
Abstract
This article explores the introduction of the 1930 Mental Treatment Act (MTA) and places it within a longer-term trajectory of the development of acute services. While many historians have considered the apparent novelty of the MTA, they have tended to see the development of outpatients clinics as separate from the ongoing demand on in-patient services. Using patient case files from the West Riding Mental Hospital, in the northern English county of Yorkshire, consideration is given to the links and overlaps between the creation of the new legalistic categories of temporary and voluntary inpatients and the development of outpatients clinics over the longer-term. Using quantitative and qualitative evidence it demonstrates the continuities in terms of the provision of services and the financial limitations that impacted on their delivery. While attention is paid to the medical story, including the place of female psychiatrists and social workers in the delivery of services, this article emphasises the role of patients, families and non-specialist practitioners in their successes and failures.
Introduction
The 50-year period between 1890 and 1940 saw local and national changes in the legal and practical administration of mental health and learning disability provision. Following the 1890 Lunacy Act, the twentieth century brought more revisions to both Poor Law and mental health legislation, and the advent of new treatments and services. Included in this were the 1913 and 1927 Mental Deficiency Acts, which aimed to separate the learning disabled from the mentally ill, and the 1930 Mental Treatment Act (MTA), which held the promise of reduced overcrowding in mental hospitals, facilitating earlier and easier access to mental health provision (Long, 2014). This all reflected wider, longer-term aspirations to move those who were seen to be chronically ill and incurable away from those whose symptoms and prognosis suggested that they were indeed curable and worthy of medical intervention, and of the funds needed to provide them. As part of that process, the MTA created new ‘voluntary’ or ‘temporary’ gateways into mental hospitals for patients, which allowed individuals and/or their families to circumvent the existing but protracted processes of certification (TNA, FD 1/1398, 1930). For the first time, non-fee-paying patients were theoretically able to admit and discharge themselves from mental hospitals (Pearce, 2006) and Unsworth (1993: 486) described the 1930 act as a ‘harbinger of the post-carceral era,’ and step towards ‘therapeutic liberalism’ (Unsworth, 1987: 132). Contemporaneously, the Local Government Act of 1929 transferred many duties of the old Board of Guardians to the local councils, officially ending the terminology of pauperism. For medical professionals these reforms were long overdue (Anonymous, 1932; Morris-Jones, 1930) and it was hoped that they, along with a re-branding of asylums as mental hospitals, and pauper lunatics as rate-aided patients, would encourage individuals to seek assistance at a more curable stage of their illness (Busfield, 2004, 2006). Within the period too, was a continuing development of outpatients clinics which contributed to a blurring of the boundaries between institutional and community care (Bartlett and Wright, 1999; Mooney and Reinarz, 2009).
Within this story of ‘progress’, there have been attempts to shine a light on some of the darker sides of these changes. This has included the under-investment in the care of chronic and long-stay patients as attempts were made to somehow curb the influx of those seen to be silting up the asylum beds and wards (Cox et al., 2013; Long, 2014). There was also a recognition that the introduction of the MTA corresponded with a time when new and distinctly unpleasant treatments were being imposed on vulnerable people (Busfield, 2006; Dickinson, 2015; McCrae, 2006; Pearce, 2006). Baur (2013: 177) has revealed that ‘many patients and relatives welcomed some of these new treatments, as they often provided the only glimpse of hope for a cure’ but, in the main, the focus of these assessments has, nevertheless tended to be on inpatient treatment. What is often missing is any sense of what happened in outpatients clinics and it is only by exploring their ways of working can we hope to understand their impact (Westwood, 2001). This, however, can be a frustrating process and Hugh Freeman (2005: 121), confessed that his ‘examination of government records from the 1930s about these new outpatients clinics [had] not revealed very much as to what went on in them’. Cherry’s (2003: 183) analysis of Norfolk and Norwich’s outpatients department reveals little insight into what actually happened within the clinic or how successful their treatments were. Likewise, whilst providing a detailed overview of the origins of the 1930 legislation and the move towards voluntarism, Unsworth’s work does not identify how the legislation affected the realities of patients’ lived experiences.
To address this lacuna, this article considers the development of outpatients provisions before and after the introduction of the MTA. It utilises privileged access to the records of the mental hospitals and outpatients clinics of the West Riding of Yorkshire, England. This includes the West Riding Mental Hospital at Wakefield, which was known formerly as the West Riding Pauper Lunatic Asylum, and more recently as the Stanley Royd Mental Hospital. Whatever its name, its history means it holds an important place in our understandings of treatments and care. It had an international reputation in medical circles for its apparently innovative attempts to address the rising numbers of insane patients. That status is underlined by UNESCO recognition for the significance of its archive (Anonymous, 2014).
With special dispensation to explore case records from the 1920s, 1930s and 1940, the chronology chosen for this article unlocks previously inaccessible sources that enable us to move our gaze out of mental institutions and into the communities they served to more fully understand treatment regimes in this period. This is important, not least because most studies of this period are reliant on official legal and administrative records, and the reflections of staff taken from the pages of professional journals (Cherry, 2003; Freeman, 2005). This is, no doubt, driven by a time limited closure on medical records but it draws the attention away from the role of patients and their families in the development of services.
The first section presents an overview of existing attempts to provide outpatients facilities from the late 1880s onwards. Whereas studies of developing treatment paradigms have understandably focussed on the role of the National Council for Mental Hygiene and the Board of Control (Hilton, 2025) and recognised the role of charitable organisations in the development of community services (Long, 2014), it considers earlier examples of outpatients clinics and shows how they worked in practice. This will include perceptions of stigma in relation to the patient population and the responses to it, but also the place of local taxes (the rates) in that development. The second section considers the role of these existing services after the introduction of the MTA. By this time there was a web of interconnected spaces and services for people described as mentally ill, and it builds on research that has analysed the often complex and multi-faceted roles played by patients and their families in their acceptance of and resistance to treatments (Baur, 2013). Crucially, however, while there is a recognition that the MTA did little to stem the flow of inpatients, there has been no understanding of the role of outpatients clinics in that story (Busfield, 2006: 16). This section addresses that gap, and shows how they contributed to increased numbers. In the final section, the connections between inpatients and outpatients are emphasised with the exploration of the claims being made about the modernisation of services. Central to this will be case studies of Edith Wrigley, a social worker, and Dr Harriette Wilson who worked across inpatient and outpatient services in the cities of Wakefield and Leeds and, in some cases, became the face of them. These examples build on important works which have uncovered the role of women in similar positions of authority in front line services (Broad, 2021; Dale and Mills, 2007; Long, 2011, Westwood, 2006). Drawing these themes together, we contribute to the longer-term understanding of people being treated in community settings from the end of the nineteenth century, up to and including the Second World War. In doing so, we demonstrate, quantitatively and qualitatively, the place of outpatients clinics in that process both before and after the passing of the MTA. Moreover, in our exploration of patient records we show why neither the MTA nor the development of outpatients clinics in this period did little to stem the flow of inpatient numbers. Instead, we emphasise the place of those outside of the mental health system – the patients, their families, and other practitioners – in that process.
