
Abstract
We tested whether experience of playing a musical instrument was associated with lifetime change in cognitive ability. Participants were 366 older adults from the Lothian Birth Cohort 1936 who had completed general cognitive-ability assessments at ages 11 and 70 and reported their lifetime experience of playing a musical instrument at age 82. This sample included 117 participants with musical-instrument experience, mostly at a beginner or an intermediate level. There was a small, statistically significant positive association between experience of playing a musical instrument and change in general cognitive ability between ages 11 and 70; specifically, individuals with more musical-instrument experience were likely to show greater gains in general cognitive ability. This association was reduced but remained statistically significant following adjustment for covariates (childhood and adulthood socioeconomic status, years of education, and disease history). These findings suggest that playing a musical instrument is associated with a long-term cognitive advantage.
Learning to play a musical instrument is a complex multisensory task that has inspired substantial research attention. In particular, there is a long-standing interest in the potential effects of musical training on other, nonmusical domains of functioning, including cognitive ability (Hetland, 2000; Moreno, 2009; Overy, 1998; Swaminathan & Schellenberg, 2021). The present observational study tested whether experience of playing a musical instrument is associated with lifetime change in general cognitive ability.
Observational studies comparing the cognitive performance of adult musicians and nonmusicians often find a cognitive advantage in favor of musicians. This advantage has been found across a variety of cognitive tests, including tests of general cognitive ability (for reviews, see Costa-Giomi, 2015; Swaminathan & Schellenberg, 2014). Observational studies with children have found similar positive associations between musical-training experience and cognitive performance. For instance, in one cross-sectional study of 6- to 11-year-olds, Schellenberg (2006) found that, after analyses controlled for family income, parents’ education, and participation in nonmusical extracurricular activities, duration of musical training was positively correlated with general cognitive ability, accounting for 6% of the variance in cognitive test scores.
Building on observational findings, intervention studies have tested whether musical training might have a causal effect on cognitive development. These studies work from the premise that musical training might promote the development of specific perceptual or cognitive abilities, which in turn support general cognitive enhancements. Barbaroux et al. (2019) found that children from a low-socioeconomic-status background tested before and after 18 months of musical training showed significant improvement on a test of general cognitive ability; although the study did not include an active control group, the authors did control for cognitive-maturation effects by comparing age-normalized scores at each stage of the study. In another intervention study (Moreno et al., 2011), young children assigned to a computer-based music-training program for 20 days (including training in rhythm, pitch, melody, and voice and focusing on listening activities rather than instrumental training) showed improvement in verbal ability and in executive-function tasks relative to a group of children assigned to a computer-based visual art-training program. Similar results were reported in an earlier study by Schellenberg (2004), who found that children randomly assigned to 1 year of music lessons (small-group lessons in either keyboard or voice) showed greater gains in general cognitive ability than children in two control groups (attending drama lessons or having no additional lessons). Such studies are complemented by other intervention studies investigating the neural correlates of musical training: For example, children who participated in 15 months of keyboard training have been found to show greater structural brain changes in motor and auditory areas than a passive control group (Hyde et al., 2009).
Reviews of intervention studies (including those described above) have drawn differing conclusions regarding the potential for musical training to enhance cognitive function. A meta-analysis of 54 intervention studies that tested for potential cognitive or academic benefits of musical training found that among studies implementing active control designs or randomization procedures, there was an overall null effect of musical training on children’s cognitive or academic performance (Sala & Gobet, 2020). However, a reanalysis of the Sala and Gobet (2020) data set by another group (Bigand & Tillmann, 2021) illustrated that the original analytical decisions made had led to an underestimate of the potential benefits of musical training; this new analysis showed a significant effect size (Hedges’s g = 0.234). A similar finding of a small to medium positive effect of musical training on cognitive performance in children (even in studies using an active control group) was reported in another meta-analysis of 21 studies by Cooper (2020).
A critical question that follows from studies demonstrating a causal link between musical training and cognitive function is whether any potential cognitive benefits of musical training are long-lasting, that is, whether they are sustained beyond the period of musical training. Findings from cross-sectional observational studies provide some initial support for this effect. Schellenberg (2006) found that years of playing a musical instrument in childhood was positively correlated with performance on a test of general cognitive ability in early adulthood after accounting for socioeconomic variables (r = .21). A similar cognitive advantage was observed in a study of older adults; former and active musicians scored higher on a test of verbal ability than nonmusicians (Strong & Midden, 2020). Other studies have demonstrated the potential long-term effects of musical training on the auditory system. White-Schwoch et al. (2013) found that older adults who played a musical instrument in childhood and/or young adulthood showed more efficient auditory brain-stem responses to fast-changing sounds than did older adults with no musical training.
