
Abstract
In a social atmosphere of expecting mothers to sacrifice their own wellbeing for the sake of their children's wellbeing, pregnant women are compelled to find their stance in relation to these sets of expectations. The current study aimed at exploring the relationship between Israeli women's tendency to meet social expectations, that is, defensiveness at the end of pregnancy and parental self-efficacy five months postnatal, and at examining the role of anxiety and depression two months postnatal in this relationship. Participants included 238 Israeli women who completed self-reported questionnaires at three time points: during the third trimester of pregnancy (T1), two months after giving birth (T2), and three months later (T3). The questionnaires focused on background variables, defensiveness (T1), anxiety (T2), depression (T2), and parental self-efficacy (T3). Multiple regression analyses were conducted to assess a serial mediating model, which revealed that defensiveness (T1) impacts parental self-efficacy (T3). Additionally, anxiety (T2) and depression (T2) mediate this relationship, while controlling for age, education, and income (T1). The findings suggest that in the relationship between defensiveness at the end of pregnancy and parental self-efficacy five months postnatal, anxiety and depression served as the detrimental mechanism. The findings are discussed considering self-theories.
Some psychologist feminists focus on motherhood through the lens of how its social expectations place pressure on women, leading to unrealistic expectations about what it means to be a mother (Enlander et al., 2022; Henderson et al., 2016; Reppond & Bullock, 2020). Israel, where the current study was conducted, contains a mixture of traditional and innovative approaches to motherhood, as does most of the Western world. For example, in Israel, while the birth rate is the highest among OECD 1 countries, most mothers work outside the home (75%) and, at the same time, they earn 16.3% on average less per hour than men (Central Bureau of Statistics, 2020). Thus, the social expectations from mothers continue to dictate that they still be regarded as primary caregivers in Israel (Shapira-Berman, 2005), as in most countries (Apple, 2006; Jacques & Radtke, 2012). These expectations concern the extent to which mothers are sensitive and responsive to children's needs, prioritizing them over their own wellbeing (Henderson et al., 2016). Mothers tend to adopt this orientation almost uniformly and fulfill these social expectations. They do so through the leading parental style of the Western middle-class: intensive motherhood, which is labor-intensive, emotionally absorbing, expert-guided, and financially expensive (Hays, 1996). Importantly, its most prominent characteristic is child centrism (Budds et al., 2016). But does adaptation to social expectations translate into the self-perception of being capable of success in this maternal role?
The concept of defensiveness (sometimes called social desirability; Kline & Allen, 2008; Lévesque et al., 2010) can be productively drawn on to answer this question. Defensiveness is a personality trait characterized by the tendency to satisfy social expectations to avoid fear, internal conflict, or unpleasant emotions that might harm self-esteem (Crowne & Marlowe, 1960; Lane et al., 1990). The satisfaction of social expectations may be met by adopting socially desirable behaviors such as conforming to the opinions of others or by lying about inappropriate behaviors and/or suboptimal performance (Lévesque et al., 2010).
In the context of motherhood, the personality trait of defensiveness may be expressed as identification with the agenda of child-centrism. It was found that mothers characterized by high levels of defensiveness tended to adopt child-centric practices (Kestler-Peleg & Lavenda, 2018). This tendency to embrace child-centrism has been explained as a way for defensive mothers to avoid the threat of horrible feelings that arise from the conflict between what feminism has conceptualized as “the myth of motherhood”, referring to motherhood as easy, instinctive, and the peak of women's aspirations (Ambrosini & Stanghellini, 2012; Badinter, 1981), and the more complex, exhausting, demanding, and confusing reality experienced by women (Enlander et al., 2022; Kestler-Peleg & Lavenda, 2018; Reppond & Bullock, 2020).
The current study aims at exploring the relationship between defensiveness as a personality trait among women at the end of pregnancy and parental self-efficacy (i.e., parental confidence in their ability to effectively take care of their children and fulfill their role as parents) five months after giving birth, by which time mothers have already gained some experience in parenting. To my knowledge, this relationship has not yet been examined, let alone longitudinally.
