
Abstract
When we see new people, we rapidly form first impressions. Whereas past research has focused on the role of morphological or emotional cues, we asked whether transient visceral states bias the impressions we form. Across three studies (N = 94 university students), we investigated how fluctuations of bodily states, driven by the interoceptive impact of cardiac signals, influence the perceived trustworthiness of faces. Participants less often chose faces presented in synchrony with their own cardiac systole as more trustworthy than faces presented out of synchrony. Participants also explicitly judged faces presented in synchrony with their cardiac systole as less trustworthy. Finally, the presentation of faces in synchrony with participants’ cardiac diastole did not modulate participants’ perceptions of the faces’ trustworthiness, suggesting that the systolic phase is necessary for such interoceptive effects. These findings highlight the role of phasic interoceptive information in the processing of social information and provide a mechanistic account of the role of visceroception for social perception.
Keywords
The formation of first impressions when we see new faces shapes our social interactions as we appraise others on the basis of their facial appearance. These face-based inferences occur spontaneously (Klapper et al., 2016) and as fast as 33 ms (Todorov et al., 2009). An important aspect of such appraisals relates to perceived trustworthiness (Winston et al., 2002), which is tightly linked to threat evaluation (Adolphs et al., 1998; Engell et al., 2007; Todorov et al., 2008; Winston et al., 2002) and influences a wide range of behaviors, from approach and avoidance (Fenske et al., 2005) to investment decisions in trust games (van ’t Wout & Sanfey, 2008). Whereas past research has mainly focused on morphological or emotional cues of facial appearance, we here turned our attention to how visceral states that are interoceptively perceived can bias our first impressions.
The long-standing interest in the role of interoception in emotional and social processing has been motivated by the hypothesis that the physiological condition of the body acts as the basic substrate for feeling states and emotions (Craig, 2002; James & Lange, 1922). Afferent information from bodily organs influences various psychological functions, from consciousness (Craig, 2009; Damasio, 2003), emotional experience (Barrett et al., 2004; von Mohr et al., 2021), and empathy (Grynberg & Pollatos, 2015) to intuitive decision making (Werner et al., 2009) and information sampling (Galvez-Pol et al., 2020). Although several studies have examined the role of interoception in various facets of social cognition (Grynberg & Pollatos, 2015; Heydrich et al., 2021; Shah et al., 2017; von Mohr et al., 2021), little is known about the role of interoception in the processing of social information and appraisal of others. We here focused on whether and how cardiac afferent signals can influence the first impressions of trustworthiness, with the aim of providing a mechanistic account of the role of visceroception for face and social perception.
One way to study the impact of visceral signals on cognition is to synchronize the presentation of stimuli with the participants’ physiological rhythms (Aspell et al., 2013; Monti et al., 2020). This can be done by presenting visual stimuli in synchrony with the participants’ heartbeats (i.e., cardio-visual synchrony). Here, we used this approach as a way of modeling bodily feelings and their influence on face perception. Previous research inspired by classic bodily-illusion paradigms (Aspell et al., 2013; Heydrich et al., 2018; Sel et al., 2017; Suzuki et al., 2013) has shown that superimposing visual stimuli in synchrony with participants’ hearts over virtual avatars increases participants’ identification with the foreign body. This suggests that cardio-visual synchrony facilitates the integration of external body cues into the neural representation of our own bodies, even if participants are typically unaware of the contingency between interoceptive and exteroceptive information (Sel et al., 2017; Suzuki et al., 2013). Cardio-visual synchrony effects can even modulate access to conscious awareness (Salomon et al., 2016) and the subjective appraisal of affectively neutral visual stimuli (Azevedo et al., 2015). From a mechanistic perspective, the temporal congruency between interoceptive and exteroceptive information promotes their integration (e.g., Suzuki et al., 2013). However, there is still uncertainty regarding precisely how interoceptive signals contribute to these effects. Specifically, it is not clear whether cardio-visual synchrony depends only on the frequency, and not on the cardiac phase, of coupling (Salomon et al., 2016) or whether it is determined by the specific phase of the cardiac cycle the visual stimulus is synchronized to (Azevedo et al., 2015; Sel et al., 2017; Suzuki et al., 2013). The latter proposal is based on a related experimental technique capitalizing on the phasic discharge of aortic baroreceptors—namely, pressure and stretch sensors in the aortic arch that signal variations in blood pressure to the brain at each heartbeat. By time-locking the presentation of a brief single stimulus to the systolic period (i.e., ~200–400 ms after the electrocardiogram’s [ECG’s] R-peak, when the baroreceptors are maximally represented in brain) or to the diastolic period (i.e., the remainder of the cardiac cycle, which corresponds to a period of baroreceptor quiescence), recent studies have documented the influence of these cardiac afferent signals (i.e., at systole vs. diastole) in several sensory and cognitive domains (Ambrosini et al., 2019; Azzalini et al., 2019; Critchley & Garfinkel, 2015). Most notably, afferent cardiac signals contribute to an upregulation of motivationally salient stimuli, such as fearful faces, which are more easily detected (Garfinkel et al., 2014; but see Leganes-Fonteneau et al., 2021), engage more attentional resources (Azevedo et al., 2018), and are judged as more intense (Garfinkel et al., 2014; Leganes-Fonteneau et al., 2021) when perceived during systole than during diastole. It is argued that such enhancement in the processing of threat signals reflects a selective influence of physiology on motivational systems to direct resources toward relevant impending information (Critchley & Garfinkel, 2015). In other words, these interoceptive signals of bodily arousal help prioritize salient and motivationally relevant information. This idea is further supported by research showing the modulation of activity in brain regions associated with both saliency detection and autonomic regulation—such as the amygdala, insula, and brainstem—during the perception of threat-related stimuli (Garfinkel et al., 2014; Gray et al., 2009; Makovac et al., 2015). Even though a recent study found that in conditions of high attentional load, people tend to judge faces presented during systole as less trustworthy than those presented at diastole (Li et al., 2020), it remains unclear to what extent the modulation of social judgments is dependent on cardio-visual synchrony or phasic signals of bodily arousal.
