
Abstract
This paper provides a first study into the complex setting of Emergency Medical Dispatch (EMD), through a textual trajectory lens. We draw on ongoing research on risk negotiation in emergency decision making and we unpack the process by which texts are produced and co-produced in the daily practice of multiprofessional teams making time sensitive, high-stakes decisions. We introduce an Interactional Sociolinguistic (IS) model, P.A.T.H.S. (standing for: Participants, Artefacts, Transition Stages, Historicity, Setting) to contribute to the study of how complex text trajectories work in professional settings, and the ensuing implications for research methodology and design, using EMD as a case in point. The paper discusses textual trajectories and illustrates the EMD textual ecosystem through P.A.T.H.S. before turning to a case to illustrate the patterns in our data. We close the paper with implications and directions for future research.
Keywords
Introduction
Texts 1 play a pivotal role in professional environments. They are multimodal, dynamic entities that evolve as they move through different contexts and are engaged with by different professionals. The inter-relationship and inter-connectivity of texts has drawn the attention of scholars in: writing (e.g., Allen, 2022; Mason, 2019), critical discursive studies (e.g., Fairclough, 2023; van Dijk, 1993, 2015), socio/applied linguistics(e.g., Holmes and Stubbe, 2015; Lillis and Maybin, 2017) among others; the inseparable relationship between text-context as well as the shift from a focus on writing as a product to the process (Paré, 2002; Prior, 2003, 2008) are common positions irrespective of disciplinary or methodological concerns. Despite this agreement, the process by which texts are produced, circulate and interact with other texts and (human) authors in a complex professional ecosystem is not well understood and has, by comparison, received limited attention. Relatively recently Komter (2012) discussed the interrelatedness between the (written) suspect statement and the (spoken) police interview as well as how the statement was de- and re-contextualised as it went from the interrogating room to the courtroom. Yet, there is rarely any similar research in the recent decade that features a text in its trajectory in a multi-actor system, not least in emergency services which is our focus.
Against this backdrop, this paper aims to discuss a complex and sensitive setting, that of Emergency Medical Dispatch (EMD), through a textual trajectory lens. We propose a model for capturing the process by which texts interact with one another when core actors make time-sensitive decisions in the EMD setting. We seek to contribute to the understanding of how complex text trajectories work in professional settings, and the ensuing implications for research methodology and design, using EMD as a case in point.
EMD is the process by which an ambulance service receives a healthcare-related emergency call through a national number and must decide which resource, if any, is appropriate to dispatch. EMD in the UK is operationalised via 999 emergency calls that are heavily regulated and processed through sequentially-prompted emergency triage protocols. EMD is designed and expected to provide rapid and efficient on-site responses to medical emergencies and injuries. But with limited human capacity and resources, delayed or inaccurate dispatch occurs more often than it should. Dispatch, especially that of pre-hospital critical care which delivers advanced clinical interventions for critically ill patients at the scene of incidents beyond the scope of standard ambulance services, has long been recognised as the weakest link in the chain of response, with a paucity of evidence to guide their optimal deployment (McQueen et al., 2015). Accordingly, there are calls to immediately strengthen EMD and emergency medical services both in the UK and internationally (Department of Health and Social Care, 2023; World Health Organization, 2019, 2023).
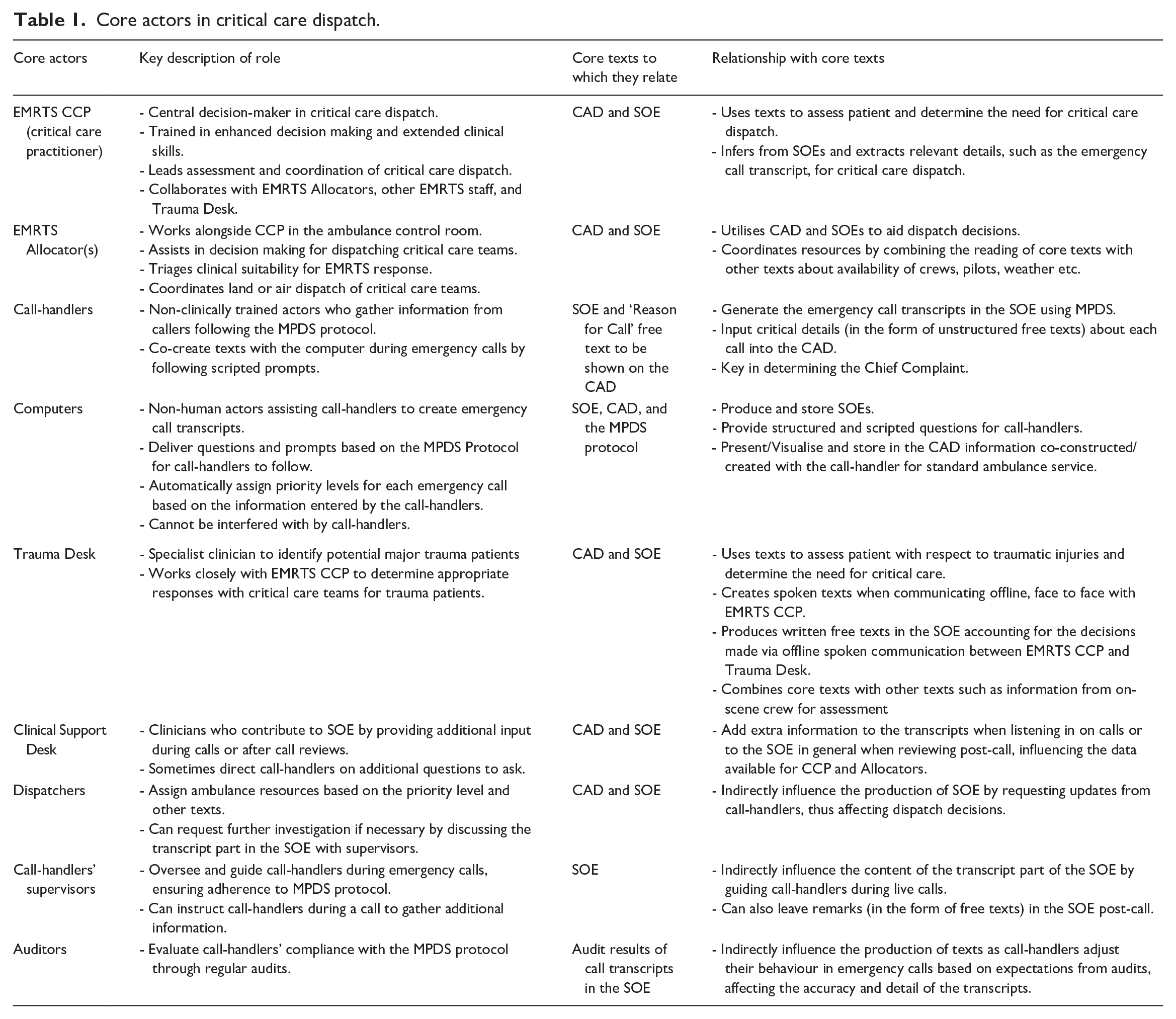
EMD is directly related to risk assessment and is the result of a decision-making process involving the caller and health care teams coordinated through an Emergency Operations Centre. This multi-actor process has not been systematically studied despite its immediate impact on patient safety and resource; it is the focus of ongoing research by the authors. In this paper, we (a) focus on mapping the key texts produced and used by the core stakeholders in the EMD decision making – namely the MPDS (Medical Priority Dispatch System) Protocol, the CAD (the interface of a Computer-Aided Dispatch software), the SOE (Sequence of Events record) and the emergency phone call (see Figure 2 and Table 2) – and (b) show the complexity of the system beyond the well-known caller/call-handler encounter, which, despite being a focal interactional site and a typically researched dyad, is but one single point in the whole chain.
