger regarding dismissal from healthcare providers and the necessity for self-advocacy. Based on the data, the term “abject” was interpreted by me to represent PMDD as an experience of disgust and unassimilable nature; that which is estranged from the “I” (Kristeva, 1941/1982).
The voice toward the Other
Descriptions of the weeks when symptoms of PMDD were present in participants’ cycles were similar across all participants at the beginning of each interview: “being in survival mode and doing whatever I had to do to get through a day” (Sandy); “extreme emotional and psychological responses” (Molly); “dark clouds rolling in” (Tina); “absolute death for a good 2 weeks out of every month” (Nicole); and “[the] dark era, a dark and negative time” (Dala). Chelsea describes her experience further: “when I was going through it, I would have been like ‘it's the end of my life. I don’t know who I am anymore. I hate myself.’” Each also acknowledged the divide between “PMDD” and “not PMDD” regarding their sense of self: “it just doesn’t feel like me. I feel like a completely different person” (Mai); “I was a different person” (Chelsea); “it's polar opposites” (Sandy); “flipping off a light switch” (Tina); and “this isn’t normal … this isn’t a normal way to feel … there's something wrong with me” (Nicole). The variation between Self and Other can be noted in an I Poem from Sandy's interview:
Multiple women described a sense of otherness as a singular crisis point within their story of PMDD and PMDD recovery. For some women, this moment was described in a quiet voice, almost a whisper: “I ended up having suicidal ideation, and I ended up spending, like 3 days in a behavioural health facility” (Tina), and would become louder as the interview progressed. Tina's voice of desperation highlights this progression: I don’t normally share this but I’m going to share this … I was driving home, I just had a meltdown. Just, like, screaming at the top of my lungs in the car about how awful I am and how I can’t believe that I just did that to myself and that I was just ashamed and just screaming horrible things to myself in this car. And I’m like, “I just, I just want to drive off the road. I just want to drive myself into a ditch right now.” I was so embarrassed. And there was nobody there to see me … “I cannot, I cannot do this because what happens if there's another time, if this is the farthest I’ve gone, like being by myself and actually wanting to do something to hurt myself, what was next?” That was scary.
Chelsea's voice of desperation bridges private moments and attempts for help: Nothing, absolutely nothing made me want to live during that time. I would just go to bed and hide under the covers, or I’d cut myself or whatever it was … I looked at him [a general practitioner] and said, “I don’t know if I’m going to survive 3 more months.”
For Molly: I was just in the bathroom one day just sitting there … I remember thinking, looking at my wrists and thinking, “if someone says to me that this can’t get better, I would want it to end.” I couldn’t keep living like this because I was too terrified of every single moment.
Moving back into a quiet voice again, “How am I going to make it to my 40s?” (Dala); “I want to be able to know that going into my next cycle, I’m going to come out alive” (Chelsea).
The voice silenced
Experiences of being silenced and the interpellation of silence were common in all seven participants, profoundly illustrated in Molly's I Poem:
Being silenced by healthcare professionals was described similarly among most participants: “I think you’re just having a midlife crisis” (Tina); “You’re just a new mum, take less pressure on yourself … You’ve probably just got a bit of postnatal depression left” (Chelsea), “You’re probably just stressed from school or something” (Mai); and “there's nothing wrong with you based on these things. We can see here, none of these fits. So therefore, there is nothing wrong with you” (Molly). For many participants, PMDD was equated with PMS by their healthcare providers or, like for Dala, healthcare providers just “didn’t really understand anything about it. They didn’t know anything about it.” Participants were initially misdiagnosed with bipolar, borderline personality disorder, depression, postpartum depression, posttraumatic stress disorder, autoimmune diseases, chronic fatigue syndrome, fibromyalgia, polycystic ovarian syndrome, and cancer in the lymph nodes. When asking for a hysterectomy and oophorectomy, Tina describes a gynaecologist saying to her bluntly, “That's not the way that it works. And I’m not going to do that for you.” The option of a hysterectomy was instead described by Molly as a silencing tool: “the gynaecologist said to me, ‘look, you’ve just got to deal with it. It's going to be like this until you stop your periods, or we can give you a hysterectomy. Look, it's just your choice.’”