Since parental self-efficacy is a key variable for predicting various parental and child outcomes (see for example, Cao et al., 2022; Harpaz et al., 2021), a growing number of studies have focused on it (see for example, Bentley & Zamir, 2021; Saleh et al., 2022). Given that defensiveness is based on threat perception and avoidant reactions in a way that meets social expectations at the expense of authentic expression, I hypothesized that higher levels of defensiveness would predict lower levels of parental self-efficacy. Additionally, as postpartum anxiety and depression essentially reflect the mental state of postpartum women, I assumed that they constitute the mechanism by which defensiveness predicts parental self-efficacy. Thus, considering the positive association documented between defensiveness and anxiety and depression (Kline & Allen, 2008; Winer et al., 2017), and the well-documented negative associations reported between anxiety and depression and parental self-efficacy (Feligreras-Alcalá et al., 2020; Leahy-Warren & McCarthy, 2011), I further hypothesized that the relationship between the personality trait of defensiveness and parental self-efficacy would be mediated by anxiety and depression. Therefore, I hypothesized that higher levels of prenatal defensiveness predict higher levels of anxiety two months postnatal, which, in turn, predict higher levels of depression two months postnatal, which, in turn, predicts lower levels of parental self-efficacy three months later (i.e., five months postnatal).
Methods
Sample and procedure
Participants were followed for six months (M = 6.23; SD = 2.14) and surveyed at three intervals: during the third trimester of pregnancy [25–42 weeks of pregnancy (M = 33.81, SD = 4.46; T1)], about two months postnatal (M = 1.80; SD = .28; T2), and about five months postnatal (M = 5.20; SD = 1.28; T3). Potential participants were recruited from 18 women's health clinics from all four Israeli public health funds. Research assistants approached potential participants, briefed them on the research, and invited them to participate in the study. Questionnaires were filled out at participants’ homes and returned by mail or email. Institutional Helsinki committees approved the research design, and all the participants signed informed-consent forms.
Six-hundred and one pregnant Israeli women participated in T1; 472 mothers participated in T2 (78% of the total); and 375 mothers participated in T3 (62% of the total). Those who dropped out provided several reasons for their decision: lack of time, distractions, and difficulties in concentration due to fatigue, and so forth. To evaluate whether there had been a trend of selective attrition, a series of t-tests were carried out comparing participants and leavers in demographics and study variables as measured at T1. These analyses indicated that except for income levels [the level of leavers’ income (M = 2.37, SD = .05) was significantly lower than that of participants (M = 2.61, SD = .04), [t (417.99) = −3.55, p < .001)], participants and leavers did not differ in age, years of education, and defensiveness levels. Overall, only 238 participants who completed all measures at the three waves of data collections were included in the analyses.
Participants were between the ages of 20 and 46 years old (M = 29.86, SD = 4.20) at T1, relatively well-educated (M = 16.27 years of education, SD = 2.11), and their family income was similar to the average in Israel or higher (91.9%). Most of the participants were native-born Israelis (87.0%), married (95.4%), and employed (84.0%). During the pregnancy, the participants had between 0 to 7 children (M = 1.02, SD = 1.15).
Measures
Background variables: At T1, participants were asked to indicate their age, number of years of education, country of birth, marital status, level of family income compared to the average income in Israel (1 = below average, 2 = about the same as, or 3 = above the average family income in Israel), employment status, and number of children. At T2, they were asked to report information on the gestational week of birth and infants’ weight at birth.
Defensiveness was assessed using The Marlow-Crowne Social Desirability Scale (Crowne & Marlowe, 1960). The scale consists of 33 true/false items describing behaviors that are perceived by society to be exemplary but are actually infrequent behaviors. This scale is commonly used to evaluate the personality trait of defensiveness (e.g., Kline & Allen, 2008; Lévesque et al., 2010). Negative items were reverse coded so that the higher the score, the greater the level of defensiveness (α = 0.76).