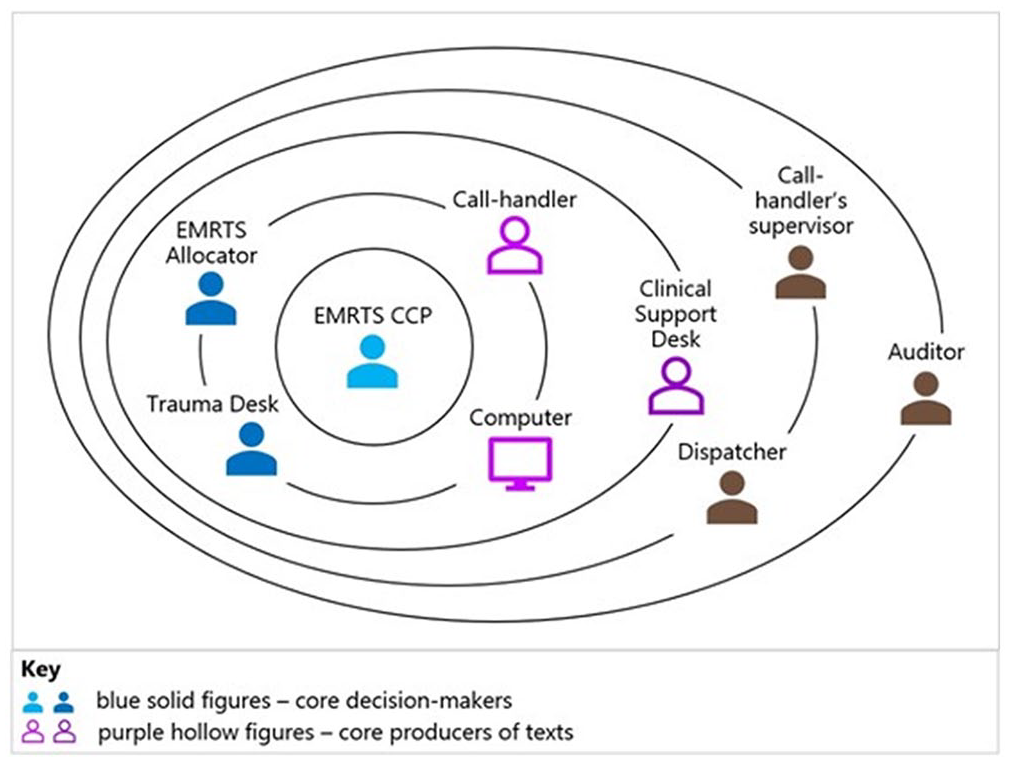
In more detail, behind and alongside the caller/call-handler, there is a multi-actor system which interprets risk indicators and makes (non-) dispatch decision of critical care resources. This multi-actor system involves operational and clinical staff and external agencies (see Figure 1 and Table 1). These individuals and teams communicate and interact in a number of ways: by internal (or inter-agency) telephone call, radio communication, or notes written into a specially developed digital system (the CAD). Each professional shares the common goal of delivering the most appropriate response to patients. Yet, each has access to a subtly nuanced (and restricted) information picture, and each has a role that is shaped by competing priorities. Each also produces texts spoken and written intended to add to the immediate task in hand in reaching a decision as well as to provide an account/a justification in this heavily regulated system where decisions come with medicolegal implications.
Core actors in critical care dispatch.
Core actors in critical care dispatch.
EMD is, therefore, a prime real-world example illustrating the need to understand the cumulative effect of the documents as agents in an ‘entire network of activities and agents of which it forms a part’ (Prior, 2003: 168). The professionals/actors involved in EMD produce different texts including records showing non-verbatim transcripts of speech, unstructured written notes (also known as ‘free texts’), formulaic written responses, and pre-set written texts selected by an actor. The production of these texts is multimodal, involving computer-based communication, phone conversations, and face-to-face interaction. We unpack this in the next sections and discuss the EMD system through text trajectories and introduce a framework for studying complex, high risk professional settings.
The paper is organised in seven parts. Part one elaborates on the textual trajectories with reference to workplace writing. Part two introduces the textual system in EMD. Part three explains the context and methodology of our ongoing project on EMD, as an exemplification for our proposed model. Part four and five each illustrates two elements of the model, contextualised in the EMD system. Part six provides a case example on the co-constitutive relationship between texts. Part seven comprises our final discussion of the proposed model and concluding remarks.
Workplace writing: The silent journey of textual trajectories
Workplace writing is a high-stakes activity: it carries implications for individuals, teams and the ability of systems to cope with the complexity of information they need to handle, and has immediate real-world results. In the majority of workplaces, texts are the product of ‘document cycling’, where they are passed back and forth among various contributors for review and revision (Paradis et al., 1985). In written texts, it is often considered difficult to attribute authorship to a single individual and to distinguish between human agency and institutional requirements.
With the perspective of intertextuality (see e.g., Johnstone and Andrus, 2024), texts always contain other texts produced in other places and times (Prior, 2003: 122); they make sense due to their relationships with these other texts (Coffey, 2014: 373) and play an active role in perpetuating dominant structures and mechanisms of control in bureaucratic workplaces (Sarangi and Slembrouck, 1996). Readers and users of texts consider the (whole) network of relations among those – and other – texts (Allen, 2022: 1). Going from one context to the next continuously means that texts are constantly decontextualised and recontextualised (Blommaert, 2005: 76), which with the texts carry out a sequence of performances wherein meaning would be ‘produced, reproduced, translated, and transformed’ (Bens, 2021: 144). On the one hand, ‘initial functions often get removed’, on the other hand, traits that do not appear as prominent at the beginning will be accumulated and added to later stages (Blommaert, 2005: 76).
The few studies on trajectories of texts highlighted the pervasiveness and significance of textual trajectories for understanding the practices that constitute the modern workplace (Komter, 2012; Lillis and Maybin, 2017) as well as the relationship between ‘the system’ and ‘the user’ in bureaucratic societies (Sarangi and Roberts, 1999; Sarangi and Slembrouck, 1996). In line with those studies, we use trajectories as a meta-term to refer to a variety of terms and concepts from genre/chains to discourse itineraries to en-, de- and re-textualisation. We also consider it a useful term to capture the situated and time-sensitive nature of text interaction with other artefacts and actors. ‘Trajectories’, in effect, points to: the dynamic nature of texts as they transcend and transform teams and professional boundaries; their stability as ‘nodes’ of organisational practice; and their role in reflecting and perpetuating power dynamics at work. This is a discursive process which goes to the heart of the ways in which many workplaces in general and medical in particular operate: professionals work in teams which need to align understanding of a situation and allocation of resource, account for decisions made for the respective regulator and meet societal expectation for efficiency in providing services. Texts are central, deeply ingrained in this process, and have immediate accountability implications. This is the case in medical decision making, and certainly in interactions not directed to the frontend (cf. Rock, 2017, 2018). Examining text trajectories, then, means delving into these directionalities, movements, and changes in the production and uptake of texts across time and social space, and the relationships among them, that are captured in that organised setting (Lillis and Maybin, 2017: 409–410). This entails tracking and studying the production, consumption, circulation, and archiving processes of the texts, ‘be they technical, linguistic or conceptual’ and situating texts in both their social and textual contexts (Coffey, 2014: 370). We next turn to the under-researched and uncharted EMD context.
The EMD (textual) system
In EMD, scripted systems and different formal and informal sequences of questions/answers (Hayashi, 2019; Perera et al., 2022) are central in the decision-making process for providing care and ensuring systematic, efficient and equal access to resources. Since 1974 when a paramedic provided unscripted advice and pre-arrival instructions over the phone (Dunford, 2002), the importance of call-handler-assisted instructions has been growing in implementation and research activity. The introduction of scripted systems, notably the MPDS in 1979 in the US was landmark in standardising the dispatch process, offering structured protocols for information gathering and resource allocation. In 1991, the London Ambulance Service became the first UK service to implement a CAD system, another important technological advancement aimed at improving dispatch efficiency and accuracy. By 1997, the UK NHS (National Health Service) incorporated MPDS as part of a nationwide standard for dispatch, 2 ensuring uniformity in the handling of medical emergencies, optimising resource allocation across the country’s healthcare system, and reducing risks for patients and the system. Platform(s) in use for dispatch continued to develop and different variants exist, however their intertextual processes are omnirelevant.
As resource allocation emerged as a critical concern, dispatch protocols were designed not only to assist callers but also to optimise the emergency response system by reducing over- and under-response, both with obvious adverse outcomes for patients. However, limitations of scripted systems to handle the complexity of risk negotiations are also often documented (Fotland et al., 2024; Riou et al., 2018a; Wennlund et al., 2022).