In conversations with healthcare providers as well as in their social life, many women described periods of self-silencing and a sense of self-doubt: “I lost my confidence and I stopped saying what I really felt and what I really thought” (Chelsea); “I stopped talking to people” (Sandy); “It also took me a really long time to be able to describe these feelings” (Tina); and “it's kind of just like having to doubt yourself or analyse every little thought or everything that you’re feeling” (Mai). When I asked how this experience was for participants, answers presented themselves: “It's meant I have felt like a victim. I felt misunderstood” (Molly); “I feel misunderstood mostly … I was incredibly defeated” (Tina); and “For 3 years, I was on my own … I was on my own” (Dala). Two participants explicitly described these experiences as feeling “gaslit”: “‘I don’t think you have really had PMDD’ [said a doctor] almost gaslighting me … pushing women into not feeling heard, feeling kind of medically gaslit” (Chelsea), and feeling “gaslit by the medical world, by people around me” (Molly).
The voice of anger
Moments of anger were experienced both in the narratives and in their retelling. In each interview, the participants expressed anger regarding the dismissive, uninformed, or misinformed advice from health professionals, alongside exhaustion from ongoing self-advocacy. “There was no actual conversation with me!” Molly explains about her experience of dismissal, “…nobody really spoke to me about what the symptoms were, why it was happening, or where it was coming from, or how it would develop.” Similarly, Nicole says, “I’d gone in thinking she was just going to take one look at me and put me back on birth control or send me for a blood test or just not validate my feelings whatsoever.” Compared with Mai's description of being prescribed medication, “they didn’t run any hormone tests. They didn’t do anything.” Alongside Dala, “I kept telling the doctor, like, those antidepressants, they’re not going to work for me! I’m not a depressed person.”
“I knew what it was,” Tina states, “And he was like, ‘Yeah, you have this, but, you know, you’re making bad choices.’ And I’m like, ‘Well, I know I’m making bad choices, but I can’t stop myself from making bad choices!’” Knowing “what it was” (PMDD) and still being dismissed was a common experience among participants: “They’re [healthcare providers] like, ‘oh, PMDD, that's just PMS’” (Mai); “That was not PMS, because PMS does not make you want to kill yourself during that time!” (Chelsea). Here, advice commonly given for alleviating PMS symptoms, such as walking and altering diet, was further commented on: “I literally couldn’t some days, I couldn’t move, I couldn’t get dressed” (Sandy); “I’m just like … that's bullshit! … It just feels like a punishment” (Tina).
Experiences of healthcare providers being uninformed about PMDD were also shared: “They didn’t really understand anything about it. They didn’t know anything about it … In fact, just like many cases, he misdiagnosed me” (Dala); “He was Googling it,” Chelsea said about a general practitioner who told her “‘well, it doesn’t really lend itself neatly to gynaecology, and it doesn’t lend itself neatly to mental health. We’ll refer you. See if anyone's interested in this kind of thing.’” For Chelsea and Molly, these experiences culminated in anger and exhaustion: I went to CBT. That didn’t really work for me. I still felt shit. I went to talking therapy, still felt shit. I remember just turning up to the doctors, just crying and crying and crying … I went to talking therapies, went to a psychiatrist, went to all these different places! (Chelsea) I swear to God, I just wanted to just fire all my doctors! Basically. I wanted to say to them, “Just stop fucking pretending you know it all. Stop pretending that you’ve got all the answers and check in! If you know you’re going to put me on something … You know this history! Don’t just leave me for 3 months!” (Molly)
Anger directed to broader, societal systems related to womanhood was also heard. “It's a massive atrocity on our society and on the medical system … I could see all these social constructs and systems that were pushing women into not feeling heard,” Chelsea states. “And really the people who experienced it are marginalised because they are either women or nonbinary … and therefore we’re not cis men. And so that makes me angry,” Molly continues. “Especially as women were told to put on a smile, don’t complain, don’t get angry. And actually, there are things that we should be angry about!” (Chelsea). “I see that people are actually committing suicide because of it! People are dying because of it! So that's a real issue that needs to be challenged” (Mai).
