
Abstract
In this paper, we sought to give voice to the unspoken issue of mothers’ disintegrative responses—that is, intrusive thoughts and dissociative experiences—in the context of infant care. Three methodologies were employed: (a) in-depth interviews were conducted with 23 Israeli women up to 3 months postpartum; (b) 126 Israeli women up to 12 months after childbirth responded to an open-ended questionnaire; and (c) a clinical case study was performed. Mothers referred to intrusive thoughts as “attacks,” and related primarily to three themes: fear of losing their grip, aggressive fantasies, and guilt and shame. Dissociative experiences were described as vague and elusive, with three major themes emerging: detachment, disorientation, and helplessness. We argue that the findings correspond with psychosocial approaches whereby disintegrative responses may be an indication of maternal ambivalence and a reflection of “contagious arousal” in which the mother identifies with the experience of the infant. The findings offer a new direction to clinicians working with mothers by suggesting that the mother's openness to these responses may be an opportunity for her to acknowledge subjective and repressed parts of herself and undergo a process of reintegration out of disintegration.
Early caregiving can arouse a broad spectrum of feelings in a mother, ranging from harmony and connectedness to her infant to helplessness and negative emotions directed toward herself, the infant, and her surroundings (Graham et al., 2002; Huth-Bocks et al., 2016). The intensity of these feelings may be expressed through two types of disintegrative responses: (1) intrusive thoughts, that is, uncontrolled thoughts and images with unwanted content (Fairbrother & Woody, 2008); and (2) dissociative experiences, that is, transient or recurring experiences of disconnection or discontinuity in the integration of consciousness, memory, identity, emotion, and perception of body representation (Lyons-Ruth, 2015; Solomon & George, 2011).
Intrusive thoughts in the postpartum period generally take the form of unwanted aggressive reflections and images relating to harm to the infant caused by an external accident or by the mother herself (Brok et al., 2017; Buchholz et al., 2020). Although these thoughts do not usually constitute a clinical warning sign of a pathological disturbance or any actual injury the mother may cause (Collardeau et al., 2019), an increase in their frequency, duration, intensity, and consequent distress may indicate the development of obsessive-compulsive disorder (OCD; Buchholz et al., 2020; Fairbrother et al., 2018). Similarly, early infant care may trigger dissociative experiences in the face of the helplessness the mother may feel in the maternal role (Huth-Bocks et al., 2016; Solomon & George, 2011). In addition, dissociative experiences may be evoked by a traumatic birth experience, past traumas, or the increased fatigue that characterizes the postpartum period (Giesbrecht & Merckelbach, 2004; Jacobvitz et al., 2006; Oh et al., 2016; Thiel & Dekel, 2020).
Studies examining dissociation in the context of motherhood, and specifically in the postpartum period, are scarce. Moreover, the few existing investigations have employed two main methods: self-report questionnaires measuring the mother's general dissociative experiences (e.g., Lev-Wiesel & Daphna-Tekoah, 2010; Oh et al., 2016) and a coding system based on observations of mother–child interactions (Jacobvitz et al., 2006; Main & Hesse, 2006).
The usual range of intrusive thoughts and dissociative experiences in the context of infant care was recently examined by means of a self-report questionnaire (Chasson & Taubman – Ben-Ari, 2022b), and found to be higher among mothers who reported insecure attachment and childhood trauma (Chasson & Taubman – Ben-Ari, 2022a). However, the body of evidence regarding intrusive thoughts as experienced and described by mothers, as well as such descriptions of mothers’ dissociative experiences, is lacking. This knowledge could contribute to a deeper understanding of the onset and manifestation of these phenomena in reality. The current study seeks to help fill that gap.
Overall, mothers’ subjective experiences have been largely overlooked, despite the fact that the mother–infant dyad is at the root of most psychotherapeutic theories. In general, classical psychoanalytic theories relate to the infant as experiencing unintegration arising from necessities, desires, and feelings that constantly appear and disappear, with the mother containing, responding to, and holding these strong feelings for the infant (Bion, 2013; Winnicott, 1984). Furthermore, according to attachment theory, in order to ensure the prosperity and positive development of the infant throughout life, the mother must be available to them, responding to their needs sensitively and appropriately (Ainsworth, 1979; Bowlby, 1982).
Particularly little attention has been paid to the fact that besides containing the infant's feelings, the mother herself may experience painful and mixed feelings in view of the complexity entailed in mothering an infant. Consequently, not only is this issue not well understood, but mothers’ negative feelings toward their infants remain hidden and secret, similar to parents’ negative feelings toward their children in other contexts (Erel-Brodsky, 2014).
New psychosocial and feminist theories have sought to highlight the significance of the maternal experience and subjectivity. According to these theories, the barrier to removing the taboo surrounding the mother's subjectivity lies in social idealization and the fantasies that present the mother as “perfect,” a woman who always puts her children's needs before her own and has no negative thoughts or feelings toward them (Benjamin, 2013; Chodorow & Contratto, 1982). This idealization, which is prominently reflected in the parental culture of “intensive mothering” (Hays, 1996), prevents both society at large and mothers themselves from giving room to the wide range of feelings and thoughts that appear to be inconsistent with the image of the perfect mother (Raphael-Leff, 2010). In addition, while the binary view of mothers is associated with greater pathologizing of a mother who expresses negative or hostile feelings toward her child, the feminist view regards ambivalent feelings and thoughts as natural, healthy, and essential for understanding maternal subjectivity.