Statement of Relevance
Independently of whether we are right or wrong, we often make inferences about people’s personalities on the basis of the first impressions we form when we look at their faces. Rather than looking at how specific facial features may bias our impressions, as past studies have done, we focused here on the perceiver’s physiological signals from the heart and their influence on first impressions. We bridge social psychology research with new insights from state-of-the-art psychophysiology on the role that physiological signals play on social perception. We show how physiological signals influence how trustworthy we judge different faces to be. Across three studies, faces presented at the moment of a heartbeat, rather than between heartbeats, were perceived as less trustworthy. These effects highlight how signals from the heart bias the social judgments we make, providing a first mechanistic account of how bodily states influence social evaluations and first impressions.
Here, we implemented a cardio-visual stimulation paradigm to study the influence of transient interoceptive states on the perceived trustworthiness of new faces across three studies. In Studies 1 and 2, participants judged the perceived trustworthiness of faces flashing either in frequency and phase synchrony (i.e., at systole) with their own heartbeats (systole-self condition) or following someone else’s previously recorded heart rhythms (other-hearts conditions). Study 3 followed the same paradigm but with a constant phase shift in the cardio-visual synchrony to coincide with cardiac diastole (diastole-self condition), rather than systole, to test whether the cardiac influence is dependent on the phase of the cardiac cycle. Following the known cardiac cycle modulation of saliency networks in the brain and the increased sensitivity to motivationally salient and threat-signaling stimuli (Azevedo et al., 2017, 2018; Garfinkel et al., 2014; Li et al., 2020), we predicted reduced trustworthiness during synchronous cardio-visual stimulation. Moreover, we predicted that this effect would be cardiac-phase specific (i.e., synchronous with systole) rather than simply frequency dependent (i.e., synchronous with either systole or diastole). In other words, we expected the bodily signals of arousal conveyed at systole to selectively increase vigilance or sensitivity to salient social stimuli, which in this context of threat-related judgments would lead to increased perceptions of untrustworthiness.
Open Practices Statement
All data and analysis scripts for Studies 1 to 3 have been made publicly available via OSF and can be accessed at https://osf.io/m74tj/. The design and analysis plans for the studies were not preregistered.
Study 1
Method
Participants
A total of 35 volunteers (age: M = 22.6 years, SD = 3.4; 27 females) were recruited via the departmental subject pool. Calculations in G*Power (Version 3.1; Faul et al., 2007), based on a previous study of cardiac gating on emotional valence (Garfinkel et al., 2014), indicated that a sample size of 35 would be needed to obtain an effect size (f 2) of .40 at a power of 85% with an α of .05, which is consistent with other studies in the field (Azevedo et al., 2018; Li et al., 2020). The study was approved by the Royal Holloway University of London Department of Psychology ethics committee, and written informed consent was obtained from all participants.
Stimuli
Stimuli consisted of images (400 × 477 pixels) of computer-generated Caucasian male faces with neutral facial expressions against a black background (Oosterhof & Todorov, 2008). The faces were created using FaceGen (Version 3.1; http://facegen.com) by the Social Perception Lab at Princeton University (https://tlab.uchicago.edu/databases/) to vary along the dimension of trustworthiness. The selected stimuli set comprised a total of 150 different images consisting of 25 different face identities, each of them with six versions that varied in trustworthiness by increments of 1 standard deviation. The face masks were created by maintaining the shape of the faces but replacing them with pixel-size black-and-white random noise (see Fig. 1a).
