
Abstract
This article investigates the content and the consequences of the prototypes of people with depression in a multimethod fashion. Fourteen preregistered studies (total N = 5,023, with U.S. American, British, and French adult participants) show that laypeople consider people with depression as having specific psychological, social, and physical features (e.g., unattractive, overweight, unsuccessful, introverted). Target prototypicality influences how much laypeople believe others have depression, how much observers believe that depression-like symptoms cause someone to experience psychological pain, and how much professional mental health care is appropriate for others. This effect was not reduced by instructing people to focus on the symptoms and ignore the target features yet was weakly reduced by informing them of the effect. We discuss theoretical implications for the understanding of prototypes of people with depression and practical implications for alleviating the impact of prototypes.
More than 264 million people are estimated to suffer from major depressive disorder (MDD; James et al., 2018), and depression is projected to be the leading cause of global disease burden by 2030 (World Health Assembly, 2013). Although there are effective treatments for depression (Muñoz et al., 2010), many people with depression remain undiagnosed or untreated (Wang et al., 2007). Laypeople hold various negative attitudes about people with depression (Angermeyer & Matschinger, 2003), and in turn they fail to properly recognize people with depression (Jorm et al., 2005), resulting in underdiagnoses by mental health professionals (Sheehan, 2004; Williams et al., 2017).
In this article, we first elicited laypeople’s multifaceted prototypes of people with depression, including physical, psychological, and social features. Next, we examined whether a person who does not fit the person-with-depression prototype is less likely to be considered to have depression, feel psychological pain, and be recommended psychological treatment even when showing the clinical symptoms of depression. Further, we explored ways to reduce people’s reliance on prototypes.
Category-Specific Prototypes
People have very specific notions about how certain categories of people are and should be. These prototypes have consequences. People believe that veterans are more hands-on and less emotionally competent than nonveterans, and therefore recruiters recommend them to hands-on jobs (Shepherd et al., 2019). Nonprofit organizations’ employees are considered to be more moral than for-profit organizations’ employees and are therefore punished more harshly after a moral violation (Stiegert et al., 2021). Medical doctors are considered less able to feel negative feelings than the average worker, and therefore people believe that doctors are better able than most to ignore physical and mental issues (Goranson et al., 2020).
Clinical psychologists and opinion researchers have long been interested in what the public thinks about people with mental illness, particularly people with depression (Cox et al., 2012; Link et al., 1999; Star, 1955). Most of this research, however, investigated how laypeople (Byrne, 2000; Corrigan & Kleinlein, 2006; Lauber, 2008; Link et al., 1999; Link & Phelan, 2001; Norman et al., 2008; Rüsch et al., 2005) and professionals (Lauber et al., 2006; Nordt et al., 2006) stigmatize people with mental illness, with the objective of reducing stigmatization to improve access to care and integration of people with mental illness into society (Byrne, 2000). This research focused on observers’ reactions to someone they believed as having depression (Lauber, 2008) or on the schemas that people with depression have of themselves (Beck, 1967; Cox et al., 2012) but neglected to investigate the content of the prototype of people with depression. This includes lay beliefs about what people with depression look like and how they behave, including a variety of psychological, social, and physical features. The present investigation aims to fill this gap in the literature.
Potential Contents of Stereotypes of People With Depression
When clinicians make diagnoses for depression, they use an established set of criteria (e.g., those described in the Diagnostic and Statistical Manual of Mental Disorders–5 [DSM-5; American Psychological Association, 2013] or the International Classification of Diseases 11th Revision [ICD-11; World Health Organization, 2022]). When using these criteria, they evaluate whether individuals experience a certain number of symptoms for a prolonged period and whether these symptoms also cause distress and/or impairment in social and psychological functioning. However, when laypeople categorize someone as having depression, they might use much less complex information. We aim to understand what information laypeople use to recognize someone as having depression.
Most stereotypes about people with depression are negative, including being needy, dependent, helpless, and unpredictable but also being strange, aggressive, and dangerous (Angermeyer & Matschinger, 2003). On the one hand, negative stereotypes about people with depression are thought to come from the media, where inaccurate and inappropriate views of people with depression are widespread (Goepfert et al., 2019). For instance, research shows that the news media implies that people with depression were responsible for their condition (Zhang et al., 2016). On the other hand, 97% of the symptoms about depression in Australian media items mentioned in relation to depression were accurate (Francis et al., 2005), which might be due to the increasing levels of mental health literacy campaigns (Jorm et al., 2005).
Statement of Relevance
How do people imagine people with depression, and does this affect how laypeople understand depression symptoms? We asked U.S. American, British, and French adult participants and found that they had a multifaceted prototype of people with depression. Laypeople imagined people with depression with specific physical, social, and psychological features (unattractive, overweight, unsuccessful, introverted). People thought that if someone did not fit the prototype, the same symptoms (e.g., lack of sleep, continuous sad mood) were less indicative of depression, that they would experience less psychological pain, and that mental health care would be less appropriate for them. It was hard to correct these perceptions, and interventions yielded only small reductions of the effects of prototypes. These findings are important to show what people believe a people with depression should look like and how they would behave when someone who does not fit the prototype of the person with depression shows potential depression symptoms.
Recognizing Depression and Its Consequences
Laypeople (especially close others, like partners, family, or friends) often recommend others to seek treatment for depression (Jorm et al., 2005; Link et al., 1999). Laypeople may not consider someone to have depression despite the presence of symptoms because this person may not fit the person-with-depression prototype. Then, it might be more likely that the person with depression will not seek treatment. Further, observers may minimize symptoms among people with depression, which might compound their suffering (Ormel et al., 1991). It is unclear what information people use to recognize depression (but see N. S. Kim and Ahn, 2002) and whether they rely on prototypes of people with depression or the clinical symptoms. This article aims to fill this gap as well.
When people’s features do not conform to a certain prototype, observers are less likely to judge what is happening as a prototype-linked behavior. For instance, because people believe that the prototypical woman victim of sexual harassment is conventionally feminine, they are less likely to categorize ambiguous behaviour as sexual harassment when directed to a less feminine woman (Goh et al., 2021). Similarly, if people do not believe that someone fits their prototype of a person with depression, they might be less likely to interpret the same symptoms as indicative of depression. This may also lead them to discount the target’s suffering and to be less likely to recommend mental health care as a solution to the symptoms. Therefore, another goal of this article is to test the effect of prototypicality on the classification of a person as having depression.
Some researchers argue that when diagnosing depression, it makes sense to consider information that is not strictly included in diagnostic instruments. This is because diagnoses and diagnostic instruments are varied and unreliable (Fried et al., 2022) and should not be blindly relied on, lest we fall into “diagnostic realism” (i.e., mistaking diagnoses for syndromes) (Kendler, 2016; Kendler et al., 2011). Further, because mental illnesses are biopsychosocial diseases, researchers have argued that to diagnose someone with MDD, mental health care professionals should take into account a larger variety of patients’ features and not just the symptoms described in diagnostic manuals such as the DSM-5 or the ICD-11 (Fried, 2022). Without taking a position on the cues that should be taken into account when diagnosing depression, the present investigation can help this debate by cataloging some of the features that make laypeople more likely to classify someone as having depression.
Finally, can the effect of prototypes be reduced? For instance, making people aware of the importance of depression prototypes on classification of a person as having depression might reduce their overreliance on personal features. In addition, explicitly instructing people to ignore personal features and focus on the symptoms alone may also moderate the effect of depression prototypes on classification as depression (a similar method was used to reduce people’s reliance on extraneous cues in Dietvorst & Simonsohn, 2018, and in Ziano & Wang, 2021). We also test these ideas.