According to Raphael-Leff (2010), ambivalence is inherent in the maternal experience, and can be expressed in a variety of feelings and orientations. Raphael-Leff (2010) describes, for example, mothers who identify with the totality of motherhood, for whom acknowledging natural flaws in their maternal functioning causes feelings of anxiety and guilt. Other mothers may feel exploited and persecuted by the needy infant and the sense of loss of their autonomy. Additionally, according to Raphael-Leff (2010), specific factors can intensify conflict in mothers, such as unresolved traumas from their past or the experience of “contagious arousal” inherent in infant care. “Contagious arousal” is the term used to describe the emotional state that can be transmitted from the infant to the mother during their interactions. It encompasses the mother's exposure to the infant's raw and nonverbal communication, as well as primal and primary substances like milk, urine, and blood. These sensory experiences can evoke repressed, intense, and bewildering emotions and memories. In line with this concept, the theoretical notions of intergenerational transmission of attachment and childhood relational trauma relate to early and unresolved experiences of insecure relationships with the caregiver and adverse childhood events as “ghosts” that flood the mother's current relationship with her infant with pain and memories of her past (Fraiberg et al., 1975).
At the same time, Raphael-Leff (2010) suggests that these intense and unsettling emotions can be a source of development and even healing for the mother, providing an opportunity for her to recognize and process primary and inaccessible contents. Applications of this idea can be found in the therapeutic approaches of mother–infant psychotherapy, which stress the importance of processing the complex emotions and memories that may arise in the mother as a response to infant care, both for the mental health of the mother and her relationship with the infant (e.g., Baradon et al., 2016; Lieberman et al., 2020).
In a similar vein, Parker (1995) identifies parallel processes in the mother and the infant, contending that like the development of the infant's ambivalence and ability to mediate between and combine their love and hate of the mother, the mother develops the ability to bear conflicting emotions toward the infant. In other words, the mother's recognition of her negative feelings is not only healthy, but also crucial for her personal and subjective development.
In line with Parker's (1995) perspective, Baraitser (2009) suggests that the often-painful moments of disruption that mothers experience during childcare have the potential to enable them to acknowledge a wide range of emotions and develop a creative and renewed awareness of themselves. She argues that the mother should not attempt to overcome or control ambivalence and feelings of disintegration, but rather accept them as an inherent part of her subjectivity.
Relying on the psychosocial theories outlined above, Murray and Finn (2012) analyzed the reports of mothers experiencing thoughts of harming their infant. They sought to examine whether these thoughts serve as a creative impulse that can be constructively incorporated into mothering and maternal subjectivity. Here, and in other studies of mothers’ intrusive thoughts (Boyd & Gannon, 2021; Burton, 2021; Meehan et al., 2021), it was found that mothers described their thoughts as related to ambivalence toward the maternal role, the heavy responsibility of caring for a helpless infant, and painful feelings such as shame, guilt, and loss. While some of these studies investigated the intrusive thoughts of women diagnosed with OCD (Burton, 2021; Meehan et al., 2021), others focused on the experience within a normative range (Boyd & Gannon, 2021; Murray & Finn, 2012). All of them, however, shared the common goal of removing the taboo surrounding this issue and presenting the lived and subjective experience of mothers.
Nevertheless, the attitude to mothers’ disintegrative responses remains ambiguous, both in research and clinical literature, and little is known about their normative expression. In addition, to the best of our knowledge, no previous study has considered these experiences in the context of infant care. The present study therefore sought to give voice to the unspoken issue of mothers’ disintegrative responses in the context of infant care, focusing on intrusive thoughts and dissociative experiences. By combining theoretical approaches to maternal ambivalence and subjectivity with mothers’ descriptions of their experiences, we aimed to gain new insights that would lead to a deeper understanding of the subject, both clinically and empirically.
The present research
Our study uses three data sources, namely (a) in-depth interviews, (b) responses to an open-ended questionnaire, and (c) psychoanalytic analysis of the clinical case of a mother experiencing disintegrative responses. We conducted a grounded theory analysis of the first two data sets, generating two categories for explaining the experience of maternal disintegrative responses in the context of infant care: (1) intrusive thoughts and (2) dissociative experiences. This phase of the research is presented in Part 1 below. These two categories were then refined through application of a clinical case study, producing two main theoretical concepts (see Figure 1): (a) maternal disintegration as a response to ambivalence, and (b) maternal disintegration as a response to “contagious arousal” or projective identification, which we explain further below.