Statement of Relevance
Good cognitive skills can be linked to positive life outcomes, including academic achievement, occupational attainment, and health. It is thus important to identify factors, experiences, or interventions that can support the development of cognitive skills. Learning to play a musical instrument is a complex, multisensory task, and musical training has been shown to be associated with better performance on cognitive-ability tests; however, it is less clear whether any potential benefits of musical training last over the long term. We addressed this question by examining changes in cognitive performance between the ages of 11 and 70 years. We found that more experience of playing a musical instrument was associated with slightly more positive cognitive change over this period of the life span. Results from this observational study cannot conclusively show that musical training causes an improvement in cognitive ability; however, our findings indicate that musical training is associated with some long-lasting cognitive advantages.
One interpretation of these cross-sectional observational findings is that musical training causes a positive change in cognitive ability and that this advantage is sustained over time. However, these studies cannot rule out the potentially confounding effect of childhood cognitive ability, that is, the tendency of more cognitively able children to engage in musical training (Schellenberg, 2011) and to perform well on cognitive tests in adulthood and older age (Deary, 2014). With a longitudinal design and repeated assessments of cognitive ability, it is possible to control for early-life cognitive ability and to test directly whether musical training is associated with more positive change in cognitive ability over the long term.
The Lothian Birth Cohort 1936 (LBC1936) study includes data on general cognitive ability at ages 11 and 70, making it possible to assess cognitive change over approximately 60 years. Information regarding LBC1936 participants’ childhood environment, education, adult occupational class, and disease history are also available (Deary et al., 2007; Taylor et al., 2018). We recently gathered lifetime musical-experience data with this cohort, reported retrospectively at age 82 (Okely et al., 2021). We used these data for the current preregistered study (https://osf.io/r9fbx) to test whether more experience of playing a musical instrument was associated with more positive change in general cognitive ability between the ages of 11 and 70. In this study, the term “change in general cognitive ability” describes the net result of rapid cognitive development in childhood and adolescence, as well as decline in certain cognitive abilities, typically seen from early to middle adulthood onward (Salthouse, 2019).
Considering the findings reviewed above, we predicted that, in an analysis controlling for sociodemographic variables and disease history, greater experience of playing a musical instrument would be associated with more positive change in general cognitive ability between ages 11 and 70.
Method
Participants
The LBC1936 is a longitudinal study of community-dwelling individuals. All were born in 1936 and most are surviving participants of the Scottish Mental Survey of 1947 (SMS1947). The SMS1947 tested the cognitive ability of 70,805 Scottish schoolchildren born in 1936 at a mean age of 11 years old (Scottish Council for Research in Education, 1949). LBC1936 participants were mostly recruited from the Edinburgh and Lothian areas of Scotland, and the first wave of testing was conducted between 2004 and 2007 with a sample of 1,091 participants (age: M = 69.5 years, SD = 0.83). Since then, participants have returned for cognitive, medical, genetic, brain-imaging, lifestyle, and psychosocial assessment every 3 years in Waves 2, 3, 4, and 5, which took place between 2007 and 2010 (N = 866; age: M = 72.5 years, SD = 0.71), between 2011 and 2013 (N = 697; age: M = 76.2 years, SD = 0.68), between 2014 and 2017 (N = 550; age: M = 79.3 years, SD = 0.62), and between 2017 and 2019 (N = 431; age: M = 82.0 years, SD = 0.47), respectively. The present study used data from age 11 (collected as part of the SMS1947) and Wave 1 (age 70), as well as additional musical-experience data collected at Wave 5 (age 82) of the LBC1936 study. Further details regarding the background, recruitment, and testing of LBC1936 participants are documented by Deary et al. (2007) and Taylor et al. (2018). Ethical permission was granted by the Multi-Centre Research Ethics Committee for Scotland (Wave 1: MREC/01/0/56), the Lothian Research Ethics Committee (Wave 1: LREC/2003/2/29), and the Scotland A Research Ethics Committee (Waves 2, 3, 4, and 5: 07/MRE00/58). Written consent was obtained from participants at each wave.
Measures
Cognitive ability
Cognitive ability was assessed at ages 11 and 70 with the same test, the Moray House Test No. 12 (MHT; Scottish Council for Research in Education, 1949), with the same instructions and time limit at both ages. The MHT is a test of general cognitive ability and consists of 71 items that involve following directions, same–opposites, word classification, analogies, practical items, reasoning, proverbs, arithmetic, spatial items, mixed sentences, and cypher decoding. The test has a maximum score of 76 (note that only total MHT scores are currently available for analysis). MHT scores at age 11 were validated against the Terman-Merrill revision of the Stanford-Binet Tests of Intelligence (Scottish Council for Research in Education, 1949; Terman & Merrill, 1937). MHT scores at age 70 were highly correlated (r = .67) with a concurrently measured factor of general fluid cognitive ability, assessed by five nonverbal subtests from the Wechsler Adult Intelligence Scale–III UK (Deary et al., 2010). Further details regarding the MHT are documented by Deary et al. (2004). At age 70, participants also completed the Mini-Mental State Examination (MMSE; Folstein et al., 1975), which is often used as a dementia-screening instrument. Scores range from 0 to 30; a score of less than 24 is sometimes treated as an indicator of possible cognitive impairment.