West Riding outpatients clinics in context
In its Annual Report published in 1930, the overseeing body for lunacy and mental deficiency, the Board of Control, described the new MTA as ‘a great landmark in the history of legislation’ (WYAS, C85/1/15/13, 1929) and it is easy to see why. Influenced by both the mental hygiene movement and the impacts of the First World War, it marked an apparently new era in patient agency, ‘enshrining the right of all adults to seek outpatient and inpatient mental healthcare’ (Hilton, 2025). Central too, however, were the longer-term medical, administrative and financial concerns relating to the proliferation and growth of lunatic asylums. Scull (1979, 1993) famously described the overcrowded and stultifying wards of fin de siècle asylums as ‘museums of madness’ and, while there have been numerous challenges to that assessment (Crammer, 1994; Jones, 1982; Mersky, 1994), there is no doubt that contemporaries continued to consider ways to address the apparently never-ending stream of in-patients, many of whom became classed as chronic cases, destined never to leave (WYAS, C85/1/6/10, 1931). Maudsley (1867), the well-known Victorian psychiatrist, spoke of the asylums that made lunacy ‘permanent’ and he, like others emphasised the importance of early treatment and ways in which that might be achieved. A second wave of asylum building that followed the introduction of the 1845 Lunacy Acts did not stem the apparently inexorable demand for services and it is within this context that the asylum authorities sought to manage the pressures on their resources in different ways (Crammer, 1992; Hare, 1983; Scull, 1984).
As some commentators were apt to point out, they had been advocating for many of the changes brought about by the MTA for decades (Hilton, 2025), and this included the development of outpatients clinics. In the late 1880s discussions and possibilities were shared in such august publications as The Times, and this helped to prompt the Bethlem Royal Hospital to move towards an outpatients department that would offer advice and treatment to persons in the early and curable stages of their insanity (Anonymous, 1888). Bethlem’s clinic opened in 1893 and other institutions in London opened clinics before 1890 (Jones et al., 2007). These initiatives can be seen as part of another, longer-term trend to differentiate between acute/curable and chronic/incurable services, with research and resources increasingly focused on the former. It was the West Riding of Yorkshire, and its asylum at Wakefield however, that earned a special mention in a 1925 Board of Control review of outpatient provision. Along with a later collaboration between Oxford’s Radcliffe Infirmary and the Littlemore Mental Hospital, the clinics demonstrated the possibilities for treating people in the community (Hilton, 2025).
Wakefield’s pre-eminence can be explained by an early adoption of the outpatients model in 1889 (WYAS, C85/4, 1889), but also its longer-term reputation, in medical circles at least, for its innovative and inspirational treatments (Ellis, 2006; Levine-Clark, 2000; Wallis, 2017). As early as 1876, James Crichton-Browne its renowned Medical Superintendent predicted the need for a new era of psychiatric treatment, arguing that ‘the medical psychologist of the future cannot be confined to his hospital wards. It must be his duty to walk abroad and anticipate disease’ (Crichton-Browne, 1876; Todd and Ashworth, 1991; Turner, 1996). It was, however, an administrative change and the passing of the 1888 Local Government Act (LGA) that was the immediate inspiration for Wakefield’s 1889 outpatients clinic. From this point on, asylums in England and Wales became the responsibility of democratically elected County Councillors for the first time (Ellis, 2020). Although there were many continuities in terms of those serving on the various Asylums Committees before and after the passing of the LGA, the injection of new personnel had led to discussions within London County Council about the provision of a small-scale hospital for the insane (WYAS, C85/1/12/5, 1890: 10–11). That scheme was ultimately unsuccessful, but it inspired the then new West Riding County Council (WRCC) to introduce an outpatients clinic, opening two days a week, specifically designed to treat those in the early stages of insanity (WYAS, C85/4, 1889).
The service at Wakefield was not free and neither was it straightforwardly an open one. Whilst patients could purchase any necessary medicines from the asylum dispensary at cost price, it was made clear at the outset that this initiative would not impact in any way on either the expenses of the institution or the West Riding’s rate-paying public. Costs had always been important but to the decision-makers on the WRCC’s Asylums Committee, who now had to face their electors every three years, it became even more so. Indeed, it was expected that the clinic would not affect the ordinary duties of staff but the logistics of how this would work in practice were not made clear. The Commissioners in Lunacy argued that the clinic would require the appointment of another medical officer if it was to be successful (WYAS, C85/1/12/5, 1890: 42) but William Bevan-Lewis, the Superintendent of the Asylum at Wakefield, claimed that his colleagues had expressed ‘no dissent at the extra duties thus devolving on them’. Meanwhile, plans were already in place to appoint a fourth medical officer along with a slight rearrangement of duties that had made this possible (WYAS, C85/1/12/5, 1890: 10–12).
Access to the clinic was dependent on a recommendation from one of those normally involved in the completion of the then usual reception order. This meant a prescribed form from a doctor, a Justice of the Peace, a Chairman of the Board of Poor Law Guardians, or a member of the Asylums Committee (WYAS, C85/1/12/5, 1890: 5–6). Many patients using this pre-MTA outpatient clinic were reported as having ‘slight,’ ‘incipient’ or ‘acute’ forms of melancholia, neurasthenia, insomnia and transient depression, enfeebled health, epilepsy and even alcoholism (WYAS, C85/838: 1890–1895). At the LCC Asylum at Bexley, the new acute hospital was offering what were then described as cutting-edge treatments, including the ‘application of electricity’ for its inpatients in 1907, but the West Riding authorities were proudly reporting their use in the new clinic (Commissioners in Lunacy, 1907).
Within its first year, the West Riding Asylum clinic had received 49 applications for treatment (WYAS, C85/1/12/9, 1890: 3). In the years that followed the numbers were to fall and in 1892, for example, the number of people attending the clinic was 24 (WYAS, C85/1/12/9, 1892: 3). With its proximity to the city of Wakefield, and its accessibility for those travelling by train, the clinic was apparently accessible to the local population (Hilton, 2025) but it and the asylum where it was based served the whole of the West Riding of Yorkshire, the largest county in England at the time. On their discharge, all inpatients were informed of the opportunity to use the clinic in the event of a relapse but, as one patient asked rhetorically, ‘I should be glad to do it, but how is a poor man to get here?’ (WYAS, C85/1/13/5, 1890). This helps to explain the relatively low numbers and the majority of outpatients came from areas in and around the city, as well as those who travelled from the city of Leeds, approximately nine miles away or more, depending on where they lived in the city and its suburbs. For all former patients, there were other factors to consider too, including the availability of transport from remote districts, the time needed away from work or other responsibilities, and the costs of any medicines.
Significantly, the figures above illustrate that the stigma of the mental hospital was not necessarily the main issue for patients. Instead, it was the distance to and accessibility of the institution. For many patients this was linked to an ‘inability to attend on account of leaving their daily work’ (Bullen, 1893: 491) and figures for the Maudsley, the well-known hospital in London, revealed that the vast majority of its 2000 patients in 1932 lived within a two-mile radius. Therefore, whilst the key benefit of outpatient treatment was that, theoretically, a patient could receive medication and support whilst still in employment, balancing attendance at the clinic with work and home life could be difficult for those who lived further afield.