The voice of agency
Agency, inclusive of self-advocacy, was a distinct shift throughout most participants’ narratives and interviews themselves. Louder voices talking with and talking back to healthcare providers, within professional life, within PMDD support groups, and to themselves, were heard. Movement between silence and agency—between being told and telling—is illustrated in Molly's I Poem, as following from her I Poem quoted above:
The voice toward healthcare professionals was most prominent: “I said, ‘listen, I’m not going to be able to make it’” (Dala); “I need you to listen to me because you know a lot about what you’re talking to me about, but I know a lot about me” (Molly); “I’m like, ‘I already have a psychiatrist, I don’t need to see someone who doesn’t know what they’re talking about’” (Tina); “I told my gynaecologist ‘I might want a hysterectomy and I’ll let you know when I want one. I’m not waiting for you to tell me’” (Molly); “So I went to her, and I walked out of our session mid-session. I said, ‘I’ve heard you. Now I don’t want to hear anymore’” (Molly); “In that appointment, I just went, ‘you know what? I have no faith in this route of healing anymore. I’m just going to do this myself. I’m going to find another way’” (Chelsea). Molly explains further, “I have to be my own advocate … What they [healthcare providers] can do is provide me with information about things they’re educated in, and then I can provide them with things that I’m educated in, which is me.”
When I asked how participants understood their transition from PMDD to where they were now, softer, more private moments of realising agency were expressed. Tina pauses to answer: “That it was life or death. And I made a decision. And I chose life.” For Molly, “My journey out of it was starting to really, really honour the value of the knowledge that I had about myself.” Chelsea moves this realisation of agency into action: “It's a real watershed moment when a woman realises, actually they need to come first.”
Beyond abjection
The second narrative theme surrounds participants’ reflections of moving “beyond” PMDD. Descriptions of action in self-help, surrender to symptoms, alongside resistance to dominant narratives regarding PMDD and the menstrual cycle, were equally heard. A final voice, that of reembodiment and deep appreciation for the body, was also clear. Based on the data, I interpreted the term “beyond abjection” as representing the malleability of PMDD and PMDD symptoms as a process of moving beyond abjection.
The voice of action
Action was described, in an assertive voice, as a process of reflection and change. Experiences of action arose following experiences of agency. Both the changes participants had made in their lives in relation to PMDD and the understanding that they had the ability to make such changes had each allowed for the malleability of symptoms themselves. For many participants, this meant “adjusting [their] lifestyle completely” (Sandy) to fit around their menstrual cycles, alongside a process of letting go of “things that didn’t serve [them]” (Chelsea), including overworking themselves, tumultuous relationships, and stressful jobs. For Sandy, this began by asking herself “What do I value?” “I just literally did a big overhaul of everything in my life … You kind of stock take all your relationships and what you’re doing with your life and what’s helping you and what’s dragging you down.”
Chelsea describes PMDD as a “vehicle for a huge amount of change,” a “rebirth” into her adult life, “shedding so many layers.” The voice carries through most participants: “I’ve changed my diet. I’ve changed my lifestyle … I’ve been trying to do everything I can,” Molly states. “I also changed to a less stressful job” (Sandy). Dala, too, felt the “need to cut back on those toxic relationships, need to cut back on bad foods, bad people, to fix my relationship and ties with family, trying to build it, construct it.” Similarly, Chelsea describes, “through the journey, you unpick so many other toxic things in life and then reframe those and reconstruct them for yourself.” For Sandy, this change was largely reflected by understanding and honouring the differing phases of her menstrual cycle: “if you have a restful PMDD phase that sets you up for a successful bleeding phase and then a successful cycle.” Hearing this, Sandy now aligns her work schedule with her menstrual cycle: working from home in the days leading up to menses, and scheduling meetings and events around the time of ovulation. She also states, “The main thing was releasing that pressure to have things done” (during her luteal phase).
