
Abstract
This article discusses the Admission and Treatment Unit at Fair Mile Hospital, in Cholsey, near Wallingford, Berkshire (now Oxfordshire). This was the first new hospital to be completed in England following the launch of the National Health Service. The building was designed by Powell and Moya, one of the most important post-war English architectural practices, and was completed in 1956, but demolished in 2003. The article relates the commission of the building to landmark policy changes and argues for its historic significance in the context of the NHS and of the evolution of mental health care models and policies. It also argues for the need for further study of those early NHS facilities in view of current developments in mental health provision.
Keywords
Introduction
This article discusses an early post-war, purpose-built mental health care facility, the Admission and Treatment Unit at Fair Mile Hospital, 1 in Cholsey, near Wallingford, Berkshire (now Oxfordshire). The institution, which later became Fair Mile Hospital, was built as a lunatic asylum in 1870. The post-war building, designed by the firm Powell and Moya, is directly associated with the launch of the National Health Service (NHS) in 1948: it was only the second new hospital building to be authorized by the government in England – after the Princess Margaret Hospital in Swindon, again by Powell and Moya (Powell, 2009: 87–8) – and, due to its smaller scale, the first one to be completed, in 1956. It was also the first hospital design to be completed by Powell and Moya, one of the most important post-war architectural practices in England. The firm went on to design a number of early NHS hospitals, introducing a series of significant hospital design innovations – and was awarded a Royal Institute for British Architects (RIBA) Bronze Medal in 1957 (BRO: P/HA2/1/1/3, 1160, 9 May 1957). Nonetheless, following the hospital’s decommissioning and closure in 2003, sadly the building has been demolished, although the Victorian asylum building has been listed at Grade II and converted to housing.
Following the brief introduction here, the article includes a literature review and a summary of the main available sources. It also presents all information available in archival and secondary sources on the commissioning and realization of the building, as well as information on its active life. This part demonstrates the limited coverage that the building has received in existing scholarship, while subsequent discussion also positions the building within the context of the introduction of the NHS and the evolution of mental health care models and policies. The article therefore points out how early the commission was, despite strict budgetary constraints, and argues for the historic significance of the building. As a result, this study also highlights the significance of the Oxford Regional Hospital Board as leaders in the production of specialist hospital spaces in the early years of the NHS. The region has been widely recognized for several of its new general hospitals and for its development of a ‘steel-framed system for building quickly and economically – the “Oxford method”’ (Harwood, 2015: 292–3). However, its contribution to mental health facilities has received limited attention, although this information is needed for a more complete understanding of the pioneering role that the Oxford region played in terms of modern health care built environment in the early post-war period.
More broadly, the article uses the Admission Unit at Fair Mile as a case study that can reveal a much wider gap in existing historiography: the virtual absence of psychiatric facilities as a whole for the post-war period – not simply an individual building. In this connection, the discussion aims to make the case that a wider consideration of all mental health facilities designed for the early NHS is long overdue and can contribute to a more complete understanding of the evolution of mental health care provision from the early and mid-twentieth century to the present time. Considering current shortages in mental health ‘beds’ and certain similarities to Acute Mental Health Units commissioned and built in recent decades, especially following the issue of the National Service Framework at the beginning of the millennium (Chrysikou, 2014: §2.6), the article also claims that such a study is not simply of historical significance and that a closer examination of those overlooked but novel designs remains relevant today.
Literature review
Post-war psychiatric facilities
Buildings and other spaces accommodating private and public institutions for the mentally ill and the mentally ‘deficient’ have been extensively covered in existing scholarship in a wide range of study fields (Philo, 2004; Stevenson, 2000; Taylor, 1991, 2007; Yanni, 2007). Relevant historiography covering global examples continues to expand by addressing unexamined or under-examined aspects, a range of spatial scales and an interdisciplinary approach that, far from limited to the field of architectural historiography, also embraces areas such as the social history of medicine, the history of psychiatry, and human geography (Topp, Moran and Andrews, 2007).
In sharp contrast to the extensive and well-established scholarship on asylum architecture and its role in the development of psychiatry and the social history of madness, scholarship on mental health care facilities in the twentieth century remains largely fragmentary, although it is growing (Scull, 1989; Soanes, 2011; Topp, 2007, 2017). However, as regards the second half of the century in particular, emphasis is often placed on the gradual transition away from institutionalized care, and this radical shift in policy has also had a remarkable impact on related architectural historiography – or rather its striking scarcity. The new care model was initially associated with a turn to the assimilation of specialist psychiatric wards within the general hospital and seems to have largely distracted architectural historians from mental health care facilities as an area that deserved particular attention. Although there have been several studies emerging which focus on mental health in the post-war period, these do not focus on architecture and buildings or have not been published (Davies, 2001, 2002, 2007; Gittins, 2007).