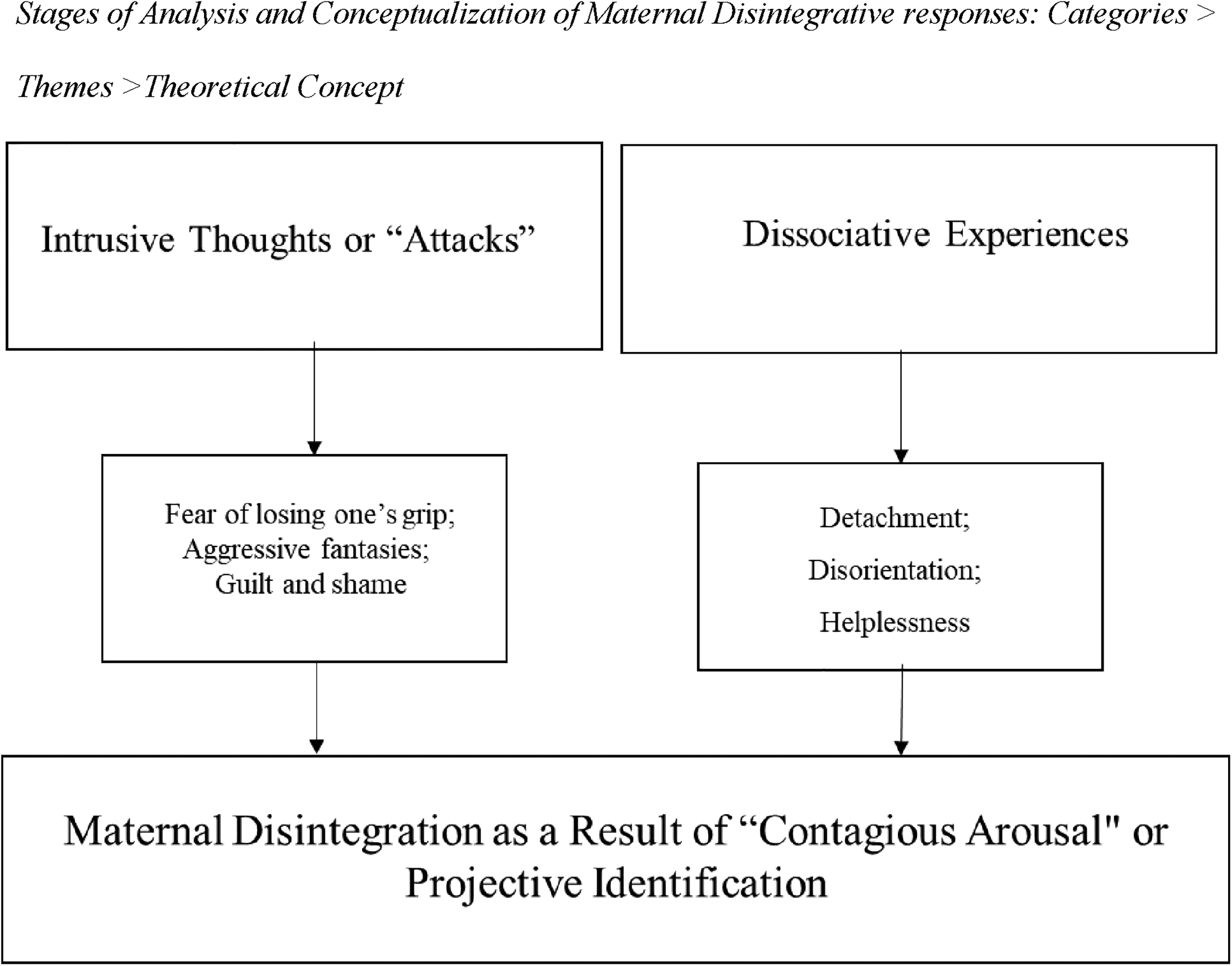
Stages of analysis and conceptualization of maternal disintegrative responses: Categories > themes > theoretical concept.
Part 1: Mothers’ experiences
In-depth interviews and open-ended questionnaire
Approval for the study was granted by the Bar-Ilan University School of Social Work’s Review Board. In Phase 1, which is part of a larger project that deals with mothers’ experience of their devotion to their infant in the postpartum period and some of whose findings have previously been published (Chasson & Taubman – Ben-Ari, 2020), open in-depth interviews were conducted with 23 mothers. The participants were recruited via an invitation posted on social media forums for mothers, asking for women who had given birth in the past 3 months and were willing to be interviewed at home or elsewhere of their choosing. The criteria for participation were that the woman spoke fluent Hebrew, had a child less than 3 months old, and was still on maternity leave so that she was mainly occupied with caring for the infant.
All the participants chose to meet with the researcher in their home together with the infant. Before beginning the interview, participants were informed that it would be audio-recorded for purposes of transcription and analysis, which would be performed by the researchers alone, and were assured confidentiality and anonymity. In light of the sensitive topic of the study, they were also told that should they feel distressed during or after the interview, they could contact the researchers for help or referral to treatment in a specialized clinic. In this manner, we sought to encourage the free and authentic expression of complex thoughts and feelings on the one hand, and to assist mothers who found the subject particularly distressing in receiving additional psychological counseling or treatment on the other. Following this introduction, the women were asked to sign an informed consent form.
The interviews lasted about 60–90 minutes and were conducted by the first author as an unstructured conversation with no preset interview schedule. The participant was asked to describe her experience of caring for her infant. The ensuing questions were aimed solely at clarifying what she had said.
The interviews in Phase 1 contained several descriptions of intrusive thoughts and dissociative experiences in the context of infant care. However, since the women were asked about their experience of caring for the infant in general, we decided to recruit additional participants in order to expand the data obtained in the interviews and relate specifically to intrusive thoughts and dissociative experiences. Therefore, following approval from the university's Institutional Review Board to expand the study, in Phase 2, we posted a further invitation on social media forums calling for women who had given birth in the past year to participate in the study, and including an electronic link to the questionnaire. The questionnaire consisted of several sociodemographic items and two open-ended questions, namely:
Since giving birth, have any unwanted or threatening thoughts suddenly come into your mind when you are with the baby or caring for him/her? If so, please describe these feelings and thoughts and give examples. Since giving birth, have you felt a sense of confusion and/or momentary or continuous detachment from yourself and/or from the infant when you are with the baby or caring for him/her? If so, please describe these feelings and thoughts and give examples.