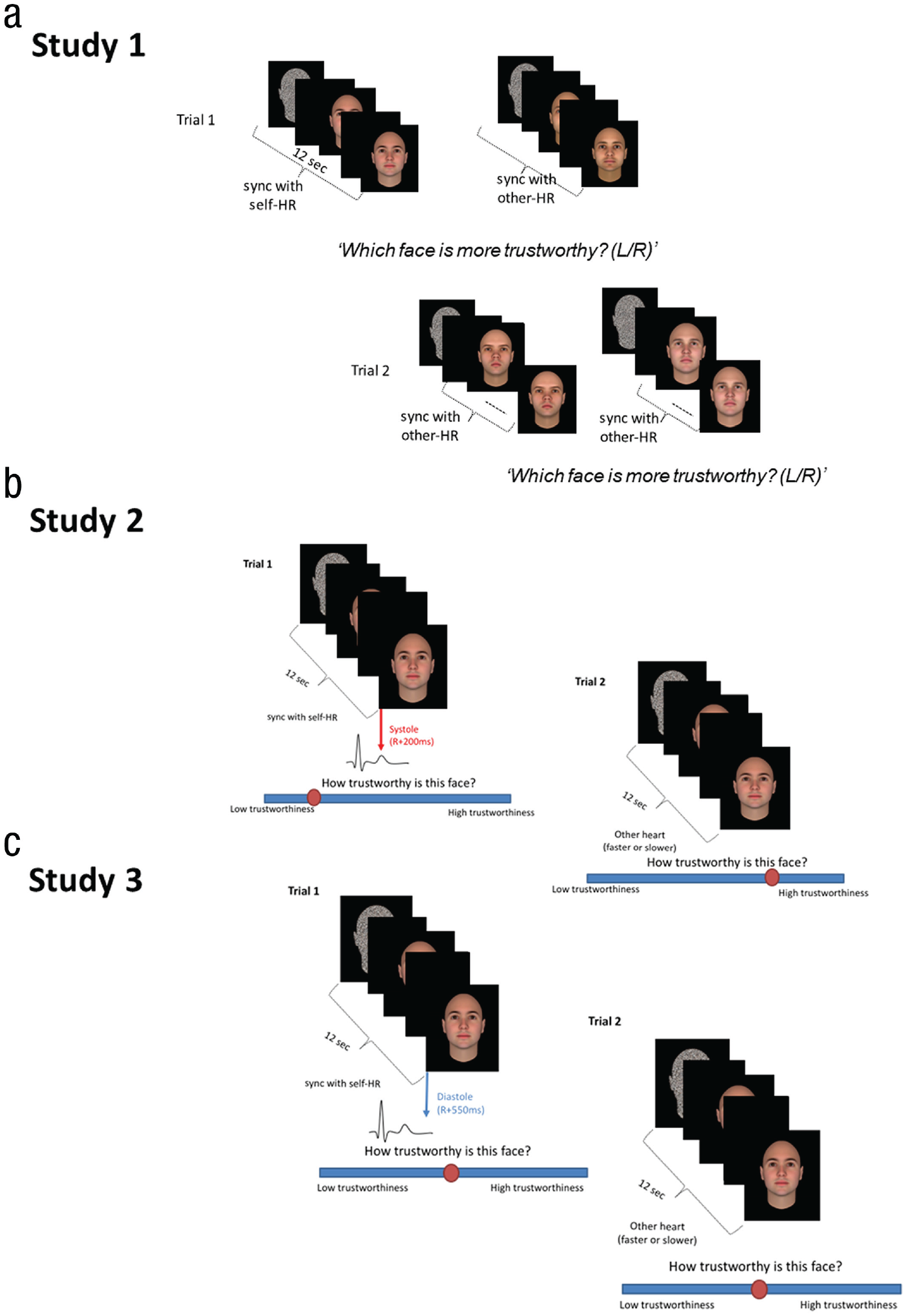
Example trial sequences in the three studies. In Study 1 (a), each trial began with the presentation of two shapes of faces (masks) flashing side by side, which were then replaced by two different pictures of male faces that continued flashing with the same rhythms, either in synch with the participant’s own heart rhythm (HR) at systole (left) or in synch with someone else’s previously recorded slightly faster HR (right; for details on the three possible combinations of rhythm pairings, see the text). Once the faces disappeared from the screen, participants were asked to press a key to answer the question, “Which face is more trustworthy?” In Study 2 (b), only one face was presented at a time (at three possible HRs: systole-self, other-slow, other-fast), followed by the instruction to judge the perceived trustworthiness of each face using a visual analogue scale ranging from 1, low trustworthiness, to 100, high trustworthiness. Study 3 (c) followed precisely the same design as Study 2 except for a phase shift in the synchronization for the stimuli in the self condition, which was presented during cardiac diastole (between heartbeats; diastole-self) instead of cardiac systole as in Studies 1 and 2.
Trustworthiness judgment task
Each trial began with the presentation of two shapes of faces (masks) flashing side by side on a 1,280 × 1,024 computer screen (the distance between the center of the two pictures was 700 pixels). After a variable period of time (8,500–9,000 ms), the masks were replaced with two different pictures of male faces that continued flashing at their individual rhythms for 3,000 to 3,500 ms (see Fig. 1a). Once the faces disappeared from the screen, participants were asked to press a key to answer the question, which face is more trustworthy? Importantly, each mask/face of the pair flashed (for 100 ms) with different rhythms: synchronized with the participant’s heart (systole-self condition) or following another person’s heart rhythm that was either 8% faster (other-fast condition) or 8% slower (other-slow condition) than the participant’s heart. Faces were always paired with another face with an equivalent trustworthiness level, and each face, and thus face pair, was presented three times, once in each rhythm combination: systole-self versus other-slow, systole-self versus other-fast, other-slow versus other-fast. The task contained 90 trials, 30 per condition combination, randomly presented. The intertrial interval was 1,200 ms or 2,200 ms plus a variable time to detect an R-peak in trials with the systole-self condition and a variable delay (from 1 ms to the average interbeat interval) in the other-hearts conditions. Cases with scores 2 standard deviations above or below the mean were excluded from main analyses. No participants met these criteria, and thus there were no exclusions on this basis.