Significant publications that focus specifically on realized health care buildings in England, and aim to provide an overview of the field, have either stopped at 1948 when the NHS was launched, or have effectively overlooked the post-war period. A national survey by the Royal Commission on the Historical Monuments of England (RCHME) – carried out between 1991 and 1994 and published in 1998 – ‘set out to create a representative archive of all types of purpose-built hospitals’ (Richardson, 1998: ix), but has only covered the period 1660 to 1948: ‘from the earliest purpose-built post-medieval hospital in England, Bethlem Hospital in London, to the inauguration of the National Health Service’ (p. ix). Beyond the selected examples that are discussed in the book – each ‘chosen to demonstrate an aspect of the evolution of hospital design’ and representing ‘a wide variety of both the typical and the atypical’ (p. x), the survey compiled a database of some 2000 sites. ‘A county-by-county list of these is given in an appendix to this book’, 2 whereas ‘the archive material is publicly accessible in the National Monuments Record Centre at the Royal Commission’s head quarters [now the Historic England Archive]’ in Swindon (p. x). The survey analyses ‘the evolution of English hospital design during a period of enormous change in English society and of important discoveries and developments in medical science’, and recognizes that hospitals (including mental hospitals) are a ‘substantial but little-studied building type’ (p. vii). 3
Thirteen years after the RCHME survey, English Heritage published a ‘Listing Selection Guide’ on ‘Health and Welfare Buildings’, but this only tangentially touches on twentieth-century mental health care facilities. In three long paragraphs discussing asylums, there are just two sentences that briefly mention one particular influence on design in the 1920s (English Heritage, 2011).
Conversely, the ‘hospital’ remains an area of inquiry for architectural historians, with some of them even revisiting earlier periods only (Arnold, 2013). Yet mental health care is not automatically included, presumably reflecting differences in care models – either earlier distinct categorizations between mental and physical health, or the subsequent move away from the medical to the psychosocial model (Risse, 1999). In addition, more recent hospital studies have a range of geographical coverage and are gradually including increasingly longer periods of the twentieth century (Adams, 2008; Kisacky, 2017; Taylor, 1997; Thompson and Goldin, 1975; Verderber and Fine, 2000; Willis, Goad and Logan, 2019), and have even started stepping into the twenty-first century (Verderber, 2010).