Many participants describe an intense phase of research after their experience of noticing symptom cyclicality and discovering the term PMDD, describing this action as due to lack of resources or knowledgeable healthcare providers: “I had to find out so much stuff on my own … there's not a whole lot of research, evidence, or advice” (Sandy); “That was the only information I got, and so everything after that, I learned from the Internet” (Tina); “And so I read loads of books, like Fix Your Period, In the Flow…” (Chelsea); “I read all the literature on IAMPD [International Association for Premenstrual Disorders]” (Tina); “I went searching and I found a lot of extra information. There were Instagram accounts out there dedicated to PMDD” (Nicole); “So I just keep learning more and more about my body, about how this works” (Mai).
The voice of surrender
Descriptions of surrender were common amongst some participants when discussing how they now manage symptoms of PMDD that may arise: “It's definitely something that's always like in the background in my life … in the back of my mind” (Mai); “I’ve had to get used to understanding my experience of the extreme lows around my period” (Molly); “so now I have to sit with some really icky feelings, and just know that they’re going to pass” (Tina). To Sandy, surrender looks like, “literally just giving up, like going, ‘okay, we’re at this cycle, just focus on rest and sleep and it will end in a week or so … Just hermit down and plan everything from day one onwards.’”
Nicole describes surrender as gentleness toward herself, giving herself “permission to be annoyed and be snappy and be tired and just kind of, I guess, educate people a little bit more about it.” Descriptions of acceptance towards oneself and one's body were also heard: “I just have grown a lot to accepting myself and accepting PMDD, seeing how I can fit it in my life and live around it, plan my life around it” (Mai). For Dala, this voice was most prominent: So, I have fully embraced and accepted it. I accepted that I am not going to be that person who was going to do 10,000 things in their schedule … So, my body wants me to slow down. So, I’m just going to slow down, and lie on the bed, and enjoy the moment of not doing anything. It [PMDD] brought me that. And I’m okay with not doing anything, just simply resting my body. I’m completely okay with that.
The voice of surrender was also heard as humour. Ending the interview, when I asked how participants viewed PMDD presently, most used a single, externalised description, followed by a laugh: “It's such a huge beast” (Chelsea); “It's a devil I know more about” (Molly); “It is a loss, but it's not my enemy, it's just the way my body is” (Dala); “I mean, we’re frenemies, I guess … It's like just having that visitor that you really wish would not come” (Tina).
The voice of resistance
Parallel to surrender and acceptance were strong voices of resistance to suffering, the idea of recovery as possible. This voice was relaxed, unfazed, yet confident: “It just doesn’t affect me as much” (Sandy); “Honestly, I don’t really have PMDD that much … I feel better, and I don’t have PMDD symptoms anymore” (Mai); “It just feels a lot more like this is what people can manage … a normal amount … It really doesn’t affect my day to day life the way that it did” (Nicole); “It's not scary to be alone anymore because I’m not facing those suicidal feelings” (Tina). Chelsea discusses recovery during the creation of her coaching business for others with PMDD: By the time I actually came to launch my membership, I didn’t have PMDD anymore. And it was 3 months, and I just didn’t have it. I just didn’t have it anymore. And I was like, I could work through the month, didn’t feel suicidal. I didn’t have the five of the eight symptoms that you need. It had all changed.
Chelsea goes on to discuss how she views PMDD at present: PMDD, for me, is just the beginning of a journey for bigger discovery into what is going on beneath the surface of a woman in a woman's life. It's so much to me, it can be used for so much good in terms of I’ve seen people completely transform their lives, including, obviously, myself.
Shared amongst other participants was the passion for sharing knowledge about PMDD and assistance for those suffering. Mai explains, “It put me on the course of my career goal to go into public health and women's health, so it's always something that has kind of directed me,” she continues, “[it is] the reason why I get out of bed in the morning.” For Molly, this passion exists in her counselling practice and toward her children, “because we all should be aware.” Similarly, Nicole “hope[s] that other people hear more about it … for high school children to be getting educated on all the things that come with the cycles of women.” Mai reflects on her experience as a whole: “I’m lucky to have had this experience because now I can help educate others and help other people … being able to empathise with other people has been a real gift.” Molly summarises: I believe that if we had a more holistic approach to education or for practitioners, and we had more advocacy for people to be believed around their own experiences around their bodies, and we were more affirming in the way that we treat humans generally around their bodies and their health, that a lot of this would have been avoidable.
