
Abstract
Endometriosis is a condition which affects around 1–2% of women worldwide and has profound effects on their everyday lives. Previous research has tended to focus on physical symptoms (such as chronic pain); how women manage changes to their identity and relationships as a result of endometriosis has received less attention. This paper discusses qualitative data examining how women negotiate changes to identity while living with endometriosis, in a social context where women are expected to minimise their symptoms and conform to feminine role expectations. We conducted thematic analysis of 34 replies to an online survey seeking qualitative text responses. The women identified disruptions to personal identity as a result of living with endometriosis. They talked about not feeling like themselves (Theme 1) and about reactions from medical and social connections prompting feelings that they were going “mad” (Theme 2). Participants also expressed feeling as though they were a burden to loved ones (Theme 3), which often resulted in self-silencing (Theme 4). Findings are discussed in the context of Western expectations of women’s roles in social relationships and suggest that professionals who support women with endometriosis should be aware of strategies such as self-silencing which may reduce effective self-care.
Endometriosis is a condition where tissues similar to that found in the endometrium in the uterus are found in other areas in the body. The inflammation experienced in this tissue, often linked to hormonal changes across a woman’s menstrual cycle, causes pelvic pain and can interfere with the functioning of organs such as the ovaries, bladder and bowels, and lead to infertility (Ballard et al., 2008). Population-based studies suggest that the condition affects around 1.3–1.5% of women (Ballard et al., 2008; Gao et al., 2019), and there is considerable research on the adverse effects of endometriosis on women’s lives. However, there is relatively little research which addresses changes to a woman’s identity, and therefore her role in social relationships, when daily functioning is profoundly changed by endometriosis. The current study examined accounts of women recruited from endometriosis support organisations to explore the challenges to personal identity posed by living with the condition.
Negative impacts of endometriosis
The negative effects of endometriosis symptoms are well-documented by both qualitative (e.g. Moradi et al., 2014; Young et al., 2015) and quantitative (e.g. De Graaff et al., 2013) researchers as including infertility, sexual difficulties and chronic pain. Chronic pain appears to be important; women who experience pelvic pain as part of the condition have reported poorer mental health and quality of life than those who do not experience such pain (Facchin et al., 2015). However, more recently the psychological literature has shifted emphasis from the effects of physical symptoms of endometriosis on quality of life to the management of relationships with healthcare providers, romantic partners and friends and family by those with the condition.
Many women with endometriosis wait decades from first reporting symptoms to receiving a diagnosis (Young et al., 2015). Women have reported that they often feel as though they had to “be [their] own doctor” (Young et al., 2020, p. 31) and be strong advocates for themselves because of reluctance to diagnose and even treat endometriosis by health professionals (Young et al., 2020). The condition has also been positioned as psychological as well as physical (Shohat, 1992) with the consequence that women are constructed as hysterical or difficult if they do not present themselves in certain ways in interactions with clinicians (Young et al., 2018).
Given the reports that endometriosis symptoms are often trivialised by doctors, it is unsurprising that friends and family also struggle to understand the potential seriousness of the condition. Problems in the social relationships of women with endometriosis often arise from a lack of awareness of the impact of the condition (Grogan et al., 2018) and these problems can make coping with symptoms more difficult. Friends and family are described as mistaking experiences of endometriosis symptoms for being in a “bad mood” (Facchin et al., 2018, p. 540); misunderstanding by family and friends, colleagues, and intimate partners (Moradi et al., 2014; Young et al., 2015) is frequently discussed as a source of distress for women with the condition. Difficulties with intimate relationships are also common (Fagervold et al., 2009) due to sexual difficulties and infertility concerns (Culley et al., 2013). Partners of women with endometriosis can feel frustrated and helpless when providing support, because they are unsure of how to help with, for example, the debilitating pelvic pain some women experience (Hudson et al., 2016) and because they do not know how to sensitively maintain their sex life (Culley et al., 2017).
Although the potential disruption to relationships has received extensive attention in the literature, fewer studies have directly examined how difficulties in relationships may also be linked to women’s own struggles to redefine themselves in the context of an endometriosis diagnosis. The following sections use the concepts of biographical disruption and self-silencing to explore how women’s identity and their role in relationships may be affected by endometriosis.