To try and address this, a decision was taken in the following year to open similar clinics at the other West Riding Asylums at Menston near Leeds and at Wadsley, near Sheffield (WYAS, C85/1/12/9, 1890: 4). In the short-term, the numbers attending these additional clinics was also small but this was to change (WYAS, C85/1/13/5, 1888–1894, 18 December 1890). Even before the introduction of the MTA, the clinic at Wadsley Mental Hospital, had received ‘over 1,000 attendances’ in 1929 and, as Figure 1 shows, the numbers at Wakefield were also to rise (WYAS, C85/1/15/13, 1929: 277). Indeed, while there was fluctuation both before and after 1930, the peak for the Wakefield clinic came in 1910 with 105 patients attending, well before the introduction of the MTA.
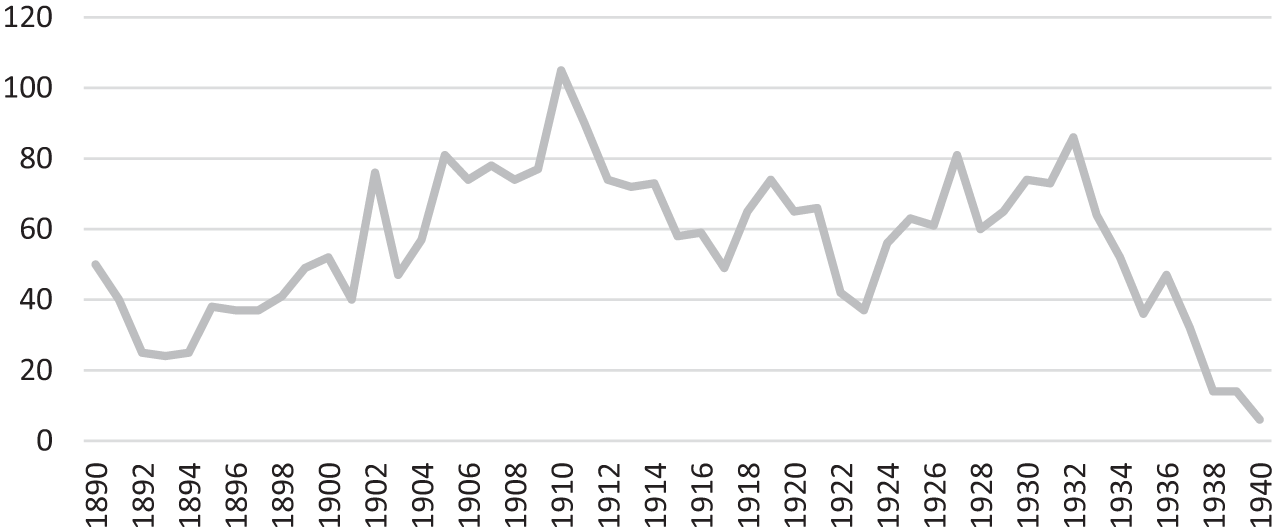
Outpatient attendances at the West Riding Pauper Lunatic Asylum/West Riding Mental Hospital, Wakefield, 1890–1940.
The MTA and the extension of outpatients clinics in practice
The outpatients clinics which were pioneered after 1930 were similar to these early clinics, but there was a general belief that many patients would be more easily persuaded to seek help and advice at the more ‘neutral’ location of their local general hospital (Anonymous, 1930). The consensus at a conference in London, convened by the Local Government Board, was that the general hospital was the right place for clinics (WYAS, C85/1/15/13, 1929). This was not a straightforward turning point, because some outpatients clinics were already in place in such places, if on a relatively small scale. This included ones in the general hospitals of London (Jones et al, 2007) and Oxford (Hilton, 2025), and in the West Riding at the Royal Hospital and the Royal Infirmary in Sheffield, both of which had been in operation since 1920 (WYAS, C416/1/65, 1920: 64). The mental hospital clinics, like those ones described above, had offered a glimpse of their wider potential but so too had the First World War, which acted as an important catalyst with the development of city centre clinics offering models for care that were separate from existing institutions (Jones, 1993: 127).
At the mental hospital in Wakefield, the Medical Superintendent, Dr Joseph Shaw-Bolton, sought to address issues around accessibility and worked with a local hospital to find space for outpatient consultations. This clinic, nearer to the city centre than the mental hospital site, would eventually open at the Clayton General Hospital, named after its most important benefactor in January 1933 (Marland, 1987: 112–113; WYAS, C235/1/48, 1930–1934: 28 and WYAS, C85/1/13/8: 17 November 1932). Later that year, the clinics at both the mental hospital in Wakefield and at Clayton were described as being well attended and were joined by the opening of another at Leeds General Infirmary (LGI; WYAS, C85/1/13/8: 16 November 1933). In 1934, Cyril Thomas, Shaw-Bolton’s permanent successor, commented on the increasing numbers and importance of outpatients clinics and saw their further growth as being ‘inevitable’. On 1 August 1935, the Tonbridge Clinic opened in Leeds, which was named after a house and the street where it was based. A few years later, Thomas pushed for other clinics in the densely populated areas of Dewsbury and Doncaster, which were to open in July 1936 (WYAS, C85/1/13/9: 19 July 1934., no day, February 1936). It was not just the sites of the clinic that were important but also their hours of operation, which reflected a working week that often included Saturday mornings. The one at Leeds Infirmary was staffed by two staff from the mental hospital at Wakefield who were available on a Saturday afternoon (Anonymous, 1935).
Pickstone (1992: 188) refers to this movement as being part of ‘a general drift of inter-war policy for psychiatry, which urged more integration with general medical facilities.’ Importantly however, the clinic at Wakefield Mental Hospital continued to operate during these years and the newer clinics in general hospitals were established to complement, rather than to replace them. The data available for these general hospital outpatients clinics is patchy, but some broad conclusions can be drawn. The figures for the Asylum/Mental Hospital clinic in Wakefield show that the majority of people who attended were women — 91 compared to 63 men in 1924 and 110 women compared to 80 men in 1931. More generally, Table 1 gives some indication of the numbers attending them in 1935 and 1936. The relatively low figures for the clinics in Dewsbury and Doncaster can be explained by their novelty, but the data emphasises the fact that many patients were repeat visitors. A simple division of the available data of patients and attendances in Table 1 indicates that the average number of attendances per patient at the Clayton clinic was 4.6 in 1935, whereas at Dewsbury it was 7.1. Despite what might appear to be relatively low numbers, the relationship between clinics and patients could be a long-term one. Martha P. who attended the Asylum clinic at Wakefield in its first year of operation in 1890, aged 23, for example, was only ‘discharged’ when she died in 1916.
Outpatient consultations in West Yorkshire, 1936.