Some recent studies that provide an overview of the historical evolution of mental health facilities to the present day have focused on geographical contexts other than England (Kovess-Masfety, 2004). Other publications covering a range of geographical regions, including England, discuss mainly contemporary principles and specialist professional guidance and analyse contemporary case studies, but they do not discuss historic examples from the post-war period or other earlier periods (Chrysikou, 2014).
Case study: Admission and Treatment Unit at Fair Mile Hospital
Despite their virtual absence from related historiography, a number of purpose-built in-patient facilities for mental health provision in the early NHS period featured in the architectural press of the time and also appear in general architectural historiography. In her comprehensive study of post-war architecture in England, Space, Hope and Brutalism: English Architecture, 1945–1975, Elain Harwood (2015: 283) identifies the Oxford Regional Hospital Board as ‘the most architecturally ambitious’ in commissioning and building ‘several lightweight acute admissions units in the grounds of its Victorian institutions’. She specifically lists two units for the mentally ill that opened in 1956 – one at Fair Mile Hospital, Cholsey, by Powell and Moya (Figures 1 and 2), and one in Stone, Buckinghamshire, by Gollins, Melvin, Ward and Partners – and one unit for the mentally handicapped at Borocourt, Oxfordshire, also by Powell and Moya, which opened in 1964 (pp. 283–4). The two buildings by Powell and Moya also feature in Kenneth Powell’s monograph on this exceptional post-war practice (Powell, 2009: 87–8). These two secondary sources provide some general historical context, but their content remains limited as regards their association with specialist developments in the field of mental health care, or any in-depth typological or stylistic analysis of these units.
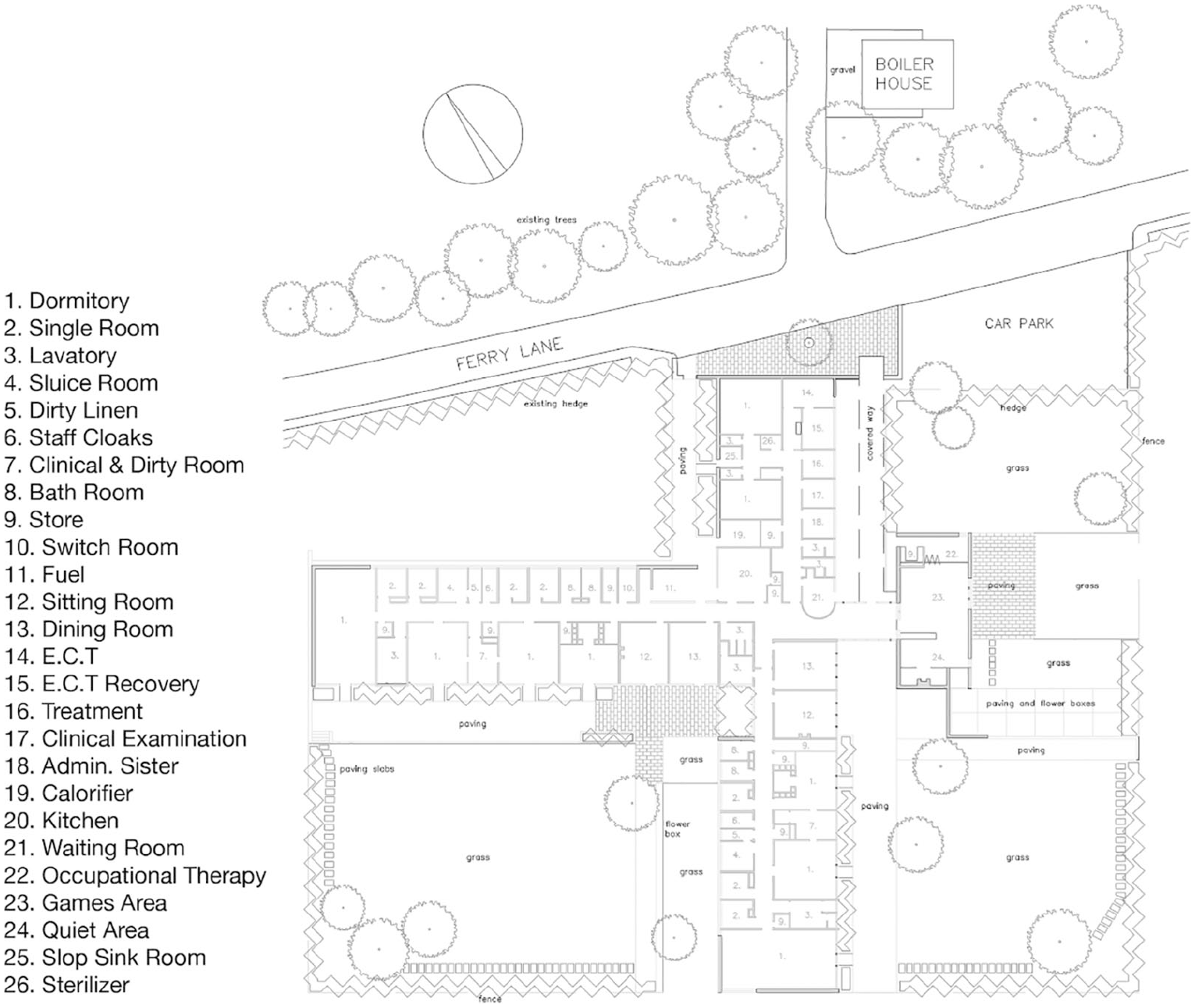
Powell and Moya, Admission and Treatment Unit at Fair Mile Hospital, in Cholsey, near Wallingford: ground floor plan (drawn by Alex Wood).
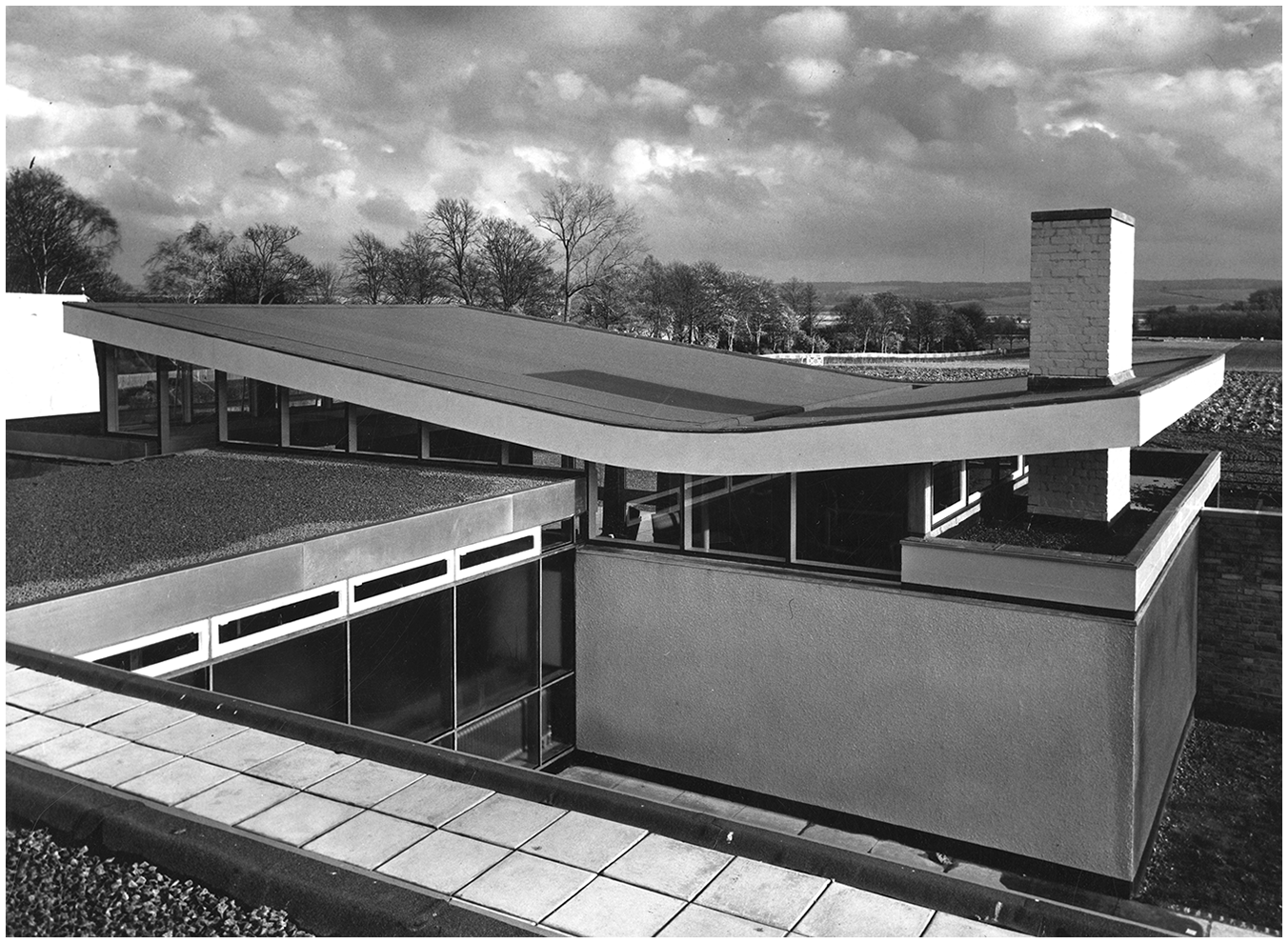
Powell and Moya, Admission and Treatment Unit at Fair Mile Hospital, in Cholsey, near Wallingford: exterior, 1956 (source: RIBA Architecture Image Library, RIBApix Ref. No. RIBA56472; published with permission).