Identity disruption
The framework of biographical disruption is useful for understanding how long-term conditions can alter our sense of personal identity. Bury (1982) describes this concept as the disruption of the “structures of everyday life and the forms of knowledge which underpin them” (p. 169). This disruption requires an adjustment to patterns of behaviour; as a result, how the person with the condition views themselves may change in order to accommodate any effects on their lives and relationships.
A woman with endometriosis may be forced to rethink the role she plays in her relationships (and the role of these relationships in her life) as part of the rethinking of self-concept which is necessitated by biographical disruption (Bury, 1982). Evidence examining disruption in the heterosexual relationships of women with endometriosis suggests that this is possible and can lead to positive change. Hudson et al. (2016) interviewed women with endometriosis and their male partners about effects of the condition on each dyad’s romantic relationship. They found that some couples were able to reappraise several aspects of their relationship in the face of changes brought about by endometriosis. However, Hudson et al. (2016) also suggested that the ability to navigate a disruption to identity by using reappraisal of the self is dependent on “relational identities and gendered expectations” (p. 732). An expectation that a feminine role in relationships is self-sacrificing may potentially hamper a woman’s ability to “mobilise resources” (Bury, 1982, p. 170) needed to renegotiate her identity after an endometriosis diagnosis.
Barriers to reappraisal
The barriers to identity reappraisal facing women with endometriosis can be thought of in two ways: firstly, in terms of the assumptions medical professionals make about treatment priorities and, secondly, in terms of the broader expectations regarding how women function in social relationships. In critical work on the ways in which medical professionals talk about their patients with endometriosis (Young et al., 2018), it was found that clinicians made assumptions about what women required from their care, and prioritised [heteronormative] sex and reproduction for treatment. These priorities did not match the priorities for treatment found for endometriosis patients in other research; Young et al. (2016) suggested that many patients with endometriosis instead prioritise treatments that address pain and quality of life. There may be consequences in terms of relationship reappraisal and psychological distress if women with endometriosis internalise clinician assumptions about the importance of treatment related to fertility. Hudson et al. (2016) noted, for example, that the women interviewed in their study reported more distress at the potential fertility implications of endometriosis than their male partners did, and had more trouble reappraising their relationship than partners when to do so meant a future without children. In addition, emphasising motherhood for women with conditions affecting fertility and/or menstruation may result in these women feeling that they have failed in their role as a woman. Women interviewed about experiences of polycystic ovarian syndrome (PCOS) (Wilmott, 2000), for example, constructed the presence of menstrual periods as defining womanhood and felt “freakish” or as though they were not “normal” (p. 110) because their reproductive function was disrupted.
Women with endometriosis must also manage these potential changes to their identity in a context where they may be experiencing extreme, chronic pain (Young et al., 2015) but are expected to be a good woman who is caring and self-sacrificing even when in discomfort (Ussher, 2004). The pressure for women in pain to repress negative feelings may be emphasised when the pain is related to the “intrinsically unpredictable, leaky and disruptive” female body (Shildrick & Price, 1999, p. 2) because of taboos associated with menstruation (Chrisler, 2011). In attempting to maintain their role as a good partner, mother, and daughter, women experiencing endometriosis symptoms may choose coping strategies which are incompatible with self-care, such as self-silencing.
The practice of self-silencing describes where [usually] women avoid speaking up in their close relationships to avoid conflict and maintain these relationships (Jack, 1991), and this lack of voice is associated with a loss of self. In addition to silencing of the self, a woman may start to judge herself by external standards (externalised self-perception) and show her attachment to important others by putting their needs before her own (care as self-sacrifice; Jack & Dill, 1992). The strain of maintaining an external “compliant self” (Jack & Dill, 1992, p. 98) in parallel to a hostile inner self can lead to a divided self where women feel as though their identity is split in two. These elements of self-silencing are associated with poor mental health and quality of life (Sormanti, 2010), and reduced self-care and treatment adherence (Brody et al., 2014).