Synchronization procedure
Three disposable ECG electrodes were placed in a modified lead I chest configuration: Two electrodes were positioned underneath the left and right collarbone, and another was placed on the participant’s lower back on the left side. The ECG signal was recorded at 1000 HZ (band-pass filtered between 0.3 and 1000 Hz) with a PowerLab 8/35 data acquisition device (ADInstruments, http://www.adinstruments.com/) using LabChart 8 Pro software (ADInstruments). Heartbeats were detected on-line with a hardware-based function (fast output response; ADInstruments), which identifies the ECG’s R-wave with a delay smaller than 1 ms when the amplitude exceeds an individually defined threshold. In the systole-self condition, pictures were presented at R + 200 ms (Azevedo et al., 2015; Sel et al., 2017) to coincide with the cardiac systole and the period of maximal representation of arterial baroreceptors in the brain. Other heart rhythms consisted of prerecorded interbeat intervals of previous participants performing a similar task (Azevedo et al., 2015) and were adjusted on each trial to be 8% faster or slower than the participant’s heart, as estimated during the preceding trial. In other-slow versus other-fast trials, the average heart rhythms were 4% slower and faster, respectively, than the participants’ own heart to maintain the 8% relative difference between the two rhythms. The other-hearts database contained several different heartbeat samples from distinct participants, and each trial presented a random portion of one of these samples. Thus, no other-heart trials had exactly the same heart rate variability.
Heartbeat detection task
To measure participants’ ability to detect their heartbeats (i.e., their interoceptive accuracy; Garfinkel et al., 2015), we asked them to perform the heartbeat detection task (Whitehead, 1977) at the end of the trustworthiness judgments protocol. In this task, participants were presented with sequences of 10 auditory tones that could be either synchronous with their heartbeats (R + 200 ms) or in between heartbeats (R + 500 ms) and asked to judge whether each sequence was synchronous (i.e., “on beat”) or asynchronous (i.e., “off beat”) with their own hearts. There were 20 trials for each condition presented in random order. The percentage of correct answers was taken as an index of participants’ interoceptive accuracy.
Results
Each condition (systole-self, other-slow, other-fast) and condition pair (systole-self vs. other-slow, systole-self vs. other-fast, other-slow vs. other-fast) had the same number of trials; therefore, our dependent variable was the number of times each participant chose as more trustworthy a face flashing with each rhythm. We submitted these values to a repeated measures analysis of variance (ANOVA) with rhythm (systole-self, other-slow, other-fast) as a within-subjects factor and performed post hoc comparisons (two-tailed t tests) between each rhythm. As shown in Figure 2a, results revealed an influence of flashing rhythm in participants’ judgments, F(2, 68) = 3.50, p = .036, η p 2 = .093, with Bayes factor (BF) analysis (BF10 = 5.85) indicating moderate evidence in favor of the alternative hypothesis (Dienes, 2014; Quintana & Williams, 2018). People less often chose faces synchronized with their own heart as more trustworthy (M = 28.26, SD = 3.66, 95% confidence interval [CI] = [27.00, 29.51]) than faces synchronized with other-slow (M = 30.66, SD = 3.72, 95% CI = [29.38, 31.93]), t(34) = −2.40, p = .022, Cohen’s d = 0.40, and other-fast (M = 31.08, SD = 4.39, 95% CI = [29.58, 32.60]), t(34) = −2.33, p = .026, Cohen’s d = 0.39, rhythms (see Fig. 2a). No difference between other-fast and other-slow trials was observed, t(34) = −0.35, p = .73, Cohen’s d = 0.059. We also reanalyzed the data using multilevel mixed log-linear regression analysis to control for the possible picture-specific effects (i.e., item-level variability) and to understand whether the effect of rhythm varied according to the “objective” level of trustworthiness of each face pair. This analysis confirmed the main effect of rhythm and revealed no interaction between rhythm and the trustworthiness levels of face pairs (see the Supplemental Material available online).