Experience of playing a musical instrument
Many previous observational studies on the association between musical training and cognitive function compared the cognitive performance of musicians with that of a nonmusician group. In contrast with this approach, our study treated experience of playing a musical instrument as a continuous latent variable in which participants with the most experience (including a semiprofessional musician) were at one end of the continuum and participants with no experience of playing a musical instrument were at the other.
Participants’ lifetime musical experience was assessed at Wave 5 of the LBC1936 study (age: M = 82 years) with the Edinburgh Lifetime Musical Experience Questionnaire (ELMEQ; Okely et al., 2021). The ELMEQ is a 30-item measure consisting of four sections that cover playing musical instruments, singing, reading musical notation, and listening to music. The ELMEQ was posted to participants as part of a larger questionnaire booklet that was completed at home prior to attending clinic visits for Wave 5. Following Okely et al. (2021), we used five items from the ELMEQ section on playing musical instruments in the present study; each had five or six response options (listed below in parentheses). The items were number of musical instruments played (0, 1, 2, 3, 4, 5 or more), years of formal training (e.g., school lessons, private lessons, or conservatoire training; 1 or less, 2–5, 6–10, 11–20, 21+), years of regular practice (5 or less, 6–10, 11–20, 21–40, 41+), hours of practice per week during years of regular practice (1 or less, 2–3, 4–6, 7–13, 14+), and performance level reached (beginner, intermediate, advanced, semi-professional, professional). Because participants with no experience of playing a musical instrument did not respond to further items in this section of the questionnaire, we added an additional baseline response category to each item for the purposes of analysis (e.g., 0 years of formal training, 0 hours of practice, and no level of music performance). The distribution of responses to each item are shown in Table S1 in the Supplemental Material available online. For the main analysis, we combined responses to the five ELMEQ items to create a latent variable representing experience of playing a musical instrument. This latent variable was estimated as part of the structural equation model (described in the Analysis section below).
Potentially confounding covariates
We identified years of education, childhood socioeconomic status, and adulthood socioeconomic status (indexed by childhood environment and occupational class, respectively) as variables that might potentially confound the relationship between experience of playing a musical instrument and lifetime change in general cognitive ability (Elpus & Abril, 2019; Ritchie & Tucker-Drob, 2018; Steptoe & Zaninotto, 2020; Theorell et al., 2015; Von Stumm & Plomin, 2015). Importantly, the relationship between these variables and the latent variable (experience of playing a musical instrument) was confirmed in a previous study using LBC1936 data (Okely et al., 2021). The current analysis also accounted for variables associated with more severe age-related cognitive decline, including history of possible dementia, high blood pressure, stroke, diabetes, or cardiovascular disease.
At Wave 1 of the LBC1936 study (age: M = 70 years), participants reported their living conditions in childhood, including the number of people living in their home, the number of rooms in their home (excluding bathroom, toilet, and landings), the number of people sharing toilet facilities, and whether toilet facilities were outdoors. These variables were standardized and then summed to form a composite score of childhood environment, in which higher scores indicated greater environmental deprivation. Participants also reported their age at leaving school, any further and higher education, and details of their highest qualification; these variables were used to calculate years of education. Participants’ main occupation before retirement was also recorded at Wave 1 (age 70). We grouped occupations into six occupational-class categories ranging from “professional” (coded as 1) to “unskilled” (coded as 5), following the Classifications of Occupations system 1980 (Office of Population Censuses and Surveys, 1980). For the purposes of the analysis, the “partly skilled” and “unskilled” categories were combined because these categories had very few cases (n = 9 and n = 2, respectively). Occupational class was treated as a categorical variable and dummy coded for the analysis with “professional” as the reference category. Finally, participants self-reported, at Wave 1 (age 70), whether they had ever been diagnosed with dementia, high blood pressure, stroke, diabetes, or cardiovascular disease. Participants who reported a history of dementia at age 70 or who scored below 24 on the MMSE at that age were categorized as having possible dementia (n = 2).
Analytical sample
The analytical sample included participants who had attempted the ELMEQ (at Wave 5, age 82), had not continued playing a musical instrument between the ages of 70 and 82, 1 and had complete data on the covariates. The process for including participants in the analytical sample is summarized in Figure 1. The final analytical sample included 366 participants; 194 (53.0%) were women. Participants had a mean age of 10.9 years (SD = 0.28) when they first completed the MHT, 69.5 years (SD = 0.85) when they completed the test for a second time, and 82.0 years (SD = 0.47) when they completed the ELMEQ. Participants had a mean of 10.9 years (SD = 1.172) of education, and the majority reported either a professional (22.1%), managerial (39.3%), or skilled nonmanual (23.2%) occupation, indicating a sample with relatively high socioeconomic status. For further details regarding the composition of the analytical sample, see Table 1.