In both questions, participants were asked to relate freely to any such experiences or thoughts.
Participants
The age of the 23 women interviewed in Phase 1 ranged from 23 to 40 years, and the infants’ age from 1 to 3 months. All the women were on maternity leave at the time of the interview. They all resided in the center of Israel, had an academic education, and held full- or part-time jobs. For eight of the women, this was their first child; for ten of them, it was their second child; for four, it was their third child; and for one woman, it was her fourth.
In Phase 2, of the 360 women who opened the electronic questionnaire, 126 completed it in full (35% response rate) and were included in the sample. The relatively low response rate might stem either from the sensitive nature of the questions or from the fact that some women found them too complex or irrelevant to their personal experience. In the final sample, participants’ age ranged from 20 to 47 years (M = 31.93), and infants’ age from 1 to 12 months (M = 5.64). All the mothers were Jewish, and most were married (92.2%) and had an academic education (80%). In terms of employment, just over half (54.3%) were on maternity leave, and the remainder worked at full-time (17.3%) or part-time (15.2%) jobs. The majority of the women already had older children (70.2%), with the number of children ranging from one to eight (M = 2.50).
Data analysis
First, preliminary thematic analysis of the interviews and the responses to the open-ended questionnaires was manually conducted by two of the researchers (M. Chasson and O. Taubman – Ben-Ari). In this stage, we performed open coding on the transcripts, coding each theme related to the subject under investigation. In the next stage, following Strauss and Corbin (1990), grounded theory analysis was implemented in an iterative process through inductive and deductive thinking (Chun Tie et al., 2019). More specifically, we conducted axial coding to identify the connections and differences between the themes, and then used selective coding to define two core categories. Next, we identified a comprehensive framework for all the themes that had led to the definition of the core categories in order to produce a theory grounded in the data that had explanatory power (Birks & Mills, 2015). As a result of this process, we developed a new inclusive theoretical concept that provided a suitable explanation for the experience of disintegrative responses among mothers in the context of infant care.
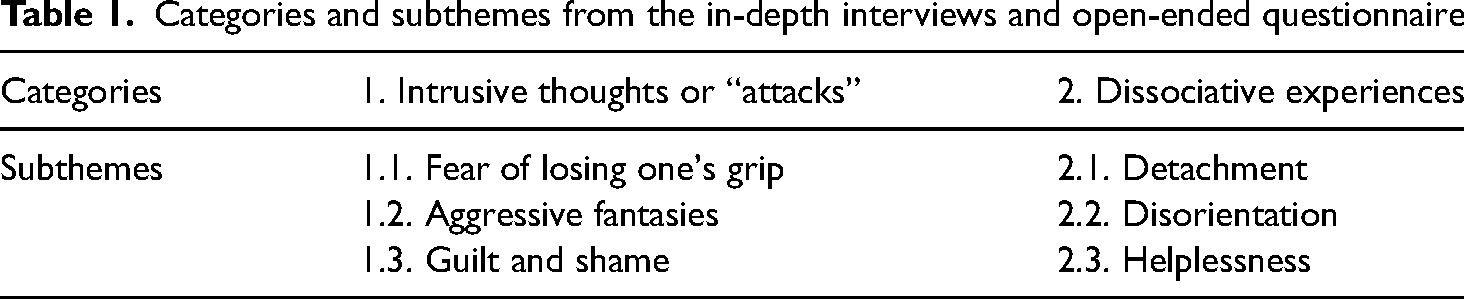
As presented in Table 1, in our analysis, we noted references to several aspects of disintegrative responses that could be grouped into two core categories: (1) intrusive thoughts, described as “attacks”; and (2) dissociative experiences, depicted as vague and elusive. Below, we present each of these categories along with the themes contained within them.
Categories and subthemes from the in-depth interviews and open-ended questionnaire
Category 1: Intrusive thoughts or “attacks”
This category contains a variety of unwanted and uncontrollable thoughts or images that strike mothers while caring for their infant. These intrusive thoughts are described as “attacks” of intense anxiety concerning the child's well-being and the mother's ability and functioning. They can be divided into three subthemes: fear of losing one's grip, aggressive fantasies, and guilt and shame.
Fear of losing one's grip
A number of women stated that routine activities may evoke uncontrollable fear that they will lose their grip, literally and figuratively, and consequently not be able to take proper care of the child and might even hurt the baby, which may reflect a fear of not being a good enough mother. As one woman described it: To this day it's hard for me to wash him alone. I’m afraid he’ll slip and fall. When I go downstairs with him and he's in my arms I’m really scared. I walk down very afraid that he could suddenly fall. I get him his sterilized pacifier and I think that I could burn him. I put him to sleep and suddenly imagine a closet falling on him. (Mother of a 3-month-old boy, her first child; Phase 1)
This mother describes situations when, although she should be the one holding and caring for the infant, like the infant himself, she becomes frightened and feels helpless. She appears to perceive herself, the baby, and reality as fragile and unstable. In her struggle to contain her thoughts of harming the infant, she projects them onto external objects, such as the pacifier and the closet. Her remarks may indicate ambivalence toward her ability to be a reliable caregiver for the infant, a doubt that “attacks” her suddenly and prevents her from meeting the infant's needs and her own expectations.