A number of other related studies do not include these buildings, or any discussion of mental health care facilities in the post-war period. A 1974 monograph on Gollins, Melvin, Ward and Partners does not include their Admission Unit in Stone completed in 1956, nor a subsequent one for Dorchester designed in 1957, although it does include two larger hospitals of the 1960s (Aldous, 1974). A broader study of the role of architecture in the welfare state includes the early post-war period, with British examples among a wider range of case studies across Western Europe, but does not include mental health facilities (Swenarton, Avermaete and Van den Heuvel, 2015). In fact, in this 2015 collection of essays exploring ‘the complex role played by architecture in the function and development of the welfare state in both theory and practice’ (p. i), the authors recognize ‘hospitals and health centres’ as among the components of the built environment that related to its association with the ambitions of economic redistribution and social welfare set out by the welfare state (p. 1), but they do not focus particularly on health care in the main chapters of the book (although one London institution – Woodberry Down – is included). Finally, a recent collection that looks into twentieth-century architecture of public service in Britain has a chapter on health care buildings, but this focuses on the inter-war period (Brady, 2018).
Primary and secondary sources
The available primary and secondary sources on the chosen case study include a range of written and visual material. Archival sources comprise written documents and photographic material, whereas secondary literature also contains published drawings. The material identified to date spans the fields of architecture and architectural history as well as mental health history, policy and practice: architectural monographs, historical survey studies, and journals; architectural photographic archives; mental health policy studies; administrative hospital records (general and estates); and records of the General Nursing Council for England and Wales. Journal repositories consulted include the Royal Institute of British Architects (RIBA) Library, the British Library and the Wellcome Library in London. A full list of the archival sources is given in the references at the end of the article.
Secondary sources on Fair Mile provide valuable information about the institution and its new Admission Unit. The book entitled Diary of a Regional Health Authority 1947/1994: A Year-by-year History of Oxford Regional Hospital Board and Oxford Regional Health Authority (Moss and Everton, 1996) provides an overview of principal events, challenges and aspirations, similar to the first annual report mentioned below, but spreading over the full life of the first two administrative bodies for the region under the NHS. From a local history perspective, Fair Mile: A Victorian Asylum (Wheeler, 2015) focuses primarily on the period prior to the NHS, but does include useful references to the Admission Unit and its significance for Fair Mile.
Visual material includes archival black and white photographs held at the RIBA Robert Elwall Photographs Collection (RIBA: REPC: 55218-55218/37). Mentions of the building also appear in Philip Powell’s beautifully illustrated lecture notes from the 1980s and 1990s (RIBA Drawings and Archives: PoP/8). Additional visual material can be traced in published sources, most notably Wheeler’s book which reproduces several of a collection of photographs by ‘Mr Tony Spackman, Mental Health Service Manager at Fair Mile in its final years’ (Wheeler, 2015: 10). An online exhibition set up by the Berkshire Record Office (BRO) dedicated to the Fair Mile includes a very brief summary of the rapid developments in the post-war era, from 1948, when Fair Mile joined the NHS, to 2003 when it closed, following the key transition to care in the community in the 1980s (BRO: ‘For the Welfare of the Insane Poor’). But this includes no mention of the new Admission Unit, either in the text or in the accompanying images.
Fair Mile Hospital and its new Admission and Treatment Unit
Fair Mile Hospital
Initially introduced in the architectural press as ‘Berkshire, Reading, and Newbury Lunatic Asylum’ (Anon., 1870), Fair Mile has been known under a number of different names during its lifetime. These mainly comprised variations of the following: ‘Moulsford Asylum’ (1870–97); ‘Berkshire Lunatic Asylum’ (1897–c.1915); ‘Berkshire Mental Hospital’ (c.1915–48); and ‘Fair Mile Hospital’ (1948–2010) (BRO: D/H10/Admin. Hist.; see also Wheeler, 2015: 18). The original building for Fair Mile was purpose-designed and built as a Lunatic Asylum in 1870, and further extended in 1878, by Charles Henry Howell, one of the ‘key contributors to the design of asylums’ during the 1870s (Taylor, 1991: 153), who also held the position of Consulting Architect to the Commissioners of Lunacy (National Heritage List for England [NHLE]: Fair Mile Hospital; see also Wheeler, 2015: 12).
The size of the institution varied significantly during its lifetime. Initially, it would accommodate ‘133 male and 152 female patients – a total of 285’ (Wheeler, 2015: 13), but these numbers were far exceeded in subsequent decades. The Administrative History summarized in the Berkshire Record Office notes: During the First World War additional patients were transferred to the asylum from other hospitals, such as the Sussex County Asylum, when these were taken over as military hospitals. This also happened during the Second World War, when the hospital reached its greatest size, accommodating over 1,400 patients, as patients were transferred from Brookwood Hospital in Surrey, Great Yarmouth Naval Hospital, Norfolk, and Hill End Hospital in St Albans, Hertfordshire. (BRO: D/H10/Admin. Hist.)