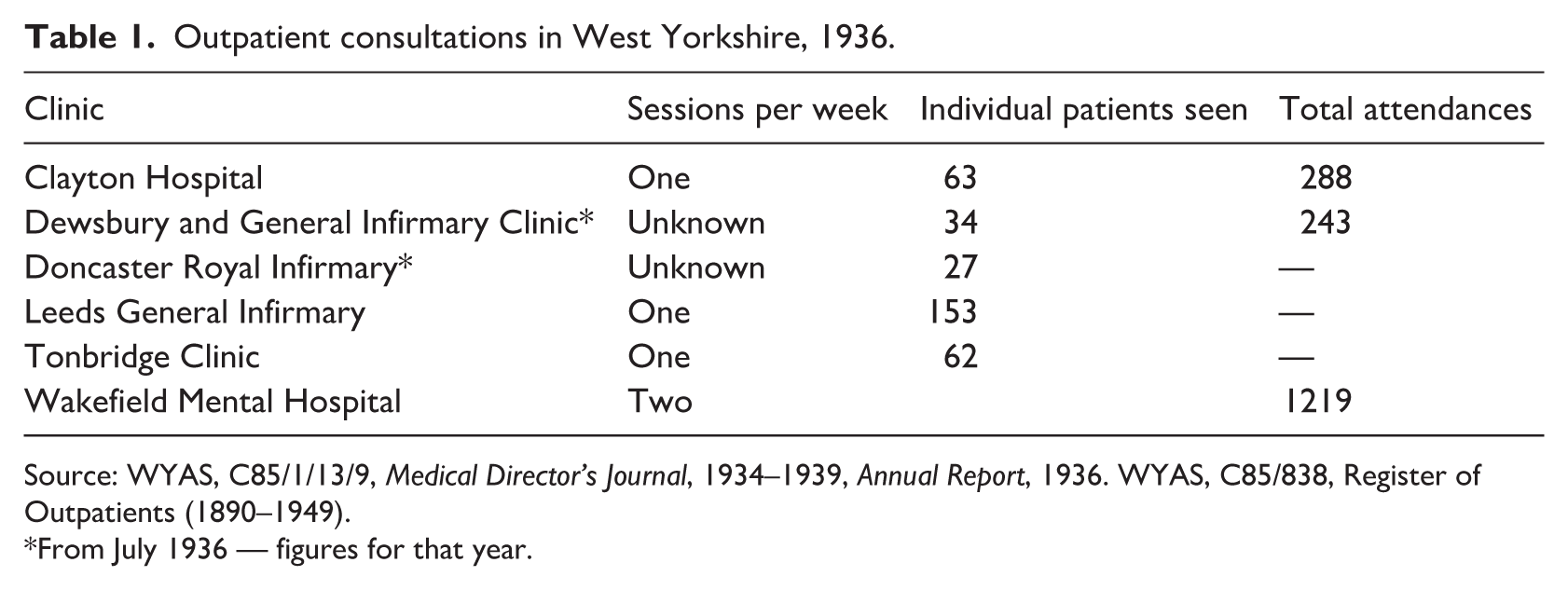
Source: WYAS, C85/1/13/9, Medical Director’s Journal, 1934–1939, Annual Report, 1936. WYAS, C85/838, Register of Outpatients (1890–1949).
From July 1936 — figures for that year.
As Table 1 also shows, the more-established clinic at the mental hospital was still receiving the majority of attendances in 1936. It was only after 1933 (Figure 2), when both the number of attendances (1659) and the number of outpatients on the register (220) had peaked, that the numbers began to fall. Whilst new patients continued to attend the clinic, and despite a temporary increase after 1934, the overall trend was downwards. It may be that this was linked to the availability of clinics in other, more accessible parts of the county but the privations brought about by the Second World War and the loss of staff to the war effort offer more immediate explanations.
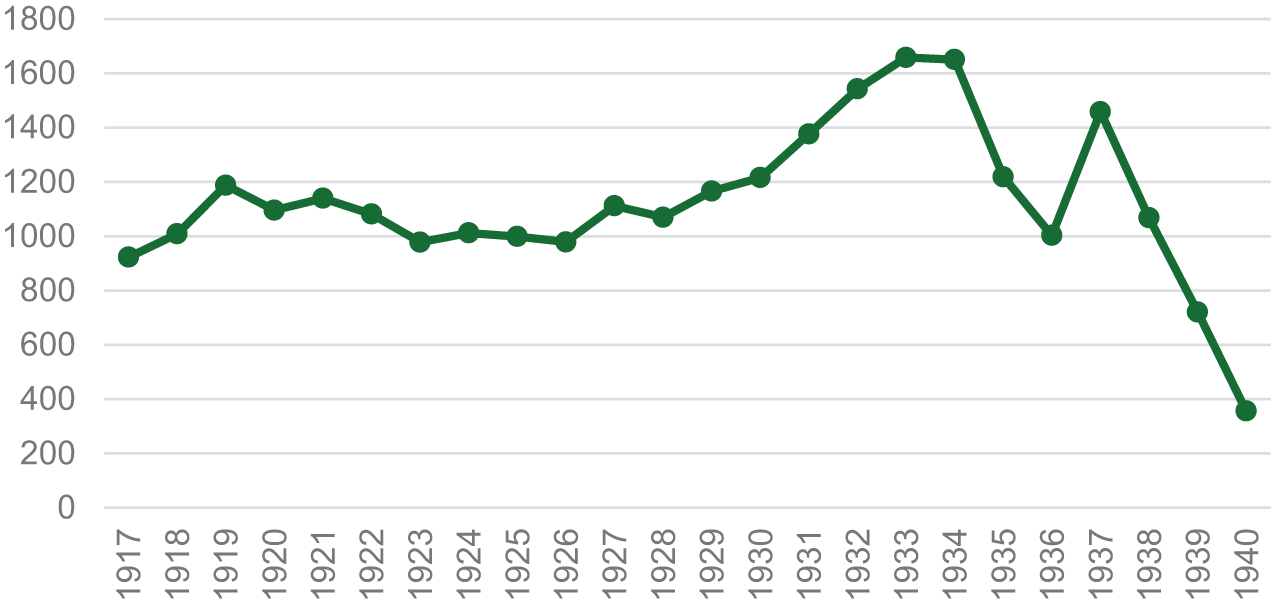
Outpatient consultations at West Riding Asylum, later West Riding Mental Hospital.
Outpatients clinics in practice in the 1930s
The ‘Mental Welfare Centre’ opened at Tonbridge Street in Leeds in August 1935 (Anonymous, 1935). Funded by the WRCC, via the West Riding Mental Hospital’s Visiting Committee, and staffed by a full-time, nurse-trained welfare worker, the building included a waiting room, a social worker’s office and a doctor’s consulting room. The working arrangements were modelled on what was happening at the clinic at Leeds Infirmary, which was staffed by two of Wakefield’s medical staff. The case notes for both are sadly missing but the overlaps between all of the West Riding’s clinics allow insights into their operation and relatively detailed case notes of patients survive for both the clinic at West Riding Mental Hospital and Clayton General Hospital after 1930. These case notes provide insight into the workings of the clinics and the patients who attended them.