Risk indexing is, largely, a linguistic act and in high-stakes situations, it is interactionally complex. It involves the combined use of a range of linguistic indicators: from lexis, to breathing, high pitch voice and silence (e.g., Booker et al., 2018; Coffey et al., 2018; Riou et al., 2018b) to repetition and ellipsis. EMD must provide a rapid, efficient on-site response, based on successful assessment of those indicators. Scripted systems can quickly and efficiently recognise some of the speech risk indicators (e.g., lexical indicators), but other risk indicators are less easy to codify (e.g., intonation). Scripted systems, therefore, rely on the interaction skills of the call-handler, who, however, cannot deviate from the systems. Further, the EMD environment is one where service-users and service-providers need to align worldviews and expectations. Scripted systems follow a text architecture that is designed by the recipient institution; however, the input is provided by a lay user who is not familiar with the institutions’ rituals and is using ordinary conversation architecture for communicating urgency, while the call-handler is legally bounded to adhere to the script. This results in the call-handler and the caller negotiating at the interface of two different codes in an emergency call encounter. This translation between two codes is fraught with risk points for information loss and heavily constrained by the non-human actors involved in the process. Adding on top the characteristics of telephone communication (e.g., lack of visual cues, communication breakdown, noise), the challenges multiply and can hinder the process of appropriate decision-making. This can and does result in inaccurate assessment: overuse of ambulances and under-detection of critical illness and injury, exactly what scripted systems aimed to reduce.
Risk indexing gets further complexified by the fact the caller/call-handler dyad is only one part of a complex and fast-paced decision-making environment. Undoubtedly significant, it is the only dimension linguistic research has examined in some detail focusing on the spoken interaction between the two actors (Riou, 2024). This misses the work of a very active and busy backstage in the ambulance control room where multiple actors and texts work together for decision making (see Figures 1 and 2 for an overview and Figure 15 for a full representation). There are various paths through which multiprofessional teams draw on the call-handlers’ interpretation of risk indicators and reinterpret them in their own decision making of appropriate course of action. In doing so, they transfer and transform risk, which, in its turn, feeds into the overall dispatch decision. As risk indicators are picked by the different stakeholders, a process of de- and re-contextualisation and repositioning of the encounter in general and risk in particular is taking place. The iterative process of teams negotiating risk (illustrated by the various paths/arrows in Figure 15) is simultaneously transient (dynamic) and permanent (recorded) so that the contributions/impacts of the actors with the texts can be audited.
Linguistic research is still very limited in EMD in general. In this paper, we provide a landscape, through the model that we are proposing, of the process from when an emergency phone call is made to the management of the call in the backstage, encompassing the core actors and the core texts interacting in the negotiation of the decision. Our proposed model contributes to linguistic research in EMD and goes beyond to provide a heuristic for supporting Interactional Sociolinguistic (IS) research in healthcare settings.
The 999RESPOND context and methodology
We draw on data from an ongoing project (999RESPOND) researching the EMD decision making ecosystem and seeking to identify patterns in the communication between caller/call-handler and call-handler/backstage teams. The work is based on ongoing interdisciplinary collaboration with the Welsh Ambulance Service (WAST) and a critical care provider – Emergency Medical Retrieval and Transfer Service (EMRTS). WAST covers an area of 20,640 km with around three million people. EMRTS serves the same terrain and population with four bases across Wales. Both operate 24/7. WAST receives 1400 calls per day on average, among which 140 are triaged for EMRTS deployment, and 10 calls are allocated to EMRTS. This is a busy system and inter-agency partnership that attempts to serve a diverse sociodemographic and geographic/topological challenges of a nationally-boundaried health system. Whereas the project draws on data from the ambulance and critical care service from Wales, the examples and visual representations of system architectures concern matters of wider relevance in EMD. We will return to issues of research design for the study of textual trajectories in the discussion part of this paper.
Our design includes five datasets: 1. audio recordings of original 999 emergency phone calls; 2. audio recordings of the backstage team interactions; 3. the SOE textual record; 4. policy, operating procedures and service guidelines relating to critical care dispatch; 5. ethnographic observations.
We associate the datasets with three analytical levels of analysis: the interactional moment (micro level), the team (meso level) and the policy (institutional level). We take an Interactional Sociolinguistic (IS) perspective. IS is typically associated with spoken texts; we argue, however, that this points to how researchers have used the approach rather than the approach itself. To the contrary, IS is a theory of context and a programme of work which allows researchers to make structural connections between the analysis of a text and the sociocultural environments of the teams where those texts are co-produced, negotiated, revisited and changed (Angouri, 2018; Holmes et al., 2011). We use IS to explore the relationship between the situated moment of emergency decision making and the wider environment where teams operate (Figures 1 and 15), working closely in collaboration with the professionals in the ecosystem. This participatory/real-world aspect of our project is, in our approach, a core condition for studying complex systems such as EMD. In line with our IS foundation, we situate the core of our interest in the interaction between all core stakeholders but seek to make connections with the wider organisational context of the service providers and the macro-societal expectations within which the system operates (see also the Language in the Workplace Project, e.g., Holmes and Vine, 2021). IS enables us to study the decision-making process through analysing the spoken interaction between all stakeholders (e.g., callers, call-handlers, clinical staff) and the written artefacts they produce.
IS looks into patterns of language use in specific settings and domains of activity. It studies what is unmarked, the interactional norms of particular groups, and clashes that may result from different interactional priorities and agendas. IS shares tools and techniques with Conversation Analysis (CA) on the detailed analysis of interaction and sits at the interface of sociology and sociolinguistics. Both IS and CA systematically examine interactions as patterned communication seen as ‘practice’. Unlike CA, however, IS moves beyond the sequential organisation of the encounter. Drawing on ethnographically informed methodology, it connects the situated moment (micro/interactional context) with the wider organisational and sociocultural context (macro/policy context) within which the speakers operate. This reflects the foundational work of John Gumperz and Dell Hymes who put emphasis on the dialectic relationship between cues (linguistic signs) and the sociocultural knowledge users mobilise, which, is directly relevant to studying and capturing textual trajectories. IS has traditionally been multi-method and has also looked into institutional documents as significant sites where institutional priorities and control are enacted and perpetuated (e.g., Gumperz, 1999) but without becoming particularly visible in research on workplace writing.
More broadly, IS has not managed to become as established as other approaches, notably CA, for the analysis of workplace interaction, spoken or written – if one maintains a binary between the two. A detailed discussion on this goes beyond the scope of this paper (see Angouri and Holmes in prep). In brief, however, IS has never put forward a ‘set’ analytical toolkit. To the contrary, it has encouraged a fairly eclectic, albeit clearly linguistic, programme of work. This brings fluidity but also lacks a structure that poses challenges, particularly to those coming new to the field or paradigm. Capturing the dialectic between linguistic cues and the social order requires: interdisciplinary design and multiprofessional expertise, access (subject to timely ethics approval for complex projects) and disciplinary expertise in combining macro-micro analytical tools. IS allows, or even requires, the researcher to choose analytical tools, which makes it much more complex, although fluid, to teach and implement.
Our work contributes to the development of IS and adds to the toolkit for sociolinguistic workplace studies. Building on IS foundational work, we propose a framework to explore core dimensions of textual trajectories. This seeks to provide a heuristic for approaching a complex system and deciding ‘how much context’ is relevant for textual trajectory work to be possible (note the well-known and widely cited debates between traditions concerning how much or little and what ought to be included in the context when analysing texts, e.g., Heritage, 1987; Schegloff, 1997). We propose a model under the acronym P.A.T.H.S. which captures what we consider the core aspects of context: actors, artefacts, sequence of events in an EMD case and the relationship between past/present texts and their projected impact on future.
P.A.T.H.S.:
P - Participants (Actors): Who is involved in creating, revising, using and interpreting the text?
A - Artefacts (Text Types): What forms and genres does the text take and belong to?
T – Transition stages (Sequence of Events/Time): How does the text evolve through different stages?
H – Historicity (Stability/Change): Does the text stay stable or undergo changes over time?
S – Setting (The immediate environment): Where does the text appear?
The P.A.T.H.S. model seeks to capture aspects of practice that ‘form’ the context from which researchers can adequately draw inferences when analysing multiprofessional interaction in medical emergency settings. Although it reduces the richness of ethnographic material a researcher may have access to, it aims to provide a scaffold upon which complexity can be progressively build.
To sum up, non-sociolinguistic studies call for theoretical/analytical tools for examining interrelatedness in written and spoken discourse (e.g., Mason, 2019), and specifically to track how what is already written and already read in previous texts affects the ways in which future texts are read and interpreted by multiple human and non-human actors in a workplace context. IS provides those tools and an opportunity to expand and extend a valuable approach that has yet to reach its full potential. We will revisit the P.A.T.H.S. model in the light of our data and findings to which we turn next.
The EMD textual ecosystem and core actors – Participants and Artefacts
When an emergency call is answered by a call-handler in the ambulance control room, it initiates an activity system which involves human and non-human actors in fast-paced interaction. Applying P.A.T.H.S., Figure 1 is a simple representation to overview the core human actors (Participants) engaging in producing, utilising, and re-producing texts (Artefacts) central to dispatch decision. Some actors contribute more to creating the texts while others contribute more to making decisions from reading the texts.