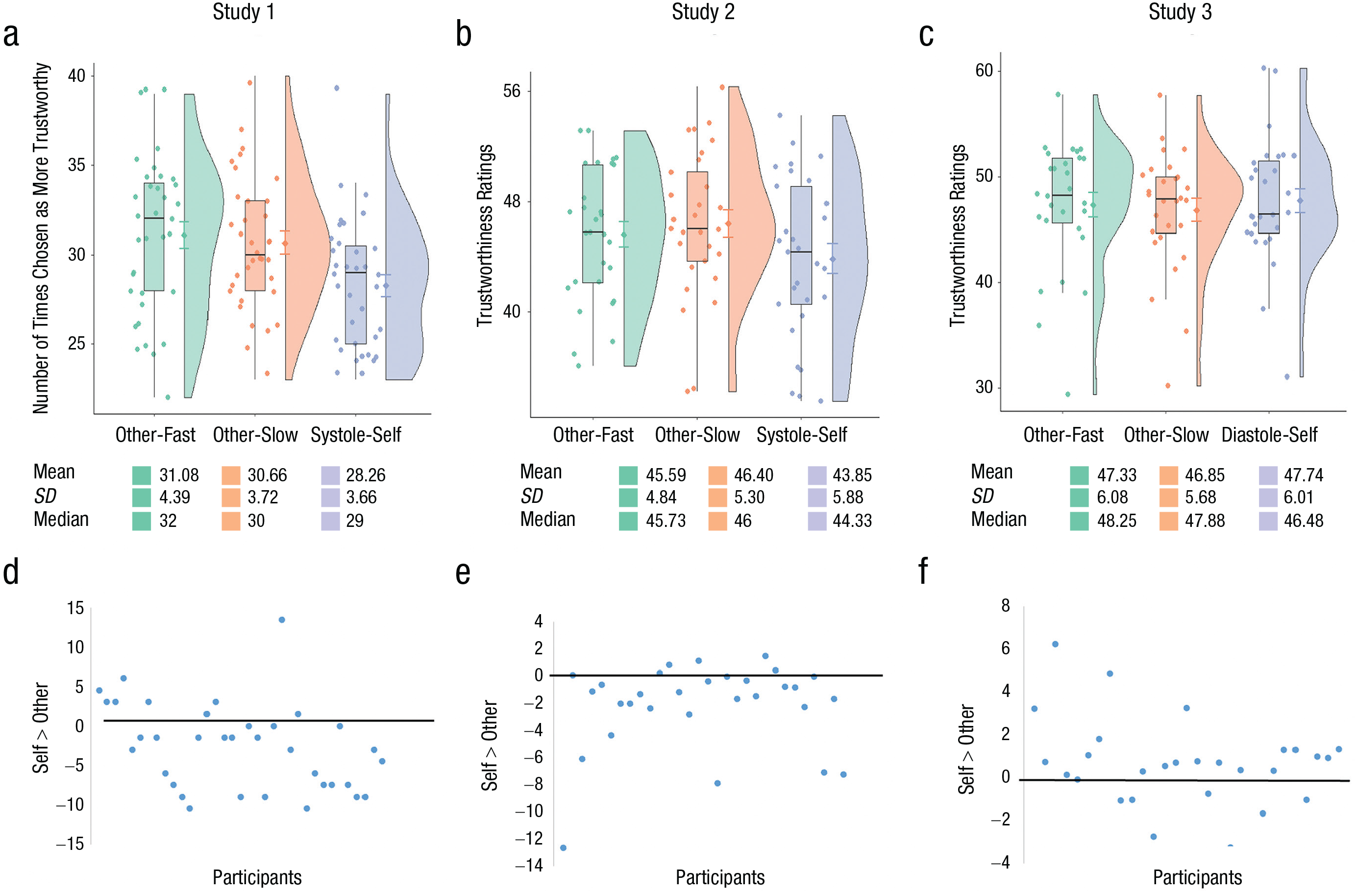
Trustworthiness judgments for Study 1 (a), Study 2 (b), and Study 3 (c) for each cardiac rhythm condition. The raincloud plots provide a data distribution, the box plots show the interquartile range, the central lines in the box plots indicate medians, and individual raw data are indicated by dots (jittered for readability). Error bars denote standard errors of the mean. The mean, standard deviation, and median are shown for each condition. The magnitude of the other versus self bias in Study 1 (d) is shown for each participant. The bias was calculated as follows: systole-self – (other-slow + other-fast)/2. Values below zero reflect a lower number of times that participants chose faces synchronized with their own hearts as more trustworthy compared with faces synchronized with someone else’s heart. The magnitude of the other versus self bias in Study 2 (e) is shown for each participant. This was calculated by subtracting the average ratings across other-fast and other-slow trials from those to systole-self trials. Values below zero indicate reduced trustworthiness ratings in the systole-self condition compared with the other-hearts conditions. The magnitude of the other versus self bias in Study 3 (f) is shown for each participant. This was calculated by subtracting the average ratings across other-fast and other-slow trials from those to diastole-self trials. Values below zero indicate reduced trustworthiness ratings in the diastole-self condition. Note that no effect of heart rhythm was found in Study 3.
To understand whether the observed effects were related to participants’ ability to detect their own heartbeats, we correlated interoceptive accuracy scores (M = 57.6, SD = 10.7) with the difference between the number of times participants chose the face in the systole-self condition and the average of the other-hearts conditions. No significant relation between the two measures was found (r = −.22, p = .20). Thus, participants less often chose faces synchronized with their own heart rhythm as more trustworthy than faces flashing according to someone else’s prerecorded heart rhythms, which suggests an influence of ongoing interoceptive information when making social inferences from others’ faces. However, because the two faces were presented almost simultaneously, it is also possible that stimuli presented in synchrony with the participants’ hearts were given less attention and therefore chosen less often. To rule out this hypothesis, we carried out a separate study.
Study 2
Method
In Study 2, we presented only one face at a time and asked participants to judge the perceived trustworthiness of each face (see Fig. 1b). Lower ratings to faces synchronized with the participants’ heartbeats would provide a conceptual replication of Study 1 and rule out the possibility that the previously observed effects were driven by attention competition between the two faces.