The case notes for both clinics were organised fairly simply, but the records at Clayton were more fully completed. Key headings at the top of the patient records were: Name, Address, Age, Marital Status, Occupation, the date of first attendance, and the name of the physician referring the patient. Occasionally, letters of referral from individual doctors were appended to the files, but these only included a line or two on the reason behind the referral. Unlike asylum reception orders, details of ‘family history’, ‘personal history’ and ‘history of the present illness’ came primarily from a dialogue with the patient, which could be supplemented by family members if they were in attendance (WYAS, C85/840, Box A–G). In the 1940s at least, patients at Clayton were given a small business-style card with the words ‘Psychiatric Clinic’ on it which included a space for their name and their clinic number (WYAS, C85/840, Box N–Z: 739). This ensured that the appropriate case notes could be annotated and updated on each visit. Patients were instructed to attend clinics on Wednesdays at 3.00pm and to take the card with them on each visit.
Records reveal that, although local or family doctors were aware of the clinic, they were not necessarily aware of the people who were running it, with referral letters addressed to the ‘Dr’, ‘the Psychiatrist at Clayton Hospital’ and even the ‘Dr on duty at the Psychiatric Clinic’ (WYAS, C85/840, Box A–G: 52; 116; 589). Letters attached to individual case notes, indicate that the majority of patients arrived at the clinic at Clayton via this method of referral. In return, updates on the progress of patients from the clinic back to those doctors reveal evidence of a dialogue and negotiation between the specialists and General Practitioners. In addition, referrals came via the Probation Service, the Public Health Department and from various Education Committees (WYAS, C85/840, Box A–G: 406; 411; 484. See also WYAS, C85/3/6/301, 1935). On occasion, patients could bypass these various gatekeepers altogether and there is evidence to suggest that patients attended on their own volition. George B., for example, had written to the hospital in the first instance and had been advised to attend the clinic on Thursdays for a consultation (WYAS, C85/839: 37). A letter to Thelma B. included options for her to attend clinics at Clayton General Hospital, Leeds General Infirmary, or the West Riding Mental Hospital at Wakefield and included details of the bus routes from her hometown (WYAS, C85/840, Box 1 A–G, 623). With the varied routes to the clinics, it is not surprising that patients and doctors used them very differently in each case. Table 2 reveals that every clinic ushered some individuals into inpatient mental hospital care, with the majority referred from Clayton, the LGI and the West Riding Mental Hospital. Significantly, 109 individuals made their way to the inpatient wards, invariably impacting on the already overcrowded institutions.
Outpatients to inpatients in West Yorkshire, 1936.
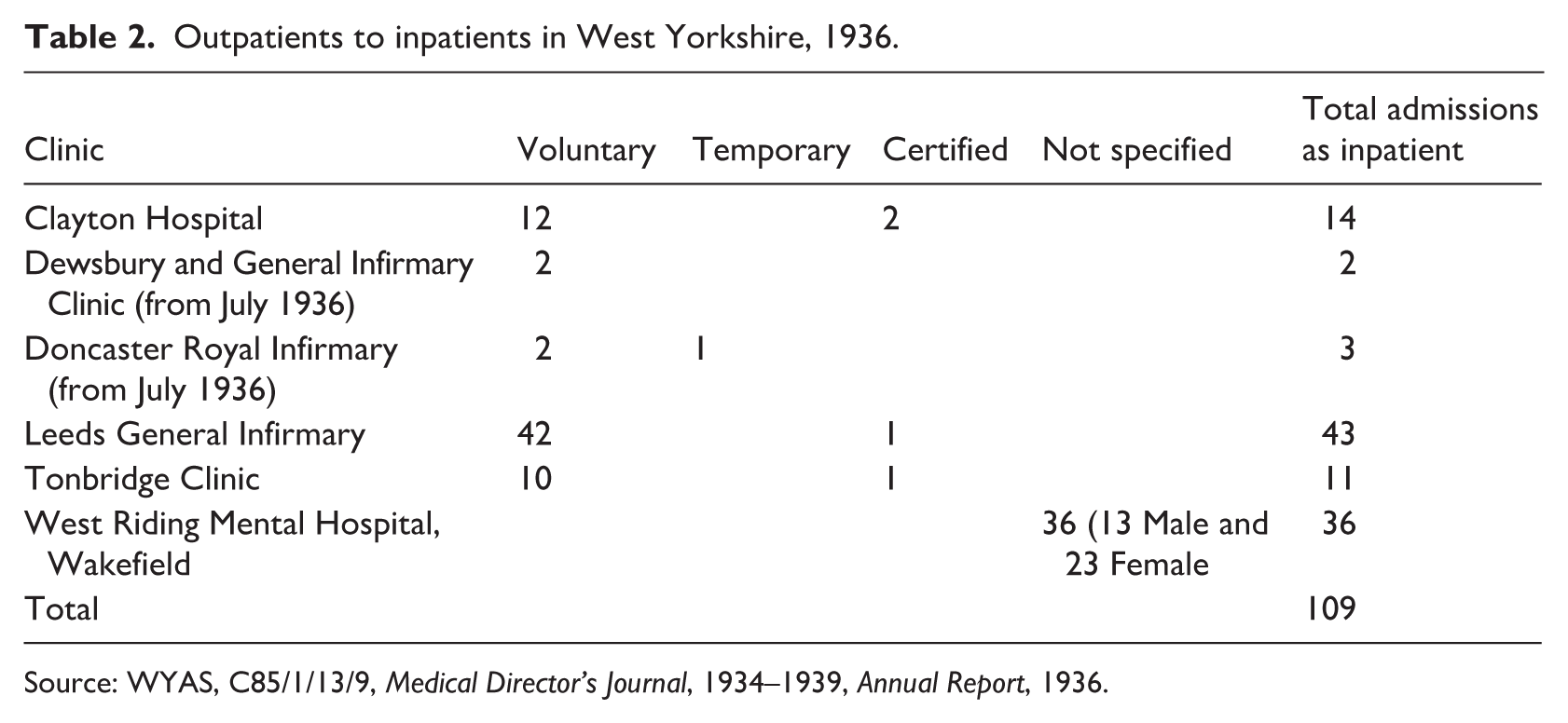
Source: WYAS, C85/1/13/9, Medical Director’s Journal, 1934–1939, Annual Report, 1936.
With the Mental Treatment Act came new categories and terminologies of patients that sought to circumvent the existing legal and administrative processes of reception into asylums. ‘Voluntary’ and ‘temporary’ patients were to rise steadily throughout the 1930s. 1 Within these national figures there was an uneven spread with Voluntary and Temporary admissions ranging from 5% to 22% across different mental hospitals in 1931 (WYAS, C85/1/15/15, 1931: 28). This uneven picture was to continue throughout the decade. At Wakefield Mental Hospital, the trend was upward and by November 1931, Voluntary and Temporary cases were making up one quarter of all admissions and early in the following year that had risen to one third (WYAS, C85/1/13/8: 19 November 1931; 18 February 1932). By 1936, temporary and voluntary admissions made up 52% of all cases (WYAS, C85/1/13/9: March 1936). These figures are much higher than other institutions (Pearce, 2006: 118) but, by this time, Dr Fernadez, West Riding County Councillor and Chairman of Wakefield Mental Hospital’s Visiting Committee was stating that another institution needed to be built (Anonymous, 1935). The evidence here shows that the new clinics did little to arrest that demand and even added to it.
