
Abstract
In 1957, the British-Indian child psychiatrist Dr Elwyn James Anthony travelled to the Zurich International Congress of Psychiatry to show a film featuring 70 children with such complex symptomatology and behaviour that they betrayed the certainty of contemporary theories of developmental psychology and psychoanalysis. This article examines the significance of Anthony’s film to the creation of new scientific models in international developmental psychology and psychiatric epidemiology. It marked a significant change in the use of filmed evidence that sought to create a truly global and universalist approach to atypical child development based purely on scientific observations. This new observational work was important in shaping new internationally ratified models to study the epidemiology of children’s psychiatric conditions.
Keywords
Introduction
This article explores the significance of film in generating new international observational methods in child mental health sciences in the 1950s. It focuses on the work of Elwyn James Anthony who presented the first objective film evidence of different behaviour associated with childhood schizophrenia. Anthony’s goal was to move the field of children’s mental health away from culturally biased theoretical assumptions based on language, and towards a universally acceptable model of diagnoses and treatment based on observable symptoms. Instead of focusing on ‘norms’ and their aberration, as in the well-known developmental films of Arnold Gesell, Anthony focused on the shared behavioural characteristics of atypical children, producing a new kind of objectivity in children’s mental health sciences. This study explains why Anthony’s work is important to the history of international, transcultural and cross-cultural psychiatry, as well as the expansion of psychiatric diagnoses that have achieved fame and notoriety in the twenty-first century via the International Classification of Diseases (ICD) and the Diagnostic and Statistical Manual of Mental Disorders (DSM) (e.g. Antić, 2022; Delille, 2018; Wu, 2021).
Contemporary work in transcultural psychiatry is encouraging new perspectives on the origins of contemporary scientific and theoretical modelling in psychiatry. As Emmanuel Delille has argued, much prior work in the history of psychiatric epidemiology has had a very present-centred focus, showing how past work eventually led to models of theoretical and epidemiological agreement in the twenty-first century (Delille, 2018). However, looking deeper into the origins of psychiatric theoretical modelling and international psychiatry demonstrates that changes in the classification and application of psychiatric diagnoses over the twentieth century has been neither self-explanatory nor predictable (e.g. Berrios, 1996; Ellenberger, 1970). This article focuses on attempts to build and promote international and universal methods in child psychiatric research through the use of film and visual evidence. Anthony encouraged a new approach to the problem of international agreement based on film evidence at the International Congress of Psychiatry in Zurich in 1957. He used this to challenge the authority of John Bowlby and other psychiatrists who had advised the World Health Organization (WHO), and he set new limits and standards for the international assessment of psychopathology in childhood. The Zurich Congress was thus an important milestone in the study of children’s psychiatric symptoms that have influenced international child psychiatric epidemiology.
Post-war optimism and child mental health
The post-war period saw radical changes in approaches to psychiatric research and treatment. This paralleled a new-found optimism to generate international consensus and agreement on child development. The post-war establishment of organisations such as the United Nations (in 1945), the United Nations Children’s Emergency Fund (UNICEF, in 1946), and the United Nations Educational, Scientific and Cultural Organization (UNESCO, in 1946) encouraged child psychiatric organisations to move towards united goals of supporting healthy child development and identifying symptoms and behaviour that may require psychiatric intervention. This is why World War II was a turning point in the development of child psychiatric approaches, and encouraged a move towards international agreements and accords. Nevertheless, there is little historical work that explores how these accords were formulated and the influence they have had on the international diagnostic systems that followed.
The late 1940s and the 1950s represent an important period in this history because colonial approaches were still dominant in many areas, yet internationalism and theoretical agreements were also increasing. This led to a mix of post-war scientific and political optimism, coupled with Western obstinacy that required correction from a growing international community. The establishment of the World Health Organization in 1948, and the central role played by Brock Chisholm in placing mental health at the core of WHO values via its Mental Health Unit, set the scene for child psychiatrists to reconsider their role and legitimacy within an expanding global psychiatric network (Delille, 2018; Pols and Wu, 2019). The publication of the UNESCO statements on race (1950), and Frantz Fanon’s (1952) and others’ criticism of psychoanalysis, put increasing pressure on the WHO to address lack of scientific validity in describing psychological development. The use of intelligence testing to deny rights to children in colonial contexts, through eugenic ideologies in general, and via Nazi race hygiene policies, placed child psychiatry and psychology under new scrutiny (Dubow, 1995; McCulloch, 1995; Scheffer, 2018; Thomson, 1998; Vaughan, 1991).
The profession of child psychiatry had been established in most industrialised countries in the early twentieth century via the expansion of compulsory schooling and government intervention into childhood via eugenic and welfare policies (Rose, 1999; Thomson, 2006). This was further encouraged by the popularity of work by Sigmund Freud, Eugene Bleuler and other specialists in adult psychopathology, who started to focus on infantile thought as the cause for later mental disturbance (Bleuler, 1911; Freud, 1905/2001a). Renowned European and North American psychiatric clinics such as La Salpêtrière in Paris, the Maudsley Hospital in London, the Burghölzli in Switzerland, and the Johns Hopkins Hospital in Baltimore served as focal points for training, and eventually enabled an independent profession of child psychiatry to grow. This profession increasingly distinguished itself from child psychology through its commitment to severe psychopathology, rather than normal development, and lack of intelligence. The development of quantitative tests for intelligence in the early twentieth century, following Alfred Binet’s and Theodore Simon’s work, solidified this distinction, enabling a division between ‘mental deficiency’ and ‘psychopathology’ in childhood to be progressively mapped out (Berrios, 2003; Evans, 2017).
Jean Piaget had an important influence in guiding theoretical, as well as the clinical treatment, of children internationally, and he drew significantly from the theories of Bleuler and Freud. Leo Kanner’s work at Johns Hopkins in Baltimore and Lauretta Bender’s work at Bellevue Hospital in New York became important in promoting particular concepts, especially childhood schizophrenia and autism, building on Bleuler and Piaget’s work. In 1925, George Heuyer established a Clinique Annexe de Neuropsychiatrie Infantile at La Salpetrière (Duché, 1990), and built international collaborations. He organised an International Congress of Child Psychiatry in Paris in 1937 with the goal of generating international consensus in child psychiatry as a discipline distinct from neurology and psychology. A second congress, planned for Germany in 1941, was delayed by the war and was later held in Britain in 1948, when the International Association for Child Psychiatry was formed (Schleimer, 2012: 7).
Heuyer’s early attempts at international collaboration in child psychiatry had featured primarily European and North American collaborators (Solomon, 2016). Yet in the post-war period, the WHO began to fund and support child psychology and psychiatry at an international level. Many agreements and accords that had been made between largely European and North American collaborators were then challenged. The growth of more representative international medical and political organisations placed new demands on international and cross-cultural diagnoses (Wu, 2021). Discussions on child diagnoses at these early international meetings were plagued with controversy over the legitimacy of approaches that had been permeated with Western eugenic and ‘race hygiene’ philosophies. This was part of a denazification of science, and a move away from eugenic and race concepts within the sciences (e.g. Bangham and de Chadarevian, 2014; Hall, 2019; Sheffer, 2018). When the WHO sought experts to guide policies on child mental health, they turned to British experts such as John Bowlby, and to Jean Piaget because his Swiss nationality gave him neutral status (Bowlby [WHO report], 1951; Lovell, 2014). This was politically significant but not based on an attempt at international scientific agreement.
In 1950, Jean Delay and Henri Ey established an International Congress of Psychiatry that was independent of the ‘mental health’ objectives of the WHO, and sought to generate new theories of psychopathology, in particular infantile psychiatry. This was encouraged by Robert Debré’s developing work at the Centre International de l’Enfance in Paris that had established collaborations with the Institute for Child Study in London and other centres internationally. The First International Congress of Psychiatry had ended with an agreement to employ the term ‘behaviour disorders (troubles de comportment)’ as a general term to cover all conditions in childhood, as opposed to character disorders. The object was to avoid any kind of moral judgement of a child. These behaviour disorders could be divided into neurotic, organic, reactive states, and those of a precocious psychopathic nature, all of which were distinct from intellectual deficiency (Ey et al., 1952).