Self-silencing has been primarily used to explain the higher incidence of depression in women compared to men (Jack, 1991), but it has been evidenced in many other long-term conditions such as cancer (Sormanti, 2010), HIV (Brody et al., 2014) and heart disease (Eaker & Kelly-Hayes, 2010). There is evidence of self-silencing across cultures (see e.g. Jack & Ali, 2010). However, there are also cultural variations in feminine stereotypes which may influence self-silencing, such as the image of the “strong black woman” affecting the experience of silence in black women (Beauboeuf-Lafontant, 2008, p. 391) in the United States.
There is evidence from previous qualitative work suggesting that self-silencing may play a role in managing endometriosis. For example, in research by Young et al. (2018), clinicians appeared to construct a good endometriosis patient as one who agreed with clinical assessments and, when nothing further could medically be done, “got on with life” (p. 347) without complaint. In other research on experiences of healthcare interactions (Young et al., 2020), women with endometriosis argued that they had to be careful in how they presented themselves to avoid the label of “problem patient” affecting their care. Both studies could be interpreted as evidence that self-silencing is a potential issue for management of social relationships in the context of endometriosis.
The present study
The negative changes in daily life brought about by endometriosis are now well-documented. A more detailed consideration is needed, however, of the effects of these changes on identity, and how women redefine and construct their relationships with others as a consequence of living with endometriosis. This is important if we are to understand how these biographical disruptions might influence mental health and self-care practices of women with endometriosis. The present study therefore aimed to examine constructions of identity in endometriosis and potential barriers to identity reappraisal in a sample of women where the impact of endometriosis on everyday life may be particularly severe.
Methodology
Feminist methodologies acknowledge that the process of examining women’s experiences must reflect the principles of respect, collaboration and caring. Rather than subscribing to a single feminist methodological approach, we adopted a broadly feminist standpoint that incorporated several feminist guiding points throughout the research, following Letherby (2003). The research was strongly informed by the political and ethical concerns of feminist scholarship, rather than by a specific feminist methodological framework. Franks (2002) advocates for issue-based, pragmatic and situated feminist research that uses the relevant materials available in a specific context in order to enable cultural and social transformations. We utilised methods in ways that are consistent with feminist ideologies (Campbell & Wasco, 2000), and, given that the work is conducted with women who are experiencing a chronic, incurable health condition and who may be vulnerable, the research focus was to use these women’s experiences as a base for contributing to knowledge about living with endometriosis in order to affect social change. We ensured that feminist principles were met through the study’s design and the application of the analytic method following Franks’ (2002) pragmatic feminist framework.
Participants and recruitment
Participant recruitment was primarily through an advertisement posted on the webpages of two prominent endometriosis support charities based in the UK. The advertisement message stated that the research team were inviting participants to complete open-ended questions in an online survey regarding their everyday experiences of living with endometriosis, and provided a link to the online consent form and survey for participants to access directly from the website. The rationale for using support groups for participant recruitment was that women with endometriosis often faced negative experiences when dealing with health professionals (Grogan et al., 2018), and we did not want potential participants to think our research involved GPs/medics, etc.
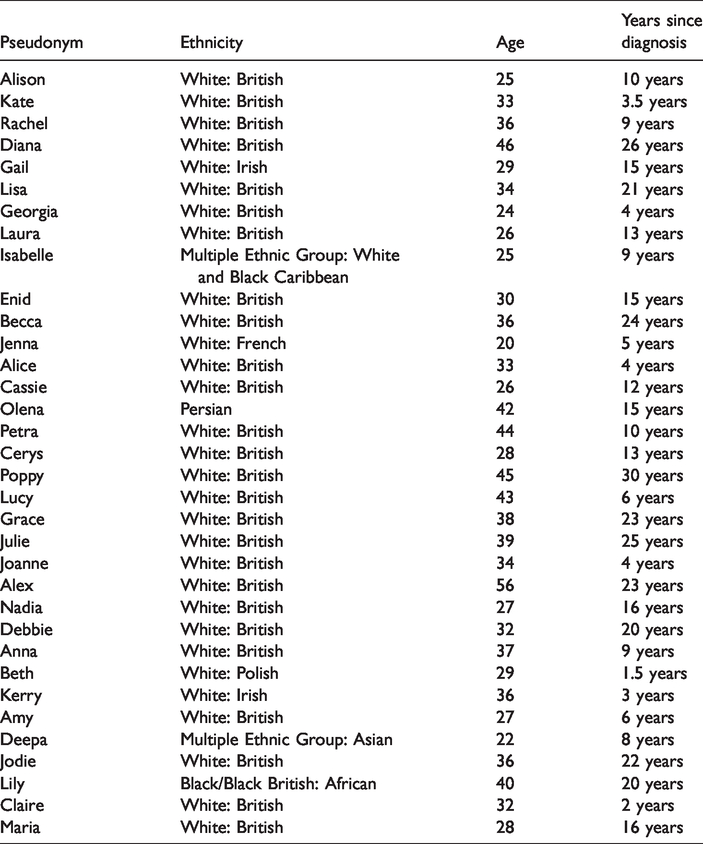
Thirty-four women self-identifying as receiving a diagnosis of endometriosis completed the qualitative survey. Of those participants 30 (88%) self-identified as White: British or other European, two (6%) as Multiple Ethnic Group (one White and Black Caribbean and one Asian), one (2%) Persian and one (2%) as Black/Black British: African. Women were aged between 22 and 56 years, and time between diagnosis and questionnaire completion varied between one week and 22 years. Time between self-reported onset of endometriosis symptoms and questionnaire completion was between one and a half and 30 years (see Table 1).