Overcrowding is noted as a significant problem in post-war hospital committee minutes. By the end of World War II, a considerable number of war-time evacuees had been moved to the hospital, and 312 were still there in 1947, when the number of beds reached a total of 1202 (The National Archives [TNA]: DT 33/1243, 13 Nov. 1947: 1 and 3; 12 Apr. 1962: 1). In 1951 and 1959, the number of patients accommodated are given as around 1000 (BRO: P/HA2/5/1 Fair Mile Hospital, ‘Into the Light’: 3; TNA: DT 33/1243, 8 Mar. 1951: 6). From the 1960s onwards, in line with the new policies, the hospital decreased in size, and by the end of the century it accommodated only 200 patients (BRO: D/H10/Admin. Hist.).
To put these figures in perspective, it is worth mentioning that some of the London County Council Asylums after 1888 were built for 2000 patients (Jones, 1993: 120), that one of the two last mental hospitals to be built in England in the 1930s – Runwell in Essex – was for 1000 patients on the villa-system (p. 138), and that, in the early post-war years, mental hospitals often reached a maximum of 2500 or 3000 beds (pp. 145–6).
NHS administrative re-organization
Following the National Health Service Act of 1946, Fair Mile Hospital sat within the area of the Oxford Regional Hospital Board from 1948 until 1974, when further restructuring took place. Fair Mile was under the Berkshire Mental Hospitals Group Management Committee, but the Committee’s name was changed in 1957; this is of interest as it reflects changes leading to the Mental Health Act of 1959. The name change was discussed in June 1957: The Chairman reported that, with the publication of the Report of the Royal Commission on the Law relating to Mental Illness and Mental Deficiency, the time was singularly appropriate to make an alteration in the TITLE OF THE MANAGEMENT COMMITTEE to accord more closely with the present trend on the part of the general public to regard mental illness and disability in much the same way as physical illness and disability. (BRO: P/HA2/1/1/3, 1191, 13 June 1957)
Although such a change did go ahead, the name reported in that meeting – ‘The Mercia-Wessex Group Hospital Management Committee’ – was not actually adopted. Instead, at some point between 16 October and 20 November 1957, the Committee name changed from ‘Berkshire Mental Hospitals Management Committee’ to ‘St. Birinus Group Hospital Management Committee’ (BRO: P/HA2/1/5/1 Works Sub-Committee minutes).
Admission and Treatment Unit
The new Admission Unit was first reported in 1954 but no details were given about the commission of the design. Yet some insight is given into the significance of the project for the development of efficient care provision: ‘A separate admission unit is to be built [at Fair Mile], which will assist in the better classification of patients, and should provide good facilities for the clinical teaching of Student Nurses’ (TNA: DT 33/1243, 8 July 1954: 6). By this time, the first Regional Architect, Bill Jobson, who is named in journal articles alongside Powell and Moya, had also been appointed by the Oxford Regional Hospital Board (around 1952).
After the completion of the new Unit, the project was hailed as a significant development in the history of the hospital. In April 1956, I. Coffin Duncan and G. A. Lilly, Commissioners of the Board of Control, specially noted the new Unit and were particularly complimentary of it: Since this hospital was last visited an important event in its history has occurred: - the opening of the Admission Hospital. This new building is original in design and appears admirably suited to its purpose. It provides beds for 23 men and 30 women and has an excellent treatment unit for both in and out patients. (TNA: DT 35/194, Copy of the Report by the Commissioners of the Board of Control at their visit to Fair Mile and Hungerford Hospitals on the 12 and 13 of April, 1956)
The official opening of the Unit followed in September 1957 (TNA: DT 33/1243, 12 Sep. 1957: 4) and the building was described as ‘modern and attractive’ (p. 12). At the request of the Hospital Management Committee (Moss and Everton, 1996: 28), the Unit was named ‘the George Schuster Hospital’, after Sir George Ernest Schuster (1881–1982), the chairman of the Oxford Regional Hospital Board from 1951 to 1963 (Moss and Everton, 1996: 42), despite his own earlier suggestion to have the new hospital named ‘Saint George’s Hospital for Nervous and Mental Diseases’ (BRO: P/HA2/1/7/2, F451 [25 Oct. 1956]). According to Wheeler (2015: 74), Schuster ‘was concerned that his own wife’s depression should be treated in a modern facility and financed this radically innovative building’.