More specifically, the activity system begins when the call-handler, following categorisation of emergencies, initiates a scripted and standardised Question-Answer sequence which generates a non-verbatim transcript to be incorporated inside a larger written recorded called SOE (to be discussed later). This text, in its turn, interacts with others in the process of assessing the risk level and the appropriate type of response and resource. There are nine roles and four core texts in the EMD ecosystem we illustrate here (respectively with Figure 1, Table 1, and Figure 2, Table 2).
Core texts in critical care dispatch.
Core texts for critical care dispatch.

The relationship between actors and text is both multilayered and multifaceted. Each text interacts with others and directly or indirectly influences dispatch decision. Meanwhile, the roles in the control room bear different institutional responsibilities, hence engage with the texts and the decision-making process from their own unique perspective. For example, a high-priority case according to the MPDS Protocol designed for standard ambulance service may not necessarily require pre-hospital critical care. Similarly, the questions asked by call-takers, who follow the MPDS Protocol, may not capture the information needed for critical care decision-making, so the CCP and Allocator(s) need to delve deeper into the SOE to make informed choices. The CCP and Allocator(s) must interpret the texts to determine a course of action for which they are accountable; in doing so they re/de- contextualise texts produced at different stages of the process.
In their turn, core texts provide both stable ‘nodes’ in the decision-making process and follow the dynamic nature of the event which shifts and changes. We summarise the core texts human actors work with in Table 2.
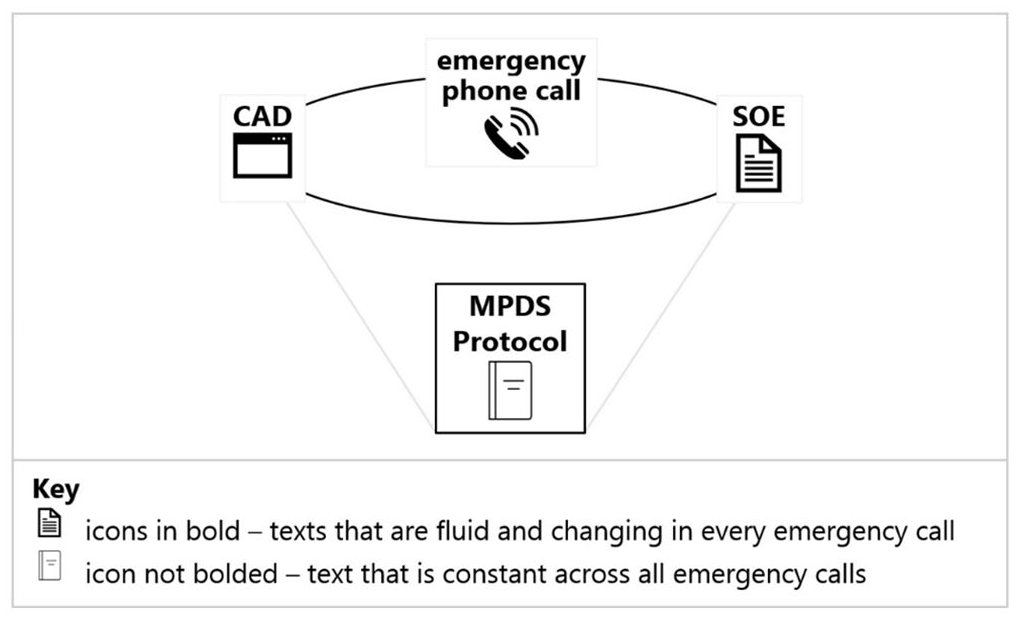
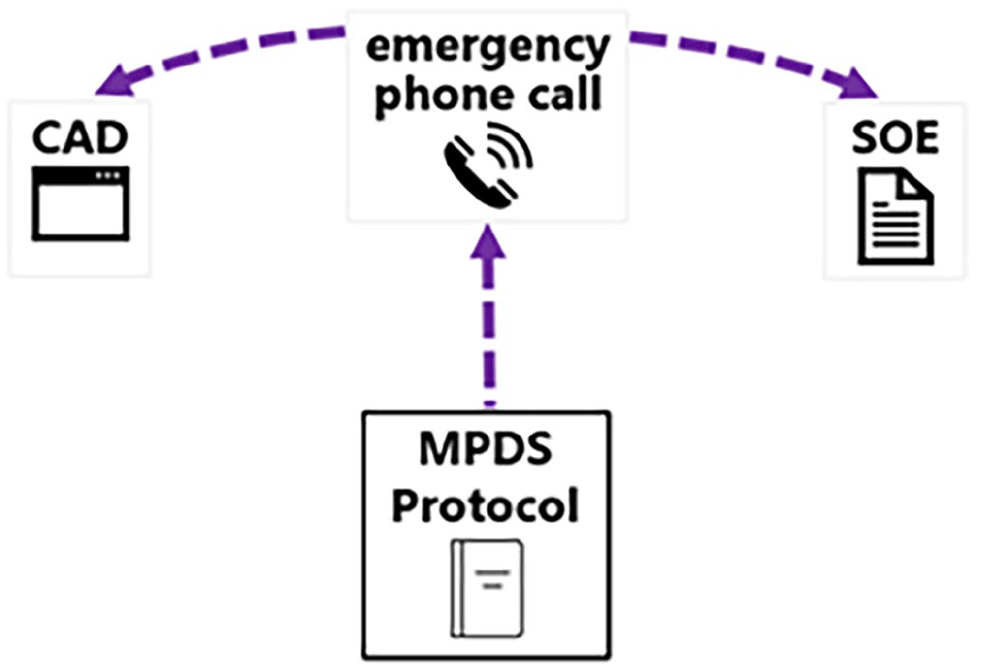
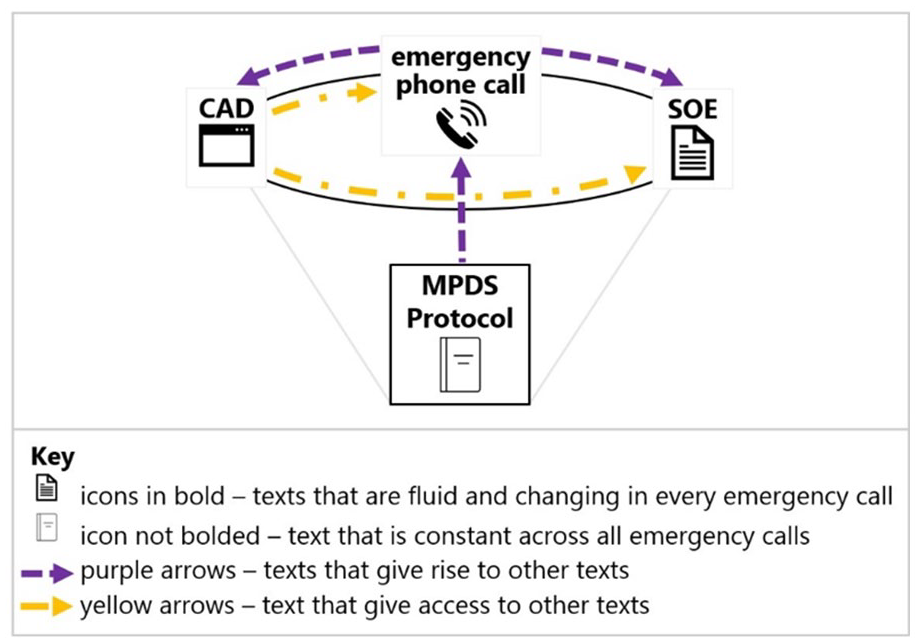
The central role of the MPDS Protocol and dynamic nature of the SOE and CAD indicate the parameters within which the human actors operate. As we will further discuss, the MPDS Protocol provides a stable textual context for the human actors to produce other texts in the system and acts as a reference point to which the human actors can anchor their reading of these other texts produced in this context of activity. Represented in Figure 2, the MPDS Protocol is placed in the square in the centre of the other core texts and remains fixed for all emergency calls, whereas the other three sets of texts placed on the circle differ in each emergency call, adding variability to how the human actors interact with each other via texts and intricacy to the decision-making process.
When core actors enact their roles by producing, using, and circulating texts within their strictly regulated positions, they reproduce their professional roles and institutional boundaries. Texts permeate those boundaries and flow; they both influence and are influenced by the process. An understanding of the texts requires an understanding of this ecosystem and, concurrently, provides a mapping of this ecosystem.