However, following this first International Congress of Psychiatry, the WHO, UNICEF and other post-war humanitarian organisations did not adhere to these guidelines to focus on ‘behaviour disorders’, and instead prioritised responses to the immediate needs of children for food, education and general support. These trumped any concerns regarding scientific classification in the immediate post-war period (e.g. WHO and UNICEF, 1951). John Bowlby’s famed 1951 report on the negative effects of ‘maternal deprivation’ was an example of immediate demand because the post-war era placed a focus on the problem of displaced and orphaned children (Thomson, 2006; Van der Horst et al., 2020; Vicedo, 2013). In fact, Bowlby had already successfully suspended major theoretical debates on child psychosis and ego development at the British Psychoanalytic Society during the war in order to prioritise child welfare projects (King and Steiner, 1992: 476–500, 867–9).
Nevertheless, the need for international agreement remained, and became increasingly important following a WHO Expert Committee Report on Mental Health in 1953. This report integrated representatives from countries beyond Europe and the USA, namely Dr MV Govindaswarmy from the Mysore Governmental Mental Hospital in Bangalore in India, Dr I Matté Blanco from the University of Chile, and Dr Phon Sansingkco from the Hospital for Mental Diseases in Thailand (WHO Expert Committee, 1953). Although prior committees had included representatives working in non-Western contexts, such as Margaret Mead and JC Carothers, these contributors had still largely adopted their own colonialist perspectives (Heaton, 2018; Lakoff, 2008; McCulloch, 1995; Pols and Wu, 2019). The 1950 meeting created a major shift in discussions on children’s mental health (WHO Expert Committee, 1953: 4). It encouraged government re-assessments of childcare facilities in countries where numbers of children in institutions were high (Evans, 2017; Eyal et al., 2010; Solomon, 2016). It also led to an increase in child psychiatric facilities in places such as India, where large-scale institutions had been less common (Malhotra, 2004). In 1956, Serge Lebovici, a child psychiatrist and psychoanalyst who had trained with Georges Heuyer at La Salpêtrière, was appointed as WHO Consultant in Child Psychiatry, and held a meeting on the proposed expansion of ‘child guidance’ clinics across the world, arguing these were ‘an essential element in the structure of social and medical services’ (Buckle and Lebovici [WHO report], 1960). However, the increased internationalism, and the expansion of child psychiatric treatment methods, was also rapidly exposing the fallacy of child psychiatric diagnoses as scientific entities. This focused attention on the objective study and understanding of children’s ‘behaviour disorders’ and how these could be linked to psychiatric classifications.
Child schizophrenia, internationalism, and the use of film evidence at the 1957 Zurich Conference
When Elwyn James Anthony presented his film on childhood schizophrenia (Aspects of Childhood Psychosis) at the Second International Congress of Psychiatry in Zurich in 1957, there were two assumptions underlying the discussions at this conference. Firstly, there was an assumption that ‘the schizophrenias’ should sit at the core of all psychiatric theorisation. Secondly, international, universal and transcultural theories of child psychopathology (childhood schizophrenias) were regarded as an entry point to understanding mental illness in adulthood. The conference was titled ‘The present status of our knowledge about the group of schizophrenias’. There were 1900 participants and the papers were presented in five European languages: German, French, English, Spanish and Italian. Instances of childhood psychopathology were discussed in China, Brazil and across Europe and the USA. Participants also came from Thailand, Nigeria, Ghana and elsewhere, although there were no participants from the USSR due to Cold War tensions (Gutheil, 1958). During the conference, Eric Wittkower held a meeting on transcultural psychiatry attended by Thomas Lambo, Pow Meng Yap and others. As Delille has argued, Wittkower’s attempts to develop a transcultural psychiatry via the Transcultural Psychiatry Unit at McGill University in 1955 were motivated in part by an effort to unite anthropology and psychiatry, and to understand how interactions between biology and culture led to cross-cultural variables in psychiatric conditions (Delille, 2018: 286). Several papers at the conference considered this issue, including those on child psychiatry. This new internationalism encouraged new agreements on diagnosis and the measurement of children’s atypical psychological states.
As well as Anthony, key speakers on the topic of childhood schizophrenia included Heuyer, Kanner, Bender, Mildred Creak, Kenneth Cameron, and also RA Gallitano from Santiago in Chile. Although there were major disagreements over causation, and there were also fierce debates over treatment, there was unanimous consensus that the schizophrenia concept was vital in overcoming these differences. A group studying ‘schizophrenia among different peoples and in various areas’ looked at comparative rates of schizophrenia in Taiwan, Turkey, Angola, Egypt, Hawaii, Argentina and the Congo, and the different symptoms exhibited in different places (Stoll, 1959: 8–42). Many of these studies referenced ‘primitive’ states of mind that accompanied schizophrenic thought, integrating anthropological and psychological theories of early development into these comparative approaches that made early statistical claims about schizophrenia. There was agreement that schizophrenia was a universal diagnosis across countries due to its similar population percentage. Most contributors, including Anthony, placed this figure at around 1% of the total population (Anthony, 1957c: 00:44–00:58; 1 Campbell, 1958; Tizard, 1968). 2
Although Anthony was not technically working in the field of ‘cross-cultural’ or ‘transcultural’ psychiatry, his position as a British-Indian doctor with widespread international experience made him acutely aware of the issues at stake in such work. Anthony was born to Indian parents in Calcutta and educated in Darjeeling, India. He studied medicine in the UK and began his first medical assignment treating ‘shell shocked’ soldiers with John Rickman and Siegmund Heinrich Foulkes. He was then transferred to Hong Kong where he was appointed as Chief Medical Officer for South East Asia and tasked with providing day care for children who had survived the Hiroshima bombings in Japan (Anon., 2014; Flapan, 1982; McDermott, 2015). On his return to London, he worked under Aubrey Lewis at the Maudsley, and also worked with Anna Freud (Shepherd, 1980). In 1950, Anthony was granted a Nuffield travelling fellowship to study with Jean Piaget at the Institute Jean-Jacques Rousseau (Institute of Psychiatry [IoP], 1951). He was then appointed to the first academic post in child psychiatry established at the Maudsley and the Institute of Psychiatry in London as ‘Senior Lecturer in Child Psychiatry’. He also lectured at the London School of Economics. After his presentation at the 1957 Congress, Anthony was recruited to hold the world’s first endowed chair in child psychiatry: the Blanche F. Ittleson Professorship at Washington University. This would place him in a highly influential position to direct child psychiatric categorisation in the USA and beyond, and he continued to maintain an interest in international collaboration (Hersov, 1986; McDermott, 2015).
Anthony’s work in the early 1950s had increasingly brought him into contact with children who were non-verbal. Observation and visual evidence were thus important sources of evidence during any assessment. As Heinz Katschnig has argued, when Emil Kraepelin developed his observational approach to the history and course of psychiatric illnesses in the late nineteenth century, he was in a unique position as a German-speaking doctor in Dorpat (today Tartu) where most patients spoke Estonian (Katschnig, 2018). Anthony’s position was similar in that he could not communicate verbally with most of his child patients, and thus had to consider new ways to class and categorise them which were not based on language. Anthony’s film (1957a) was structured to follow the principles of observational sciences, and he frequently wrote about how he studied the ‘natural history’ of childhood psychosis, observing its progression as a scientist without intervening or changing its course (Anthony, 1958a). He had also produced a public engagement film following the ‘natural history of a psychotic illness’ (Anthony, 1957c; see also Tizard, 1968).
Anthony’s film presentation at the conference tried to unite the theory of developmental psychology with theories of adult psychopathology via the schizophrenia concept. Instead of studying a total population to find statistical norms, in the model of Piaget and Gesell, Anthony used the theory of developmental psychology to study a group of ‘psychotic’ children to classify the key components of their state of mind so that this could then be extended to understand the norm. As he put it, ‘my special purpose is the reinstatement of the psychotic within the theoretical framework of our normal practice’ (Anthony, 1958b: 211–12). This built on both Bleuler and Piaget’s conviction that schizophrenic thought was a ‘regression’ to early infantile unstructured ‘autistic’ thinking (Bleuler, 1911; Piaget, 1923). It also built on Freudian theories of regression, in particular those developed by Melanie Klein (1930) and Susan Isaacs (1943/1991) who freely used the term ‘psychotic’ to describe early thought processes. National, social or cultural differences were not theoretically possible within this description of psychotic thought, because one key aspect of such thought was that it was not engaged with any form of reality. In this sense it was a perfect entry point for the universality of thought.