Study Overview
We conducted 14 studies with British, U.S. American, and French participants (total N = 5,023; summarized in Table 1; we present Study 1a to Study 3 fully in the article). Studies 1a, 1b, 1c, and S1 to S7 investigated the social, psychological, and physical features that lay observers believe people with depression have. Study 2 and Study S8 tested whether target features influence the recognition of depression, the amount of perceived psychological pain, and the perceived appropriateness of mental health care. Study 3 and Study S9 tested whether receiving information about the effect of stereotypes or instructing participants to focus on the symptoms (and ignore targets’ features) can decrease the influence of prototypicality on recognition of depression, the amount of perceived psychological pain, and the perceived appropriateness of mental health care.
Overview of the Studies in the Present Article
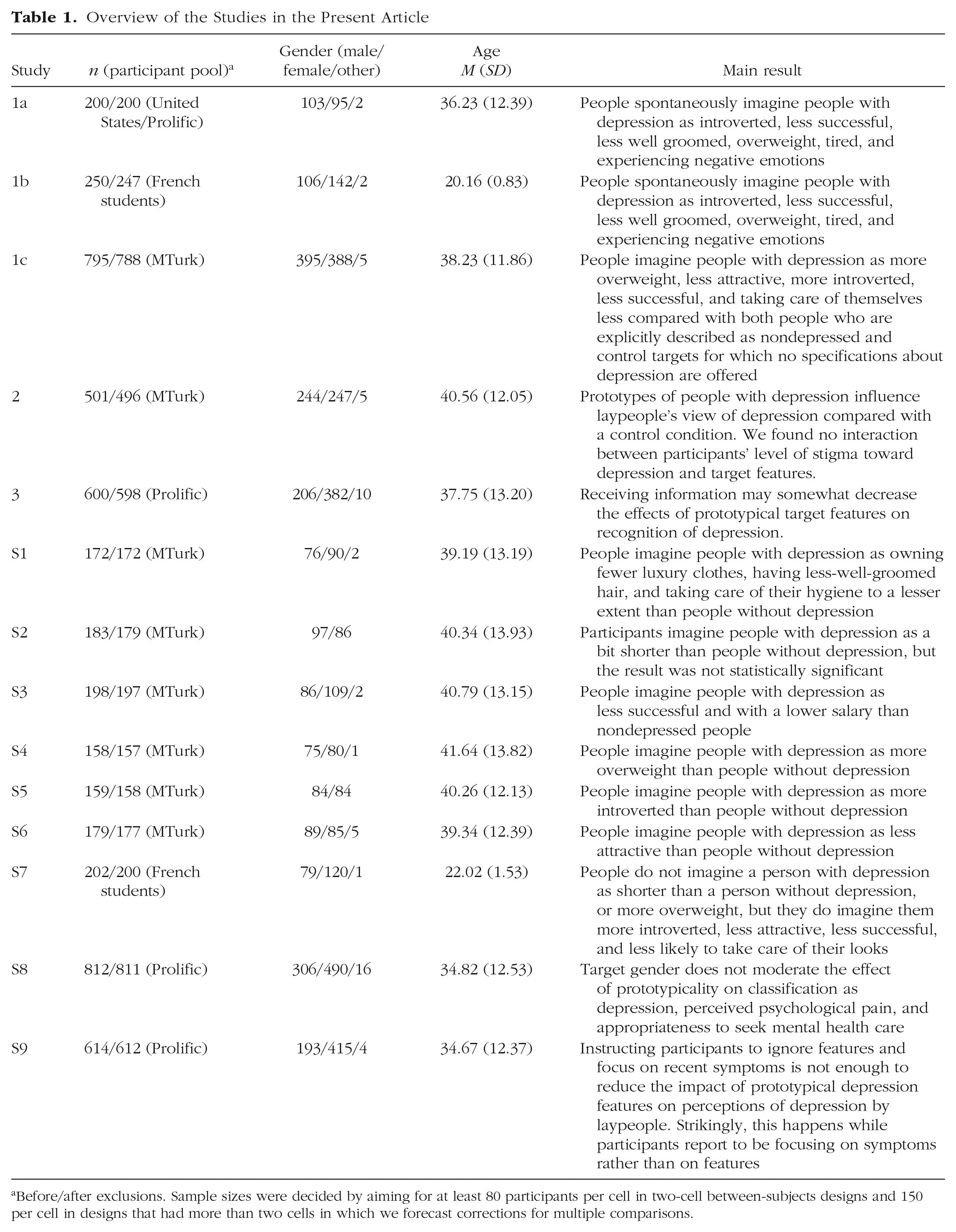
Before/after exclusions. Sample sizes were decided by aiming for at least 80 participants per cell in two-cell between-subjects designs and 150 per cell in designs that had more than two cells in which we forecast corrections for multiple comparisons.
Studies 1a and 1b: Eliciting Qualitative Prototypes of People With Depression
Method
In Study 1a, we asked participants to write down two physical, two social, and two psychological features of people with depression (six total features). In Study 1b, we asked participants to write down three features instead of two per the same categories.