For some mothers, it was the act of bathing the infant that aroused intrusive thoughts. As one woman explained: It's the fear of holding something so small in the water. Not to drop him, not to hurt him … not to get water in his mouth, not to drown him. (Mother of a 1-month-old boy, her third child; Phase 1)
Here, too, the mother describes herself as unreliable and unable to bathe the fragile infant. By merely holding the child in the water, she is attacked by nightmarish thoughts. It seems as if she is afraid of literally losing her grip, with the hands that should protect the infant being perceived as unstable and dangerous.
The fear of dropping the infant in other situations was also mentioned by a number of women, as in the following comment: When I’m standing near a barrier where there's a sharp drop on the other side, maybe an upper story of the building near the stairs, I’m afraid that by accident I’ll throw the baby over it. (Mother of a 7-month-old girl, her second child; Phase 2)
Aggressive fantasies
Alongside thoughts that the infant might be hurt accidentally or by an external factor, women reported imagining themselves causing harm to the child. These thoughts were described as associated with, or even stemming from, a sense of helplessness when they feel that they are unable to respond properly to or contain the helplessness of the infant. The mothers spoke of their thoughts of harming the infant while at the same time exhibiting reflective thinking about the reason for these fantasies. This can be seen in the following comments: In the middle of the night when she cries, I have thoughts about what would happen if I threw her out the window. Not on purpose but just because I felt helpless. (Mother of a 10-month-old girl, her third child; Phase 2)
I’ve had thoughts of how easy it would be for me to harm this small creature since she's so helpless … it comes from the shock of my huge responsibility for her. (Mother of a 2-and-a-half-month-old girl, her first child; Phase 2)
Guilt and shame
Mothers also referred to the feelings of guilt and shame aroused by thoughts of passively or actively harming their infant. As the following mothers put it: The thoughts that troubled me were that I might cause my baby pain. It was awful. I had terrible thoughts. I prefer not to talk about them. (Mother of a 5-month-old boy, her second child; Phase 2). I had a fear of forgetting my baby in the car or his falling out of my arms on the stairs. It's an awful feeling because I know I’m a good mother and I take good care of my baby and it couldn’t possibly happen. That's why I don’t understand why [I have those thoughts]. (Mother of a 2-and-a-half-month-old boy, her second child; Phase 2)
The threatening content of their thoughts impairs these mothers’ positive experience of childcare, filling them with doubt about the quality of their maternal functioning and fear that they will fail in their duties, resulting in harm to the infant. They believe that the fact that they have such thoughts is “awful,” and express difficulty dealing with this dissonance or even talking about it.
Another form in which disintegrative responses may manifest are dissociative experiences. Like intrusive thoughts, these experiences represent an upsetting and powerful emotional response to infant care.
Category 2: Dissociative experiences
This category relates to various modes of thoughts and experiences which fit the definition of dissociative experiences. Described as vague and elusive episodes, they can be divided into three subthemes: detachment, disorientation, and helplessness.
Detachment
Detachment was depicted as an episode in which the woman felt that she was not fully present in the moment. This can be seen in the following comment: There might be a situation where I feel that I’m not there for her, but I really try hard. Even if I’m alone and nobody's there, I speak to her. But it's not always 100%. I feel sort of disconnected sometimes. There's a kind of disconnection that I sometimes feel … I can’t explain it in words. (Mother of a 2-month-old girl, her third child; Phase 1)
This mother seems to be waging an internal struggle between the conscious parts of her psyche that want to maintain her presence with her infant, expressed in trying to talk to her, and less conscious parts that cast a shadow over the pleasurable experience of infant care and make her feel disconnected. She senses a barrier that does not allow her to be present, but cannot find words to explain it. Her comments may indicate her frustration at not being able to live up to what she considers the expectations of a “good mother” and be fully present with the infant.
Detachment was also reflected in a sense of acting automatically, without the mother's full awareness and emotional involvement. As one woman explained: He could be crying and I won’t notice it. Let's say I’m changing his diaper or his clothes and he's screaming and I realize later that he was crying all the time. I’m on autopilot, like I’m cold to it. (Mother of a 6-week-old boy, her second child; Phase 1)
This mother describes entering some kind of detached state that seems to block her from hearing and responding to the infant.