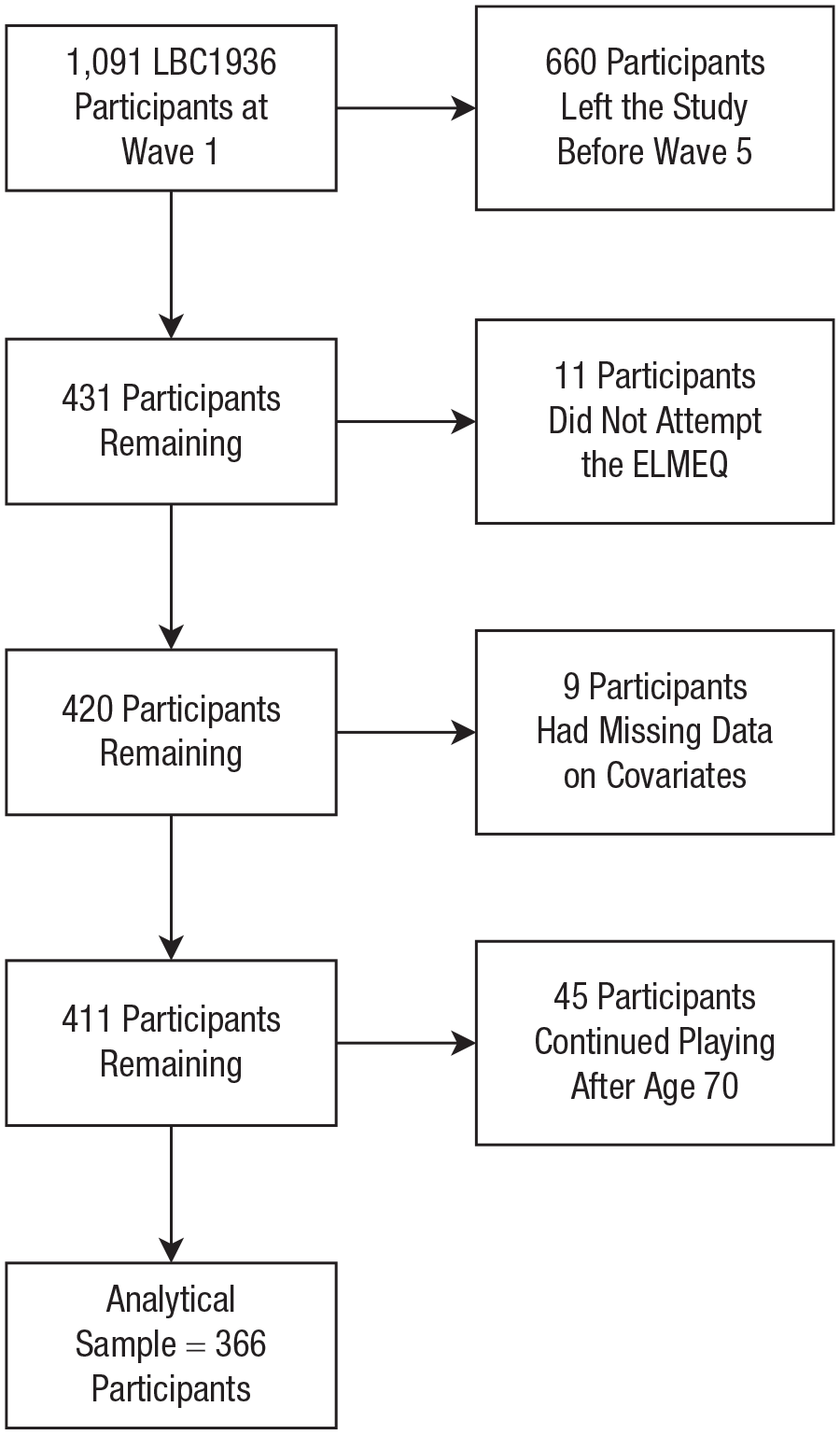
Flow chart showing the process for including participants in the analytical sample. Participants excluded because of missing covariate data had missing data on occupational class (n = 7), possible dementia (n = 1), or childhood environment (n = 1). LBC1936 = Lothian Birth Cohort 1936; ELMEQ = Edinburgh Lifetime Musical Experience Questionnaire.