Results and discussion
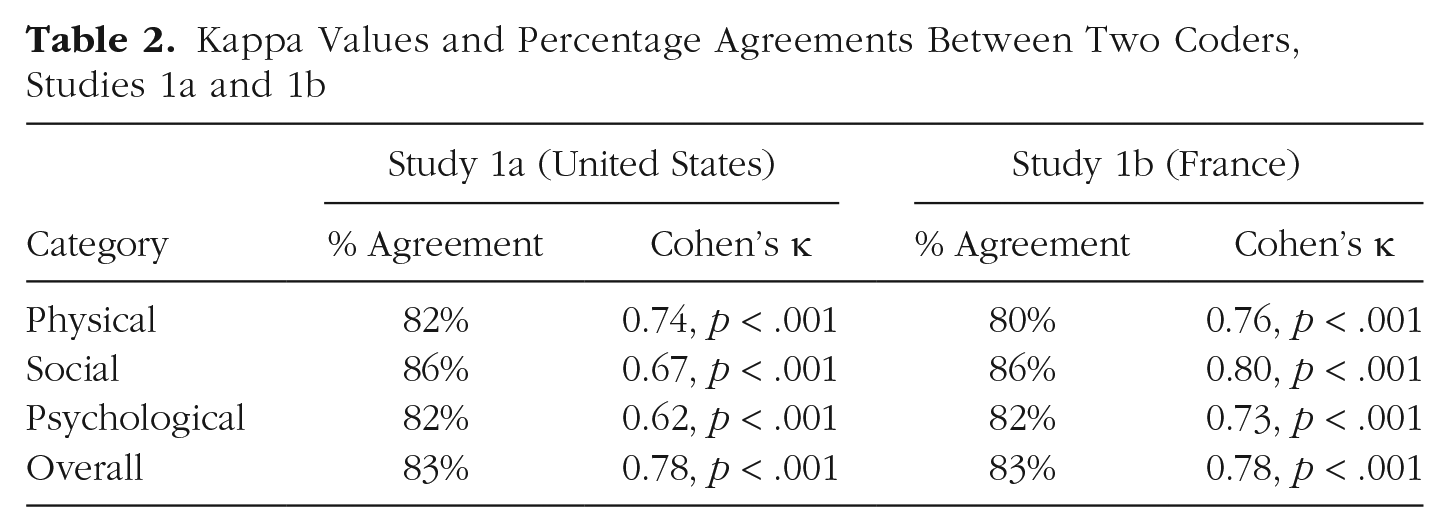
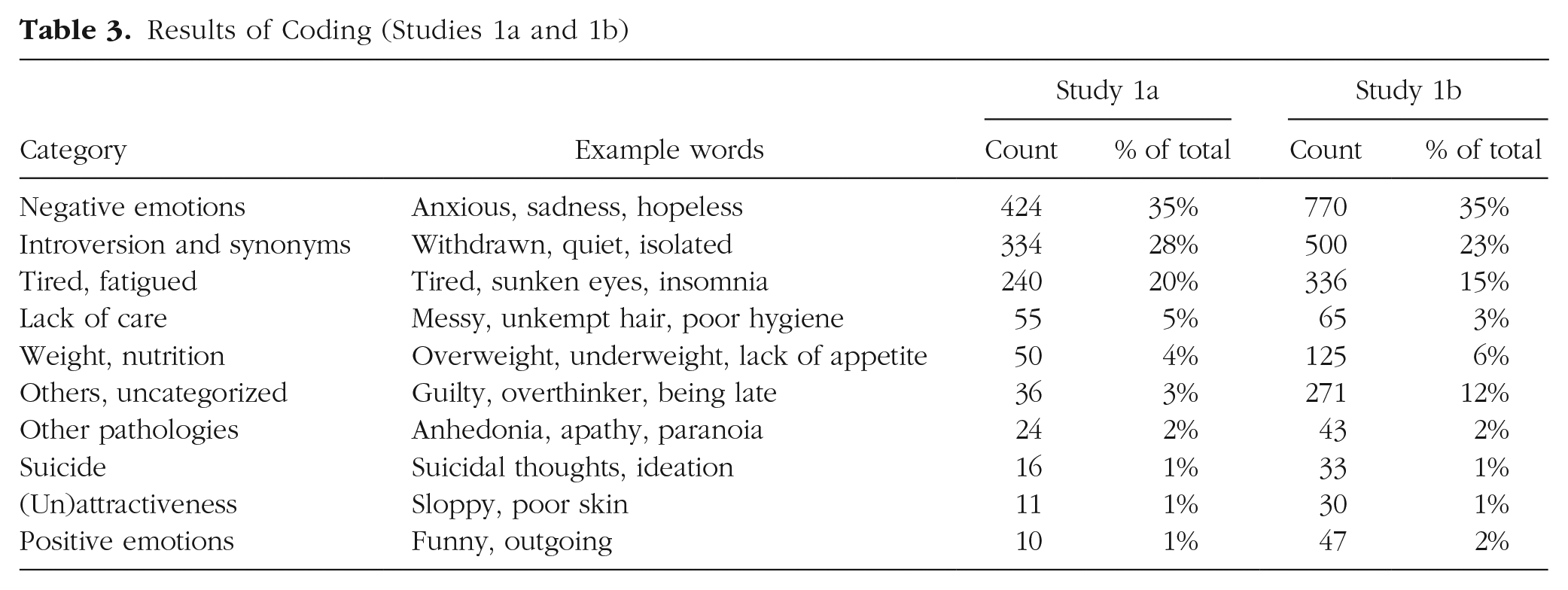
The data resulted in 1,200 entries in Study 1a and 2,223 in Study 1b. In Study 1b, some participants completed the entries in French. A bilingual author translated them to English before they were coded by the coders. There were three steps in the coding procedure. First, both authors went through the data and inductively proposed categories. Next, two independent coders, blind to the aim of the study, used the generated categories to separately code the data. Using this coding, we calculated the Kappa scores for each target feature category (i.e., physical, social, psychological) and altogether. All Kappa scores showed high agreement across the two coders (see Table 2). Finally, the coders discussed and agreed on a final coding for the disagreements. Results from the final coding are summarized in Table 3 along with the most frequent few words in each category. Word clouds based on the results are presented in Figures 1 and 2. This establishes the content of prototypes of people with depression across two different samples in two countries, at a qualitative level. In the next studies, we explore it in a quantitative fashion.
Kappa Values and Percentage Agreements Between Two Coders, Studies 1a and 1b
Results of Coding (Studies 1a and 1b)

Word cloud of responses (Study 1a).
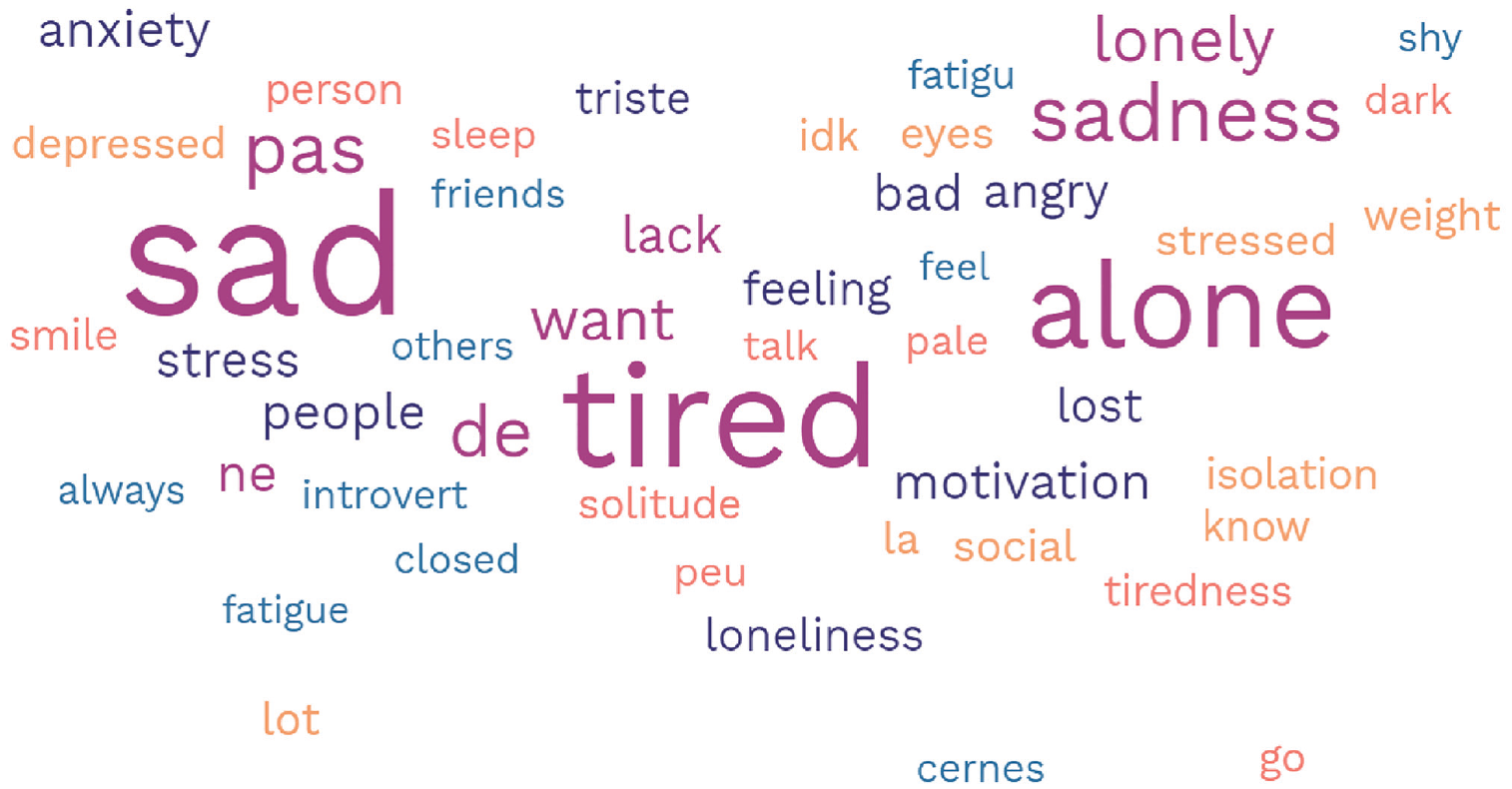
Word cloud of responses (Study 1b).