Many participants discussed resisting the narrative of suffering due to the menstrual cycle more broadly. Chelsea, reflecting on previous experiences of PMDD, and referring to how her PMDD clients were before starting therapy, mentions the idea of suffering as due to PMDD being “entrenched in [one's] identity” (Chelsea). Chelsea views her PMDD clients as “not feeling connected to who they really were … real misalignment between what they wanted and who they were and how they were showing up and what they were living with.” Mai reflects on her experience with healthcare providers: We kind of like get into that mindset where it's like, “this is my life and I just have to deal with this,” and honestly, I mean, of course, because the doctors tell us that too, “this is normal, something you have to deal with.”
Mai goes on to speak of how she rejects the above mentioned notion from medical providers: “I don’t have to suffer. I don’t have to accept that this is my life and live like this.” For Nicole, “I have probably 10 more years of periods ahead of me potentially, and I don’t have to have 10 years of being angry for half my life.” The idea of “reframing” and recontextualising experiences and meanings of the menstrual cycle concluded most interviews: “so being able to reframe PMDD is a huge part of the journey for me,” Mai states. Again, for Molly, this reframing begins for her daughter: “I feel prepared to have started changing the narrative for her at least.” And for Chelsea, for her clients: “[I am] changing the perspective, changing beliefs around what it is to be a woman.”
The voice of reembodiment
Embodiment—the making tangible of something usually intangible such as an idea or feeling, a “hum” of experiential integration, the conscious cohesion between one's psychological and physiological states—was the final voice heard throughout the participants’ interviews. Described as a process, Sandy begins “to reflect and go, actually, what's my body telling me … I actually had to start listening to my body for the first time.” As “a reminder ” for Dala, “A sign. It's my signal saying ‘Slow down. Take care. Take deep breaths’ … My body wants me to slow down, so I’m just going to slow down.” For Tina, “it's about timing and paying attention.” For Molly, embodiment was expressed regarding her work with a coach: “my body was telling me this was working for me.” For Chelsea, PMDD gave her “motivation” to listen to her body, “because we’re often told, I’ll just take this pill and get rid of the symptom, just ignore it.” She now uses her menstrual cycle “as a way to know how healthy I really am and how happy I really am.” Molly mirrors: “[I] was getting in contact with my inner wisdom … I stopped trying to let Western medicine take over … I started letting the process take over.” Chelsea closes her interview, “I didn’t need somebody actually, in the end, I just needed myself.”
Here, embodiment, the opposite of the Other, was particularly heard from Chelsea and Molly. Chelsea now views her “unique physiology” as a “superpower rather than seeing it as a weakness.” She continues, “before that, I was living in spite of being a woman rather than being proud of it.” Chelsea explains her purpose now is to “empower” other women “with the confidence to investigate their own bodies and to be proud of their bodies and reconnect with who they are … feeling love for themselves.” For Molly, this voice was heard through tears: I went through this whole process of feeling such deep gratitude to my body … falling back in love with me … becoming whole again, I guess in terms of having gratitude and acceptance for the complexity of the role my uterus has played in my life and the role that hormones have played in my life. And I’d gone from visualising my uterus as this broken thing I wanted gone … to really making peace with it and saying thank you to it and honouring it, and then also trusting myself.
Discussion
The theoretical proposition of PMS as a social construction, thus allowing for change or negotiation, has been alluded to in previous literature (King & Ussher, 2012; Ussher, 2002; Ussher et al., 2014). However, qualitative research on individuals’ experience of plasticity in PMDD is sparse. In my study, I have attempted to address this gap, providing in-depth narratives of individuals who have moved into a space of recovery, management, or transformation of PMDD. In the following discussion, I highlight how my findings link to existing literature, alongside novel findings.
My findings align with prior qualitative studies of personal experiences of PMDD and PMS, with initial narratives describing the “split” between the Self and PMDD (Chrisler et al., 2014; Hardy & Hardie, 2017; Osborn et al., 2020; Swann & Ussher, 1995; Ussher, 2002, 2003, 2004), as well as self-silencing and self-surveillance also described by my participants (Chrisler et al., 2014; Maji & Dixit, 2019; Ussher, 2004). In this regard, Ussher (2004) discusses a cycle of rupture and overrepair during premenstrual change: a break in “normalcy” due to premenstrual symptoms prompts heightened self-policing. This was evident in my study, heard in initial cycles of Self/Other splitting and the interpellation of silencing from healthcare professionals. My findings also extend Ussher's (2004) by acknowledging the voice of anger in participants’ accounts, as a resistive and celebrated rupture that prompted recovery.