Characteristics of Participants in the Analytical Sample (Overall) and Grouped According to Whether They Reported Experience of Playing a Musical Instrument
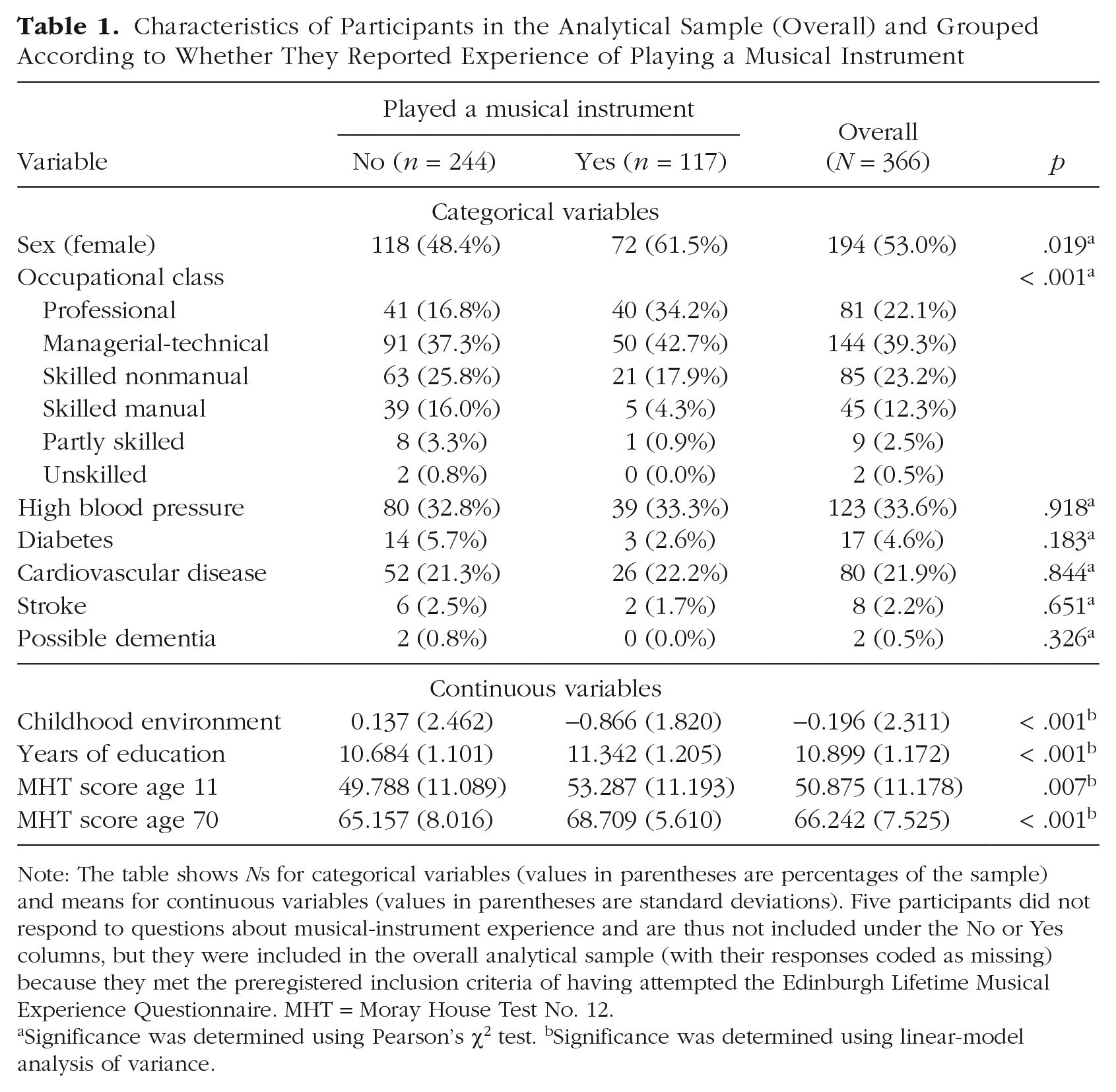
Note: The table shows Ns for categorical variables (values in parentheses are percentages of the sample) and means for continuous variables (values in parentheses are standard deviations). Five participants did not respond to questions about musical-instrument experience and are thus not included under the No or Yes columns, but they were included in the overall analytical sample (with their responses coded as missing) because they met the preregistered inclusion criteria of having attempted the Edinburgh Lifetime Musical Experience Questionnaire. MHT = Moray House Test No. 12.
Significance was determined using Pearson’s χ2 test. bSignificance was determined using linear-model analysis of variance.
The main analysis was conducted using weighted least squares mean and variance-adjusted (WLSMV) estimation. When there are no covariates in the model, this estimator handles missing data using a pairwise-present method; when covariates are included, missingness is allowed to be a function of the observed covariates (Muthén & Muthén, 2017). Participants with missing data on ELMEQ items or missing MHT scores at age 11 or 70 were included in the analytical sample. The number of participants with missing ELMEQ items ranged between 6 and 18 (see Table S1); there were 23 participants with missing MHT scores at age 11 and 2 with missing MHT scores at age 70.