Study 1c: Eliciting Prototypes of People With Depression in a Quantitative Fashion
The objective of this study was to elicit prototypes of people with depression and compare them with imagined features of people explicitly described as without depression and with a control condition where no depression symptoms are specified. Unlike Studies 1a and 1b, in Study 1c we added the trait “successful” because we believed it was interesting and relevant for life in organizations and omitted traits relative to the negative psychological state (e.g., anxious, sad) of the person because we believed that they were confounded with the symptoms presented in the ICD-11 or DSM-5 classification.
Method
Participants were randomly assigned to one of six conditions in a 3 (symptoms: depressed vs. not depressed vs. no information) × 2 (target gender: male vs. female) fully between-subjects design. First, participants were assigned to either the male or the female target condition. In the male condition, they read the following scenario: Jonathan Smith is a bank clerk at LMS, a bank in New Orleans, Louisiana. He is originally from Houston, Texas. Jonathan is 38, has an associate degree in management, and is Caucasian.
In the female condition, the name and the pronoun were changed to female: Jessica Smith is a bank clerk at LMS, a bank in New Orleans, Louisiana. She is originally from Houston, Texas. Jessica is 38, has an associate degree in management, and is Caucasian.
Then, participants were assigned to either the depressed condition, the nondepressed condition, or the no-information condition. Participants in the no-information condition proceeded to the next part of the survey (i.e., the measures) without reading any additional text.
Participants in the depressed condition read the following: This person is clinically depressed. They often have insomnia and are in a state of a really bad mood.
Participants in the nondepressed condition read the following: This person is not depressed. They have their up and downs like everyone but are overall quite OK psychologically speaking.
Measures
Then, participants replied to six questions in random order. To test what the physical features of the prototype, we asked, “Do you think this person is overweight?” and “Do you think this person has an attractive face?” To test the psychological features of the prototype, we asked, “Do you think this person takes care of themselves?” and “Do you think this person is introverted or extroverted?” To elicit a social dimension of the prototype, we asked, “Do you think this person is successful at work?” As a manipulation check, we asked, “Do you think this person is clinically depressed?” All questions were anchored at 1 (not at all) and 7 (very much), except for the introversion question, which was anchored at 1 (very introverted) and 7 (very extroverted).
Results
We did not find any interaction between symptoms and target gender for any dependent variable. Here and in all studies where we performed analyses of variance (ANOVAs), we report Tukey-corrected pairwise comparisons. Full statistical analyses are available on OSF. These results are depicted in Figure 3.
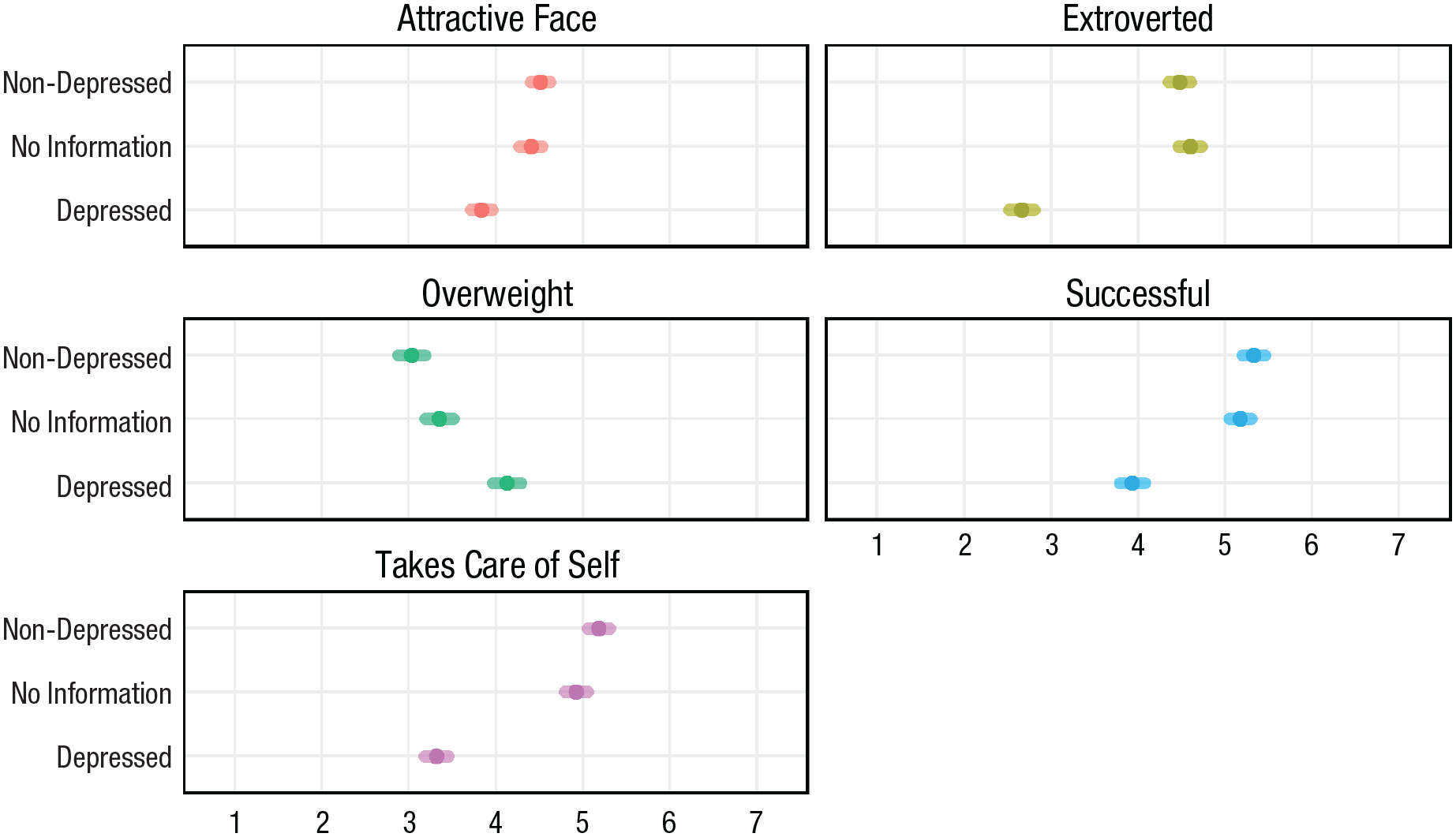
Imagined features of people with depression (vs. targets explicitly described as without depression and without information about their mental state), Study 1c. Means and 95% confidence intervals are depicted.
Overweight
Participants imagined the depressed target (M = 4.13, SD = 1.40) as more likely to be overweight than the nondepressed one (M = 3.03, SD = 1.26), t(782) = 9.41, p < .001, d = 0.82, and compared with the no-information condition (M = 3.35, SD = 1.34), t(782) = 6.67, p < .001, d = 0.58.
Care
Participants considered the depressed target (M = 3.32, SD = 1.16) as less likely to take care of themselves compared with the nondepressed target (M = 5.18, SD = 1.05), t(782) = 19.21, p < .001, d = 1.67, and compared with the no-information condition (M = 4.92, SD = 1.12), t(782) = 16.61, p < .001, d = 1.44.