Disorientation
Another expression of dissociative experiences is a sense of alienation from the infant or the maternal role, which we defined as disorientation. Although the mothers described this experience as momentary or fleeting, it was far from insignificant for them, as the following examples reveal: It sometimes happens that I look at him and ask myself “Whose baby is this? When is his mother going to come?!” (Mother of a 3-month-old boy, her first child; Phase 1)
It's like there are moments when you’re not her mother. Less of a connection, like she isn’t here, or that she isn’t mine for a moment, a feeling as if she isn’t yours. (Mother of a 2-month-old girl, her third child; Phase 1)
Helplessness
As in the case of intrusive thoughts, several women portrayed dissociative experiences as a response to the infant's helplessness and described the direct connection between this feeling and a dissociative response. Their comments may indicate that both the mother's difficulty with caring for the infant and her identification with her child's helplessness may arouse in her a similar sense of helplessness, causing her to dissociate herself. In the words of the mothers: When he cries non-stop and I can’t calm him down, I feel disconnected from myself and from him. I feel helpless and a need to disconnect. (Mother of an 11-month-old boy, her second child; Phase 2)
When the baby cries and it's not clear what's bothering her I sometimes feel helpless, irritated, and desperate, and I also have a feeling of disconnection. Sometimes it gives me a strong desire to disconnect from her. (Mother of a 1-month-old girl, her fourth child; Phase 2)
A feeling of helplessness may also be indicated by the use of the term “frozen.” As if they were locked in a different world, parallel to the child's reality, the mothers found themselves unable to relate to the infant or comfort them when they were in distress. As one woman described it: There were quite a few times that I felt disconnected. His crying was echoing in my ears and I was apathetic. I wanted him to cry till he fell asleep, alone. I sat over his crib after trying a lot of times and couldn’t understand what he wanted. I felt frozen and I didn’t do anything. I just let him cry in my arms or in the crib. It was terrible. I felt that a bad monster was rising up in me. (Mother of a 5-month-old boy, her second child; Phase 2)
In summary, the participants in the two phases of the qualitative study depicted intrusive thoughts and dissociative experiences as disintegrating, disruptive, and upsetting, and characterized them as “attacks” or vague and elusive episodes. In line with existing studies (Boyd & Gannon, 2021; Murray & Finn, 2012), mothers reported normative episodes of intrusive thoughts about harming their infant. In addition, they described the normative aspect of dissociative experiences, a phenomenon that, to the best of our knowledge, has never been qualitatively investigated. The two categories we generated through our analysis—intrusive thoughts and dissociative experiences—were further refined through application to a clinical case study, producing two main theoretical concepts (see Figure 1): (a) maternal disintegration as a response to ambivalence, and (b) maternal disintegration as a response to “contagious arousal” or projective identification. The case study and resultant theoretical concepts are presented next.
Part 2: Clinical case study
In order to deepen and develop the emergent concepts above, we analyzed a clinical case study in which similar descriptions of intrusive thoughts and dissociation were evident. The patient's approval in writing was obtained for use here, and any identifying details have been obscured. Sharon (not her real name), a patient of one of the researchers (H. Erel-Brodsky), was a young mother in her postpartum period. She, too, reported intrusive thoughts and dissociative experiences. By means of this psychoanalytical reading, we hoped to expand knowledge of how disintegrative responses may appear within the therapeutic context and how, from a psychoanalytical and feminist perspective, they can be addressed.
The case of Sharon: Reintegration out of disintegration
Sharon was 25 years old when she came to therapy. She lived in a rented apartment in the center of Israel, had an academic degree, and worked in a full-time job. She came to psychoanalytic psychotherapy twice a week because of her feeling that she was unable to establish a solid marital relationship.
Sharon described her difficulties articulately. At the same time, however, she was highly emotional and found it hard to regulate her emotions. In the course of therapy, it became clear that she had a complex relationship with her mother, who was apparently coping with pathological grief over the death of her brother. During the first 2 years of therapy, unintegrated parts of Sharon's personality were processed and she became more integrated and better able to contain the full range of her emotions and their intensity. As a result, she decided to have a child, and both she and I believed she was ready to take this step.
Sharon had no trouble getting pregnant. However, toward the end of the second trimester, she began to express the fear that she might not love her baby. She said she had never been fond of babies, so why could she expect to love hers? We talked about her questions about her own mother and how much she felt she had invested in her daughter and in her maternal role.
When Sharon went into the delivery room, she sent me an emotional text. She was in labor for a long time, but the birth was uneventful. When she returned home with the infant, however, her fears were realized. She asked to speak with me over the phone and later came to my office. On the phone she told me she felt as if the feet she was walking on weren’t her own and the hands holding her daughter weren’t hers. It frightened her very much because she was afraid those strange hands would drop the baby. She described waking up in the morning and feeling she was still in a dream or a nightmare. For quite a few minutes she didn’t know whether she was awake or dreaming, and she would ask herself who this creature screaming next to her was.
On the basis of what I had learned about her in the course of therapy, I helped her to ground herself and focus on the things in reality that indicated that she was in the moment, as well as strengthening her maternal abilities. There were times I feared her condition might become pathological. Therefore, during this period, I continued to speak with her at the high frequency of twice a week. Keeping her and her condition in my mind, I sought to bolster her confidence. When she eventually came to my office, she brought her daughter with her. Although the baby was calm at the start of the session, she began to move restlessly in her carriage the more Sharon spoke of her difficulties and anxieties. At a certain point, she looked at me with a similar discomfort, displaying frustration and anger at the baby. Sharon: Something inside me wants to yell at her and cry.
Me: There are times when it's hard to hold an infant in your arms and you feel like you’re both crying babies.
Sharon: I’m scared I’m going crazy, that I’ll do something to her. Maybe I won’t know how to protect her like I wasn’t protected.
The child's crying became ear-splitting. I was angry and wanted her to stop, as if her screams were a personal attack on me. At that moment, I gained a certain understanding of the intensity of Sharon's helplessness and hostility toward the baby, and perhaps of her anxiety and fear of dropping her daughter as well. I steadied my breathing until I was able to think clearly again.
The baby continued to cry, and Sharon and I bent over the carriage together. Sharon smiled at me and I looked at her knowing that her fears were also her way of protecting her child from the painful and unprocessed part of her own personality. Sharon: Do you think she senses how fucked up I am? That I’m so scared? That I don’t know how to be a mother?
Me: There's a part of you that's afraid that if you get too close to her she’ll “catch” your pain and fear. Your maternal instinct at those moments is to push her away. But that's exactly what makes you a good and devoted mother. You’re protecting her from any harm, even from yourself at such times.