Participants
The effect size obtained in Study 1 (η p 2 = .093) suggested that at least 27 participants were needed to obtain a power of 95% (power analysis run in G*Power Version 3.1; Faul et al., 2007). Thus, a similar sample size was selected for this study. Specifically, 30 volunteers (age: M = 24.17 years, SD = 4.90; 21 females) were recruited from the departmental subject pool in Royal Holloway University of London. Data from one additional participant were excluded because of technical problems during the session. The study was approved by the Royal Holloway University of London Department of Psychology ethics committee, and written informed consent was obtained from all participants.
Trustworthiness judgment task
The stimuli, task, and procedures were identical to those of Study 1 with the exception that in this study, only one face was presented at a time in the center of the screen (see Fig. 1b). The trial ended with participant’s answer to the question, “How trustworthy is this face?” on a visual analogue scale (1–100) anchored with the labels low trustworthiness and high trustworthiness. Each face was presented three times, once with each rhythm type: systole-self, other-slow, and other-fast. As in Study 1, in the systole-self condition, pictures were presented during cardiac systole (R + 200 ms). Cases with scores 2 standard deviations above or below the mean were excluded from the main analyses. One participant was excluded on this basis (note that we obtained the exact same pattern of results when including this participant in the main analyses).
Results
Average trustworthiness ratings were submitted to a repeated measures ANOVA with rhythm (systole-self, other-slow, other-fast) as a within-subjects factor. In line with results from Study 1, results showed a significant effect of rhythm, F(2, 56) = 8.57, p = .001, η p 2 = .23, with BF analysis (BF10 = 81.982) also indicating very strong evidence in favor of the alternative hypothesis (Dienes, 2014; Quintana & Williams, 2018). This is explained by lower trustworthiness ratings for faces in the systole-self condition (M = 43.85, SD = 5.88, 95% CI = [41.62.00, 46.09]) compared with those in the other-slow (M = 46.40, SD = 5.30, 95% CI = [44.38, 48.41]), t(28) = −3.78, p = .001, Cohen’s d = 0.70, and other-fast (M = 45.59, SD = 4.84, 95% CI = [43.75, 47.43]), t(28) = −2.69, p = .012, Cohen’s d = 0.50) conditions (see Fig. 2b). There was no difference in the ratings given to faces in the other-slow and other-fast conditions, t(28) = 1.44, p = .16, Cohen’s d = 0.27. No correlation was found between participants’ interoceptive accuracy (M = 55.23, SD = 9.03) and the difference in trustworthiness ratings in the systole-self and the average of other-hearts conditions (r = .16, p = .42).
As in Study 1, we also carried out linear mixed model regression analysis to understand whether the effect of rhythm varied according to the level of trustworthiness of each face. Again, only the main effect of rhythm, and not its interaction with trustworthiness levels, was found to be significant (see the Supplemental Material), confirming that the observed effects did not seem to depend on morphological features typically associated with trustworthiness or untrustworthiness. This pattern provides a conceptual replication of Study 1 by showing that faces presented in synchrony with participants’ hearts are judged as less trustworthy, consistent with the cardiac cycle literature showing increased sensitivity to threat-related stimuli (Azevedo et al., 2018; Garfinkel & Critchley, 2016; Garfinkel et al., 2014, 2021; Leganes-Fonteneau et al., 2021) and diminished trustworthiness ratings (Li et al., 2020) when faces are presented during cardiac systole. However, both Studies 1 and 2 implemented the cardio-visual synchrony manipulation only during systolic periods. To establish whether the observed effects were indeed associated with transient neuromodulatory states induced by phasic cardiac signals, we needed to test whether cardio-visual synchrony delivered during diastole would lead to similar effects.
Study 3
Method
In Study 3, we made a single but important modification to the design of Study 2. Here, self-heart synchrony was defined by presenting faces during cardiac diastole, when the representation of cardiac signals in the brain is minimal (see Fig. 1c). An absence of modulation in participants’ ratings across the different conditions would confirm our hypothesis that cardiac afferent signals are essential for lower trustworthiness judgments.
Participants
To maximize comparability between studies, we set our target sample size to be equivalent to that of Study 2. Specifically, a new group of 29 volunteers (age: M = 25.03 years, SD = 5.27; 20 females) were recruited via the departmental participant pool. The study was approved by the Royal Holloway University of London Department of Psychology ethics committee, and written informed consent was obtained from all participants.
Trustworthiness judgment task
The stimuli, task, and procedures were identical to those of Study 2 with the exception that in this study, stimuli in the synchronous condition were presented during cardiac diastole (R + 500 ms; diastole-self condition). This procedure preserved the frequency and heart dynamics of the previous cardio-visual stimulation procedure but introduced a phase shift (i.e., consistent delay) of the visual presentation in relation to the cardiac cycle (cf. Salomon et al., 2016). In other words, the exteroceptive and interoceptive information were still coupled, but synchrony was now achieved by presenting stimuli during the quiescent phase of the cardiac cycle. Cases with scores 2 standard deviations above or below the mean were excluded from the main analyses. One participant was excluded on this basis (note that we obtained the exact same pattern of results when including this participant in the main analyses).