Successful
Participants imagined the depressed target (M = 3.93, SD = 1.20) as less likely to be successful compared with both the nondepressed target (M = 5.33, SD = 1.08), t(782) = 14.46, p < .001, d = 1.26, and the no-information condition (M = 5.17, SD = 1.03), t(782) = 12.94, p < .001, d = 1.13.
Attractive face
Participants imagined the depressed target (M = 3.84, SD = 1.07) as less attractive than the nondepressed target (M = 4.51, SD = 0.96), t(782) = 7.61, p < .001, d = 0.66, and less attractive than in the no-information condition (M = 4.40, SD = 1.10), t(782) = 6.26, p < .001, d = 0.54.
Introversion
Participants imagined the depressed target as more introverted (M = 2.65, SD = 1.24), t(782) = 18.28, p < .001, d = 1.59, compared with the nondepressed target (M = 4.47, SD = 1.08) and the no-information condition (M = 4.60, SD = 1.10), t(782) = 19.54, p < .001, d = 1.70.
Depressed (manipulation check)
Participants imagined the depressed target (M = 6.27, SD = 1.02) as more likely to be depressed compared with the nondepressed target (M = 1.60, SD = 1.01), t(782) = 48.12, p < .001, d = 4.19, and with the no-information condition (M = 2.66, SD = 1.31), t(782) = 37.18, p < .001, d = 3.23. Participants imagined the targets in the no-information condition as less likely to be depressed compared with the depressed condition, t(782) = 10.86, p < .001, d = 0.96.
This study shows that people imagine people with depression as more overweight, less attractive, more introverted, less successful, and taking care of themselves less compared with both people who are explicitly described as nondepressed and control targets for which no specifications about depression are offered. The nondepressed and the no-information conditions were quite similar to each other across dependent variables.
Studies S1 to S7: Extending and Testing the Robustness of the Prototype Across Features, Study Designs, and Populations
Results
It is important to test the generalizability of these results to different scenarios (different jobs, age, names) and participants from different countries. For this, we conducted Studies S1 to S7. Full details are available at https://osf.io/2f8yn/?view_only=8ac1f586d72f4a33af6ff84a5c44227b.
Studies S1 to S6 had a between-subjects design with two conditions, and participants read a short description of a person followed by the information either that they were diagnosed with depression or that their mental health was fine. Study S1 shows that U.S. American participants imagined a depressed welder as owning fewer luxury clothes than a nondepressed one (p = .012, d = 0.39), paying less attention to their dress choices (p < .001, d = 0.99), having less-well-groomed hair (p < .001, d = 1.04), and taking care of their hygiene to a lesser extent (p < .001, d = 1.57). Study S2 shows that participants imagined people with depression as a bit shorter than people without depression, but this result did not reach conventional statistical significance (p = .08, d = 0.26). Study S3 shows that participants imagined a banking clerk as less successful (p < .001, d = 0.96) and with a lower salary (p < .001, d = 0.43) when he was described as depressed compared with when he was described as nondepressed. Study S4 shows that a clerical employee was imagined as more overweight when she was described as depressed compared with when she was described as nondepressed (p < .001, d = 0.87). Study S5 shows that participants believe that a depressed nurse was much more introverted than a nondepressed one (p < .001, d = 2.43). Study S6 shows that people imagine a person with depression with a less attractive face than a person without depression (p = .02, d = 0.35). Study S7 (with French participants) employed a within-subjects design presenting two people as either depressed or not depressed, and it showed that participants did not imagine a person with depression as shorter than a nondepressed one (p = .06, d = 0.13) or more overweight (p = .16, d = 0.10), but they imagined them to be more introverted (p < .001, d = 0.81), less attractive (p < .001, d = 0.60), less successful (p < .001, d = 0.99), and less likely to take care of their looks (p < .001, d = 0.84). Table 4 shows descriptive statistics of these studies. The objective of the next study is to test the impact of prototypes of people with depression on how observers interpret clinical symptoms of depression.
Results of Studies S1 to S7
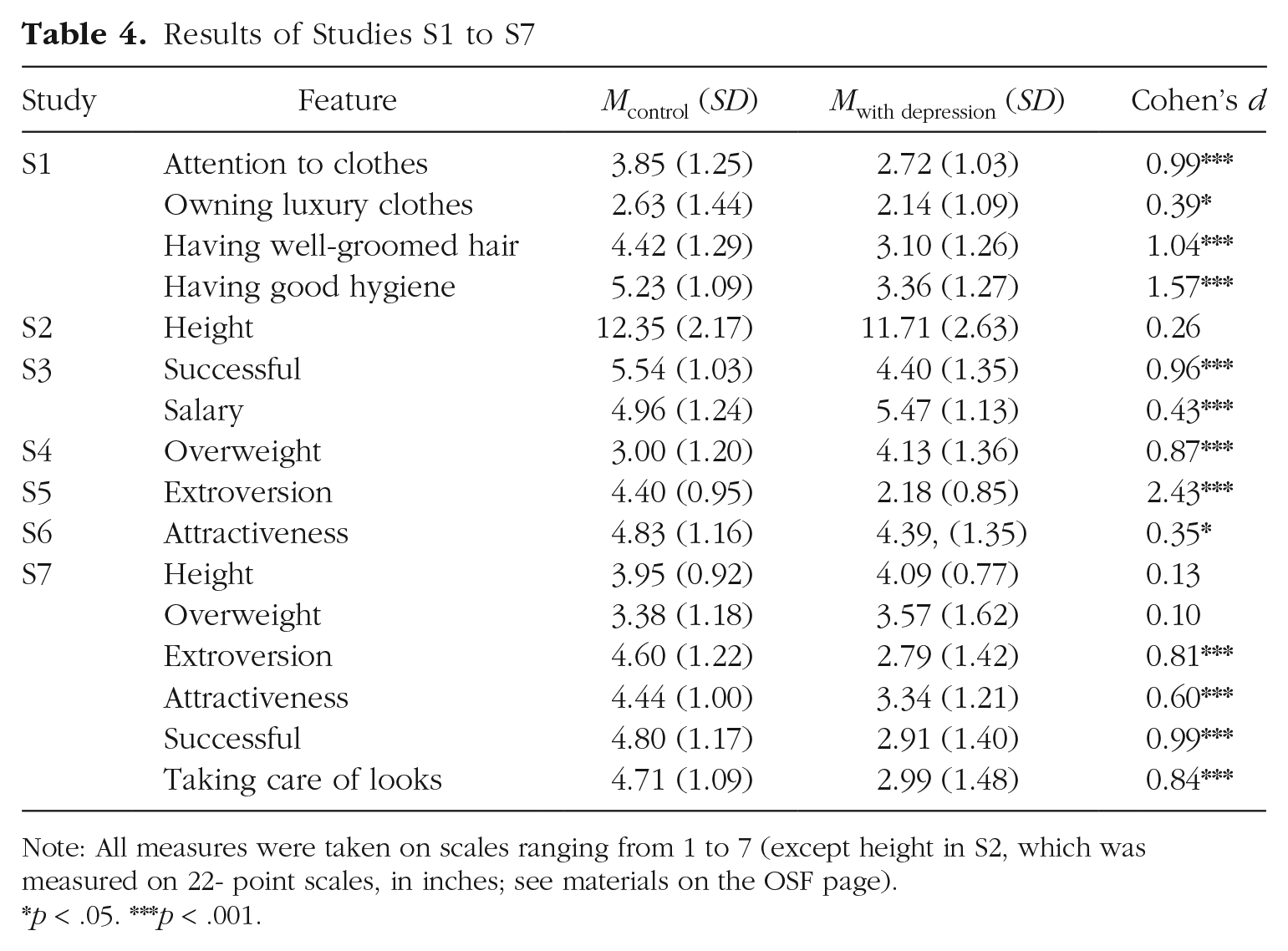
Note: All measures were taken on scales ranging from 1 to 7 (except height in S2, which was measured on 22- point scales, in inches; see materials on the OSF page).
p < .05. ***p < .001.