Participant Characteristics.
Data and data collection
Data were collected as part of a larger study, and this is a re-analysis and re-interpretation of data from a paper focused on health-related experiences (Grogan et al., 2018). This previous publication focused on treatment and did not examine wider issues related to gendered expectations and social context. The current analysis is presented as a re-analysis and re-interpretation in line with APA recommendations (APA, 2016, Section 8.13).
A qualitative online survey approach was adopted, where respondents were asked open-ended questions and encouraged to answer in detail (Terry & Braun, 2017). This method can be an effective way of gathering in-depth data from a wide range of participants, including those with chronic conditions who may struggle to attend interviews, for example. Although this method may lack the opportunity for dialogue between participants and researchers, we anticipated that the use of an anonymous online survey would increase the level of disclosure of practices and interactions which may be constructed as “problematic,” such as lack of adherence to recommended treatment. Women were not able to access a copy of their responses after participation because no identifying information was collected. The average number of words provided was 799 (min. 181, max. 1980).
After the information page and consent information, the survey contained: 13 open-ended questions; demographic information; requests for details about when and how participants found out that they had endometriosis; an estimate of how long they had experienced symptoms before diagnosis; feelings at diagnosis; experiences of symptoms; and whether these symptoms impacted on participants’ day-to-day life in relation to various types of relationships and contexts. Participants were able to write as much as they liked to answer each question. The questionnaire was designed to allow participants to save their progress and take a break if needed, recognising that for some women completion of the questionnaire on a single occasion would be mentally and physically fatiguing.
Ethical approval was granted through the Institutional Ethics Committee. Informed consent was gained through a forced response item at the start of the questionnaire; the women consented specifically to the use of anonymised extracts from their responses in reports of the research. Upon completion, women were given details of the researchers should they have any outstanding queries, and information on UK websites offering support for women with endometriosis.
Data analysis
We examined the data using Braun and Clarke’s method of reflexive thematic analysis to develop themes from the text provided by our participants (Braun & Clarke, 2006; Terry et al., 2017). This method enables researchers to identify patterns of meaning across qualitative data sets; we were concerned with patterns across all survey questions rather than similarities across participants for specific questions. Our approach to analysis was primarily inductive; the codes identified in the data, and the resultant themes, were constructed from the data provided by participants.
We took a critical realist approach to the data. This approach has features in common with social constructionism in that, for example, language is understood as constructing realities for participants. However, critical realist researchers argue that these social realities are constrained by “possibilities and limitations in the material world” (Sims-Shouten et al., 2007, p. 102). Material conditions of the social structures in which women exist, and particular physical realities of an endometriosis diagnosis, may mean that some discourses are more or less likely than others. As researchers we cannot access an objective reality; we can only access participants’ social realities, constrained by the broader social contexts in which their accounts are produced (Terry et al., 2017).