Anthony’s approach to childhood schizophrenia was to investigate the phenomenon at its core by observing, categorising and classifying the minute behaviour that compromised it. Although disagreements in cross-cultural psychiatry and child psychology were rife in this period, Anthony latched onto the areas of developmental psychology where there was significant agreement. By this time, psychologists had achieved some international agreements over critical developmental stages via film studies. In 1912, the psychologist Éduoard Claparède, director of the Psychological Laboratory in the Faculty of Sciences at the University of Geneva, had teamed up with the microbiologist Jean Comandon to create a film documenting experimental tests with children (Lefebvre and Pastre, 2012). Claparède and Comandon’s (1922) film, Scènes de psychologie de l’enfant, traced psychological development from infancy to late childhood, and employed comparative psychology to demonstrate children’s differing abilities to conduct tests and tasks (Evans, forthcoming 2024). These films documented standard developmental norms and intelligence tests, and inspired Claparède’s prodigy, Jean Piaget, to continue this work at L’École des Sciences de l’Éducation (Institut Jean-Jacques Rousseau). In the USA, Arnold Gesell produced thousands of films documenting developmental norms according to age at the Yale Clinic of Child Development in New Haven (Curtis, 2011). By gathering information on typical behaviour, Gesell’s extensive films (e.g. Gesell, 1931) documented the average ages when children gave their first smile, took their first steps, spoke their first word, etc., according to a Galtonian normal distribution curve (Curtis, 2011).
However, neither Claparède’s nor Gesell’s films had focused on states of distress and psychopathology. Psychoanalytically oriented thinkers, such as the anthropologist Margaret Mead, had produced films of the mother–infant relationship. In her studies of Balinese culture in the late 1930s, Mead depicted the distress exhibited in infants in response to their mother’s actions, making claims about the psychological consequences. In her written work, Mead (1928) made biased assumptions about weak forms of ego development in non-Western cultures that supposedly influenced general psychological development within the culture. René Spitz produced similar films in Mexico and the USA, highlighting the dangers of lack of maternal care in infant development, and demonstrating outcomes in very young children, yet again with a focus on mothers. John Bowlby’s films on ‘maternal deprivation’, e.g. A Two Year Old Goes to Hospital, also became well known for showing distress in children separated from their mothers (Bowlby and Robertson, 1952). Lisa Cartwright and Katie Joice have argued that these psychoanalytically influenced films from the 1930s to the early 1950s represented a new kind of visual representation, Joice maintaining this enabled a ‘micro-analysis’ of behaviour that interrogated the mother–infant relationship in minute detail (Cartwright, 2004; Joice, 2021). However, none of these films had investigated childhood psychopathology in any detail, and none had used ‘psychotic children’ as a group via which one could study similar behaviour and movements. It was not until the 1957 Congress that this focus on the behaviour of individual childhood psychopathology began to gain a shared visual language that would go on to underpin international child psychiatry. Anthony’s film explicitly tried to remove the human element from his objective sequences of children’s behaviour, in a mode similar to what Daston and Galison have described as ‘mechanical objectivity’. He sought to remove himself, and all other actors, from the process of classification, and to let the child’s behaviour speak for itself (Daston and Galison, 2010).
Anthony’s film was based on 70 children who had attended the ‘psychotic clinic’ at the Maudsley that Anthony had established with Kenneth Cameron (Evans, 2014). In the film, Anthony argued that there were four contemporaneous views about the phenomenon of childhood psychosis. One view was that it did not exist at all; the second was that it was a ‘rag bag’ for many other clinical conditions; third, that it was a specific disease entity; and fourth, his own view, that it was ‘a syndrome with a mixed aetiology but a common symptom pattern’ (Anthony, 1957a). This focus on the ‘symptom pattern’ of schizophrenia drew from Kraepelin’s studies on dementia praecox and manic-depressive insanity that tracked the form and progression of adult psychopathology over time (Berrios, 1988; Berrios and Hauser, 1988). Yet, Anthony also drew from Claparède’s, Piaget’s and Gesell’s work on developmental patterns in infancy and childhood. He argued that childhood schizophrenia could be identified by behaviour alone, claiming that the diagnosis was both universal and international.
The film featured internal titles interspersed with images and sequences of film depicting children engaging in activities such as painting, drawing, playing with sand, etc. It argued that each child’s mental state affected their ability to do these tasks. In almost every shot the children were filmed independently, with adults featuring only as helpers who were frequently ignored. The film began with the statement that: ‘the story begins with an infant rendered vulnerable by genetic, organic, maturational and other unknown factors’ and ‘on this vulnerable child, a “bad” environment begins to act, sometimes from the very beginning’ (Anthony, 1957a). The viewer was then shown still shots of small babies next to images of the ‘psychotic’ children that they would then grow up to become (Figure 1). The film then presented text classifications of all possible types of childhood psychosis, coupled with short clips showing behavioural demonstrations for each type. Anthony then turned to the different phases associated with all childhood psychotic illnesses. Finally, he looked in more detail at the behavioural symptoms that ensued after the full psychotic episode had stabilised (Anthony, 1957a).
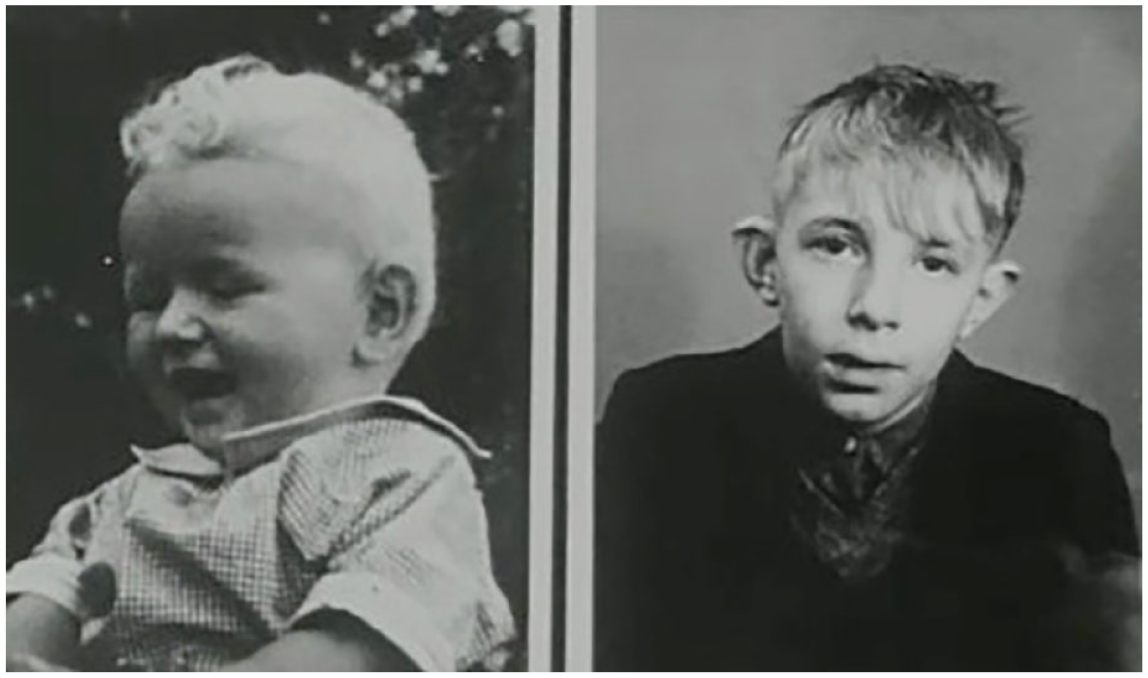
Stills from Elwyn James Anthony’s film Aspects of Childhood Psychosis (1957a); all images are stills from this film, with permission of Bethlem Museum of the Mind, Beckenham, UK.