Analysis
First, we described the characteristics of the analytical sample in terms of their responses to the ELMEQ, MHT scores at ages 11 and 70, and the covariates of childhood environment, occupational class, years of education, and disease history. We also compared participants with and without any experience of playing a musical instrument and participants included and excluded from the analytical sample using Pearson’s χ2 tests and linear-model analyses of variance (ANOVAs). Next, we tested for correlations between the five ordinal indicators of experience of playing a musical instrument, MHT scores at ages 11 and 70, and indices of change in MHT between ages 11 and 70; we undertook analyses with both raw change scores (MHT at age 70 – MHT at age 11) and residualized change scores (the residuals from the regression of MHT at age 70 on MHT at age 11). This latter approach resulted in a change score that was independent of MHT score at age 11 (i.e., only variance that was unexplained by MHT at age 11 was left). Note that because these indices of change differ in their method of accounting for initial MHT scores, they can produce different results.
We tested for associations between experience of playing a musical instrument and lifetime change in general cognitive ability using structural equation modeling. As part of this model, which is summarized in Figure 2, a latent variable labeled “lifetime change in MHT score” was estimated using a latent-change-score model (McArdle & Nesselroade, 1994). Lifetime change in MHT score was estimated by setting the autoregression of age-70 MHT score on age-11 MHT score equal to 1 and the loading of lifetime change in MHT score equal to 1. Our model additionally regressed lifetime change in MHT score on age-11 MHT score. Consequently, this latent variable represented the difference between MHT scores at ages 11 and 70, excluding any variance explained by MHT score at age 11. Also, as part of the model, experience of playing a musical instrument was modeled as a latent variable using the five ELMEQ items as ordinal indicators and the marker-variable method of scale setting (fixing the loading of the first indicator to 1). Model fit was assessed using the comparative fit index (CFI), Tucker-Lewis index (TLI), and root-mean-square error of approximation (RMSEA). A CFI and TLI of .95 or more and an RMSEA of .08 or less were considered to indicate acceptable fit.
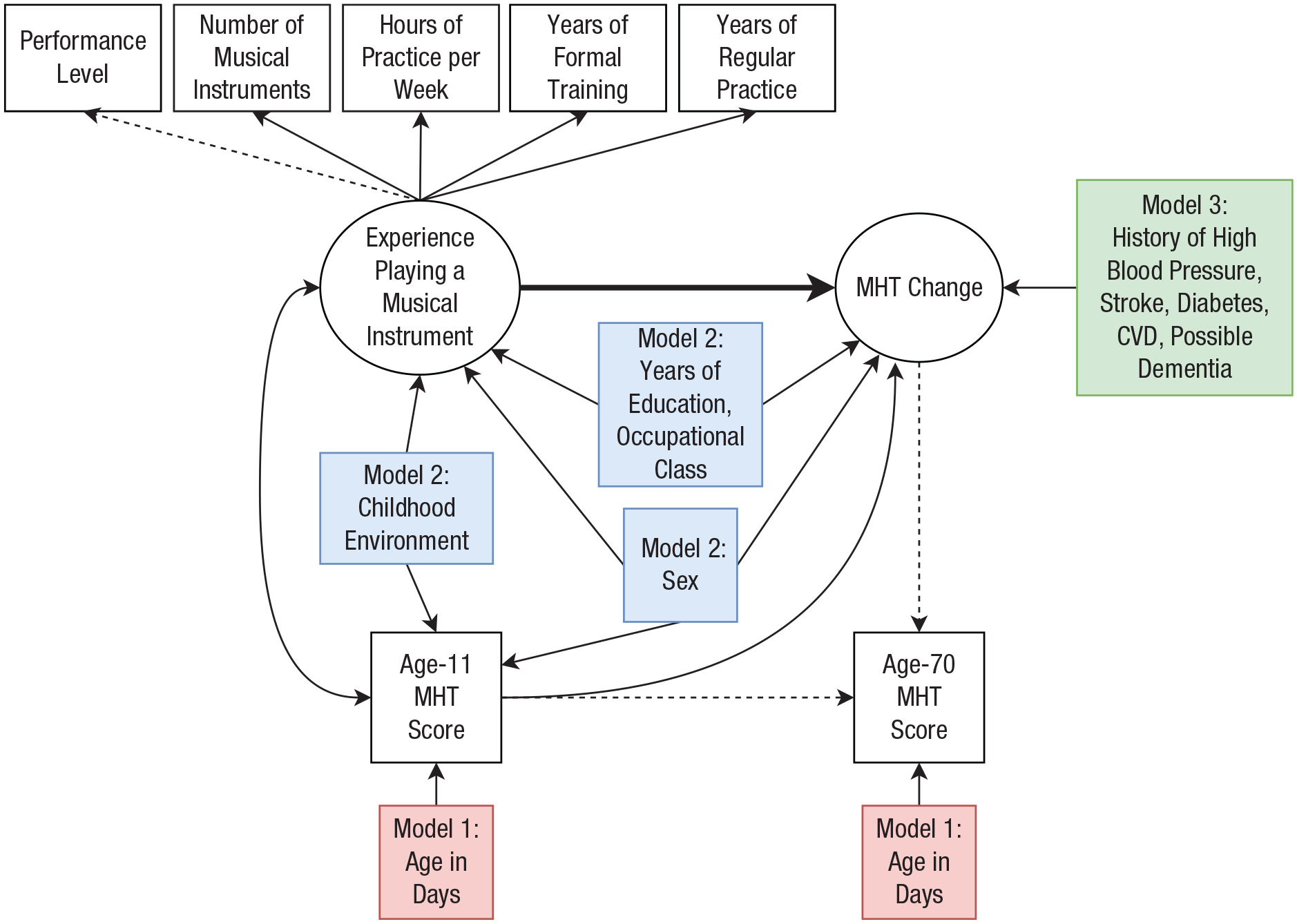
Summary of Models 1, 2, and 3, which tested for an association between experience of playing a musical instrument and lifetime change in Moray House Test No. 12 (MHT) score. Ellipses represent latent variables, rectangles represent observed variables, single-headed arrows represent regression paths or factor loadings, and the double-headed arrow represents covariance. Dashed arrows are fixed at 1 for identification purposes. Covariates were entered in three stages; the diagram shows which additional variables were added at each stage in Models 1, 2, and 3 (shown with red, blue, and green shading, respectively). Participants with possible dementia (n = 2) were excluded from the analytical sample in Model 3. CVD = cardiovascular disease.