Study 2: The Effect of Prototypicality on Classification as Depression, Perceived Psychological Pain, and Recommendations to Seek Mental Health Care
Method
The goal of this study was to test whether prototypical target features influence the recognition of depression, the amount of perceived psychological pain, and the perceived appropriateness of mental health care when depression symptoms are kept constant across the conditions. Moreover, we tested the potential moderating role of mental health stigma.
Participants were randomly assigned to one of three conditions (between subjects): control, prototypical, counterprototypical. All participants read this introduction: Below, a woman who is 41 years old and lives in the Los Angeles area is described. This person’s initials are S.K., and she works at a social media company.
Only participants in the prototypically depressed condition then read the following description: S.K. is not successful in her job, does not take care of her looks, is quite overweight, is physically unattractive, and is quite introverted.
Participants in the counterprototypically depressed condition read the following instead: S.K. is successful in her job, takes care of her looks, is in good physical shape, is physically attractive, and is quite extroverted.
Participants in the control condition were not given any information about S.K.’s features and read only about S.K.’s recent symptoms, taken from the ICD-11 (World Health Organization, 2022), as did all the participants in the prototypical and counterprototypical conditions as well: For the past 4 weeks or so, this person has felt quite sadder than normal and could not get to sleep as well as they would have in the past.
Measures
After reading the scenario, participants completed three outcome variables, anchored at 1 (not at all) and 7 (very much): “How much psychological pain do you think this episode caused to this person?” as a measure of perceived psychological pain caused by the episode (we focused on psychological pain because we believed that recognizing pain in others might be the first step to recognizing whether they are depressed and further to recommending them mental health care); “Do you think this person is clinically depressed?” as a measure of classification as depression; and “Do you think this person should seek professional help for mental health?” as a measure of the appropriateness of seeking professional mental health help. Either before or after reading the scenario (we randomized the order), participants completed a short version of the Personal subscale of the Depression Stigma Scale (Griffiths et al., 2004) on seven 5-point Likert items. This scale showed good reliability (Cronbach’s α = .82), and we averaged it in a stigma scale index to test its potential moderating effect.
Results
Perceived psychological pain
Participants believed that the prototypically depressed target experienced more pain by the same symptoms (M = 5.42, SD = 1.23) compared with both the control target (M = 4.63, SD = 1.26), t(493) = 5.78, p < .001, d = 0.63, and the counterprototypically depressed target (M = 4.26, SD = 1.31), t(493) = 8.40, p < .001, d = 0.92. The control target was considered as experiencing less pain than the counterprototypically depressed target, t(493) = 2.59, p = .027, d = 0.29. Results for all our measures are depicted in Figure 4.
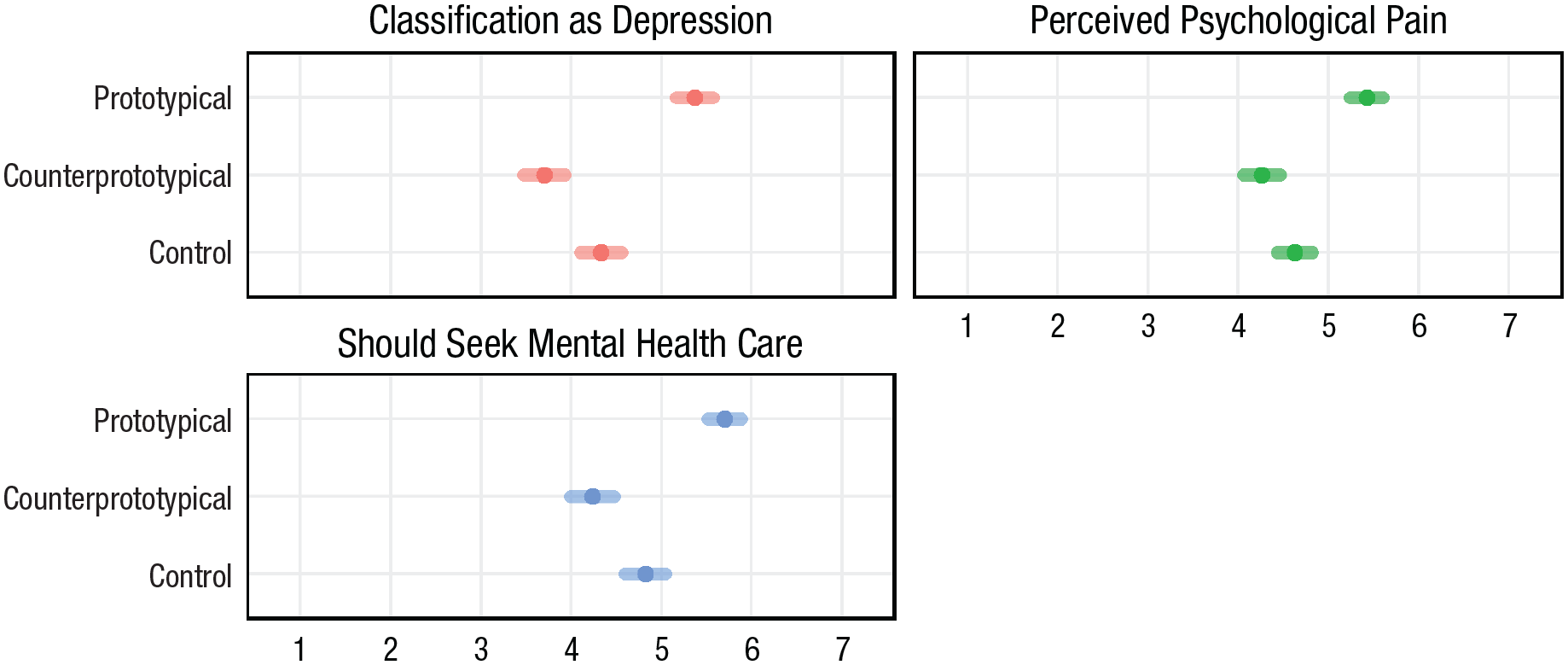
The impact of prototypicality on classification as depression, perceived psychological pain, and appropriateness of seeking professional mental health care, Study 2. Means and 95% confidence intervals are depicted.
Classification as depression
Participants believed that the prototypically depressed target was more likely to have depression (M = 5.37, SD = 1.38) compared with both the control target (M = 4.33, SD = 1.47), t(493) = 6.68, p < .001, d = 0.73, and the counterprototypically depressed target (M = 3.70, SD = 1.44), t(493) = 10.66, p < .001, d = 1.17. The control target was considered more likely to have depression than the counterprototypically depressed target, t(493) = 3.93, p < .001, d = 0.44.
Appropriateness of professional mental health care
Participants believed that professional mental health care was more appropriate for the prototypically depressed target (M = 5.70, SD = 1.26) compared with both the control target (M = 4.82, SD = 1.47), t(493) = 5.72, p < .001, d = 0.62, and the counterprototypically depressed target (M = 4.24, SD = 1.54) t(493) = 9.45, p < .001, d = 1.03. Participants believed that professional mental health care was more appropriate for the control target compared with the counterprototypically depressed target, t(493) = 3.67, p < .001, d = 0.41.