Results
A repeated measures ANOVA with rhythm (diastole-self, other-slow, other-fast) as a within-subjects factor was used to test for differences in average trustworthiness ratings in each condition. Contrary to Study 2, results showed no significant effect of rhythm, F(2, 54) = 0.93, p = .40, η p 2 = .033 (see Fig. 2c), with BF analysis (BF10 = 0.21) indicating moderate (Quintana & Williams, 2018) or substantial (Dienes, 2014; Jeffreys, 1939/1961) evidence in favor of the null hypothesis. These results were further confirmed by a linear mixed model regression analysis (see the Supplemental Material) that also showed a lack of a significant interaction between rhythm and “objective” trustworthiness levels on subjective ratings.
The contrast with Study 2 was further qualified by an additional analysis merging the two data sets in a single ANOVA with study (Study 2, Study 3) as a between-subjects factor. Although we found a significant Rhythm × Study interaction, F(2, 110) = 7.32, p = .001, η p 2 = .117, BF10 = 7.74, neither the main effect of rhythm, F(2, 110) = 1.86, p = .16, η p 2 = .033, BF10 = 0.27, nor the main effect of study, F(1, 55) = 2.10, p = .15, η p 2 = .037, BF10 = 0.81, were significant. Critically, even though the significant Rhythm × Study interaction merely suggests that the rhythm effect was smaller in Study 3 relative to Study 2, our BF analyses indicated that the data supported the null hypothesis of no effect of rhythm for Study 3. As in the previous studies, we found no correlation between interoceptive accuracy (M = 50.80, SD = 8.4) and the difference in trustworthiness ratings in the diastole-self and the average of the other-hearts conditions (r = −.25, p = .20). Thus, contrary to Studies 1 and 2, Study 3 did not show a modulation in participants’ judgments as a function of the presentation rhythm, suggesting that the phase (i.e., systole) of the cardiac cycle in which synchronization occurs is crucial for the effects to take place.
General Discussion
We investigated the role of cardio-visual stimulation on trustworthiness judgments. Faces presented in synchrony with the participant’s heart rhythm (at systole) were chosen less often as more trustworthy (Study 1) and were explicitly judged as less trustworthy (Study 2) than those presented asynchronously. These patterns suggest an influence of ongoing interoceptive information when people make social inferences from others’ faces. Importantly, we found substantial evidence (BF10 = 0.21; Dienes, 2014; Jeffreys, 1939/1961) suggesting that presenting faces synchronized with the participant’s heart rhythm at diastole (Study 3) does not have an effect on participants’ judgments, indicating that the cardiac cycle phase is critical. Thus, the mere integration between the visual and cardiac modalities that may take place because of the temporal congruency between the two is not sufficient to modulate the processing of external social information, such as perceived trustworthiness. These results suggest a crucial role for the transient phasic cardiac afferent signals conveyed to the brain during systole in the modulation of social judgments. Together, these results advance our understanding of the mechanisms underlying the integration of interoceptive and exteroceptive information via cardio-visual stimulation by highlighting the importance of phasic interoceptive information in the modulation of social judgments.
Indeed, heightened arousal has been associated with reduced perceived trustworthiness of other people. For example, when judging trustworthiness of faces, participants tend to give lower trustworthiness ratings following a negative arousal induction procedure (Abbott et al., 2018). Hooker et al. (2011) also suggested that individuals in a heightened state of arousal perceive unfamiliar individuals as less trustworthy. The link between arousal and trustworthiness was further qualified in a study by Aguado and colleagues (2011) showing that untrustworthy faces were judged more negatively and as more arousing than trustworthy faces even after both types were conditioned to elicit positive associations. Our findings provide a mechanistic illustration of these patterns. Given that, at systole, one’s own cardiac physiological information is accentuated, when faces are presented when one is in a state of heightened physiological arousal, they are more likely to be perceived as less trustworthy.
In line with this, Li and colleagues showed that people tend to judge faces presented during systole (vs. diastole) as less trustworthy in conditions of high attentional load (Li et al., 2020). We extend these findings by showing that biases in judgments can occur across constant attentional conditions and that the critical process underlying cardiac modulation on trustworthiness judgments seems to be driven specifically by systole-related neurovisceral states rather than those occurring during diastole. In fact, standard cardiac cycle paradigms, such as that employed by Li and colleagues (2020), compare responses to stimuli presented at systole relative to those at diastole, making it difficult to ascertain which condition is driving the observed effects (e.g., whether “diastolic states” are associated with increased trust or “systolic states” are associated with decreased trust). The dissociation observed between our Studies 2 and 3 disambiguates this pattern: These effects are indeed driven by phasic activity taking place during systole alone.