Reflexive thematic analysis is characterised by six stages: familiarisation, code generation, theme development, reviewing and defining the themes, and finally writing of the analysis (Braun & Clarke, 2006). All three researchers familiarised themselves with the data in parallel by reading and re-reading the responses. Following familiarisation, the authors met and discussed their initial thoughts. The aim of collaboration at this stage was not to attempt an assessment of inter-rater reliability, for example, but rather to benefit from the insights of members of the research team with different subjective positions in relation to the topic (i.e. one researcher has lived experience of endometriosis, the other two do not) early in the analysis process (see Terry et al., 2017). Following this initial pooling of ideas, the first author generated initial codes through systematic examination of the data, creating units of meaning related to the research question. These initial codes were used to develop the four themes presented below by grouping codes into meaningful broader categories which captured a core concept related to the research question. The first author then presented this analysis to the other two authors, who provided assistance in the reviewing of the themes before the first author wrote the first draft of the final report. All themes and associated quotes were reviewed and agreed by all authors.
Analysis and discussion
Many women talked about the disruption that endometriosis had caused to their sense of identity (Theme 1). The consequences of this disruption for the day-to-day reality of living with endometriosis included doubting their own sanity (Theme 2), and feeling like a problem for their friends and family (Theme 3) and there was evidence that some women utilised self-silencing to cope with these changes by minimising their symptoms or hiding their experiences from others (Theme 4). The themes discussed below explore the presence of and consequences of identity disruption in endometriosis. Pseudonyms are used to identify participants, and quotes are cited verbatim.
Theme 1
“Not feeling like myself anymore”: Losing one’s sense of self
Women often indicated that they did not feel like they were still themselves. In some cases this was specific, and related to aspects of identity such as gender identity (feeling they had failed as a woman) and body image (body hatred related to changes in appearance and functionality). However, there were many cases of general unease and discomfort related to the perceived changes endometriosis had wrought in their core identities.
In most cases, this change in identity was framed as negative, suggesting a disruption rather than a reappraisal: Deepa: I was always an optimist and unbeknownst to me I have begun to hate myself and hate life. I was always bright and sunny and now I am utterly miserable and gloomy. I have become selfish and have a victim mentality. Jenna: I feel deprived of my agency concerning myself, and that any choice has been taken away from me. It is really hard to renegotiate myself, I am a very dynamic person and the treatment and the disease dispossess me from my energy and it is frustrating.
In some cases, participants spoke specifically about gender when discussing negative changes to their identities, referring to effects of endometriosis such as reduced fertility, reduced sex drive (or wanting to avoid painful intercourse) and treatments such as hysterectomies. For example, Joanne argued that “as a woman you are designed to have children, I’m so scared that I won’t be able to experience that.” She constructs a woman’s ability to have children as unquestionable and she is fearful (“scared”) of not being able to complete the function for which she feels she was “designed.” Amy also expresses the consequences of not being able to fulfil this role as having “failed at becoming a mum naturally which is all I have ever wanted.”
The notion of childbearing as constituting the “normal” role of a woman supports previous research examining identity in endometriosis (Hudson et al., 2016) and also research on PCOS, where ideas about the naturalness of childbearing were associated with describing infertility as “freakish” (Wilmott, 2000, p. 110). This sense of feminine failure was not always constructed as purely functional; while discussing her hysterectomy as a result of endometriosis, Kristy stated that “I don’t feel I am fulfilling my role as a woman,” referring to a biological aspect of womanhood. However, in a later extract, she also expressed that she felt “less feminine, less attractive,” moving to a construction of women contingent on social stereotypes about feminine appearance (Wilmott, 2000).
The extracts explored in this theme make clear the distress many of the women expressed at feeling they were no longer themselves, and specifically no longer women in a sense which was meaningful for them. As Lily points out: “I’m not a woman. How can I be if I can’t do normal womanly things?” Lily does not elaborate on what these womanly things might be, but reasons that if these activities cannot be performed this automatically precludes claiming identity as a woman.
Theme 2
“I’m not some crazy hypochondriac woman”: Doubting one’s own sanity
An additional source of distress was participants feeling that others did not believe their accounts of their experiences, or that others regarded symptoms of endometriosis as psychosomatic. Receiving a diagnosis of endometriosis was constructed as a relief because the trivialisation of symptoms they had experienced, especially from medical professionals such as GPs, had led them to doubt their own bodily experiences and their own sanity: Jenna: I was relieved. I had been told that it may be in my head and the medical core did not take me really seriously. I was wondering if I was not turning crazy and I got really depressed.