Anxiety was assessed using a shortened version of The Revised Form of the Manifest Anxiety Scale, developed by Taylor (1953), that includes 28 true/false items describing participant feelings over the past two weeks. Negative items were reverse coded so that the higher the score, the greater the level of anxiety (α = 0.80).
Depression was assessed using The Edinburgh Postnatal Depression Scale (EPDS) (Cox et al., 1987). The scale consists of 10 items relating to symptoms of depression. The participant is asked to rate to what extent each one characterizes her feelings over the past week, on a scale from 0 to 3. Following a reversal of relevant items, the sum of the answers indicates the intensity of depression (Cox et al., 1987) (α = 0.83).
Parental self-efficacy was assessed using The Parenting Sense of Competence Questionnaire (PSOC) (Johnston & Mash, 1989). This 18-item scale assesses the extent to which the mother feels that she is succeeding in fulfilling her parental role. Participants were asked to refer to the extent to which they agree with the statements on a 4-point Likert scale with a higher score reflecting higher parental self-efficacy (α = 0.83).
Data analysis
Data analyses in the present study were conducted using quantitative data analysis software. First, descriptive and correlation analyses were conducted for all variables. Furthermore, serial mediating roles of anxiety and depression at T2 in the relationship between defensiveness at T1 and parental self-efficacy at T3 were examined when controlling for age, years of education, and levels of income at T1.
Results
The findings of the Pearson correlation tests are presented in Table 1, which indicated that defensiveness (T1), anxiety (T2), and depression (T2) are in significant and positive correlations with each other, and in significantly negative correlation with parental self-efficacy (T3). Background variables of age (T1), education (T1), and income (T1) were also correlated with each other. Age was negatively correlated with education and income, and education was positively correlated with income. Additionally, age was positively correlated with anxiety and negatively correlated with parental self-efficacy. And lastly, income was positively correlated with parental self-efficacy.
Means (M), standard deviations (SD), and correlations among the variables
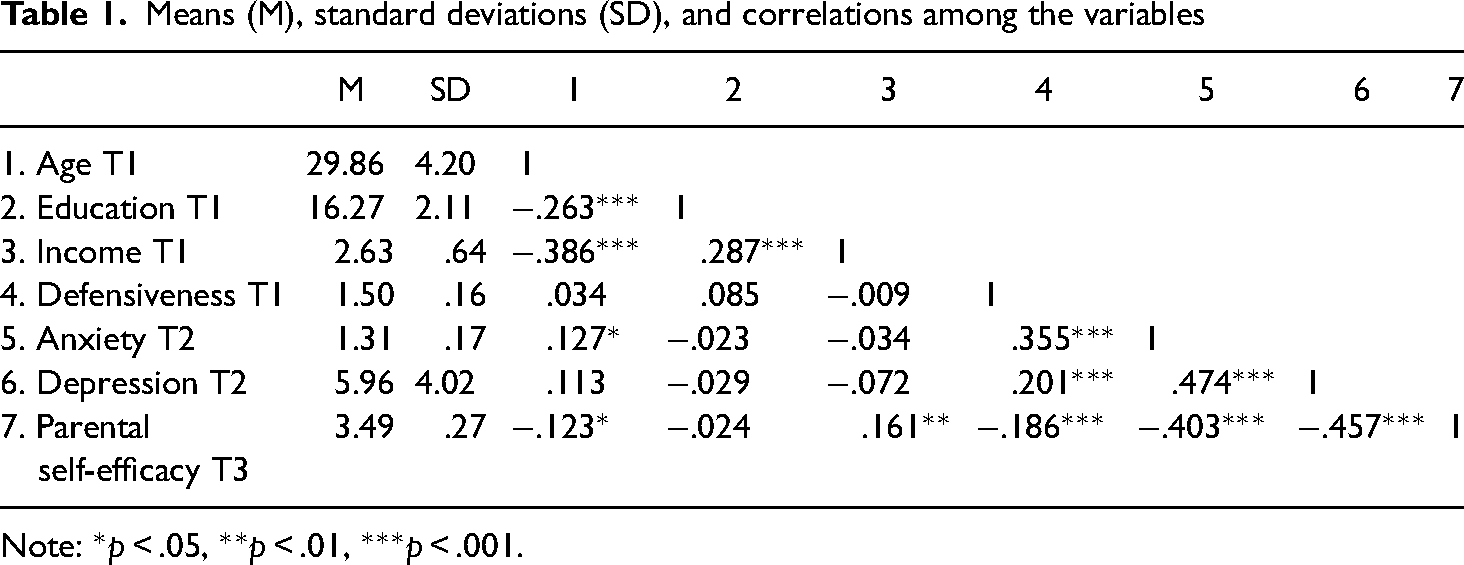
Note: *p < .05, **p < .01, ***p < .001.