Anthony argued that psychosis took place along a ‘continuum’. In his view, the mental state of psychosis was uniform across all children, yet it could be triggered by different causes, each also showing slightly different behavioural manifestations. The ‘normal’ continuum featured behaviour that could be seen in children who followed normal or typical developmental stages. The ‘defective’ and ‘organic’ forms were accompanied by behaviour that was outside this range (Figure 2). Finally, the ‘neurotic’ continuum could sometimes be confused with neurotic behaviour and obsessive actions (Figure 3). The ‘psychopathic’ continuum was associated with delinquency and sexual obsession (Figure 4). One of Anthony’s key arguments here was that children presenting with similar symptoms were not suffering from unique syndromes, but could all be located within a range of behaviour that was characteristic of childhood psychosis.
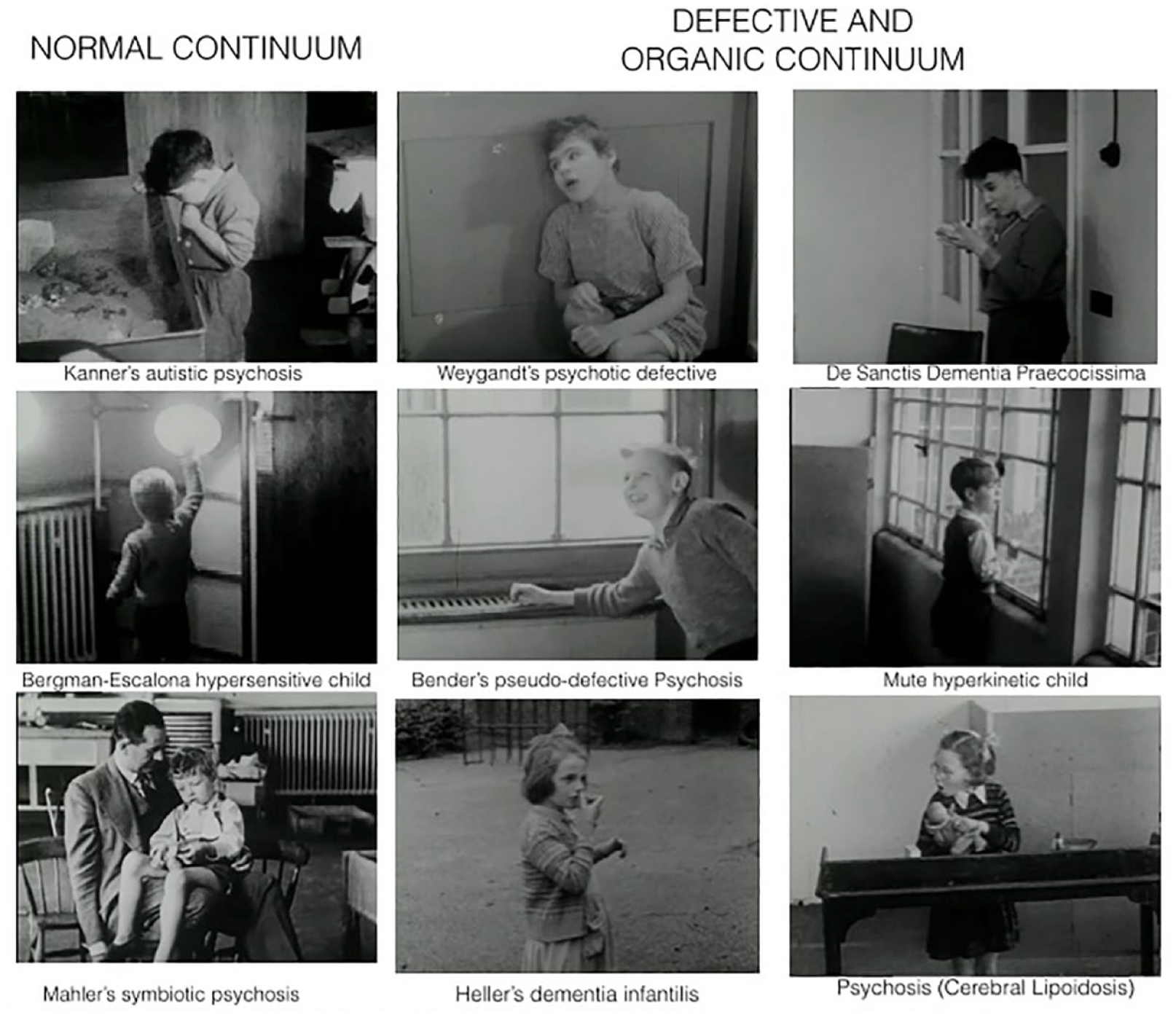
‘Normal’, ‘Defective’ and ‘Organic’ continuums (Anthony, 1957a).
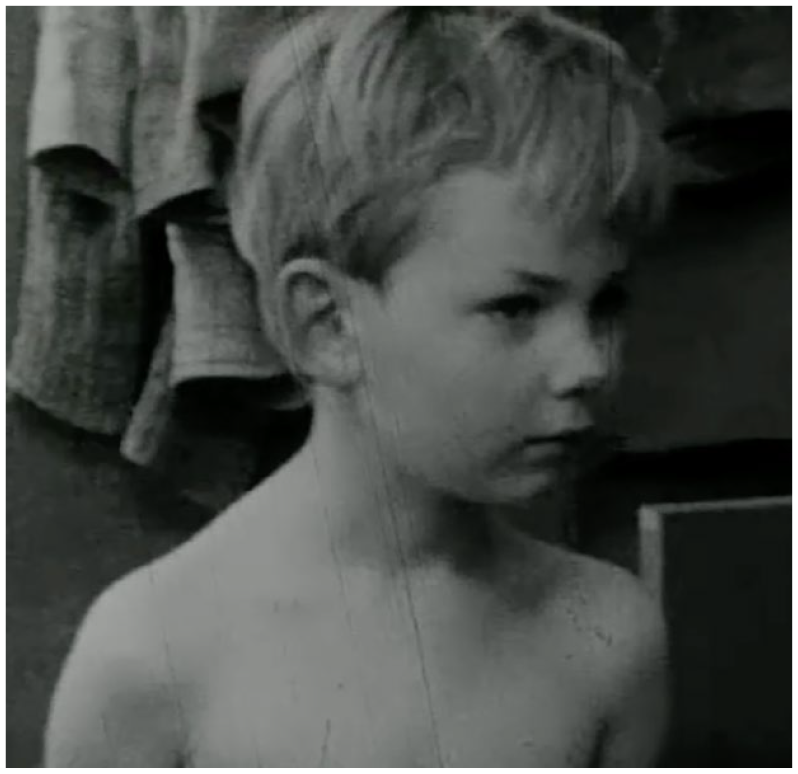
‘Neurotic’ continuum: Ekstein’s neuro-psychosis (Anthony, 1957a).
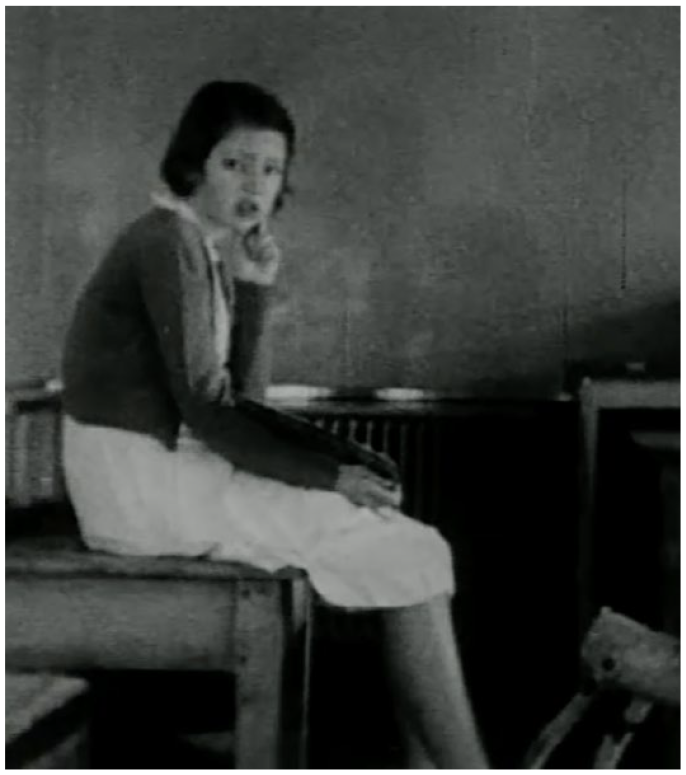
‘Psychopathic’ continuum: Bender’s pseudo-psychopathic psychosis (Anthony, 1957a).