Relief, for many of the women in this study, was part of a complex reaction to an endometriosis diagnosis, but existed even in contexts where the relief was explicitly contrasted with negative diagnostic implications: Laura: When I was first diagnosed I was devastated but relieved. Devastated I now had a lifelong condition with pain, bloating, intolerances to food and possibility of infertility but relieved it wasn’t all in my head
Participants also expressed relief at being able to prove to others, using a diagnostic label, that their experiences were real: Maria: Relieved that finally there is a reason for all my symptoms. I knew it! I’m not just some crazy hypochondriac woman who always thinks there’s something wrong with me. Finally I can turn around to my dr and say, “hey, I think my endometriosis is getting worse again.”
Many studies on endometriosis have referred to the importance of early diagnosis and the problems presented by dismissing endometriosis as menstrual cramps or stress (Fauconnier et al., 2013; Young et al., 2015) or women themselves as hysterical (Young et al., 2018). Some of the women surveyed here questioned the accuracy of this dismissive construction of endometriosis, but had started to question their soundness of mind and expressed a felt pressure to adopt a “crazy hypochondriac woman” (Maria) identity. Given that the perceptions of others had such an effect on some of the women’s sense of identity, this constitutes evidence of externalised self-perception (Jack & Dill, 1992), an element of self-silencing, where a woman judges herself (in this case her psychological state) through the eyes of others.
Theme 3
“I constantly feel like I’m a problem”: The burden on friends and family
Even once women with endometriosis had obtained perceived legitimisation of their symptoms through diagnosis, the physical symptoms of endometriosis were described as limiting participants’ ability to fulfil their social roles as they would wish. Guilt and concern for others were commonly seen in the accounts provided and constituted an additional source of distress and identity disruption for these women.
The impacts of endometriosis on participants’ social lives were often framed in terms of letting others down rather than in terms of the women themselves missing out. For example, Becca identified the worst effects of the condition on her social relationships as “letting them down when last minute pain strikes.” Social situations were even avoided to prevent disappointing others; Alice stated that “my circle of friends is now small as I can’t manage to do as much and I don’t want to let people down if I’m not well.” Alice talks here of a reduction in her circle of friends because of what she can “manage,” suggesting that she is pre-emptively limiting her social life to avoid a negative impact on her friends. Where the women felt they were letting others down, this was always talked about in terms of negative emotions. For example, Kristy stated that “I struggle with guilt all the time at not being able to keep up the pace either at work or in my personal life and feel like I constantly let people down.” She identifies guilt at not fulfilling responsibilities in the way she would like in two key areas in her life, and pressure not to let her illness show and to “keep up the pace.”
The phrase “letting people down” (e.g. Alice) was common in the data, and it was also common for participants to talk of changing their behaviour to avoid having to ask friends and family for understanding or support. Where support was received, several women, including Nadia below, expressed guilt about their family’s involvement in assisting them: Nadia: I see the strain it has on [my mother] though. Having come to every doctor’s appointment and hospital test. She has had to give up a lot to fight the battle with me and I often feel very guilty about how much strain I have put on her.
Participants claimed responsibility for the emotional well-being of their friends and family, in addition to their own, demonstrating empathy for those they shared their lives with at a time when they themselves needed help. This was especially true of romantic relationships, as Lisa describes: “My husband quite often panics when I have bad patches and gets cross when I still try to push myself so hard. This is my coping mechanism, but it’s very hard for him to see me put myself through it.” Lisa identifies her own difficulties with managing the condition, referring to the effects of pushing herself too hard, but also takes care to pair this with an awareness of distress in her romantic partner. Where women did not express guilt, they often constructed the support they received as unusual: “I really do see how good a friend I have!” (Kate). Some women also constructed supportive relationships as explained by good luck. For example, Becca says of her work colleagues that she “was very lucky to be with understanding colleagues,” and Alex said of her romantic partner: “I am very lucky in that my partner … has always been very understanding.”