Impact-of-stigma scale
We found that the stigma scale was negatively correlated with all dependent variables. This means that people higher on the stigma scale (i.e., those who were more likely to stigmatize mental health care) were less likely to rate the targets as having depression, to believe that they were in psychological pain, or to recommend mental health care. Importantly, we could not find a significant interaction between target features and the stigma scale on any of the three dependent variables, suggesting that the stigma scale and prototypes have independent effects (see Table 5).
The Impact of Stigma Scale and the Stigma Scale by Condition on the Three Dependent Variables
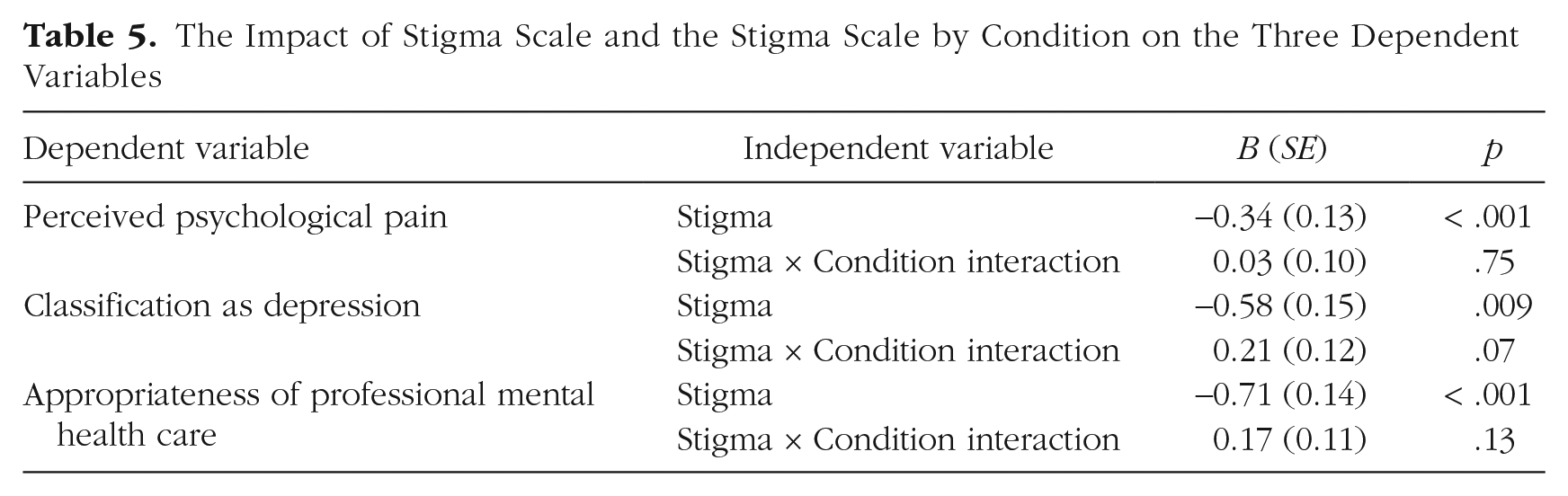
These results show that prototypes of people with depression influence laypeople’s view of depression compared with a control condition and with a counterprototypical condition. Even though all participants read the clinical symptoms of depression for each target, it seems they relied on the prototypical information to evaluate the target rather than the symptoms of depression as listed in the ICD-11. We found no interaction between participants’ level of stigma toward depression and target features, indicating that prototypes of people with depression and stigmatization are largely independent constructs. To verify the robustness of these results, we also conducted a replication (Study S8, in the Supplemental Material) in which we randomly assigned participants to judge either a female or a male target, and target gender did not moderate these results. In the next study, we tested whether simply informing participants that prototypes exert influence on depression recognition could reduce the effect of prototypes. We also added affiliation measures to test whether information about the effect of prototypes could reduce social isolation of prototypical people with depression.
Study 3: Attempting to Reduce the Effect of Prototypes by Informing Participants of the Effect Itself
Method
The goal of this study was to test whether the effect of prototypes can be reduced by informing participants of the influence of prototypes.
We manipulated two factors between subjects: target features (prototypical vs. counterprototypical) and information about the impact of prototypes (shown vs. not shown) on judgments. Participants were therefore randomly assigned to one of four conditions. Participants read the following introduction: Below, a person who is 41 years old and lives in the Los Angeles area is described. This person’s initials are S.K.
Then, participants in the prototypical condition read the following description: A woman is not successful in her job, does not take care of her looks, is quite overweight, is not physically attractive, and is quite introverted.
Participants in the counterprototypical condition read the following description instead: A woman is successful in her job, takes care of her looks, is in good physical shape, is physically attractive, and is quite extroverted.
All participants read the following symptoms: For the past 4 weeks or so, this person has felt quite sadder than normal and could not get to sleep as well as they would have in the past.
Then, participants in the no-information condition proceeded to the measures, whereas participants in the information condition were shown the following: Note: Research has shown that most people consider the same symptoms (e.g., sadness and lack of sleep) as more indicative of depression if the people who have such symptoms fit the prototype of a person with depression (for instance, they are not successful in their job; do not take care of their looks; are physically unattractive, introverted, and overweight), compared with people who do not fit the prototype of a person with depression (for instance, they are successful in their job; take care of their looks; are physically attractive, extroverted, and in good physical shape). Take this into account when replying to the following questions.
Measures
Then, participants were asked six questions, all anchored at 1 (not at all) and 7 (very much). The first three were the same questions about classification as depression, perceived psychological pain, and appropriateness of mental health care asked in previous studies. The second three measured desires of social affiliation with the target (“Would you want to be friends with this person?” “Would you want to be colleagues with this person?” “Would you want to be neighbours with this person?”) and were averaged in an index (α = .91; this decision was not preregistered).
Results
Classification as depression, psychological pain, appropriateness of mental health care
Analyzing the three measures individually with two-way ANOVAs, we found similar results, with large and strong effects of target features, which replicate prior results (all η2 > .09, all p < .001), and small interactions between target features and information (pain, p = .063, η2 = .005; classification as depression, p = .024, η2 = .007; appropriateness of mental health care health, p = .16, η2 = .003), showing that the effect of target features was somewhat reduced in the shown-information condition. For the classification-as-depression measure, there was a large difference between the counterprototypical (M = 3.65, SD = 1.31) and the prototypical condition (M = 5.26, SD = 1.39) when information was not shown (p < .001, d = 1.17). The difference between the counterprototypical (M = 3.83, SD = 1.39) and the prototypical condition (M = 4.94, SD = 1.41) was slightly but significantly reduced when information was shown (p < .001, d = 0.80). Results are depicted in Figure 5.