Multiple regression analyses were then conducted to assess a serial mediating model, in which anxiety (T2) and depression (T2) mediate the relationship between defensiveness (T1) and parental self-efficacy (T3), while controlling for age, education and income (see Figure 1). A bootstrapping procedure was conducted with bias-corrected confidence estimates. In the present study, the 95% confidence interval of the indirect effects was obtained with 5000 bootstrap resamples. The direct effect of defensiveness on parental self-efficacy (C path) was negatively significant (B = − .45, SE = .11, p < 0.01). In addition, the direct effect of defensiveness on anxiety (path a1) was positively significant (B = 0.35, SE = 0.06, p < 0.01), as was the effect on depression (path a2) (B = 3.64, SE = 1.56, p = 0.02). Also, the direct effect of anxiety on depression (path d21) was positively significant (B = 10.05, SE = 1.49, p < 0.01). However, the direct effect of anxiety on parental self-efficacy (path b1) was negatively significant (B = − .36, SE = 0.10, p < 0.01), and so was the effect of depression on parental self-efficacy (path b2) (B = − .03, SE = 0.00, p < 0.01). The effect of the controlled variables (i.e., age, education and income) on the model factors was not found to be significant, except for age on anxiety (B = .01, SE = 0.10, p = 0.01).
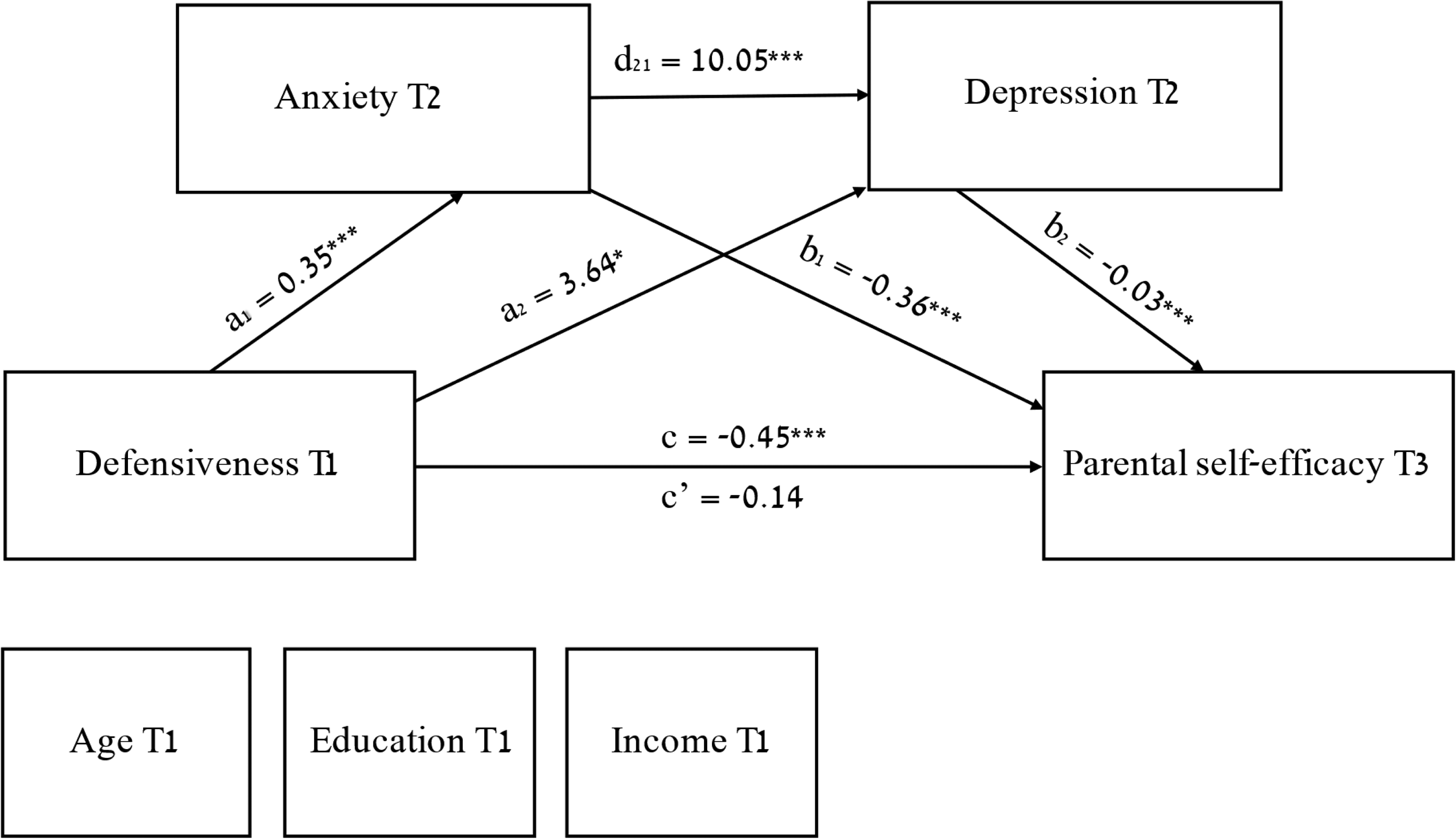
The serial mediation role of anxiety (T2) and depression (T2) in the relationship between defensiveness (T1) and parental self-efficacy (T3), and unstandardized beta values. Note: *p < .05, ***p < .001.