This theme demonstrates that women with endometriosis may feel additionally burdened by their empathy, guilt and concern for those around them, drawing on constructions of feminine gender role expectations which include the expectation that women put the needs of others before themselves (West & Zimmerman, 1987). Women’s accounts suggested that they forwent self-care to focus on the needs of others, demonstrating a construction of care as self-sacrifice, another element of self-silencing (Jack & Dill, 2010). This focus on the perspectives of others also echoes findings that women with, for example, a cancer diagnosis express concern for the feelings and health of their partners while coping with a chronic condition (Sormanti, 2010).
Theme 4
“I suffer in as much silence as I can muster and carry on”: Concealing distress
The concern demonstrated by participants for those around them was often associated with adjusting their behaviour to take their relationships into account, evidencing a silencing of the self (not saying what one thinks and feels to protect oneself and relationships; Jack & Dill, 1992). There was extensive evidence in the data of this aspect of self-silencing. For example: Julie: I usually just get on with things and take anti-inflammatories to dull the pain if it happens when I have a social event. I tend to be good at covering up if it is affecting me and suffering in silence, so people wouldn’t usually know there is a problem.
Another consequence of not suffering in silence for these women was experiencing more of the guilt and concern for others outlined in Theme 3. For example, Nadia refers to hiding the psychological toll that endometriosis takes on her: Nadia: At one point I was even under the care of a physiatrist [sic] because of my deep depression and suicidal thoughts. But I already feel like I have put enough strain on my friends and family that I don’t think I could be selfish enough to go through with it. Instead I suffer in as much silence as I can muster and carry on. Endo has got to be the most lonely condition I can imagine.
However, self-silencing seen in accounts here was not always explicitly motivated by the feelings and perceptions of others. Some women talked about self-silencing in terms of their own need for normality. For example, Laura talks about hiding pain during sex with her husband: Laura: It has affected my relationship as sometimes I cannot be intimate or I need support because I am in so much pain it is also embarrassing bleeding during intercourse, sometimes I don’t tell my partner it hurts and suffer in silence just so we can have a normal relationship.
There may be some circumstances, however, in which symptoms of endometriosis are difficult to hide. Jenna talked of her partner seeing her “fainting, vomiting and not being able to stand or having enormous panic attacks” and the resulting lack of taboo “in terms of body or any fluids or body related topics.” Jenna describes her partner as “deeply empathetic,” suggesting that self-silencing is not an inevitable reaction to endometriosis, despite a general lack of awareness of the condition, for those in sufficiently understanding relationships.
This theme suggests that self-silencing may aid attempts to present a coherent identity in the context of the physical and psychological challenges of endometriosis, but evidence on the link between self-silencing and increased depression (Jack & Ali, 2010) and supressed emotions (Geller et al., 2010) suggests that this may not be an effective coping strategy and may have unintended negative consequences. It is likely instead that women may experience a divided self (Jack, 1991). Indeed, Laura demonstrates this directly; in her account she describes how she and her partner are “very open about every aspect of my symptoms” despite referring directly to the concept of “suffering in silence” when it comes to the difficulties endometriosis posed for her sex life with him.
Conclusion
Women who have been diagnosed with endometriosis may experience many barriers to reappraising their identity and relationships in the context of the physical symptoms and psychological impacts of the condition, especially those experiencing severe symptoms. Findings from previous research concerning frustrations with late diagnosis and dismissal of symptoms from friends and family (e.g. Facchin et al., 2018, Moradi et al., 2014; Young et al., 2015) were supported in the present study, where maintenance of existing identities and relationships were constructed as a struggle. Women talked broadly about not feeling like themselves – sometimes specifically about not feeling like a “normal” woman (Lily) – and contrasted a positively constructed identity before the onset of symptoms with a negatively constructed one after the onset of symptoms. In Theme 1, participants expressed distress at struggling to maintain a feminine identity amidst infertility worries and embarrassing personal symptoms, supporting work on other conditions affecting women’s reproductive capacity (e.g. Wilmott, 2000). In Theme 2, women detailed their struggles to obtain appropriate treatment for their symptoms because they felt cast as the hysterical woman by medical professionals (supporting Young et al., 2018), and how this resulted in the women questioning their own sanity. In later themes, general expectations that women are caretakers, even when ill themselves, led to guilt and concern for the feelings of others (Theme 3) when the women’s symptoms disrupted their relationships. The expressions of guilt identified here support research which shows that women often put others first even when experiencing symptoms of long-term conditions (e.g. Hale et al., 2009; Sormanti, 2010).