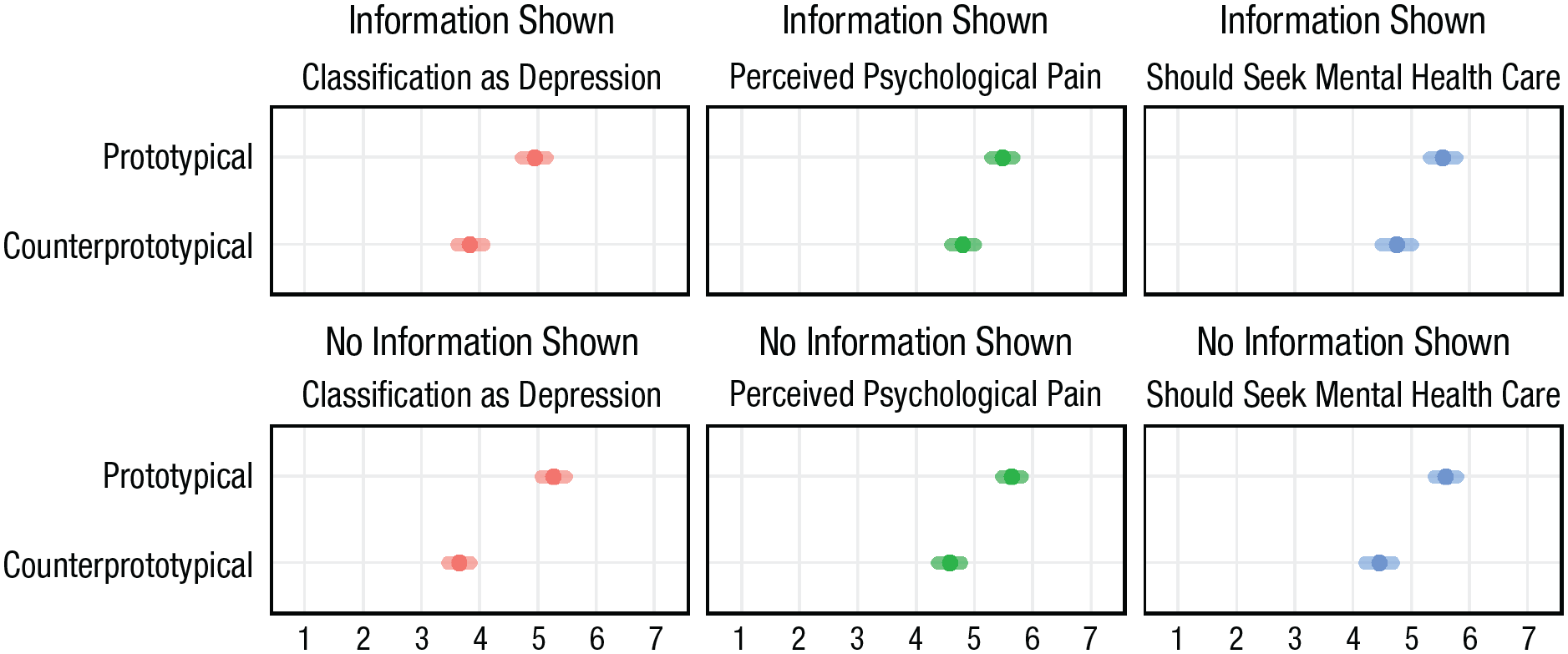
The effect of target prototypicality and information, Study 3. Means and 95% confidence intervals are depicted.
Affiliation desire
A two-way ANOVA found a significant effect of target features, F(1, 594) = 91.76, p < .001, η2 = 0.094, such that participants were more likely to want to be friends, neighbors, or colleagues of the counterprototypically depressed target (M = 4.96, SD = 1.22) rather than of the prototypically depressed target (M = 4.18, SD = 1.22). We found no effect of information, F(1, 594) = 0.84, p = .36, η2 = .001, or of the two-way interaction between target features and information, F(1, 594) = 0.79, p = .38, η2 = .001.
These analyses show that receiving information may somewhat decrease the effects of prototypical-target features on classification as depression. This study adds an important kink to our empirical argument by showing that information can be a viable avenue to somewhat reduce the effect of prototypicality, albeit perhaps with a stronger formulation than the present one. Study S9 (on OSF) shows that instructing participants to ignore target features and focus on symptoms did not moderate the effect of prototypes on the same dependent variables used in this study.
General Discussion
In 14 preregistered studies with French, British, and U.S. American adult participants, we investigated the contents of the prototypes of people with depression in a qualitative and quantitative fashion, and the consequences of these prototypes on how laypeople diagnose and understand depression, and conducted two interventions to reduce the effects of prototypes. We found that laypeople imagine people with depression as having different social, psychological, and physical features compared with nondepressed people, which come together in a multifaceted prototype of the person with depression. These prototypes greatly influence how laypeople view depression symptoms: The same symptoms are considered more indicative of depression when the target experiencing them fits the prototype compared with when they do not or when people have limited information (i.e., a no-information condition). Informing participants of the phenomenon regarding prototype-symptom fit weakly moderated the effect. Explicitly instructing participants to ignore the target’s features and focus on the symptoms did not reduce the effect.
Theoretical and practical implications
The present work has theoretical implications for the understanding of prototypes (Niedenthal et al., 1985). According to Fehr (1988), once a social category is activated, some features of this category is more central and accessible in memory. This article shows that features linked to stereotypes of people with depression are perceived more prototypical for classification of depression (and its consequences) than the actual symptoms of depression. Previous research investigated prototypes of specific categories (Stiegert et al., 2021), especially of victimized or stigmatized people (Goh et al., 2021; Greitemeyer, 2008); the present article contributes to this research line, showing that people have precise and multifaceted prototypes of people with depression. We also advance the understanding of lay theories of mental health (Corrigan & Kleinlein, 2006; Rüsch et al., 2005). Previous research (Barney et al., 2009; Griffiths et al., 2004) focused on the stigma placed on people with mental illness. This article shows that prototypes of people with depression influence judgments about people with depression, seem independent from stigma, and have very specific contents. Importantly, they affect judgments around depression even when people are instructed to resist or ignore them. In general, the present work bridges literatures about prototypes in social psychology and the lay recognition of mental illness in clinical psychology, which have largely proceeded in parallel (but see Cox et al., 2012, and K. Kim & Ahn, 2018).
The present work also has practical implications for the recognition of depression by laypeople (Link et al., 1999; Ormel et al., 1991) and for how the general public understands mental illness (Star, 1955). When diagnosing, professionals might be right to integrate symptoms with other features of the patient to avoid the trap of diagnostic realism; Kendler et al., 2011). However, our results also suggest that when targets do not fit the prototype of a person with depression (e.g., they are successful or attractive), people may not think of them as having depression, and they might remain undiagnosed because people around them are less likely to recommend mental health care. Further, their psychological suffering may be minimized by others, exacerbating the consequences of depression.
Limitations
This article has several limitations. For instance, we did not ask our participants what they thought of the age, gender, and race of the typical person with depression; therefore, we cannot claim that this article studies a universal prototype of people with depression. Second, we tested our hypotheses with laypeople; future research might test the prototype contents and its consequences in a sample of mental health professionals (e.g., psychiatrists, psychologists) to see whether they are similar to those in the lay population (as in Lauber et al., 2006). Third, we recruited participants from the United States, United Kingdom, and France, all Western, rich countries. It is possible that in populations that are not Western and rich (e.g., in Japan or Nigeria), prototypes of people with depression might be qualitatively different. It is also possible that our results might be different in populations with different socioeconomic features compared with those from which we drew. Moreover, our quantitative studies used only scenario-based survey experiments; more naturalistic observations may yield different results. Next, we focused on specific definitions of symptoms and depression, and specific features in prototypes. Using a different set of symptoms and modifying the features used in the prototypes might have different impacts on perceptions. Finally, it is possible that people have different prototypes for mental illnesses that are not depression (e.g., anxiety disorder or schizophrenia), which might have different content and consequences. We hope future research will further investigate these questions and bring new insights into the study of prototypes of depression.
Footnotes
Acknowledgements
We thank Tiziana Metitieri for her feedback on an earlier draft and Ezgi Kara, Irem Sakarya, and Malte Elson for their help in coding the data of Studies 1a and1b.
Transparency
Action Editor: Lasana Harris
Editor: Patricia J. Bauer
Author Contribution(s)
Ignazio Ziano contributed to conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, software, supervision, validation, visualization, writing the original draft, and review and editing. Yasin Koc contributed to conceptualization, formal analysis, methodology, supervision, validation, writing the original draft, and review and editing. Both authors approved the final manuscript for submission.