The association between experience of playing a musical instrument and lifetime change in MHT score was estimated in three models (see Fig. 2). In Model 1, lifetime change in MHT score was regressed on the latent variable experience of playing a musical instrument and on age-11 MHT score; age-11 MHT score and experience of playing a musical instrument were allowed to covary. This model additionally controlled age-11 and age-70 MHT scores for age in days at time of testing. Model 2 included additional variables that might confound the association between experience of playing a musical instrument and cognitive change. In this model, we specified pathways from the covariates to experience of playing a musical instrument and the MHT variables to reflect expected relationships between these variables (see Subsidiary Analysis (d) in the Supplemental Material for further details). This model additionally controlled experience of playing a musical instrument, age-11 MHT score, and lifetime change in MHT score for sex; experience of playing a musical instrument and age-11 MHT score for childhood environment; and experience of playing a musical instrument and lifetime change in MHT score for years of education and adult occupational class. Model 3 additionally controlled lifetime change in MHT score for age-related diseases known to impact cognitive decline (history of high blood pressure, stroke, diabetes, and cardiovascular disease). Because only two participants were identified as having possible dementia, we removed these participants from the analytical sample (rather than statistically controlling for cases of dementia) in Model 3.
The main analysis was conducted using WLSMV estimation. We report estimates, confidence intervals (CIs), and p values from the standardized model; standardized regression coefficients are used as a measure of effect size. According to recent guidelines for interpreting effect sizes in psychological research, an effect size of 0.10 represents a small effect, 0.20 represents a medium effect, and 0.30 represents a large effect (Funder & Ozer, 2019).
Unless otherwise stated, all analyses were preregistered on OSF before the data were requested (see https://osf.io/r9fbx). The main analysis was conducted using Mplus (Version 8.4; Muthén & Muthén, 2017). Data preparation, management, plotting, and calculation of descriptive statistics were conducted in the R programming environment (Version 3.6.1; R Core Team, 2019).
We did not correct p values for multiple comparisons because our hypothesis focused on a single association between experience of playing a musical instrument and lifetime change in MHT score. However, at a reviewer’s request, we additionally report associations between the covariates and experience of playing a musical instrument and MHT scores, respectively. Because the p values for these associations were not corrected for multiple comparisons, their statistical significance should be interpreted cautiously.
Results
Descriptive statistics
Of the participants included in the sample (N = 366), 117 reported experience of playing a musical instrument and 244 reported no experience (five participants had missing data on this item). A summary of participant responses to the ELMEQ questions (including missing data) is provided in Table S1. Among participants with experience of playing a musical instrument, the most frequent responses reported were one musical instrument played, 2 to 5 years of formal musical training, 0 to 5 years of regular practice, 2 to 3 hr of practice per week during those years, and reaching a beginner level of performance. Participants first started playing a musical instrument at a median age of 10 years (range = 6–62 years) and stopped playing a musical instrument at a median age of 18 years (range = 7–70). Figure 3 shows the age at which each participant who reported any experience of playing a musical instrument first started and stopped playing that instrument (disregarding any breaks).