The textual journey takes different channels depending on the form and function of the texts. Texts are produced digitally on the computer, verbally on the phone and subsequently entextualised/recontextualised, verbally face to face and subsequently entextualised/recontextualised. They bridge stability and change, and all directly or indirectly contribute to the decision-making of critical care dispatch. We show this through one case in the next section of the paper before turning to a discussion and concluding remarks.
Sequence and temporality: Transition and historicity
The visual representation shows the sequence of production and engagement of texts with other texts and authors. It draws on ethnographic observations and the analysis of cases that form our sample.
Sequence of text production
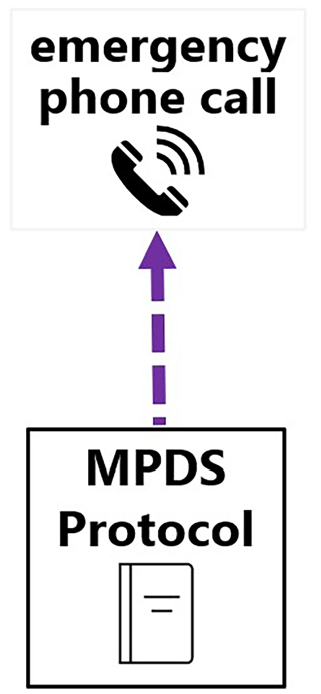
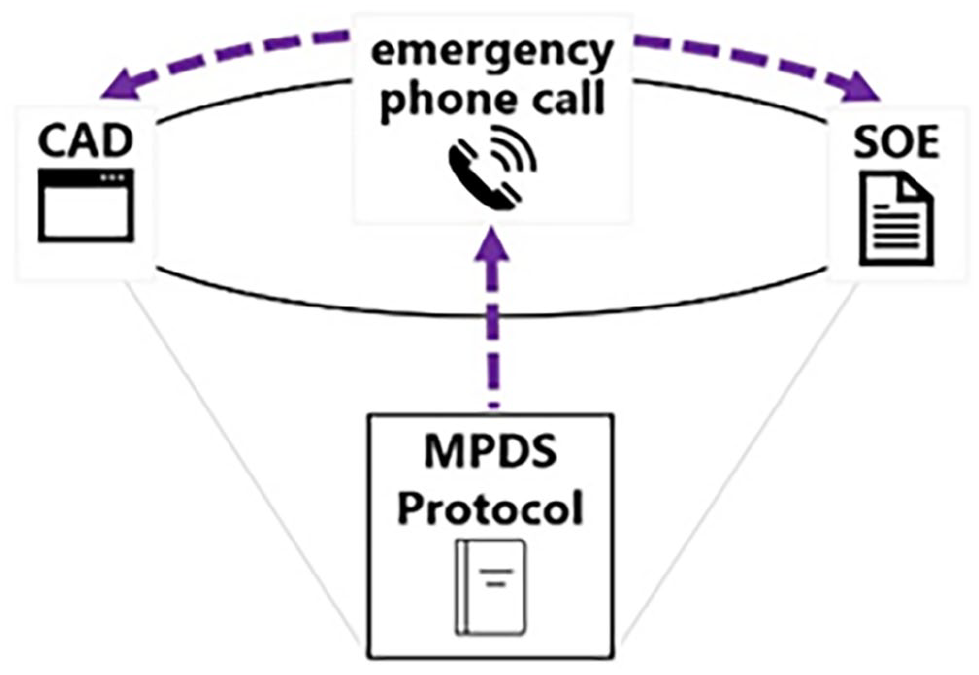
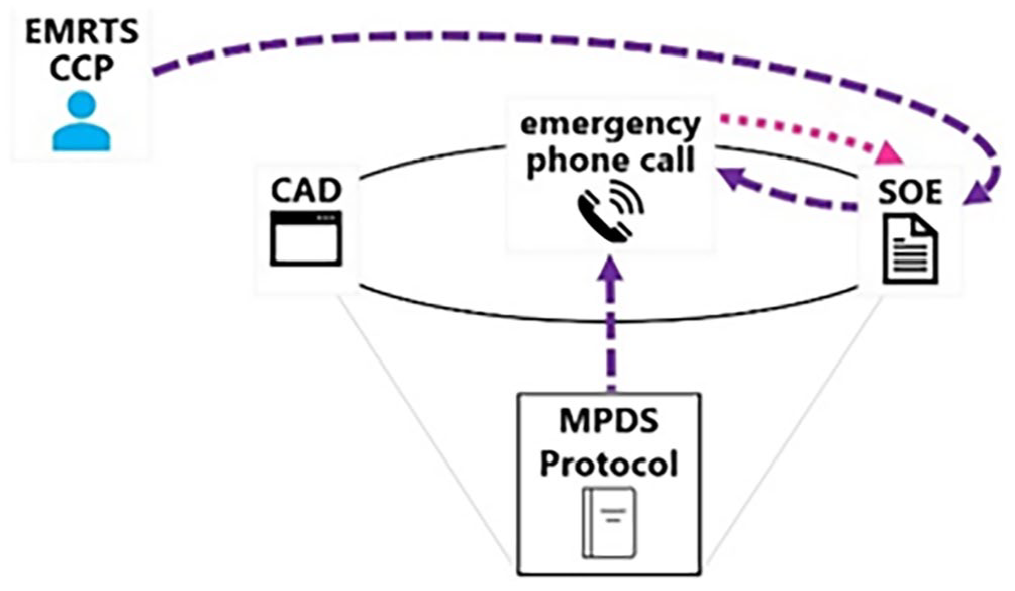
Call handlers are trained to follow the MPDS Protocol to take emergency phone calls. The MPDS Protocol itself is a significant actor, giving rise to (the recording of) every emergency phone call (Figure 3). The content of the phone call then becomes a source that form the CAD and the SOE (Figure 4). Further, the phone call and SOE from every case 3 are different, together with the CAD that keeps updating itself when a new phone call comes in, these three texts are fluid and keep changing; whereas the MPDS Protocol remains constant across all cases, often providing the foundation for understanding the shifting nature of those three texts (Figure 5).
Sequence of text production (1).
Sequence of text production (2).
Sequence of text production (3).
Sequence of accessing the texts
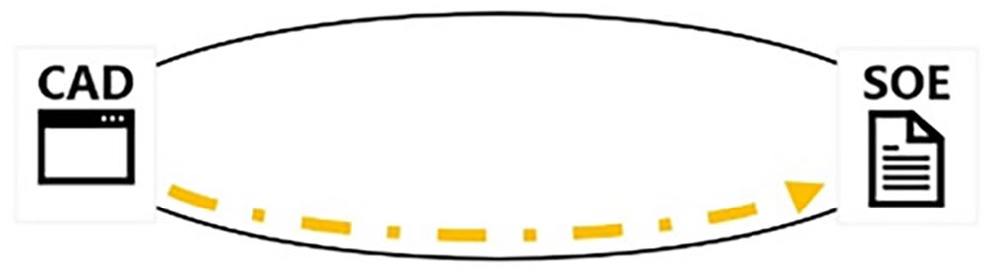
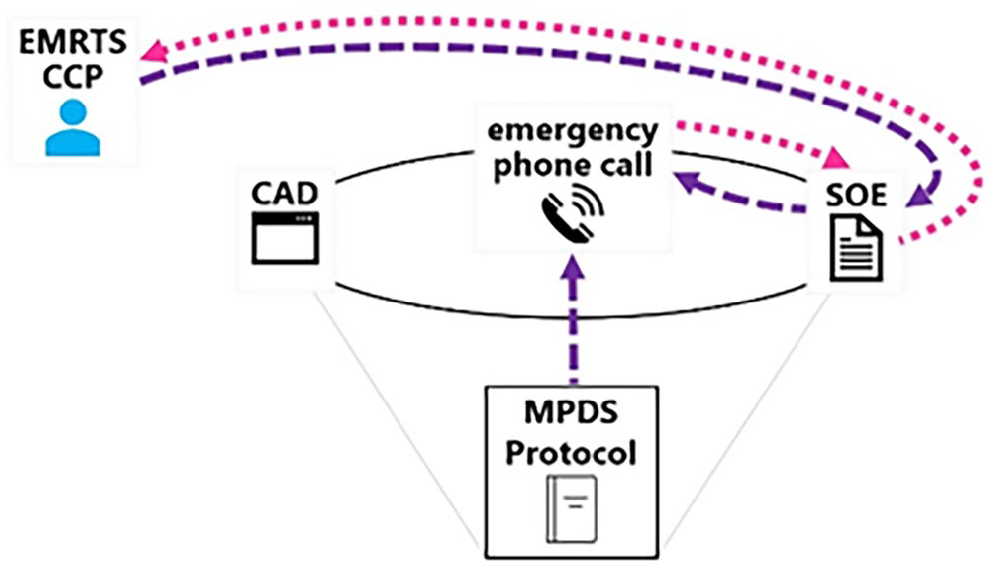
The sequence of text production in this setting differs from the sequence with which actors – other than the call-handlers – can access the texts. For instance, actors such as clinical professionals first get to see – thus learn about the existence of – a case from the CAD (as a text) (Figure 6). If the case contains elements that they consider appropriate for focused attention, they can open the case from the CAD (as a platform) to access its SOE (Figure 7). On the SOE, they can see clinically significant information gathered from and for the MDPS Protocol like the Key Questions from each Chief Complaint Protocol. They can also see, if any, the unstructured free texts that other actors – such as call-handlers, dispatchers, different clinicians – have already added by the time they access the SOE. If they want to get more information, they can access the phone call from the CAD (Figure 8). They can listen to both the phone call live when it is in progress and a recording of the phone call after it has ended.