Indeed, if the aim of the MTA had been to treat patients at the earliest stages of their illness (Morris-Jones, 1930), the figures and the patient files show that the outpatients clinic often acted as a gateway to the institution for those who had been managing their condition at home for some time (WYAS, C85/1/15/13, 1929: 2). This was the case for 42-year-old Mrs E. who had attended Wakefield Outpatients Clinic regularly, before being advised to undergo inpatient treatment in 1942 (WYAS, C85/839: 43). Her case notes reveal that she had been ‘avoiding’ treatment for the past three months, and at her next appearance at the clinic, she was advised to apply for treatment at the Mental Hospital as a voluntary patient. It was noted in the records that she and her husband accepted this advice, and she was received as an inpatient the next day.
In the case of Arthur A. attending the outpatients clinic at Clayton General Hospital appeared to be just a step towards institutional care (WYAS, C85/840, Box 1, A–G: 166). For his GP, the referral appears to have been a formality, rather than there having been any real expectation of outpatient treatment. Arthur had been a patient at the West Riding Asylum in the years 1905–1918 and had been in and out of the institution throughout the 1930s. In 1936 he was advised by his doctor to attend the clinic at Clayton, whereupon the medical attendant once again advised inpatient voluntary treatment, to which Arthur agreed. In this particular case, and many more besides, the clinic, just like the clinic at the mental hospital, acted as a stepping stone to institutional treatment. It was a place for initial diagnosis, rather than a place of extra-institutional treatment and cure.
In many cases however, most patients hoped to manage their circumstances in the ‘community’. Patients would first see their general practitioner, who would refer them on to the outpatient clinic for ‘expert’ advice. This was the case for Mrs C., 45, a housewife from Doncaster, whose private doctor wrote a letter of referral to the outpatient clinic at the Mental Hospital in Wakefield in September 1942. ‘I feel it is a matter for psychological treatment’ he wrote, ‘and I will be much obliged if you could take the case in hand’ (WYAS, C85/839: 42). After Mrs C. was seen at the clinic for the first time, she was advised to apply for and subsequently accepted treatment at Sheffield Mental Hospital as a voluntary patient. Her removal to Sheffield was linked to the proximity of her home in Doncaster, but also overcrowding at Wakefield Mental Hospital.
At other times it seems clear that a visit to the clinic was prompted by a moment of crisis and the nearest hospital with available space was suggested. For example, in 1943 the case notes reveal that Ethel B., 43, was epileptic with a young baby. Mentally she was described as being ‘in such a state of nervous exhaustion and depression that she is quite unfit to manage her home, and she promised to come up to Storthes Hall to ask for admission as a voluntary patient’ (WYAS, C85/839: 656). Similarly, for Anne H., who had already attempted suicide, the outpatients clinic was not considered a safe or suitable option and she and her husband were also advised to go to Storthes Hall Mental Hospital in Huddersfield as a voluntary patient that very day (WYAS, C85/840, Box H–M: 608).
Work on the 1930s suggests that individuals were often pressurised into treatment, problematising the notion of ‘consent’ in 1930s mental health care (Hide and Bourke, 2018) but, in these cases, we can see that institutions were also used as a form of respite (McGarry and Chodoff, 1981: 210). They emphasise the steps between care at home to institutionalisation, with outpatients clinics acting as triage centres, offering advice and often persuading patients to apply for inpatient treatment. They also demonstrate that the clinics served the county, rather than simply the cities in which they were based. Which institution patients were sent to depended upon on several factors, including the availability of bed space. Thus, whilst one of the aims of outpatients clinics was to relieve overcrowding in already full institutions and provide some relief from the unrelenting demand for asylum beds, this was not always possible in practice.
Resisting inpatient treatment
Describing the MTA, Unsworth (1987: 170) explains that patients were ‘under a social obligation to submit to the therapeutic regime prescribed by the medical expert.’ Despite this, neither patients nor their families necessarily chose to accept the advice of the doctors. The case notes at the clinic for Clayton Hospital suggest that the staff frequently had to battle with patients and families who refused to take their advice and accept recommendations for in-patient treatment. This was even after the new categories of temporary and voluntary treatment were explained to them. Whereas the site of the clinic did not appear to impact on attendance, some patients cited stigma and fear to be amongst their reasons for refusing inpatient treatment. This included two patients whose relatives had died inside a mental hospital (WYAS, C85/840, Box 2, H–M: 32; 578). When Herbert K. was pressed by outpatients staff to go to Storthes Hall as an inpatient in 1942, he simply stopped attending the clinic (WYAS, C85/840, Box 2, H–M: 32; 578). Similarly, in June 1943, John R. of Ryhill, a small village on the outskirts of Wakefield, told medical staff at the clinic that ‘he live[d] in a small place, [was] well known there and felt that it would be a stigma for him to go into a mental hospital’ (WYAS, C85/840, Box 3, N–Z: 658). This was the last entry in the case notes for John indicating that he ceased to attend the clinic after this confession. These cases illustrate some power and agency of individual patients to determine their own course of treatment (McGarry and Chodoff, 1981: 210), but patients came under lay pressure too.
In an overview of female sanitary inspectors, there has been a suggestion that the existing literature presumes that all inspectors were officious, and all clients had issues they wished to conceal (Dale and Mills, 2007: 113). An assessment of the patients coming forward for, or being pushed towards treatment, highlights the often-complex negotiations between patients, their families and doctors. Many surviving letters corroborate the work done by Baur (2013: 177) which has shown that a patient’s family was often instrumental in the decision process of admitting individuals to inpatient care, even when the individual was admitted as a voluntary patient. Edith D was unwilling to go to hospital in 1943, and only became a ‘voluntary’ inpatient after her sister was advised that there was a ‘definite danger’ that her sister might commit suicide if not. Eventually the threats made by the doctor that certification ‘might be needed in this case’ seemed to have persuaded Edith’s sister to persuade her that ‘voluntary’ care was for the best (WYAS, C85/840, Box 1, A–G: 634). However, it would appear that the family was only one element in the decision-making process and for others the journey to the clinic involved a longer-term story of advice and treatment in a bid to avoid institutionalisation (WYAS, C85/3/6/301: May–December 1935). Other cases illustrate a more complex process of negotiation which often occurred between the parties to secure institutionalisation. Often letters identify the importance of a family doctor in trying to persuade family members to encourage their kin to opt for treatment (WYAS, C85/840, Box 1, A–G: 319). In other instances, family members were left to argue amongst themselves, and family politics had a fundamental role on whether a person would accept voluntary treatment or not (WYAS, C85/840, Box 2, H–M: 555). In March 1938, the mother of Jessie W. for example was ‘unwilling’ to send her daughter to the hospital and so the matter was dropped (WYAS, C85/840, Box 3, N–Z: 337).