According to the presentation of the building in the Architects’ Journal on its completion in April 1956, ‘All new patients, most of whom are voluntary, [were] admitted to the unit instead of the main 950-bed hospital, and the majority, after observation and treatment, are discharged or become out-patients. The average stay [was] about seven weeks’ (Anon., 1956: 385). In 1971, the George Schuster Hospital, with 55 beds, was re-affirmed as ‘an integral part of Fair Mile Hospital which caters for the less disturbed admissions, and to which all consultants may admit’. However, at that time, the existence of two further admissions wards in the main building – two for women and one for men – was also recorded (TNA: BN 37/34, Oct. 1971: 4). The George Schuster Hospital also accommodated ‘Fair Mile’s Winterbourne Therapeutic Community, which opened in 1967 under chief Psychiatrist Dr David Duncan’, and reflected ‘new thinking in the form of group therapy’, until 1975 (TNA: BN 37/34, Oct. 1971: 4), when the Community moved to the ‘Villa’ (Wheeler, 2015: 69). It remains unclear whether there were further changes to its use, but it may have been used as a standard ward towards the end of its lifetime (Barton Willmore Partnership Western Ltd., 2006, Appendix viii, Photograph 14/01). 4
Historical context: NHS hospital aspirations and budget restrictions
It is argued here that the commission and realization of the Admission and Treatment Unit at Fair Mile was highly exceptional and therefore of historic significance, as it took place in the period 1954–56, precisely when funding for new hospital buildings was withheld. As is widely known and well documented, following the launch of the NHS in 1948, the implementation of this major overhaul of health care provision was a massive organizational undertaking. In the field of second-tier provision, that is, at hospital level, the NHS inherited hospitals commissioned and administered under separate systems. In addition to the need to co-ordinate existing provision, there were also significant infrastructure shortcomings, both because of the age of most hospital buildings, which were in need of maintenance and modernization, and in terms of bed shortages that dictated the commission of a number of new hospitals. Specific administrative problems relating to mental health hospitals were also soon identified, as these hospitals were considered to be in the wrong places, with ‘no direct administrative relationship between local authority boundaries and those of hospital catchment areas’ (Jones, 1993: 145).
The Minister of Health at the time, Aneurin Bevan, included mental hospitals in the top priorities set for hospitals in 1950. Whether mental hospitals should be ‘included in the centralized NHS scheme, or left with the county authorities’ had been questioned during the process of planning for a National Health Service: In April 1943, the Minister of Health, Ernest Brown, ruled that the new scheme would only apply to physical illness, and that services for mental illness would be excluded; but this decision was shortlived. Mental hospitals were included in the scheme set out by the White Paper of 1944, Memorandum On The Future Organization of the Psychiatric Services, which quoted the Macmillan Commission on the interaction of mind and body. (Jones, 1993: 143–4)
5
As regards new buildings in particular, tuberculosis was given priority, but the disease was soon obsolete, and mental hospitals were second. At the time, they were still limited by law from full integration with other services (Harwood, 2015: 283). However, budget restrictions and the underestimation of costs soon complicated things even further and, notably, although health care was one of the top priorities of the state in the immediate post-war period, it came below housing and education (Powell, 2009: 85–6). Health care buildings were first put into abeyance with the outbreak of the Korean War in 1950 (Harwood, 2015: 279) and the heightened military expenditure in the shadow of the Cold War (p. xxi). Reductions in these expenses began in 1958 (p. xxviii), but there were also loan restrictions imposed in February 1957, after the Suez Crisis (p. xxv). The Admission Unit at Fair Mile clearly fell within a brief exception of limited funding for additional psychiatric facilities in 1954–5 (the ‘mental million’) provided by the then Minister of Health, Iain Macleod (Hughes, 1996: 41).
It is of special interest here that the national overview presented above is firmly confirmed in the sources available for the Oxford region. The first annual report of the Oxford Regional Hospital Board demonstrates that, within the first year of its life, by 31 March 1949, the ‘immensity of the problems with which the Board will be faced in the next few years’ had been made clear, as ‘the emphasis seems to have shifted from scarcity of materials to scarcity of money’ (Oxfordshire History Centre [OHC]: ORHB, 1949: 5). In the same report, the Board also recognizes that there are many ways in which hospital services can be improved by more efficient organization before one proceeds to modifications, reconstruction or new developments. However, it also points out the significant weight of ‘war-time arrears’, and stresses vigorously that major developments ‘unfortunately, seem likely to have to be deferred for an unpredictable period of time’ (p. 5).
In their year-by-year history, Moss and Everton (1996) reflect in detail on the impact of money shortages, and also give an outline of the time it took to actually implement all key changes adopted in the early 1960s. ‘Money worries’ are recorded from the turn of the 1950s (pp. 15–16), and by 1952 it is noted that ‘financial pressures start to bite’, just as there is also ‘warning of severe overcrowding problems in mental hospitals’ (p. 17). The following year, 1953, long before the 1960s major shift in policy, rather than receiving additional support, mental hospitals ‘were singled out by the Minister of Health for a moratorium on further new builds (p. 19). Remarkably, though, as discussed above, the commission of the new Admission and Treatment Unit at Fair Mile was reported in 1954 and the building was completed by April 1956.
The ‘medical’ model of care
In addition to its timing in relation to the launch of the NHS and its new hospital building programme, the particular use of the Admission and Treatment Unit is also of special significance. It marks key developments in mental health care during the first half of the twentieth century leading to the landmark shift in legislation and policy that was to be fully validated by the Mental Health Act of 1959. A brief overview of the significance and historical context of the so-called ‘medical’ model of care is therefore discussed here, followed by a discussion of the origins of Admission Units and the concept of medical ‘treatment’ in the final section below.
One key indication of the ‘medical’ model has been the change of terminology associated with mental health, that is, the adoption of ‘medical’ language. Within architectural scholarship, for example, the RCHME survey that includes asylums in a study of hospitals clearly reflects a twentieth-century perspective (Richardson, 1998). Both asylums and earlier institutions, as well as their subsequent reincarnations as mental hospitals, clinics and other variations, are all placed under the umbrella topic of hospital architecture, rather than as a separate kind of institution that aimed more at confinement rather than treatment. Conversely, only seven years earlier, Jeremy Taylor’s (1991) study includes ‘Hospital and Asylum’ in the title of his book covering the period 1840–1914. Nonetheless, with the discussion below in mind, we can still accept the inclusion of asylums in a study of hospitals such as that by the RCHME as a valid exercise that serves well its principal purpose as a survey of realized buildings.