Sequence of accessing the texts (1).
Sequence of accessing the texts (2).

Sequence of accessing the texts (3).
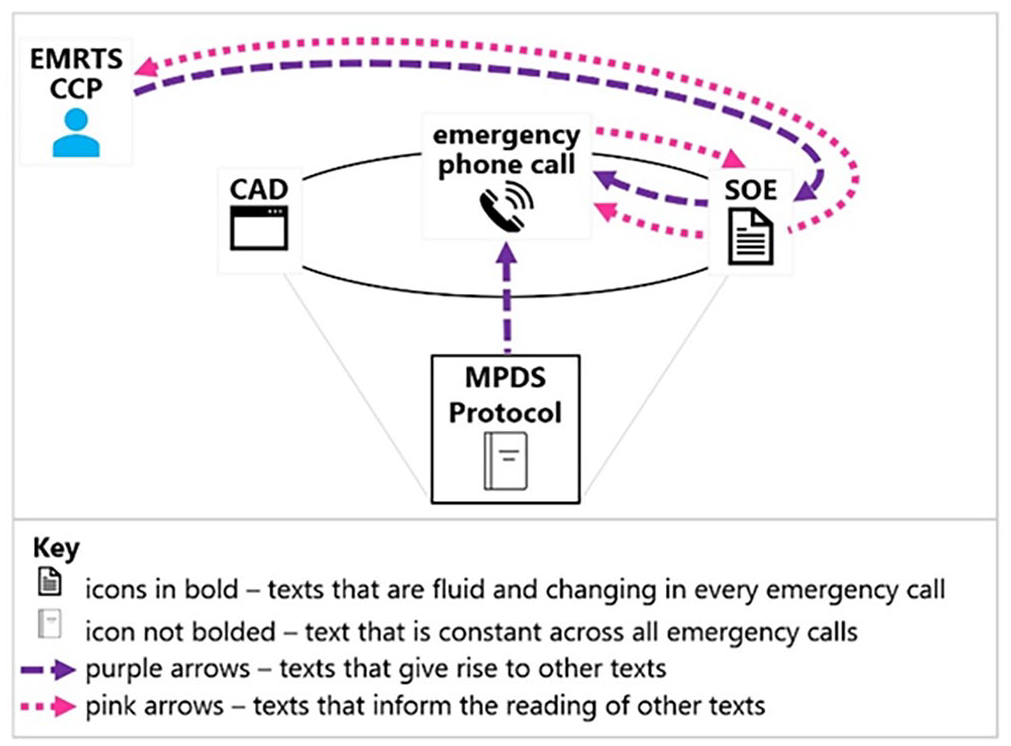
In summary then, a phone call comes into existence first before it very quickly appears on the CAD. This differs from the sequence for accessing these texts as actors do not know about the existence of a case, thus the call, until they see it on the CAD from which they can access it (Figure 9). The sequence of events is enacted in and through the texts produced at each stage, some of which are stable and some change. Looking into sequencing is directly related to the temporal dimension of text production, circulation and use.
Sequences and Transition of core texts.
Temporality
The MPDS Protocol is set and pre-exists any emergency phone call. The phone call comes into existence when a call-handler starts the conversation with a caller. It is live during the conversation, structured by the MPDS Protocol and sometimes supplemented by other actors, such as clinicians. It stops evolving after the call-handler ends the call and stays as a permanent audio record.
The SOE starts to form also when a call-handler starts talking to the caller. It grows when the phone call is in progress through recording not just key information that the call-handler obtains in accordance with the MPDS Protocol, but also ‘technical communication’ made among teams, such as on dispatch issues. The SOE keeps expanding with the technical communication even after the phone call has ended, all the way until the patient has gone into the hospital and the case is closed. For example, after a phone call has ended, an actor such as a CCP can communicate with other teams – such as the Clinical Support Desk, the Trauma Desk and the crew at scene, and then add free text notes to the SOE subsequently to record their discussion.
The relationship between the MPDS Protocol, the emergency phone call, the CAD, and the SOE is one of stability and change. The spoken interactions get entextualised and the written texts are de/recontextualised in mutual co-construction of the case. This is visually represented in Figure 10 and further illustrated in the case example that follows.
Temporality and Historicity of core texts.
Texts and intertexts: A case example
We turn to illustrate the co-constitutive relationship between texts and how they operate in direct reference between them. The case below illustrate the need of the aspects included in P.A.T.H.S. for unpacking the non-linear, multi-factoraltextual trajectory in EMD. We begin our illustration with the SOE (Extract 1).
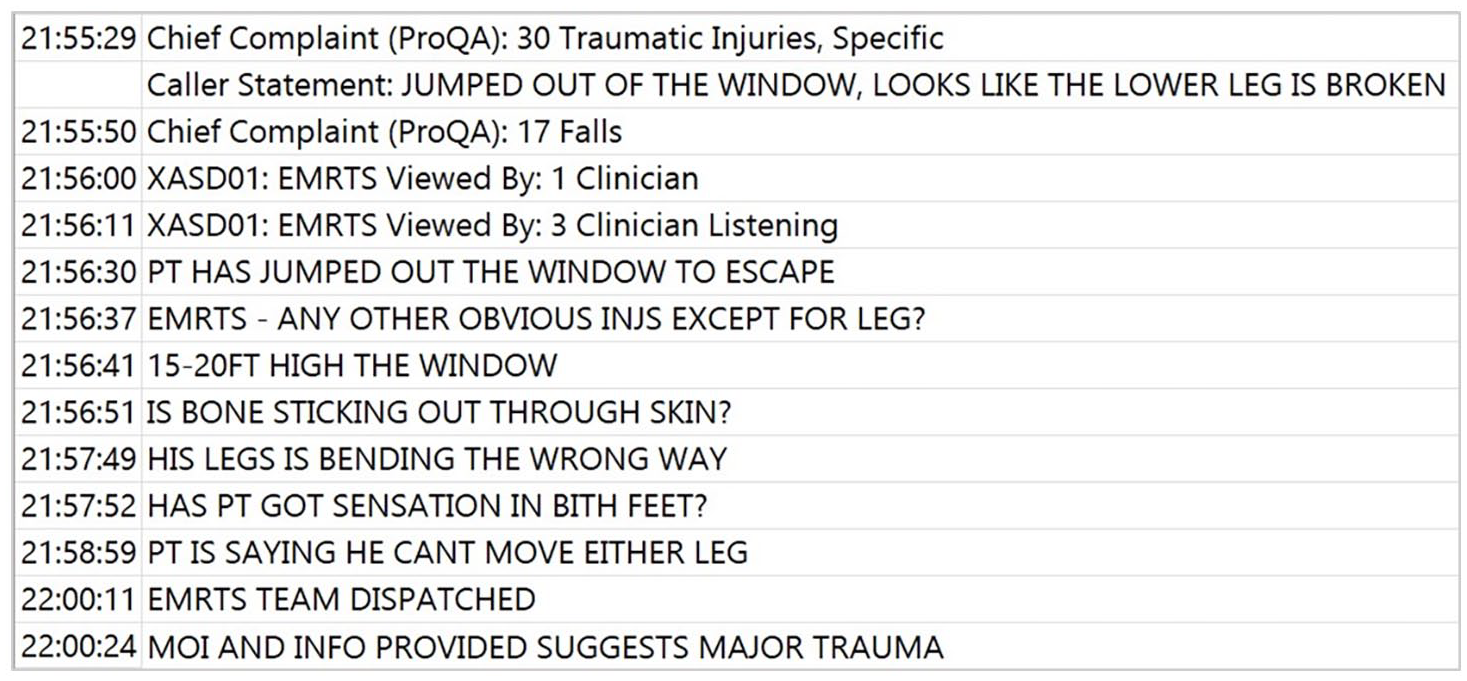
This is a case where, in the initial part of the call, the patient reported to have broken a leg by jumping from a house. Accordingly, the Chief Complaint was first shown on the SOE to be Traumatic Injuries 3 minutes into call (at 21:55:29). In the half minute after that, the Chief Complaint changed to Falls (at 21:55:50). (This change would also be visible on the CAD.) Around another four and a half minutes later, a CCP added that ‘MOI [mechanism of injuries] and info provided suggests major trauma’ (at 22:00:24).