As was shown in the introduction, legislation in the 1920s and 30s aimed to focus resources on acute and apparently treatable conditions. This was not immediately clear to those hoping to use the new services and, in addition to those who refused inpatient treatment, doctors declared many patients to be unsuitable for outpatients care. This included those who were described as mentally deficient (WYAS, C85/840, Box 3, N–Z: 739; Box 1, A–G: 597), those diagnosed with senile degeneration (WYAS, C85/840, Box 2, H–M: 613), and those with auditory hallucinations or schizophrenia (WYAS, C85/840, Box 1, A–G: 360). In June 1943, the relatives of 24 year-old Elsie H. were criticised by medical staff on the grounds that they had ‘behaved towards her most unwisely by sentimental gushing and weakening sympathy. If she had been taken away from her family some years ago’, the medical notes record, ‘it is possible that she might have been trained to some useful job’ (WYAS, C85/840, Box 2, H–M: 648). In this case, Elsie’s family were advised that outpatient treatment was ‘useless’, but this was not automatically applied in each case. In 1939 Joe B. was also deemed to be unsuitable on the grounds that he was diagnosed as ‘incipient Schizophrenic’, with his ‘delusions and entire conduct’ deemed to be a consequence of auditory hallucinations. Joe was accompanied by his sister to the clinic, but she was anxious that he would not become a mental hospital patient. With this in mind, the doctor at the clinic agreed to see him from time to time to watch the progress of his case (WYAS, C85/840, Box 1, A–G: 360). Similarly, in 1941, Ellen D was also described as ‘unsuitable’ for outpatient care. Nevertheless, her records claim that she was ‘very unwilling to go into hospital and begged to be allowed to give outpatient treatment at least a trial.’ The staff at the clinic relented to these demands (WYAS, C85/840, Box 1, A–G: 437).
For other patients who attended the clinic, the cost of treatment continued to be a significant barrier to their successful treatment. Examples include Ben H., 36, who was noted in the register to be ‘unfit for outpatient treatment- cannot pay,’ and also the unemployed Roy H. who was also described as having ‘no means of paying for medicine’ (WYAS, C85/838, 1890–1949). Both of these patients were said to be suffering from epilepsy, and clearly the cost of treatment for this condition left these two men with little hope of receiving appropriate treatment within their respective and restricted budgets. The examples above demonstrate the variety of patients that were deemed to be unsuitable for outpatient care, but they also bring into sharp relief the objectives, and the failings, of the new clinic in terms of limiting inpatient treatment. As a result, other changes were introduced which were aimed at preventing re-admission.
‘Modernisation’ in the hospital and in the community
During his short time as Medical Director from 1934–1937, and with the support of the Visiting Committee, Cyril Thomas began to modernise the Wakefield Mental Hospital. Much of this focussed on the physical health of inpatients and a range of consulting physicians with specialisms in ear, nose and throat, gynaecology, and tuberculous diseases were appointed, as were an ophthalmic surgeon and a visiting dentist (WYAS, C85/1/13/9: Annual Report, 1936). As part of more general attempts across the sector to prevent patients from deteriorating into ‘wearisome idleness’ (Jones, 1993: 134), classes for physical exercise were also regularly held in this period (WYAS, C85/1/13/9: Medical Superintendent’s Report for 1935). Other changes included the conversion of the laundry as an occupation centre on the male side and a ‘party of patients were constantly at work in doing furniture repairs etc.’ (WYAS, C85/1/13/9: February 1935). Working patients at asylums and mental hospitals were hardly new, but this was now branded as ‘occupational therapy’ (see below) and with a growing theoretical corpus to underpin its positive impact on the patients and for ‘the previously unoccupied to commence useful habits’ (WYAS, C85/1/13/9: November 1934).
These changes have to be contrasted with the ongoing and familiar refrains relating to overcrowding. At the same time as recording the first voluntary patients in January 1931, Shaw-Bolton drew the attention to the inexorable rise of inpatients. ‘In the previous nine years’, he wrote, the number had risen from 1955 to 2479 (WYAS, C85/1/13/8: 19 February 1931) and within a short space of time it had increased to 2652. These changes had a deleterious effect on patients with some forced to sleep on the floor in overcrowded wards and a more widespread use of sedative drugs (WYAS, C85/1/13/9: October 1936, December 1936).
In another bid to arrest the numbers, plans were put in place to reduce the incidences of re-admittance. This included, from 1936, a new parole ward which, again, mirrored changes across the sector and operated as a staging post to discharge (Jones, 1993: 150; WYAS, C85/1/13/9: 1936). As with other initiatives, it is hard to see just how new this was with a similar ‘halfway house’ located in a former farmhouse on the then asylum estate in the 1870s (WYAS, C85/109: Report of the Superintendent for 1873). More important were the spaces for former patients within the outpatients clinics. The short-lived clinic at Tonbridge House included activities for former patients on two days per week. These were clearly gendered and centred on a sewing guild but, in addition to ‘a pleasant social afternoon’, former patients also had access to both a doctor and a social worker (WYAS, C85/1/13/9, December 1935, July 1936).
This period also saw the development of Psychiatric Social Work, with the London School of Economics offering the first training course in the UK from 1929 (Burt, 2008: 758). Writing at a time in which electric shock and drug treatments appeared to offer miracle cures, the well-known psychiatrist William Sargant later described psychiatric social workers in pejorative terms. At the Maudsley Hospital ‘tactful women interrogators’, he opined, compiled case histories that were often ‘a waste of time’ and ‘would now be laughed at’ (Long, 2011: 225). By contrast, in her study of the post-war period, Vicky Long has described the failures of the physical therapies that Sargant and others placed so much faith in, and the role of psychiatric social workers in ameliorating the lives of those discharged. The latter, she concludes, vacillated between their pessimistic and disciplinary attitudes and their inventive attempts to alleviate their ongoing social and familial problems (Long, 2011: 238–239).
How social workers operated in practice depended on a huge range of factors that included the resources available, the geographical areas of work and significantly, the support or otherwise of the lead psychiatrist (Timms, 1964). At the Wakefield Mental Hospital, a social worker, Miss Edith Wrigley, was appointed in the summer of 1935 and her role was to visit both patients and relatives at home with a view to helping patients back into their communities (WYAS, C85/1/13/9: June 1935). Thomas wondered if a social worker going into the homes of former patients might be seen as an intruder into their privacy, but he could not think of one example where her work was met with a rebuff (WYAS, C85/1/13/9: June 1935). The records for this work are missing, but Thomas described one ‘outstanding example’ of a young friendless woman who had recovered after a long period as an inpatient. A domestic position was found for her and the visits by the social worker helped her settle in (WYAS, C85/1/13/9: October 1935). Rather than a supplement or a contrast to invasive therapies of medical staff, such activities in this period mirrored the consultative work that was going on in the outpatients clinics.
For women, in particular, correspondence with the clinics offers some limited insight into their home lives – especially those who had a longer-term relationship with the staff there. Caroline A. asked to be excused because her husband, who accompanied her, was on short time at work (WYAS, C85/839: 6) and Elizabeth W. asked if her daughter would be allowed to pick up her tablets as she ‘had a miscarriage last Thursday [and was] still ill in bed’ (WYAS, C85/840: 24). Not everyone was prescribed medication, however, and of those who did attend Anne D. was encouraged to widen her contacts and take up an outside interest, leaving the clinic with a dose of Vitamin B1 and Glucose (WYAS, C85/840: 737). For Sarah L. a ‘change of air’ was recommended, and she was discharged on the same day (WYAS, C85/838: 1934). In these cases, the doctor involved was Harriette Wilson, who worked at the mental hospital at Wakefield and whose practice straddled inpatient and outpatient responsibilities.