Sharon started crying. She took her baby in her arms and comforted her. The baby calmed down, and it seemed as if Sharon also calmed down in my therapeutic arms.
Two months after the birth, Sharon returned to herself and continued to function as a mother. Since then, she has had two more children, with whom she did not have the same experience. In the course of her ongoing therapy, we were able to process her difficulty with motherhood against the background of the lack of a mother she had sensed in her own childhood. She considered the imperfect container she felt she had to offer her daughter and her envy of the baby who was growing up with a good, loving mother of the type Sharon had never quite known. In addition, we discussed how Sharon's receptiveness toward her daughter and her ability to contain the baby's aggression, terror, and helplessness constituted evidence of her impressive strength as a mother.
The upheaval Sharon experienced in the wake of the birth of her first child was intense. At that point, she needed normalization of her feelings and validation of her tumultuous emotions. It was only later that we could draw a line between this experience and the lack she had apparently suffered as a child. We could then process the pain of the transition to motherhood while inside she was still yearning to go back and be a baby who were not required to curb and repress her elemental needs.
During our analysis from both psychoanalytical and feminist perspectives, we discovered a compelling connection between Sharon's clinical case and the findings previously discussed in the first part of our study. Consequently, we propose two main theoretical concepts (depicted in Figure 1): (1) maternal disintegration as a response to ambivalence, and (2) maternal disintegration as a response to “contagious arousal” or projective identification.
Maternal disintegration as a response to ambivalence
Sharon's experience can be understood as an expression of ambivalence. She struggled to remain a subject separate from her infant and feared temporarily merging with her. As a mother, she is required to become an object that sustains her subjectivity in order for her infant to evolve into a subject herself. When her child seemingly asks her: “Object, who am I? Who are you and who are you for me?,” she feels shaken, attacked, and disoriented, and needs to survive these attacks. In Winnicott’s words (1969): The subject [baby] says to the object: “I destroyed you,” and the object is there to receive the communication. From now on, the subject says: “Hullo object!” “I destroyed you.” “I love you.” “You have value for me because of your survival of my destruction of you.” (p. 90)
It took time for Sharon to become this container (Bion, 2013), to let herself merge into a state of maternal preoccupation (Winnicott, 1956). However, as she describes it, to get there, she had to acknowledge the ambivalence inherent in motherhood, and the powerful responses it may evoke.
Maternal disintegration as a result of “contagious arousal” or projective identification
Sharon needed to experience being-in-identification with the infant's projected, threatening, and painful experiences, to let them in and process them in her own emotional world, or what Eshel (2004) refers to as “I-dentification,” that is, experiencing a vicarious existence and the ensuing possibility of being. She was eventually able to contain her infant by means of their convergence, deep interconnectedness, and interpenetrating impact on each other, forming a conjoint, living entity in which the mother's psyche is used as an area of exploration and transformation for the infant's expelled, unbearable experiences (Eshel, 2004). We therefore suggest that this state of unintegration of the infant, which expresses the fragmentation of the parts of the self that are not yet organized, may be mirrored in episodes of disintegration of the mother, reflecting the breakdown and dissolution of the self.
As shown in the clinical case above, and in line with the theoretical notion of intergenerational transmission of trauma (Fraiberg et al., 1975; Jacobvitz et al., 2006; Solomon & George, 2011), it appears that a major source of the extreme emotional contagion that Sharon experienced with her infant emerged from the initial and painful deficits she herself experienced in infancy. Moreover, in line with Raphael-Leff (2010), as well as with the therapeutic approaches of mother–infant psychotherapy (e.g., Baradon et al., 2016; Lieberman et al., 2020), the process of “contagious arousal” may also be an opportunity for rebuilding and reorganization, both for the infant and for the mother. Thus, by acknowledging these deficits in the therapeutic sessions, Sharon slowly managed to strengthen her separation from the baby, and strengthen and ground her maternal abilities and connect to a more positive subjective maternal experience.
Concluding discussion
We have sought here to gain a deeper understanding of the largely unspoken issue of mothers’ disintegrative responses, specifically intrusive thoughts and dissociative experiences, in the context of infant care, a subject of considerable relevance to both researchers and clinicians. To this end, we conducted qualitative research as well as analysis of a clinical case study.
In order to expand our theoretical understanding, we used grounded theory methodology (Strauss & Corbin, 1990) to generate two main theoretical concepts based on an inductive and deductive analysis that relied on existing literature, the content of the mothers’ reports, and a clinical case study: (1) maternal disintegration as a response to ambivalence, and (2) maternal disintegration as a response to “contagious arousal” or projective identification.
In terms of maternal disintegration as a response to ambivalence, both the qualitative research and the clinical case study revealed numerous expressions of maternal ambivalence. Previous studies have also found conflict and ambivalence among mothers, who regard themselves as caregivers and protectors of the infant on the one hand, and have hostile and threatening thoughts of harming the child on the other (Boyd & Gannon, 2021; Meehan et al., 2021). Raphael-Leff (2010) argues that such intrusive thoughts may indicate a sense of persecution on the part of the mother, who feels that her body and mind are “being exploited” by the infant. Our findings suggest that mothers’ dissociative experiences may serve as a defense mechanism that helps them to deal with the conflict between their need to respond to the infant's demands and dependency and their need to maintain their own autonomy. These conflictual feelings may provoke even higher distress in light of the culture of “intensive mothering,” which prescribes that “the child absolutely requires consistent nurture by a single primary caretaker and that the mother is the best person for the job” (Hays, 1996, p. 8). Thus, mothers may interpret feelings that are inconsistent with this approach as illegitimate (Capdevila et al., 2022; Kestler-Peleg, 2023).