Finally, one of the ways in which participants talked about managing dismissal of their symptoms or their feelings of guilt was by experiencing their symptoms alone; self-silencing their pain and distress (Theme 4). A narrative of self-silencing runs throughout the accounts presented here. For many of the women in this study, expectations of women as selfless caretakers constructed in Western society were increasingly difficult to reconcile with symptoms of endometriosis such as infertility concerns, sexual difficulties, and the limitations of chronic pain. There was evidence of all of the elements of self-silencing, including silencing of the self, externalised self-perception, care as self-sacrifice and a divided self (Jack, 1991). The lack of understanding shown by friends and family (see Young et al., 2015) and feelings of guilt over the costs to relationships of endometriosis were identified as potential drivers of self-silencing, as well as wanting to maintain a sense of normality in relationships particularly challenged by endometriosis, such as romantic relationships.
Strengths and limitations
Women were recruited for this study online via UK endometriosis charities – a method of recruitment which has several implications. Firstly, the women who have accessed a charity for support with endometriosis are likely to be those with more severe symptoms and/or those who are feeling like they need support with managing the condition, so we acknowledge that they may be more likely to use coping strategies such as self-silencing than women who feel more supported. Although the effects of endometriosis discussed here are consistent with previous research, including reviews of other qualitative studies (e.g. Young et al., 2015), it is also possible that these are women who have found getting appropriate support from those in their social relationships particularly challenging.
The recruitment method may also have been responsible for the predominantly white sample; there may be reasons that we are not aware of which make particular routes of support more appealing to white as opposed to non-white women with endometriosis. Cross-cultural research on self-silencing suggests that there is evidence of this phenomenon in women across cultures (Jack & Ali, 2010), but that it is sensitive to changing social contexts, even within the same culture (Beauboeuf-Lafontant, 2008; Jack et al., 2010), so we cannot assume that women of all ethnicities will experience self-silencing in endometriosis in the same way.
In addition, we did not gather information about the sexuality of the women in the study, though many women talked about male partners or husbands, suggesting that the data were predominantly from women in heterosexual relationships. Although experiences with friends and family may be similar across women of differing sexual orientations, experiences of role expectations of women, particularly related to sex, childbearing and intimate relationships, are likely to differ for women who have same-sex relationships. More research is needed with a range of samples as regards sexuality.
The researchers themselves represented a range of perspectives on endometriosis, which we feel is a strength of the study. In addition to our positions as psychologists with interests in women’s health, one member of the research team has lived experience of endometriosis, and we feel that this insight meant that we were better able to appreciate some of the material consequences of a diagnosis. However, as white academics, our experience was homogeneous in other ways which must be acknowledged.
Implications
Methods of self-silencing observed in the accounts analysed here may be problematic for the management of endometriosis by women experiencing severe symptoms. Self-silencing can negatively affect self-care (Brody et al., 2014; Sormanti, 2010), and the current study suggests self-silencing is also a potential barrier to the renegotiation of identity in the context of long-term conditions, which Bury (1982) argued was important for coping with such conditions. Our findings provide examples of the ways in which role expectations of women may hamper identity reappraisal in endometriosis and suggest that supporting women may be improved by appreciating the social context of the condition. Specifically, professionals working with women with endometriosis should be aware of the possibility of self-silencing as a potential coping mechanism, and provide a space where women feel able to express their feelings about their symptoms, working with them to determine self-care strategies that work in the context of their personal relationships.
Supplemental Material
sj-pdf-1-fap-10.1177_0959353520930602 - Supplemental material for “The most lonely condition I can imagine”: Psychosocial impacts of endometriosis on women’s identity
Supplemental material, sj-pdf-1-fap-10.1177_0959353520930602 for “The most lonely condition I can imagine”: Psychosocial impacts of endometriosis on women’s identity by Jennifer M Cole, Sarah Grogan and Emma Turley in Feminism & Psychology
Footnotes
Acknowledgements
The authors wish to thank the women who took time to fill out the survey, and the anonymous reviewers who provided excellent and detailed feedback on earlier revisions of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.