Between that change of Chief Complaint and the entry about major trauma, a CCP entered clinicians were listening in the phone call. Three questions were posed by the CCP for the call-handler to ask the caller at 21:56:37, 21:56:51 and 21:57:52. This was followed by eight Key Questions from the MPDS Protocol that the call-handler completed (not shown in Extract 1).
The SOE, however, does not detail answers to those three questions. The researcher must access the phone call to find out what the clinicians had acquired through listening to more than 4 minutes of conversation before deciding that case was major trauma. We present relevant extracts of the transcript below using CA conventions (Jefferson, 2004) to visualise the interaction. We focus in particular on the interactional feature of Question-Answer sequence in the analysis/reading. In the transcript (Extract 2), C stands for caller; C-H for call-handler; Y for another person at scene.

The phone call shows that the call-handler did relay the three questions to the caller (lines 126–127, 138–139, 172) and the caller did respond to the questions accordingly (lines 132–137, 141–146, 175–179). The phone call also shows the extra information given on the caller side. Therefore, although those answers were not recorded in the SOE, the clinicians did receive direct responses to what they wanted to know from the phone call.
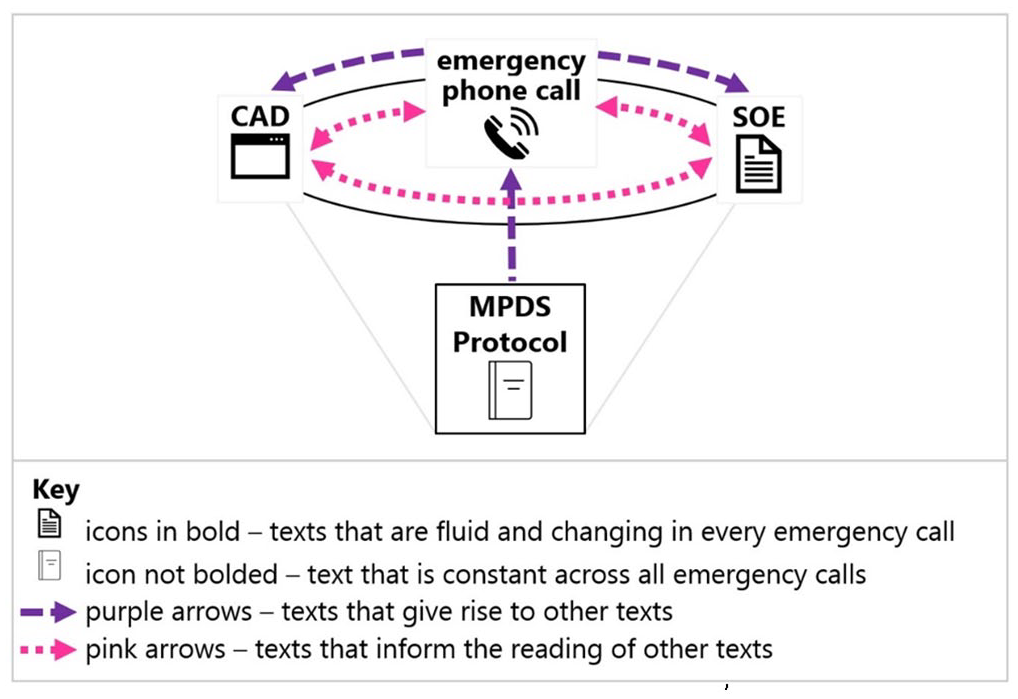
On the one hand, the entries on the SOE show that in addition to the MPDS Protocol, the CCP was a second source that co-produced the phone call in this case (Figure 11). On the other hand, the SOE shows that this text itself does not contain full details of the whole story and provides a hint that one needs to look next at the phone call to find the missing details. The phone call thus informs the reading of the SOE (Figure 12) by providing substance to the information visible in the SOE but unexplained or inadequately explained by the SOE itself. The phone call constitutes more than extra contextual information for the researcher; it is the missing piece without which the story told in the SOE could not be complete. At the same time the phone call in and by itself is not enough to understand how and why decisions were made.
Case example: co-production of texts.
Case example: interactions between texts and actors (1).
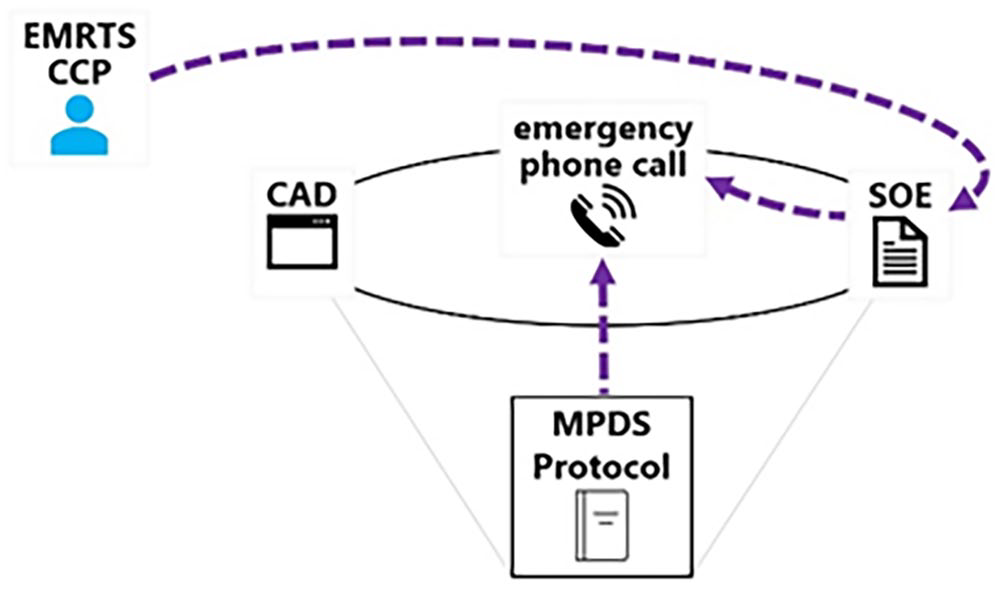
In this particular case, this part of the phone call is especially important. It is because the CCP also entered in the SOE that a critical care team was dispatched (at 22:00:11) right before the entry pointing out major trauma. The latter entry functioned as a justification for the clinicians’ dispatch decision and is an essential piece of contextualisation here (Figure 13).
Case example: interactions between texts and actors (2).
Each part of the system are necessary to capture how decisions are ‘done’ in situ. In a scenario like this example, the MPDS Protocol alone is inadequate to explain what took place in the phone call, that is, the MPDS Protocol cannot account for the source of some questions that the call-handler asked. It is the SOE that displays clinicians added three questions one by one. The SOE supports the reading the phone call (Figure 14) by enabling one to recognise that the call-handler was indeed interweaving those three extra questions with the Key Questions from the MPDS Protocol. (Two examples can be found in lines 149–150 and 159 of the phone call.) Otherwise, the phone call itself cannot explain why the call-handler led the conversation in the way they did. As such, one needs to read the phone call to understand the SOE, one also needs to read the SOE to understand the phone call. We bring this together in the next section under the model we are proposing.
Case example: interactions between texts and actors (3).
Mapping the P.A.T.H.S.: Discussion and concluding remarks
Our analysis has shown that the boundaries between spoken-written, single-multiple, stable-dynamic texts are porous; binaries are artificial and too rigid to capture the nature of communication practices in complex ecosystems such as the EMD. ‘Complex’ is an inflated term used more or less loosely across disciplines to denote a number of different dimensions, and more often than not to stand as a metaphor for ‘complicated’. However complex system research (Ladyman et al., 2013; Ladyman and Wiesner, 2020) has been growing and provides useful conceptual tools for broader interdisciplinary research (e.g., Jacobson et al., 2019; Widmer et al., 2018). Complex systems evolve and are non linear; they are standardised but also versatile (Ladyman and Wiesner, 2020). In order to be studied, disciplines need to develop frameworks and tools that capture the interactivity between the components of systems, the behaviour of whom and which cannot be captured by looking into any of the individual parts or dyads in isolation.