The specific cardio-visual effects observed on perceived trustworthiness reported here go beyond the multisensory integration process that seems to explain some of the past studies using cardio-visual stimulation (Aspell et al., 2013; Heydrich et al., 2018; Ronchi et al., 2015; Salomon et al., 2016). A key difference between these studies and the present one is the lack of social salience or relevance of the stimuli in the former studies. Judging trustworthiness is an important spontaneous inference made from facial appearance tightly related to threat evaluation and amygdala integrity and functioning (Adolphs et al., 1998). Such differential effects according to stimuli type are well known in the cardiac cycle literature (Azzalini et al., 2019; Garfinkel & Critchley, 2016). Specifically, context-relevant salient stimuli, such as those likely to promote orienting responses, are more easily detected, engage additional attentional resources, and are judged as more intense when perceived during systole (Azevedo et al., 2017; Garfinkel et al., 2014, 2021). Conversely, the processing of weak sensory stimuli (e.g., Al et al., 2020; Motyka et al., 2019) or those promoting withdrawal responses (e.g., Edwards et al., 2001; Gray et al., 2009) are inhibited during systole. This is in line with known neuromodulatory systems tightly linked to arousal and autonomic feedback, such as the noradrenergic system, that selectively increase neural gain to the processing of contextually relevant stimuli and facilitate orienting responses (Aston-Jones & Cohen, 2005; Sara, 2009). Thus, the observed selective cardio-visual effect on trustworthiness judgments at systole is likely to go beyond simple interoceptive-exteroceptive integration and may reflect a neuromodulation of saliency and orienting systems driven by the cardiac cycle. We should note, however, that the cardiac cycle effects observed were independent of the level of morphological features typically associated with trustworthiness and untrustworthiness present in each face. This suggests a modulation that is not necessarily selectively responsive to stimuli highly indicative of threat but one that is more likely to be explained by the environmental (i.e., instructions to judge trustworthiness) and internal (i.e., transient states of autonomic feedback) contexts that together bias perception to increase vigilance. This explanation is also congruent with the proposal that the amygdala, an area known to mediate cardiac cycle modulations of threat processing (Garfinkel et al., 2014; Gray et al., 2009), is more responsive to the valence than to the arousal of a face (Todorov et al., 2008).
Limitations and future directions
Despite these insights, our findings should be considered in light of the study’s limitations and directions for future research. Firstly, our studies examined the role of cardio-visual stimulation on trustworthiness judgments, yet its impact on the processing of other types of social inferences from faces remains unknown. Future studies should investigate whether ongoing afferent interoceptive signals also modulate the appraisal of other, non-threat-related social information from other people’s faces, such as physical attractiveness. Furthermore, although it has been shown that interoceptive accuracy interacts with cardiac cycle manipulations in the case of social cognition performance (von Mohr et al., 2021) and has theoretical implications for social relatedness (Palmer & Tsakiris, 2018), in the present study, interoceptive accuracy did not seem to relate to the observed effects. Future studies should examine whether other interoceptive dimensions, such as interoceptive sensibility or awareness (Garfinkel et al., 2015), play a role on perceived trustworthiness or whether they interact with the phase of cardio-visual synchrony. Finally, although we argue that the observed effects rely on baroreceptor-related mechanisms, we cannot fully discard the possibility that other bodily changes covarying with the cardiac cycle (e.g., muscle spindle activity due to cardioballistic fluctuations; Birznieks et al., 2012), contribute to modulate cognition and social perception.
In sum, across three studies, we demonstrated and substantiated an effect of cardiac-visual stimulation on the social evaluation of faces and, more specifically, on trustworthiness judgments. Moreover, we showed that these effects arise only when cardio-visual coupling occurs during cardiac systole, highlighting the importance of phasic interoceptive signals in the modulation of social judgments.
Constraints on generality
Our findings provide evidence that transient phasic cardiac afferent signals conveyed to the brain during systole modulate perceived trustworthiness. However, as with most experimental paradigms used in psychological research, there is no evidence that these findings will easily occur outside of laboratory settings. Generally, one may expect that when someone is evaluating the trustworthiness of a person, they do that over the course of several heartbeats with perceptually stable visual stimuli. However, just as other experimental approaches manipulate a specific process to study how it may impact cognition and behavior, the synchronization of visual stimuli with the cardiac cycle is a means to tap into spontaneous fluctuations of cardiovascular arousal and study how they affect perception. Arguably, the neuromodulation brought about by these transient interoceptive states also occurs in real-life situations and mirrors what may happen during (mild) sustained arousal. Moreover, recent studies have found that the way in which we actively sample the world (e.g., saccades, fixations, behavior initiation) at our own pace is modulated by the phase of the cardiac cycle (Galvez-Pol et al., 2020; Kunzendorf et al., 2019). Thus, we suspect a similar phenomenon here, where not only first impressions can be modulated by the specific phase of the cardiac cycle in which the face is perceived, especially as face-based inferences occur as fast as 33 ms (Todorov et al., 2009), but also similar neuromodulatory states will be present over the course of several heartbeats in conditions of mild arousal.
Supplemental Material
sj-docx-1-pss-10.1177_09567976221131519 – Supplemental material for From the Viscera to First Impressions: Phase-Dependent Cardio-Visual Signals Bias the Perceived Trustworthiness of Faces
Supplemental material, sj-docx-1-pss-10.1177_09567976221131519 for From the Viscera to First Impressions: Phase-Dependent Cardio-Visual Signals Bias the Perceived Trustworthiness of Faces by Ruben T. Azevedo, Mariana von Mohr and Manos Tsakiris in Psychological Science
Footnotes
Transparency
Action Editor: Yoel Inbar
Editor: Kate Ratliff
Author Contributions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.