The bias-corrected 95% confidence intervals (CI) precluded zero for indirect effects. Specifically, a significant indirect effect of defensiveness on parental self-efficacy via anxiety was found (indirect effect = − .13, 95% CI = − .216 – − .051). The effect of defensiveness on parental self-efficacy was also mediated by depression (indirect effect = − .10, 95% CI = − .190 – − .022). Furthermore, a significant indirect effect on parental self-efficacy via anxiety and depression was found for parental self-efficacy (indirect effect = − .09, 95% CI = − .155 – − .046). The total effect of the serial mediation model on parental self-efficacy was to be statistically significant (total effect = − .32, 95% CI = − .478 – − .183).
Discussion
The findings of the present study indicate a long-term association between defensiveness levels at the end of pregnancy and parental self-efficacy five months postnatal, via levels of anxiety and depression two months postnatal. In other words, and as an answer to the question asked at the outset about the association between adaptation to social expectations and self-perception of being capable to succeed in the maternal role, attempting to adapt to social expectations tends not to translate into the self-perception of being capable of succeeding in the maternal role due to the significant dynamic of mental state. Through the lens of feminist psychology, the “good mother” discourse involves the monitoring and discipline of women during transition to motherhood. Since women characterized by high levels of defensiveness are particularly sensitive to social messages, they tend to internalize the socio-cultural gender expectations, and to experience the inherent difficulty of upholding these expectations. They respond to these difficulties with guilt and shame (Shefer & Munt, 2019; Slobodin, 2019) that may be reflected in the development of postpartum depression and anxiety. These, in turn, undermine the maternal self-perception reflected by the maternal self-efficacy.