Several studies have repeatedly demonstrated that early asylum planning was closer to that of prisons, as supervision was a primary concern (Richardson, 1998: 3–4, 161, 163), and the association with ‘medicine’ can be questioned as regards its actual meaning and its exact timing. Jones (1993), in her seminal study Asylums and After: A Revised History of the Mental Health Services from the Early 18th Century to the 1990s, traces the key moments at which ‘mental illness’ was associated with ‘medicine’. As she points out, as early as the second half of the eighteenth century, ‘medical men began to experiment with more humane methods of care and treatment, and hospitals were set up in some cities by public subscription’, yet treatments were effectively ‘standard remedies of bleeding, purging, blistering and vomits’ that were soon to be side-lined by the emphasis on ‘moral treatment’, as introduced at The Retreat at York’ (p. 23). Jones also points to Andrew Scull’s scholarship for further arguments against the actual medicalization of mental illness in the early nineteenth century. She explains how Scull has argued that insanity did not ‘come to be defined as illness’ but, when faith in exorcism was being lost, the methods of medical practitioners continued to carry credibility, even though ‘the early asylum doctors were not primarily “medical men”.’ (Scull, 1979: 14–16, as cited in Jones, 1993: 38–9). Nonetheless, records at Fair Mile show that ‘30–40% of those admitted between 1870 and 1875 were discharged recovered, usually within a year’ (BRO: D/H10/Admin. Hist.). Yet, as discussed below, with the special committee for the LCC set up in 1889 and the Maudsley Hospital opened in the 1920s, the tangible shift in the built environment for the medical treatment of mental illness in England, as expressed by the introduction of Admission and Treatment Units, only materialized at Fair Mile as late as the mid-1950s (Taylor, 1991: 153).
Overall, several milestones can be identified in the transition to the ‘medical model’ – as opposed to earlier models based on ‘custodialism’ or ‘legalism’ (Jones, 1993: ch. 6). For instance, as early as the second quarter of the nineteenth century, medical publications on insanity appeared which started marking ‘the asylum doctors’ move from orthodox medicine into a new field of study’ (pp. 68–9). In addition, the advocacy of the interaction between mental and physical illness by the Macmillan Commission of 1924–26 was very widely accepted and was also reflected in a medical terminology being officially adopted: ‘hospital’, ‘nurse’, ‘patient’ and so on (pp. 130–1). This medicalization was further reinforced by the discovery of the psychotropic drugs (p. 149), as well as the development of a range of physical treatments for mental illness, and the relocation of psychiatric wards within general hospitals, as affirmed by the Mental Health Act of 1959 (p. 156).
Origins and significance of admission units: ‘medical’ treatment and voluntary admissions
The need for an Admission and Treatment Unit falls firmly within the above model of care. Specifically, the lack of an Admission Unit at Fair Mile (then Berkshire County Mental Hospital) was flagged up within weeks of the official launch of the NHS. On 23 July 1948, it is recorded in the Visitors’ Committee book that ‘the treatment of early cases is impeded by the lack of an admission hospital and convalescent villas’ (BRO: D/H10/A2/2, 23 July 1948: 24). A similar opinion is repeated three years later (BRO: D/H10/A2/2, 28 June 1951: 59), as well as special mention in 1952 of the lack of a ‘proper treatment centre’: This Hospital has no admission unit or convalescent villas as such; nor has it any proper treatment centre. We hope that financial restrictions will not in the long run stand in the way of providing these types of buildings which are essential to a Mental Hospital of this size. (BRO: D/H10/A2/2, 17 July 1952: 68)
Reviewing earlier Commissioners’ inspection reports, Wheeler identifies the need for ‘dedicated admission wards’ from ‘after about 1920’, and further points out that ‘by 1938, there was still no admissions hospital “to bring the hospital into line with modern requirements”, the infirmary wards being used instead’ (Wheeler, 2015: 28).
The 1920s date coincides with the emphasis on early treatment and voluntary admissions as best represented by the Maudsley Hospital and the Mental Treatment Act 1930. The former was initiated by Henry Maudsley who, from 1907, sought to create a new type of specialist mental hospital that was to focus on the early treatment of cases of acute mental disorder. Administrative delays and World War I caused a series of postponements, and the hospital was finally opened in 1923 (Richardson, 1998: 180). The Mental Treatment Act 1930 ‘radically altered admission procedures to mental hospitals’, and for the first time patients could be admitted voluntarily (BRO: D/H10/Admin. Hist.). Although further research is required to establish when the first admission units appeared, several new units appeared in the 1920s and 1930s and a few new admission blocks and wings are recorded in the architectural press until the early 1940s (Anon., 1940, 1942, 1943). 6
In his major study Hospital and Asylum Architecture in England 1840–1914, Jeremy Taylor discusses the appointment of a committee ‘to consider the controversial proposal for an acute hospital for curable patients’ in 1889, following the formation of the LCC (Taylor, 1991: 153). This proposal was ‘a first general use of the title “mental hospital”’, but – ‘deferred to widespread opposition by asylum medical superintendents’ – did not happen in the end (p. 153, n. 604, citing Poynter, 1964: 140). Maudsley Hospital is considered to have been the first actual realization of this major shift towards ‘medical’ treatment for mental illness, but the earlier arguments and evidence had already made that case as they put emphasis on the special treatment of insanity. Specific shortcomings identified included ‘sufficient means of isolation and classification for different classes of case, e.g. separate acute, short-stay or admission accommodation’. As a result, the suggested improvements included ‘an increasing provision of separate “acute” hospital buildings on asylum sites’ (Taylor, 1991: 153).