By the early 1950s, a number of child psychiatrists had tried to claim specific syndromes associated with mental pathology in childhood. For example, Leo Kanner (1943) had claimed a syndrome of ‘infantile autism’ based on his classic study of 11 children. Anthony argued this was not a unique syndrome, but just part of a wider pattern seen within general childhood psychosis. In Anthony’s film, ‘Kanner’s autistic psychosis’ was represented with a short film sequence of a boy repeatedly sifting sand through his fingers. Likewise, in 1947, Paul Bergman and Sibylle Escalona from the Menninger foundation had published a report of five children in which they had seen ‘unusual sensitivities manifesting themselves in several, if not all, sensory modalities (visual, auditory, tactile, etc.)’ (Bergman and Escalona, 1947). Anthony again regarded this as just a variation within the ‘psychotic continuum’. In his film, he represented the ‘Bergman-Escalona hypersensitive child’ with footage of a boy avoiding and overcoming multiple obstacles in order to reach out and touch any light bulb that he could see. ‘Dementia praecocissima’ (De Sanctis, 1906) was represented by a boy making repetitive, stereotypical and aggressive movements. Theodore Heller’s (1908) similar diagnosis of ‘dementia infantilis’ was depicted with a girl walking around in a confused state and repeatedly hitting a wooden block against her lips.
Anthony’s film sought to demonstrate was that all of these ‘syndromes’ that psychiatrists had tried to claim as their own were based on very small sample sizes. His wider sample of children at the ‘psychotic clinic’ convinced him that none of these syndromes was a unique clinical entity, but that they all slotted into a wider symptom pattern of childhood psychosis. His London location, at a time when the international community had just condemned deficiency institutions and asylums, placed him in a unique position to observe ‘child psychosis’ in all its forms. Many children previously hidden in deficiency institutions were suddenly coming to the attention of clinicians at research-focused centres such as the Maudsley and the Institute of Psychiatry. Although this was not a full population sample, as used by developmental psychologists like Gesell to identify ‘norms’, Anthony considered this a large enough sample to claim universality of psychotic symptoms. Within a growing international community challenging the spectre of eugenics and racism, this was not just an act of classification but also a call to common humanity. Anthony’s use of short behavioural film sequences challenged the idea that each ‘syndrome’ somehow sat outside the range of possibilities within normal human psychological development. Anthony argued that, although these syndromes showed different ages on onset, and had different influences on psychological development, none was in a class of its own but just part of a wider continuum of human thought patterns and behaviour (Anthony, 1957a).
Anthony argued that the ‘natural history’ of any childhood psychosis depended on the ‘age of onset’, ‘direction of illness’, ‘rate of progress’, ‘retention of speech’, ‘degree of withdrawal’, ‘degree of regression’, ‘degree of rigidity’ and ‘mother–child relationship’ (Anthony, 1957a: 12:54). The film included short sequences of children who were having a ‘psychosis’ at different ages, each characterised by different behavioural symptoms. For example, the film included a series of short sequences of children drinking milk from a bottle, prefaced with text stating that their milk consumption ranged from ‘active rejection in the younger child to greedy acceptance in the older child’, depending on the age that the psychosis took hold (Anthony, 1957a: 18:36). Anthony had written candidly on his use of Freudian concepts in collaboration with Piagetian theories of development (Anthony, 1957d). There were also therapists working at the Maudsley psychotic clinic who had been influenced by psychoanalysis, in particular Clifford Scott and Danny Oftedal. Oftedal was a Norwegian child psychiatrist, who had been offering therapy at the psychotic clinic under a collaborative scheme organised by the United Nations (Oftedal, 1953). Anthony’s depiction of milk consumption drew from Melanie Klein’s work on greed, withdrawal and aggression in children, and how ‘in early infancy anxieties characteristic of psychosis arise which drive the ego to develop specific defence mechanisms’ (Klein, 1946: 99). Although Anthony was not a Kleinian, he was attempting to develop a conceptual framework that integrated the psychoses in a similar way to Klein, although he made no judgement on whether psychotic thought could be traced to the first six months of life, as Klein had famously argued. Theoretically, Anthony drew more extensively from Piaget, regarding the earliest forms of thinking as ‘autistic‘, and from Bleuler in maintaining that schizophrenic thought could adopt a variety of forms (Bleuler, 1911; Piaget, 1923). Anthony’s understanding of psychosis was fundamentally a complete breakdown in mental functions that had a knock-on effect on development, yet this effect could only take a limited number of forms, pictured in his film (Anthony, 1957d, 1958a). The film tracked the stages of breakdown from the ‘prepsychotic’ through to a total breakdown in which children were shown running, shouting, biting and destroying objects (Anthony, 1957a).
Although Anthony’s film was focused on short behavioural film sequences that he claimed were characteristic of psychosis, his overarching method was to place these short behavioural sequences within a wider theory of psychological development and self-identification. Building on the work of Havelock Ellis and Freud, he depicted children in what he called ‘auto-erotic’ behaviour, and states of ‘auto-aggression’. In practice, this referred to any kind of non-sexual self-soothing or self-harming activity to protect the ego during psychotic states (Anthony, 1957a). The film also featured a couple of children observing their reflection repeatedly in the mirror, during a state defined by Anthony as ‘narcissism’ (Anthony, 1957a: 28:11) – a reference to Freud’s work on primary narcissism as a means to defend the ego when it felt under threat, creating a ‘disordered self perception’ (Freud, 1914/2001b). Other children were depicted in protective states, such as ‘passive retreat’ in the ‘yogi child’ – a reference to Indian Yogic traditions at a time when these were less well known in Western contexts – who shuts out all contact in order to preserve himself (Anthony, 1957a: 15:12) (Figure 5). Anthony’s attempts to understand psychosis within a wider theory of ego development also encompassed discussion of ‘primitive’ thinking and behaviour that did not show an educated response to objects, and several behavioural sequences showed children adopting, what he termed, ‘primitive relationships with things (sticks, stones, paper, etc.)’ (Anthony, 1957a: 28:58). In these behavioural sequences, children would show excessive attention to and reverence for inanimate objects. Anthony’s approach thus spanned disciplinary approaches from anthropology, psychoanalysis, psychology, psychiatry and other human sciences. His work reflected the wider themes of the International Congress of Psychiatry, and the important place allocated to schizophrenia within wider human sciences in this period.
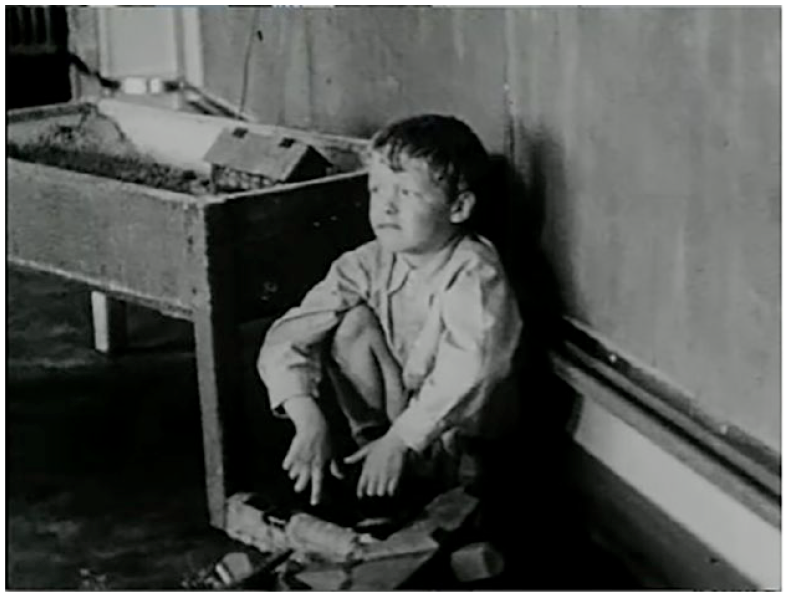
Yogi child (Anthony, 1957a).