To my knowledge, this is the first study that examines this relationship between defensiveness and parental self-efficacy in general and specifically, as a longitudinal study during the transition to motherhood. Moreover, the serial mediation model first used here demonstrates the significant dynamic of anxiety and depression two months after giving birth in the relationship between prenatal defensiveness and parental self-efficacy after the maternity leave is over, five months postnatal.
The desire to fulfill social expectations as reflected by the personality trait of defensiveness, in the long run is associated with lower maternal self-perception. Although it was previously found that women characterized by higher levels of defensiveness tend to adopt a child-centric parental style (Kestler-Peleg & Lavenda, 2018), in the current study it emerged that adopting child-centrism does not promote their perception of self-worth. On the contrary, the attempt to meet social expectations predicts higher levels of anxiety and/or depression at the end of the postpartum period, two months postnatal.
According to self-theories (Dweck & Elliott-Moskwa, 2010), defensiveness is used to keep away from threatening situations and to repel or distort threatening information. When it is exaggerated, defensiveness can deprive people of experiences from which they could learn. Therefore, defensiveness comes at the expense of learning and potential success. It leads to concealment instead of correcting flaws, to conformity at the expense of development, which is required during the period of transition to motherhood. This transition necessitates revision and adaptation in the face of a dramatically changing reality (Ambrosini & Stanghellini, 2012; Apple, 2006). Thus, the attempt to please others and avoid authentic expressions leads to fixation and difficulty in establishing parental self-efficacy. Additionally, this avoidance of authenticity has been found in the current study to be associated with postpartum adjustment difficulties, reflected by anxiety and/or depression that ultimately impairs parental self-efficacy. Thus, while the associations found between postpartum anxiety and depression are consistent with the findings of previous studies (Feligreras-Alcalá et al., 2020; Leahy-Warren & McCarthy, 2011), the current study highlights the role of this postpartum mental state in the relationship between the personality trait of defensiveness and parental self-efficacy.
Limitations
The lack of representation is the central limitation of this study. Although the data were collected from the public healthcare services, the participants were mostly married, well-educated, and have a higher family income than the average income in Israel. In addition, dropout rates during this potentially intense and disruptive period ranging from pregnancy to several months after birth may bias the findings. Therefore, generalizability of the findings should be considered cautiously. Likewise, data were gathered through self-report questionnaires alone, which might have contributed to biased results due to method-shared variance and social desirability.
Conclusions and implications
Defensiveness during pregnancy predicts anxiety, depression, and parental self-efficacy after giving birth. These findings are rooted in societies that strive for “good mothering”, which is ingrained in the Israeli social atmosphere, as well as in other Western countries, sacrificing maternal wellbeing for the sake of one's children. Attempting to mute the contradictions that arise between these unreachable social expectations and the fears of the price that new mothers should pay for their children's wellbeing via defensiveness may predict mental health issues, which are manifested in anxiety and depression about two months after birth, and to a lower maternal self-perception as capable of success in the parental role, i.e., in parental self-efficacy, five months after birth. In addition, the shaken mental state of mothers two months after giving birth also predicts parental self-efficacy.
It is crucial that health services screen levels of postpartum anxiety and depression and offer proper treatment in order to minimize personal, parental, familial and societal harm. Social intervention programs should provide information on the uniqueness of how each woman experiences motherhood and legitimize these different experiential modalities. In addition, preventive therapeutic interventions during pregnancy are narrow and limited. Hence, it is highly important that professionals who actually meet pregnant women would encourage them, in a safe and secure space, to share their critical perceptions regarding social expectations, to examine the contradictions between social expectations and their own. Additionally, it is recommended that professionals would stimulate and support women's authentic expression in a way that they will realize their own perceptions and desires to reduce risk for impaired postpartum mental health and, in turn, promote parental self-efficacy. Finally, professionals should validate and strengthen a positive maternal self-perception in a way that will increase a sense of competence and confidence in the abilities to fulfill the complex parental role.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.