This interpretation is in line with Parker (1995), who contends that just as the infant has conflicting love–hate feelings and aggressive fantasies toward the mother, so too does the mother have ambivalent attitudes toward the infant. In addition, as the infant undergoes a process in which they learn to contain these conflicting emotions and reach a more complete state, the mother goes through a parallel developmental process of being able to contain the internal contradictions of aggression and helplessness.
Moreover, according to some theoretical approaches (Baraitser, 2009; Parker, 1995; Raphael-Leff, 2010), ambivalence is an inherent, natural, and healthy part of the maternal experience, a reflection of the mother's subjectivity and sense of self. In other words, as Baraitser (2009) suggests, the mother's “strange” and irrational feelings can be the moments when she encounters her subjectivity, of which she was previously less aware. Before the child was born, there was no one to reflect these insights to her. It is the dyad with the infant that allows her to better understand herself and the feelings that were hidden and now resound in her as a mother. Thus, not only may disintegrative responses be normative, but they may also have positive and creative potential (Murray & Finn, 2012). Furthermore, in accordance with the therapeutic approaches of mother–infant psychotherapy (e.g., Baradon et al., 2016; Lieberman et al., 2020), and as strikingly illustrated in the clinical case study, openness and contact with the conflicting and painful emotions aroused by the mother's ambivalence may be a healing process that allows her to contain and hold the different parts of her personality and the emotions evoked by motherhood.
With regard to maternal disintegration as a result of “contagious arousal” or projective identification, as Raphael-Leff (2010) claims, the mother's constant exposure to the infant's emotional and physical arousal, embodied in primary and powerful emotions and substances, may cause her to have similar experiences and feelings, as if they were also hers. Thus, the emotions reported in both the qualitative study and the clinical case—such as helplessness, detachment, aggression, and disorientation—correspond with the infant's experiences at the beginning of life. As some of the descriptions indicate, the mothers’ disintegrative responses were not always triggered by a specific situation, but seemed to arise out of nowhere. The fact that these episodes occur for no apparent reason and the mother finds them difficult to describe verbally, as if they were not really her own experiences she was seeking to explain, suggests that they may be perceived as instances of “contagion” or identification with the infant.
One prominent example is one of the mothers’ intrusive thoughts of “losing her grip” and dropping the infant. These thoughts correspond with the infant's primitive anxiety of collapse and breakdown (Ogden, 2014). Constant exposure to the infant's raw feelings of helplessness and anxiety may thus arouse the mother's own primary and repressed anxieties. While she may find it difficult to put into words what she is thinking and feeling at such times, she senses the urge to collapse, to lose her grip, which is reflected in the intrusive thought of dropping the baby. Maternal dissociative experiences may similarly be understood as “contagious arousal” (Raphael-Leff, 2010) or the mother's identification with the infant's detachment and disorientation, which are inherent in the child's experience of unintegration.
Certain limitations of the study should be noted. First, as reflected in the relatively low response rate to the open-ended questions, this study deals with a sensitive subject, and therefore some women may have been hesitant to fully share their experiences. In addition, it is possible that the wording of the questions was too complex or vague for some of the women, making it hard for them to respond. Thus, those who chose to participate may be women who are more confident both in their ability to express their experiences and in the meaning and consequences of sharing them. Given the importance of the issue, however, it warrants further exploration so that more voices can be heard in order to ease the concerns and taboos surrounding the subject and give greater legitimacy to the thoughts and feelings of many mothers. Furthermore, this study was conducted only among mothers. It would also be of value to examine fathers’ disintegrative responses in the context of infant care, particularly those who serve as primary caregivers or are equal or significant partners in caring for the infant.
Notwithstanding these limitations, the current study has important theoretical and practical implications. Theoretically, it offers significant insights into mothers’ disintegrative responses in the context of infant care. Not only does it expand existing knowledge regarding intrusive thoughts, but it also provides intriguing evidence of mothers’ dissociative experiences, a subject never previously explored. Giving voice to these unspoken issues is even more important in light of the culture that still largely sees the centrality of the child as the first priority and therefore does not allow room for an authentic expression of the complex maternal experience. Furthermore, the results suggest a theoretical conceptualization that deepens our understanding of maternal disintegrative responses and may be used in future investigations and with other populations, such as fathers, as well.
On the practical level, the combination of findings from the qualitative study and the clinical case study highlights the contribution of the theoretical conceptualization to practice and its relevance not only to researchers, but also to psychotherapists and professionals working with mothers. Drawing on feminist psychoanalytic theories, the insights gained from the study, and especially from the clinical case, demonstrate the ability of the therapeutic relationship to assist the mother in touching painful and repressed areas in her personality, in containing the ambivalence she feels as a mother, and in identifying responses of “contagious arousal” and projective identification with the infant. Such intervention may help mothers develop an integrative, creative, and renewed awareness of themselves.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in the study were in accordance with the ethical standards of the Bar-Ilan University School of Social Work’s Institutional Review Board.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Consent was obtained from all participants included in the study.