In the final stages of the film the viewer was shown multiple forms of repetitive behaviour that Anthony regarded as part of long-term psychotic states of mind. These depicted ‘rigidity of behaviour characterised by endless repetition’ (21:24), ‘Bizarre motor behaviour – flapping, chopping, tapping – with a suggestion of symbolism’ (22:06) and ‘graceful elfin-like psychotic dancing movements’ (24:08) (see Figure 6).

Examples of repetitive movements and behaviour (Anthony, 1957a).
Anthony argued that these kinds of repetitive movements were common in children who had been placed in institutional care. He even claimed that it would be unusual to see any behaviour that did not fit within this range of patterns within any institutional care setting (Anthony, 1957a). This was a very strong claim because he was essentially arguing that he had identified all kinds of atypical human behaviour, and the patterns they could follow. He framed this around a wider theory of human development, ego development, and the breakdown of mental functions.
Anthony’s film and the study of ‘primitive’ and ‘regressive’ object relations
As well as the film, Anthony also presented a paper at the 1957 Congress in which he drew from the work of Jean Piaget to argue that ‘there are two basic ways in which human beings adapt themselves to the object world around them’ (see Stoll, 1959, Vol. III: 490). Firstly, this was via cognitive orientations, where they learn the object through its quantitative and qualitative characteristics. Secondly, they relate to the object via cathetic orientation, in which feelings are attached to the object. Children moved through the ‘sensorimotor’ stage of object relations, through to the ‘egocentrically-oriented’, and finally full cognitive development at age 12. However, Anthony argued that via the processes of: regression and rigidity a simplification of intention takes place, so that the child does less with fewer things, sliding backwards down the hierarchical scale of objects finally reaching a level at which the thing loses all meaning except at part of some primitive sensorimotor patterning. (p. 490)
In his understanding, psychotic children all experienced a regression to earlier stages in their understanding of objects, causing the symptoms demonstrated in his film. Anthony argued that his approach ‘brings the psychotic child fairly and squarely back into the mainstream of child psychiatry, and does not isolate him as a weird psychological monster’ (p. 492).
Anthony’s attempt to locate film depictions of childhood psychosis within a wider theory of psychoanalytic and psychological approaches to developing object relations was clear in a second film shown at the conference: The Approach to Objects by Psychotic Children. This film compared responses of ‘normal’ and ‘psychotic’ children when handed objects such as a bracelet, a little doll and a mirror. ‘Psychotic’ children were depicted showing ‘regressive’ responses to inanimate things, rather then progressively recognising their permanence (Anthony, 1957b: 00:52). For example, whereas at the end of Piaget’s sensori-motor stage, a ‘normal’ child would show the capacity to retrieve a visible object from beyond an obstacle, ‘psychotic’ children were unable to do so. In the film, one child is depicted becoming distressed and upset at her inability to reach an object. She then begins to bite the hand of the psychologist conducting the test, instead of reaching behind a glass screen to retrieve the object (Anthony, 1957b: 08:08–09:10). The film followed Anthony’s objective to show that ‘psychotic’ children merely demonstrated object relations that were ‘regressed’, and therefore remained responsive to treatment through education and therapy.
This was the first film to focus on the issue of childhood psychosis. However, after the 1957 Congress, attempts to measure and understand these short behavioural sequences increased rapidly. In many ways, the film was an abstract take on earlier films of intelligence testing. Instead of demonstrating the age at which children would complete tasks, and their abilities to do so, it simply showed children continually and repeatedly ignoring or avoiding tasks. This was the opposite of society’s well-behaved, well-organised and educated children, which had been the focus of multiple psychological studies until then (Rose, 1999). However, after Anthony’s presentation, this model was then replicated in international childhood psychiatric studies that sought universal agreement and assessment. Anthony claimed that children’s psychotic thinking was comprehensible if one could capture, track and measure the behaviour, and track similarities across children, and therefore develop a deeper understanding of what was motivating that behaviour. The study of abnormal, atypical movement or behaviour sat at the heart of the studies that analysed child behaviour across a continuum, and attempted to locate outliers. Whereas Claparède’s and Gesell’s films had focused on assessing intelligence through action and behaviour, Anthony’s focused on severe psychopathology, and then used this as the basis for new classificatory schemes in child development that were inclusive of all children.
The influence of Anthony’s films on conceptual discussions on development and schizophrenia
Anthony’s films were critical in restructuring debates and discussions on childhood schizophrenia. Between 1953 and 1956, the WHO had organised a series of meetings on ‘the psychobiological development of the child’, to develop ‘research into the biological, psychological, and cultural determinants of personality structure’ (WHO Executive Board, 1956: 1). The members and invitees were all European or North American, the main group consisting of John Bowlby, Margaret Mead, Konrad Lorenz, Bärbel Inhelder, Frank Smith and Karl Axel-Melin, with Jean Piaget contributing significant findings (Tanner and Inhelder, 1956). The members of this meeting wanted to understand cross-cultural models of child development in order to understand adult health. As Julian Huxley put it, the discussions had ‘a very big relevance to the health of the world of the next generation’ (WHO Executive Board, 1956: 10). The question of whether atypical developmental responses were caused by environmental or genetic factors was a particularly controversial topic, and this issue continued to plague all research in cross-cultural studies of child development. For example, a WHO report in 1955 had employed Bowlby’s theories to advocate for psychological interventions in cases of infant malnutrition in Africa, hypothesising that this could be caused by maternal deprivation rather than lack of food (Geber and Dean, 1955). Following this, many psychologists sought to expose the fallacy of psychological research methods that did not take account of all factors involved in causation. Anthony’s work supported these critical perspectives, and encouraged new research methods.
At the 1957 International Congress in Psychology, just one month before the International Congress of Psychiatry, Dutch-born South African psychologist Simon Bieshuevel had criticised the work of Martin Lawrence Fick and other South African psychologists for building in inherent bias in their study designs that compared intelligence in white and black children. He warned against ‘cross sectional’ studies when studying children’s psychological capacity for learning, because the ‘problems involved in examining representative groups at successive age levels are virtually insurmountable’ (Bieshuevel, 1957: 165). 3 Furthermore, tropical diseases or chronic malnutrition could impact psychological development in ways not seen or understood in most Western contexts, and this was hampering the validity of international research (p. 165). JL Laroche and P Verhaegen from the Centre de la Psychologie de L’Union Minière de Haut Katanga in the Belgian Congo echoed Bieshuevel’s concerns, arguing that European intelligence tests were not designed to test for skills developed in other environments (Laroche and Verhaegan, 1957: 167). Gustav Jahoda, an Austrian psychologist then based at the Department of Psychology at the University of Ghana, took issue with child psychologists who assumed that their work on ‘primitive’ or early thought provided a lens through which to view ‘primitive’ thinking in other cultures (Jahoda, 1957: 171; see also: Havighurst and Neugarten, 1955; Piaget, 1932). The International Congress in Psychology then developed a shared statement that, within child psychological studies, ‘Toute idée de hiérarchie interculturelle est exclue. Toute comparaison interculturelle est souvent jugée fallacieuse’ (Mertens de Wilmars et al., 1957: 174). They also argued that the most fruitful studies relevant to universal human development would emerge in the study of abnormal child behaviour (p. 175). Anthony’s film became the epitome of everything that international psychologists supported in this period because it prioritised visual evidence, objectivity and universality over any claims to cultural or racial differences. Anthony was thus able to unite psychiatric and psychological approaches in a way that most other researchers did not do at this time.