Further, Ussher’s (2008) and Ussher and Perz's (2013) research challenges dominant discourse around premenstrual change as being solely an internal pathology. My findings stand both in support and in contrast to this argument, reflected in the distinction between voices of surrender, those who accept and appreciate their bodies’ needs during PMDD symptoms as an ongoing process; and resistance, those who rebel from the notion of PMDD as unchangeable. My findings therefore uphold Ussher's (1997) MDI approach, acknowledging the biological aspects of PMDD as equal and parallel to discourse and the individual's perceptions. Some of my participants aligned with a purely biomedical model of PMDD as cause for their symptoms, but also reflected a sense of negotiation of their symptoms in the form of acceptance and appreciation.
Overall, my research supports evidence of a severe lack of patient care for those experiencing PMDD across multiple contexts. Participants’ experiences with healthcare providers align with those in Osborn et al.’s (2020) qualitative analysis. They similarly identified consistent misdiagnoses and dismissal, and gaslighting behaviours from healthcare providers, leading participants to feelings of desperation. Instead, like for Osborn et al.’s (2020) participants, self-awareness, self-education, and menstrual cycle tracking were reported as significant to recovery.
My findings further point to the lack of integration of the psychosocial into treatment and support, affirming Bryant et al.’s (2014) call to integrate mental health care in gynaecological settings. In a similar vein, Craner et al. (2014) highlight a disconnect between research and practice for PMDD. Research on support options for PMDD neglects the psychosocial aspects of health, lifestyle change, and alternative treatments from biomedical guidelines. It also lacks accounts from those who have experienced PMDD themselves. In my study, participants’ narratives highlighted the efficacy of organising one's life around the varying phases of the menstrual cycle—alongside suggestions from popular psychology and self-development books that herald menstrual positivity—but such strategies are not identified in scholarly research on PMDD.
While the findings I have reported in the narrative theme of within abjection largely align with existing qualitative research on PMDD, the narrative theme of beyond abjection—encompassing the voices of action, surrender, resistance, and reembodiment—provides novel insights. What I heard from my participants was that movement toward a space of recovery, management, or transformation of PMDD is attainable, with PMDD being a negotiable and therefore plastic experience for them. Voices of surrender depart from research accounts of PMDD as a fixed experience of distress and debilitation. Appreciation of what surrender and acceptance provide contrasts with dominant discourses of the menstrual cycle as an interruptive and constrictive experience. For my participants, slowness during the luteal phase was viewed as positive and powerful, spoken about with humour. Voices of resistance further challenge the view of premenstrual change as a pathology in isolation, portraying it rather as a material–discursive–intrapsychic phenomenon (Ussher, 1996, 1997, 2000) that has the possibility to be reconstructed as a positive experience. My study expands this observation from research on PMS to PMDD as well. Finally, voices of reembodiment suggest that interpellated narratives of menstrual suffering can be resisted and reversed. Descriptions and practices of reembodiment discussed by participants, therefore, stand in opposition to prior experiences of interpellation. Participants were able to move through a process of feeling estranged from experiences with their menstrual cycle to be able to face their Other, and reembody what was once a cause of pain to now become a source of power: a process of moving beyond abjection.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Author Biography
![]() . She has completed a Master of Counselling degree at the University of Notre Dame and is currently completing a PhD at Western Sydney University Translational Health Research Institute under the supervision of Dr Alex Hawkey, Prof Jane Ussher, and Dr Samantha Ryan. Her research focus is on developing a psychotherapy program for premenstrual change.
. She has completed a Master of Counselling degree at the University of Notre Dame and is currently completing a PhD at Western Sydney University Translational Health Research Institute under the supervision of Dr Alex Hawkey, Prof Jane Ussher, and Dr Samantha Ryan. Her research focus is on developing a psychotherapy program for premenstrual change.