By the 1950s, when the new Admission and Treatment Unit was commissioned and built, further developments in the field of mental health were also mandating change in the required facilities. ‘Physical therapies’ for mental illness, such as deep insulin therapy and electro-convulsive therapy, had been developed and were already in use at Fair Mile. By 1951, records report that ‘in addition to in-patient treatment an average of 800 out-patients are treated with electro-convulsive therapy annually’ (TNA: DT 33/1243, 8 Mar. 1951: 4), and by 1954, there is also ‘Insulin Coma Therapy now in use for male and female patients’ (TNA: DT 33/1243, 8 July 1954: 5).
‘Into the Light’ (1959)
A recruitment pamphlet describing Fair Mile Hospital and the training and job prospects available there for nurses was published in February 1959 (BRO: P/HA2/5/1 Fair Mile Hospital, ‘Into the Light’). 7 Writing while the ‘forthcoming legislation contained in the Mental Health Bill’ was before Parliament, H.R. Lambert, Chairman of the St. Birinus Group Hospital Management Committee, noted in his Foreword the optimism of a ‘changed outlook on mental illness and mental deficiency’ (p. 2). He also specifically stressed ‘the pleasant countryside of Berkshire or South Oxfordshire within easy access of Oxford, Reading and London’ as well as the major redevelopment programmes in the two main hospitals in the Group (Fair Mile and Borocourt), which he described as progressive. By the completion of the programmes, he argued, ‘both hospitals should typify all that is best in modern psychiatric treatment in accordance with the latest developments in the rehabilitation of our patients’ (p. 2).
In the main body of the pamphlet, the ‘modern Admission Unit, which is separate from the main hospital,’ (p. 3) is specifically listed as an example of the development programmes taking place in the two hospitals, and there are also details of the care provided. This included ‘all modern types of treatment for mental illness’, such as deep insulin and convulsive therapy, as well as the use of ‘new drugs’. The emphasis on rehabilitation by means of ‘occupation and resocialization, particularly in the form of group activity’ is also noted, as well as plans to enlarge the occupational and rehabilitation departments, thus stressing the alignment with ‘current legislation and changing social patterns’ (p. 3).
Conclusion
The Mental Health Act of 1959 is considered to have complemented the National Health Service Act of 1946 and brought about a legislative revolution, which in its turn also started clinical and administrative revolutions. As this new piece of legislation passed on responsibility for community care to the local authorities, it effectively led to the closure of large residential institutions, especially those in rural locations. Psychiatric wings within general hospitals became the main approach for second-tier psychiatric care, further complemented by day hospitals and supported hostels.
This shift to ‘care in the community’, which was widely implemented from the 1960s onwards, also introduced yet another transition – towards the ‘psychosocial’ model of care. This new transition followed international expert reports from the late 1950s that focused on the ‘psychosocial environment’ and stressed ‘the need to relate psychiatry more closely to the community’ (World Health Organization [WHO], 1959, as cited in WHO, 1962: 10). To an extent, this has been an apparent reversal of the process that, especially in the course of the nineteenth century, had ‘destabilized the traditional forms of welfare provided by family networks, charity organizations, feudal ties, guilds, municipalities and religious institutions’ and gradually led to ‘institutional initiatives . . . at local, regional and national levels’ (Swenarton et al., 2015: 7); and its interesting parallels to pre-institutionalized practices in numerous parts of the world have often been commented upon (e.g. Bartlett and Wright, 1999; Mueller, 2007). Although an in-depth analysis of this model is beyond the scope of the present article, it is of special significance here: not only did this further shift have a key impact on the actual management of related built environment and future commissions (or their absence), but it also resulted in the significant gap in relevant historiography, as identified above.
By pointing out the historic significance of the Powell and Moya building at Fair Mile and by identifying this wider gap in existing scholarship, the present study highlights the pioneering work of the Oxford Regional Hospital Board. Moreover, it also aims to be the first part of a broader project on mental health facilities during that period. The broader project aims to identify further characteristics that relate to local or national approaches – especially given the fact that several purpose-built Admission Units had been newly commissioned and built shortly after the launch of the NHS – and also to compare these to inter-war Admission Units.
Finally, the turn of the twenty-first century has seen a number of in-patient facilities that are separate from hospitals remaining a key part of mental health care provision in the UK, either in purpose-built or in converted buildings (Turner et al, 2015). The question of good mental health and care provision for mental illness features regularly in the general press and other media (BBC News, 2019; Campbell, 2017), and the question of ‘beds’ – as in-patient provision is colloquially referred to – remains topical (Doward, 2018; Gilburt, 2015). What is more, several purpose-built Acute Mental Health Units have been commissioned and built in recent decades and, despite marked differences in their typological development, their scale and programme also bear some notable similarities to early NHS Admission Units. Considering the above, the research in those early NHS mental health facilities remains topical.
Footnotes
Funding
The author(s) received no financial support from any funding agency in the public, commercial or not-for-profit sectors for the research, authorship and/or publication of this article.