Prior to Anthony’s film-based approach, child psychiatrists had primarily regarded childhood schizophrenia and psychoses as clinical diagnoses verified according to the number of cases that a clinician had seen. For example, Kanner’s initial article on ‘infantile autism’, which he understood as ‘the earliest possible appearance of schizophrenia in children’, had only referenced 11 cases (Kanner, 1943). Yet at the 1957 Congress of Psychiatry, clinicians were becoming more aware of the need for more evidence, rather than just clinical judgement, and they also began to take cultural factors into consideration. Kanner claimed at the Congress that he had actually seen 150 cases of ‘infantile autism’ in ‘Anglo-Saxon’ countries, claiming a greater number of cases, and a clarification on cultural context (Stoll, 1959, Vol. III: 445). Pow Meng Yapp, who had developed the concept of ‘culture bound syndromes’, argued that the most severe cases of schizophrenia that he had studied in Southern China were those that arose in very young patients and were characterised by thought disorders, poor affectivity and catatonia. However, he argued that delusions, hallucinations and intelligence were irrelevant to prognosis (Campbell, 1958; Crozier, 2018; Stoll, 1959). This raised new questions about which symptoms predicted future problems, particularly as most Western theorists considered hallucinations and delusions to be central to the severity of all diagnoses.
At the 1957 Congress, Prasop Ratanakorn, Director of the Prasat Hospital for Neurological Disorders in Bangkok, Thailand, argued that although Westerners, such as WHO expert Charles Gundry, had assumed that Buddhist culture, demand feeding and frequent cuddling exerted ‘regressive effects on psychosexual development’ and a higher tendency toward schizophrenia in Thailand, there was no proof that this was the case (see Ratanakorn, 1959). In the mid-1950s, the Nigerian psychiatrist Thomas Lambo had started collecting statistics on the incidence of psychiatric disorders while he was working at the Aro Mental Hospital from the mid-1950s (Heaton, 2018); he presented these statistics at the 1957 Congress to challenge prevailing beliefs about ‘the African Mind’, in particular the belief that African’s were inherently ‘primitive’ and childlike in their thinking (Carothers [WHO report], 1953). He claimed that this encouraged unhelpful understandings of the origins and development of schizophrenia which epidemiology could correct. As with Anthony, Ratanakorn and Yapp, Lambo’s interest was not in creating theoretical coherence in diagnostic psychiatric categories via statistics, but in using objective observation methods and statistics to demonstrate shared understandings of human development overall (Lambo, 1956, 1957, 1958). Anthony’s film was an important and new form of evidence that international and cross-cultural researchers used to challenge both racist and culturally biased methodological approaches to human development.
Anthony’s theories on childhood schizophrenia, and his visual presentation on this at the 1957 Congress, can only be fully understood when placed within this international context. He was well aware of the complexities of translating concepts across cultures, yet he occupied an interesting space in the history of psychiatry because he never wrote on cross-cultural or transcultural psychiatry explicitly. Instead, he focused on creating universal models of child psychopathology in a way that could cross cultural boundaries and achieve international recognition. It was for this reason that he was appointed to his posts at the Institute of Psychiatry in London and at Washington University. Yet his role in the establishment of Child Psychiatry as an academic subject has often been overlooked and glossed over in historical studies. Researchers with clear national and Western locations have instead been given precedence to Leo Kanner, Lauretta Bender, John Bowlby and others.
However, it is important to recognise that the establishment of child psychiatry as a discipline occurred in the midst of this growth in international collaboration. Aubrey Lewis, Anthony’s mentor, had always considered social psychiatry as a way to study different cultures and their impact on the development of psychiatric conditions, basing it loosely on William McDougall’s theory of ‘social psychology’ in which he argued that psychology should form ‘the basis for all social sciences’ (McDougall, 1908: 2). In the 1950s, transcultural psychiatry was in many ways a subfield of social psychiatry, because both had similar objectives (Antić, 2022; Delille, 2018; Hennig, Delille and Müller, 2023). In the 1950s, the concept of culture was also beginning to be used to understand ‘subcultures’ in the West, in particular by the Birmingham School which built on the work of the Chicago School from the 1920s (Hoggart, 1957). Most child psychiatrists in the UK were familiar with social studies of delinquency and deviancy linked to the Chicago School via the model of child guidance clinics that had developed in the USA (Jones, 2002; Stewart, 2009). Anthony’s work showed an in-depth understanding of what was at stake in the description of child psychopathology that included the study of society, culture and the individual. He realised that international collaboration was not possible without a major change in the understanding of childhood psychopathology, one that could cross disciplinary boundaries in psychiatry, the social sciences, and international mental health research.
This growing internationalism also had a significant effect on the psychiatric treatment of children. For example, Bender was well known for adopting an aggressive approach to the treatment of childhood schizophrenia at the Bellevue in New York. She had used highly experimental treatments on children, including metrazol ‘shock’ therapy and electroconvulsive therapy, with the goal of shocking the nervous system into a new state of functioning (Bender, 1953). These treatments were given with the same rationale as similar treatments for adults in this period, and were a continuation of those used at the same hospital by Frances Cottington from 1941 (Cottington, 1941). Bender had also written extensively on the ‘primitive’ minds of her African-American patients in a manner that was unselfconscious, privileged and racially motivated (Doyle, 2010). None of this sat well with a growing international community facing up to the realities of World War II, challenging racism and constructing new understandings of children’s developmental needs and rights in collaboration with UNESCO, UNICEF and the WHO. Bender was challenged by increasing numbers of specialists and non-specialists (Bender, 1959). Her entry into the international community therefore saw her presenting a less aggressive and entitled version of child psychiatry, and she encouraged deeper reflection on conceptual origins rather than aggressive responses. The influence of international classification approaches such as Anthony’s was thus far-reaching, and its significance cannot be underestimated in reshaping approaches to children who did not match developmental ‘norms’. In fact, changes to the study and treatment of these children did not change immediately after the war, but only after concerted efforts by Anthony and others to change the conceptualisation of their states of mind.
The international influence of Anthony’s work at the 1957 Congress
Although Anthony had been concerned primarily with building observational approaches that paralleled studies in developmental psychology, his work actually went on to form the basis for child psychiatric epidemiology that soared as a technique in the 1960s. It influenced studies of childhood psychosis and schizophrenia, and also wider psychiatric approaches to problems in childhood generally extending beyond severe cases. In 1958, a WHO Meeting on ‘Epidemiology and Mental Health’ in London had drawn attention to longitudinal studies, retrospective studies and twin studies as important new approaches to the understanding of children’s mental development; the importance of sample sizes and statistics was also discussed (WHO Expert Committee on Mental Health, 1960). Of course, all these methods required unified approaches to categorisation, and psychologists tried to find ways to reach agreement. In the same year, the Unit for Research in Occupational Adaptation was renamed ‘The Social Psychiatry Research Unit’, and came to serve as the bureaucratic hub for large population studies in psychiatry. The WHO’s calls to move away from institutional care, and towards improved social work, also influenced child psychiatry via these new models of study. The use of easy film sequences to identify children who were different, and to support new treatments for them, was an important new technology with international appeal.
In 1959, Emmanuel Miller founded an Association of Child Psychology and Psychiatry, and established a Journal of Child Psychology and Psychiatry that united these two disciplines in the same spirit as Anthony’s work, and this quickly attracted an international audience (Miller, 1960). In the first issue, Anthony considered whether children could experience ‘manic depressive illness’ (Anthony and Scott, 1960). Also, Leo Kanner grappled with the question: ‘Do behavioural symptoms always indicate psychopathology?’ This was a question that he had not asked prior to the international conference, but it was one that now occupied almost all psychiatrists from the early 1960s onwards. For his part, Kanner threw doubt on the observations of both clinicians and parents, but without offering a clear way forward (Kanner, 1960). Of course, the WHO had already begun the integration of mental disorders into the International Classification of Diseases, and in 1952 the American Psychiatric Association (APA) had embarked on its Diagnostic and Statistical Manual of Mental Disorders, which included ‘schizophrenic reaction: childhood type’ under the broader heading of ‘psychotic reactions’, framing this theoretically in relation to Adolf Meyer’s ‘reaction types’ (APA, 1952). Yet attempts to classify unique psychiatric conditions in childhood according to behaviour only began in the 1960s, and only then went on to guide psychiatric epidemiology. In 1961, Mildred Creak organised a working group to classify ‘schizophrenic syndrome in childhood’ according to behavioural measures, coming up with a list of behaviours thought characteristic of the condition, including ‘pathological preoccupation with particular objects’, ‘distortion in motility patterns’ and ‘abnormal perceptual experience’ (Creak, 1961). However, Creak’s list of behaviours did not incorporate developmental child psychology. Anthony’s film methods had been far more comprehensive in their approach.