Like Wrigley, Wilson worked to uncover the social causes of mental ill-health or individual crises. This was a period in which psychoanalysis was also on the rise and there are possible links to what Wilson was trying to achieve. As part of the modernisation process at the mental hospital she had introduced activities for women such as country dancing and painting, often involving willing volunteers from the community (Hilton, 2025). Similarly, a Medico-Psychological Clinic in Brunswick Square, London included ‘occupation therapy’, including arts and dancing, along with the psychotherapeutics on offer (Raitt, 2004). Those practising the tenets of different psychotherapies were limited to ‘a handful of dedicated individuals’, both internationally and in Great Britain (Alexander, 1998) and there is no evidence in the files consulted to suggest that Wilson was engaging with some of the other treatments on offer, such as hypnosis. There were, however, examples of ‘therapeutic conversation and persuasion’. This included recognition of what could be the stifling nature of gendered roles and, when Ethel C., a 42-year-old, single woman attended the clinic in 1943 she was ‘urged. . ..to seriously consider how to broaden her activities and develop new interests’ (WYAS, C85/840, Box 1, A–G: 681). Within this recommendation there was no discussion of class, or the opportunities arising from it, but Wilson was of ‘the opinion that her anxiety symptoms and phobias [were] developing as a result of a dull stereotyped life without adequate variety of mental interest and stimulus’ (WYAS, C85/840, Box 1, A–G: 681).
In the examples above there are no clues as to how or whether such advice was heeded, but in other cases Wilson involved herself in the practicalities of women’s lives. Winifred A., who attended the clinic in January 1944, for example, was described as having ‘an overemphasis of the fear instinct’, which may have been linked to the fact she was a premature baby (WYAS, C85/840, Box 1, A–G: 734). The immediate reason for attending the clinic were her concerns at walking to work alone in the dark. In an appeal for funds, the clinic in London explained that, typically, its patients had symptoms that included, a secret mental worry, an apparently unfounded anxiety or depression, inability to take interest in the ordinary affairs of life, a morbid fear which is recognised to be absurd, a secret habit which is struggled against, an unnatural impulse which cannot be controlled; and declared that such complaints in most cases can only be satisfactorily cured by psychotherapy (Raitt, 2004: 69).
Wilson, however, was more practical, writing to Winifred’s doctor asking him to contact her employers and to request a day shift. A note of the file records that her employers acquiesced, and Winifred’s case notes were closed. Similarly, Alice H., whose husband was away with the forces, was noted to be struggling with four children, the eldest of which was only eight years old. Wilson wrote to the relevant authorities to request a house on a council estate near to her mother who could then help with childcare. The final note in Alice’s records note that she ‘has got house near mother – much better’ (WYAS, C85/840, Box 2, H–M: 332).
In other cases, it is clear that not all social problems could be resolved quite so easily. Olive A. a 29-year-old single woman first attended the clinic in September 1942 after her doctor (Dr Lawrence) referred her with a note to say she would ‘give you her side of the story’ (WYAS, C85/840: Case No. 563). Wilson wrote to Lawrence to explain that Olive was in a state of depression which was ‘largely due’ to the changes in her work. Wilson promised to keep seeing Olive on the understanding that she might have to consider a change of employment. Lawrence wrote back immediately, wondering if ‘this woman was quite frank with you?’. Olive had ‘fallen for a married man who works in the same department and had recently been paying her attention’, but Wilson was already aware of this (WYAS, C85/840: Case No. 563). Shortly afterwards, Olive resigned to join the forces and the case notes ended.
Whilst the clinic saw considerably more female than male patients, especially during the war, it could also offer similar advice to male patients. Jack R., a pit worker started attending the clinic in 1943 after a series of fainting attacks. His records note, ‘There is a possibility that he may be suffering from emotional stress in his efforts to decide upon the right course in the face of family and country’ (WYAS, C85/840, Box 3, N–Z: 633). The doctors suggested that outdoor life and physical training in the forces would be beneficial to this patient and the notes record that ‘he himself seemed relieved at the suggestion of leaving civilian work to go into the army’ (WYAS, C85/840, Box 3, N–Z: 633). Leonard P. was also judged by doctors at the clinic; his case notes read, ‘He was not very co-operative as his sole idea in coming to the clinic appeared to be getting freedom from his present job rather than a wish to cure his condition’ (WYAS, C85/840, Box 3, N–Z: 698).
Conclusions
By placing patients at the heart of this analysis, this article has shone a light on the development of outpatients clinics both before and after the introduction of the Mental Treatment Act (MTA). Despite longer-term aspirations to reduce lunatic asylum and mental hospital numbers, those institutions loomed large throughout the period. Their sites, which were sometimes difficult to access, their funding, their hours of operation, their fees, and their staffing all help to explain their origins and their development over the longer term. Whereas there is a medical story to be told here, the immediate catalyst for change in the West Riding of Yorkshire, as well as London was the passing of the Local Government Act in 1888. Despite this legislative change, new money was not forthcoming and the continued use of clinics on asylum sites suggests that the will to address the stigma of mental illness was, perhaps, less important to the general public than the medical profession may have presumed, at least for former inpatients. Either way, initial attempts did little to reduce the demands on already overstretched services. The newer categories of ‘voluntary’ and ‘temporary’ patients ushered in by the MTA, only added to that demand. Rather than a way of keeping people out of institutions, the clinics operated as a triage service which included the prospect of inpatient stays for some people. The reasons behind this were complex but, crucially, not everyone attending the clinic did so in the early or incipient stages of their illness. Instead, for patients, their families and non-specialist practitioners, clinics became the first port of call for a whole host of other reasons, including those where the mental hospital might be presumed to be the default treatment option under other circumstances. Faced with this multiplicity of experiences, clinic staff had little choice than to recommend inpatient treatment. The patients themselves, as well as their families could play a part in that process by refusing inpatient treatment or simply by ceasing to attend outpatients appointments. Nevertheless, alongside changes in legislation and categorisation, came newer ways of working that included more therapeutic understandings of people and their everyday lives. These contributed to other successful interventions and the work of Wrigley and Wilson show how apparently practical or even common-sense solutions could ameliorate the challenges that some people faced. These solutions, however, remained dependent on a range of social and cultural context and, for all that, the wider picture of mental health remained unchanged. Funding for new services and new initiatives was finite and those institutionalised and deemed to be incurable continued to be left behind by a lack of investment and neither the MTA or the clinics could do anything to resolve that.
Footnotes
Acknowledgements
The authors wish to express their thanks to staff at the West Yorkshire History Centre/West Yorkshire Archive service for the help received in accessing materials for this publication. Thank you also to Len Smith and Rebecca Wynter for their comments on and support for an earlier draft of this article, and to the Journal’s anonymous peer reviewers for their helpful insights.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.