EMD is a multifactorial, multiprofessional system; optimal functioning of the system presupposes teams of professionals aligning perceptions of risk while balancing the resource available and the, often contradictory, priorities and teams’ capabilities. The study of trajectories of texts provides an insight into the ways in which professionals work to match these competing priorities and provide critical care where it is needed the most.
In professional sociolinguistic research the analysis of interrelatedness in (written and spoken) discourse is still underdeveloped. Few analytical tools exist to track how earlier texts shape the reading and interpretation of later ones by different actors during interactions. There is however no agreed framework to clearly illustrate how texts evolve in meaning as they are circulated, discussed, and associated across various interactions. Research needs to provide approaches that not only trace the trajectory of texts but also examine which parts different groups or stakeholders focus on and react to, based on their roles (e.g., Dall and Sarangi, 2018). Investigating how different segments of the same texts interact with various actors sheds light on the complete meaning of ‘text sets’ within its context. In its turn, this provide a more comprehensive understanding of how texts produce, transform, and interconnect as they circulate.
Against this backdrop, Figure 15 shows a full data-driven representation of the ambulance control room and both human and non-human actors in the decision making process based on an IS approach. Applying P.A.T.H.S., we landscape how multiple relevant actors (Participants) engage in re-producing a written record for dispatch decisions via different text types (Artefacts), including the latter’s sequential structure and travel directions (Transition stages and Historicity) in the EMD setting.
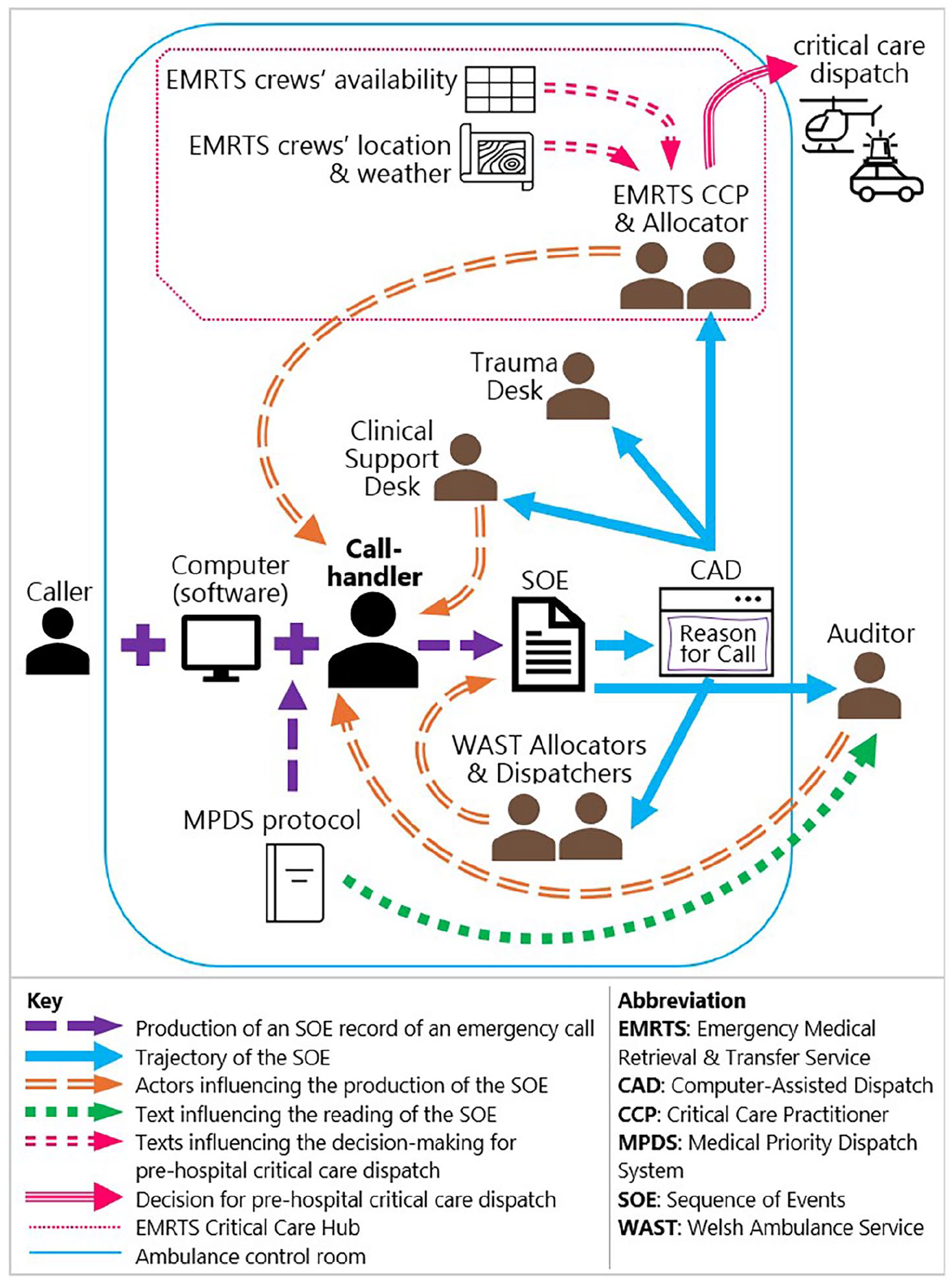
Landscaping the EMD textual system with its core actors and core texts.
The graph indicates how the core text of the SOE is initially produced (the purple arrows) and the directions through which it flows to other core actors after it is produced (the blue arrows). It also indicates which actors can influence the production of this core text (the orange arrows), both at the same time and space inside the ambulance control room and outside this time and space, as well as what other texts can influence the reading of this core text (the green and the pink arrows).
We use IS as the foundation and framework to implement P.A.T.H.S. which adds to methodological applications for future studies in this area. With Figures 1 and 2, and others in the case example, we show, through P.A.T.H.S, how researchers could visualise, or itemise, their understanding of the context, to see whether that is appropriate and sufficient for a research focus. When researchers develop their research to another focus or another relevant setting, they can modify from this established understanding to suit the needs of their new research.
IS, as a sociolinguistic approach, goes beyond the linguistic analysis of the interaction. Existing research has illustrated the potential of IS research for policy and training interventions relevant for medical teams at the frontline and professionals operating in high-stakes medical contexts (e.g., Angouri et al., 2022; Slade et al., 2015). It is also maintained that training interventions should draw on a systematic, and ideally multimodal, analysis of specific medical interaction that is sensitive to the context of that medical practice and the different specialities collaborating in that setting (Stubbe et al., 2021). This is the potential but also where complexity with IS itself lies.
Further, an IS-based piece of work needs to combine the analysis of linguistic cues with ethnographically informed methodologies, observations, interviews and document analysis. IS, then, is a programme and approach that allows to study the textual trajectories not solely because of the linguistic tools it brings, but more importantly, because it provides the conditions for these linguistic tools to interface with other methods and translate the findings to real world applications. IS can support multiprofessional teams and give the tools for social and health scientists to apply and translate research together. This is a model for future interdisciplinary enquiry which is a high priority for policymakers and a need for addressing effectively challenging problems making the best use of research capability and expertise. In real world contexts, such as the EMD, we need immediate interventions to support the use of current resource and improve the resilience of the system for the future. We designed a model to address this challenge and place sociolinguistic work at the centre of interventions. We hope future studies will continue and add to this portfolio of work.
Footnotes
Appendix: Transcription conventions
= latching
[ ] overlapping talk
(.) very short pause
(1.5) longer pause in number of seconds
? rising intonation
, slightly rising intonation
. falling intonation
_ flat intonation
> < faster than surrounding speech
- truncated speech
: lengthened speech
° ° softer than surrounding speech
WORD spoken loudly
(word) uncertain transcription
((word)) transcriber’s comments
Acknowledgements
We thank all the health professionals who participated in our research and generously shared their daily experience, insight and professional practice. We also acknowledge the contribution of the two reviewers for the most constructive feedback.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The materials presented were collected for the project 999 R.E.S.P.O.N.D. funded by Health and Care Research Wales (RfPPB-21-1847(P)).