Studies that truly challenged diagnostic categories required internationalism to push child psychiatrists to collaborate and reorganise. For example, in 1963, Tolani Asuni, a Nigerian psychiatrist, who had trained at the Institute of Psychiatry in London, claimed that labelling children was ‘no more no less’ than what the law said it was (Asuni, 1963). The most innovative child psychiatrists were working across cultures because they could see the true limits of categories that had been established within Anglo-American or European cultures. For some, like Anthony, this encouraged attempts to create universal modelling around Piagetian developmental concepts, yet it could equally encourage a radical reassessment of classificatory schemes. In the 1960s, studies exploring infant care and ‘maternal deprivation’ from the perspective of the social sciences, rather than mere observational studies, grew exponentially (e.g. Newson and Newson, 1963; Yudkin and Holme, 1963). These all questioned direct associations that had been drawn between a lack of maternal care and severe psychopathology in children, and encouraged social scientific approaches that studied large-scale samples, and thus had international applicability.
Anthony’s work provided a model in which film research could be employed to provide objective evidence in international collaborations. By the 1960s, WHO internationalism required universal agreements that were backed by statistical power. Inspired by Anthony and others, Thomas Pilkington, film consultant at the World Federation of Mental Health edited an ‘International Catalogue of World Mental Health Films’ in 1962 (Anon., 1990). Film became an important resource that could be used to corroborate findings. By 1964, many child clinics established ‘play rooms’ in which child behaviour could be filmed to enable comparisons (e.g. Lee and Hutt, 1964). Internationalism eventually pushed child psychiatrists, psychologists and anthropologists to take a behaviourist position backed by film visual evidence in epidemiological work. Furthermore, as film technologies developed and film became more accessible, film was increasingly used to validate claims about behaviour made in psychiatric epidemiological studies. From the 1960s, films about children’s psychiatric conditions extended into mainstream media. The development of child psychiatric epidemiology and the design of new psychological measurement instruments increasingly relied on video technologies to map and track behaviour.
After Anthony moved to Washington University in the late 1950s, the post of Senior Lecturer in Child Psychiatry at the Maudsley Hospital was left vacant until 1965, when Michael Rutter was appointed (IoP, 1964–1965). He had studied under Aubrey Lewis in London and Ben Pasamanick in New York (Rutter, 2001). Rutter took over responsibility for following up the children who had appeared in Anthony’s film (Rutter, Greenfeld and Lockyer, 1967). Pasamanick was an epidemiologist who was developing new ways to employ epidemiology to understand disease causation, and Rutter wanted to use this method to support the establishment of child development categories within the International Classification of Diseases. Rutter had his own experiences of cross-cultural development, having been born in Lebanon and learnt Arabic before moving to the UK and then the USA. In 1964, he had collaborated with Kingsley Whitmore, the Senior Medical Officer of the UK Department of Education and Science, to establish a survey of the ‘medical, behavioural, educational, and other handicaps’, including ‘childhood psychosis’, within a total population of children on the Isle of Wight, a small island off the south of the England with a total population of 100,000 (Rutter, Whitmore and Tizard, 1970). This study used small behavioural snapshots that were summarised and provided to teachers so that they could be employed en masse for the purpose of large statistical studies, containing behavioural definitions of human behaviour in a child, such as: ‘very restless, often running about or jumping up and down. Hardly ever still’, ‘has twitches, mannerisms or tics of the face and body’, ‘squirmy fidgety child’, ‘often destroys own or others’ belongings’ and ‘tends to do things on his own – rather solitary’ (pp. 410–11).
Shortly after setting up the Isle of Wight study, Rutter gave a lecture at the Central University of Venezuela in which he criticised the attempts of the American Psychiatric Association to develop a useful classification system for children, as it was ‘based on a mixture of phenomenology and theoretical assumptions’. Rutter (1965) then put forward his own system for dividing up psychological conditions seen in children, splitting these into 11 categories: 1. Neurotic disorders; 2. Antisocial or conduct disorders; 3. Mixed antisocial and neurotic; 4. Developmental disorders; 5. Hyperkinetic syndrome; 6. Child psychosis; 7. Psychosis developing at or after puberty; 8. Mental subnormality; 9. Educational retardation; 10. Depression; 11. Adult-type neurotic illness. This encouraged a wave of behavioural studies of key developmental concepts so that they could be used in large-scale statistical studies (e.g. Lotter, 1966). These classifications also formed the basis for recommendations to the WHO for a ‘multi-axial system of diagnosis’, with the ultimate goal of removing any kind of theoretical assumptions from classificatory methods in child psychiatry (Rutter, Shaffer and Shepherd, 1973). The late 1960s and early 1970s also saw the onset of a range of new technologies in observational sciences, such as improved access to film and improved methods in statistical psychiatry using basic computer systems. Both technologies played a part in enabling new perspectives on psychiatric disorder and difference to develop.
In the early 1970s, Peter Venables, a colleague of Rutter at the Institute of Psychiatry, established a longitudinal study of child health and development after a meeting with the WHO study group on neurophysiological methods (see Raine, Liu, Venables, Mednick and Dalais, 2010). This became a model for international epidemiological studies in child health, which problematised Bowlby’s assumptions about maternal care and psychological health further. Rutter’s criticism of Bowlby’s methodological approach, and his reliance on theoretical assumptions drawn from psychoanalytic theory, was fully mapped out in his publication, Maternal Deprivation Reassessed (1972), which sought to establish a completely new theoretical approach at the WHO. It drew from the Isle of Wight and other social science studies, such as the one by Yudkin and Holme (1963) to argue that ‘bond disruption per se has a negligible influence on intellectual development whereas lack of experience or stimulation has important deleterious effects on cognitive growth’ (Rutter, 1972: 85). As Rutter understood it, behavioural studies enabled general statements about negative effects on child development in ways that individual case studies and psychoanalytic theorisations could not. His belief was that, as more studies were conducted, it would be easier to draw associations between causation and psychiatric disorders determined via the multi-axial model. In 1975, the WHO published a report on the application of the multi-axial model for the World Health Organization (Rutter, Shaffer and Shepherd [WHO Report], 1975), and the method was later adopted in the International Classification of Diseases. This method was also introduced in DSM-III as a method to diagnose childhood psychiatric disorders.
Conclusion
The 1950s was an important period for the development of child psychiatry as well as transcultural psychiatry, international classification methods, and psychiatric epidemiology. All of these disciplines were given new impetus by growing internationalism and human and child rights agendas in the aftermath of World War II. Anthony’s work at the 1957 International Congress of Psychiatry was an important turning point for child psychiatric sciences because it popularised the view that severe psychological disturbances in children were amenable to scientific observation and study, and that such studies could generate knowledge on how to manage child populations effectively in democratic societies. There was then a surge in support for academic work on children’s psychological development that incorporated knowledge from anthropology, psychiatry and other human sciences, and created an integrated and systematic universal and humanitarian approach to child development. In fact, although there were many disagreements over how knowledge from developmental sciences should be employed to direct and intervene in the lives of children internationally, there was a remarkably high level of agreement on theoretical understandings of the development of typical and atypical thought processes in children that built particularly on the writings of Bleuler, Piaget and Freud. Anthony’s work was critical in creating a visual behavioural model for understanding children’s atypical development, and for using this as the basis for diagnosis.
When Michael Rutter advocated the use of behavioural measures and film sequences to diagnose childhood conditions internationally in collaboration with the WHO, he built significantly on the back of Anthony’s work, and the debates and discussions that had set the tone in the 1950s. Rutter was also influenced by the theoretical objectives that had driven Anthony, yet he believed that theoretical coherence would be the outcome of behavioural analysis, and the direction in which chid psychiatric research was heading in the future. Instead of proposing a uniform theoretical model, he advocated the study of behaviours that international child psychiatry would use to lead us to a unified theory in the future. Whether or not it ever reached that point, or if it ever will, is a question that still hangs in the balance.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was funded in whole, or in part, by the Wellcome Trust (Grant number 209795/Z/17/Z).