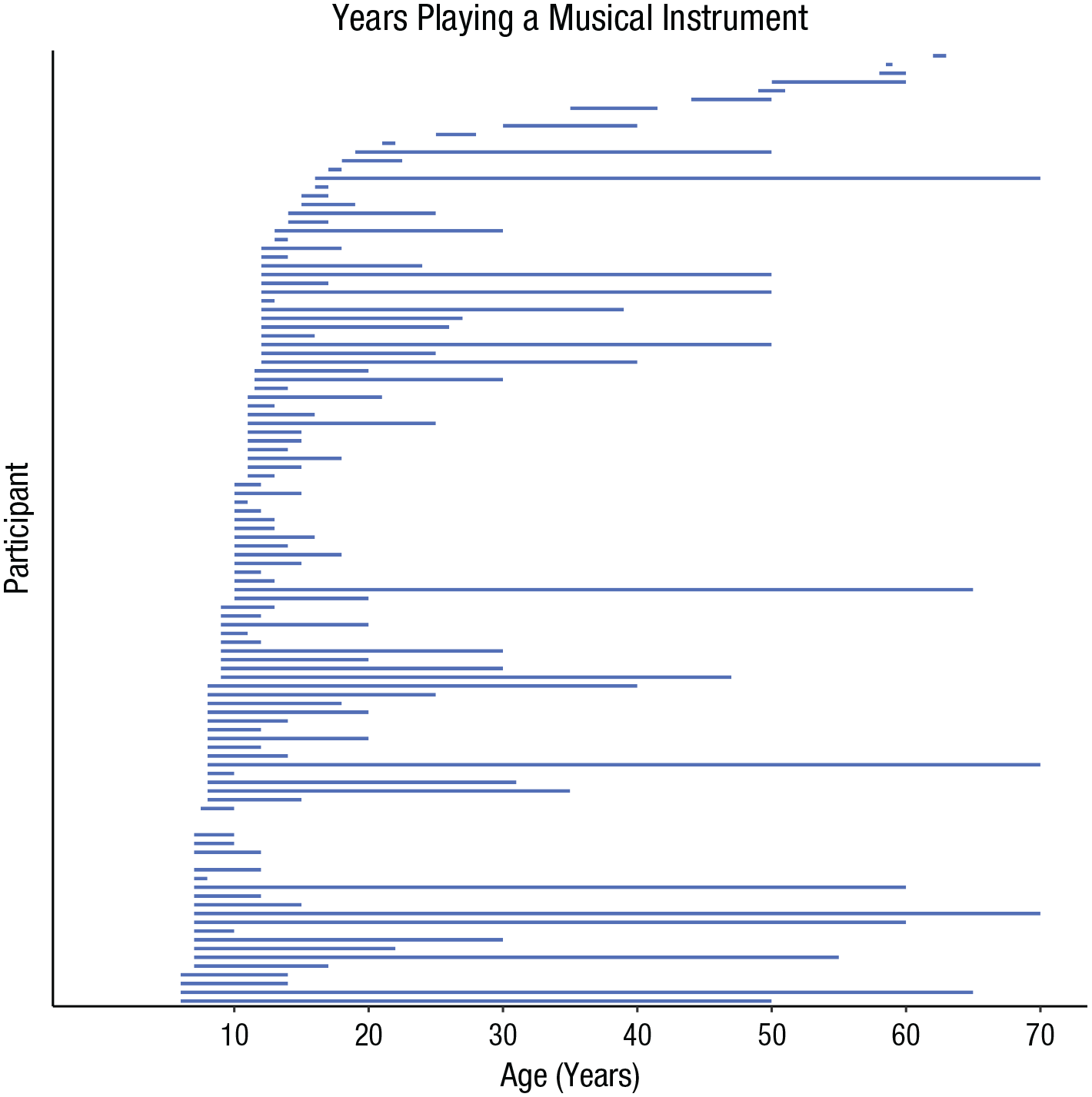
Age at which each participant started and stopped playing a musical instrument, discounting any breaks when the participant did not play. Only participants with complete data on age started and stopped (n = 109) are included; gaps indicate participants who started and stopped at the same age (n = 4).
Table 1 shows the characteristics of participants with and without any experience of playing a musical instrument. On average, participants who reported experience of playing a musical instrument had a significantly higher socioeconomic status in childhood (indicated by a lower score on childhood environment), had more years of education, and were in a more professional occupational class as adults than participants with no experience of playing a musical instrument. Participants with experience of playing an instrument also tended to score significantly higher on the MHT at age 11 and at age 70 than participants with no instrumental experience. No significant differences were found between groups in the prevalence of high blood pressure, diabetes, cardiovascular disease, stroke, or possible dementia. Among both groups (with and without experience of playing a musical instrument), MHT scores were higher, on average, at age 70 than at age 11 (96% of participants’ cognitive performance improved over this time frame).
Table 2 shows correlations between the indicators of experience of playing a musical instrument, MHT scores at ages 11 and 70, and residualized and raw change in MHT scores. There were significant, positive correlations between each of the indicators of experience of playing a musical instrument (number of instruments, years of formal training, years of regular practice, hours of practice per week, and performance level) and MHT score at age 11 (rs = .17–.20) and MHT score at age 70 (rs = .22–.25). Indicators of experience of playing a musical instrument were also positively correlated with residualized change in MHT score (rs = .12–.13) but not with raw change in MHT score. For illustrative purposes, we show the association between performance level reached and residualized change in MHT score in Figure 4. Correlations between performance level reached, MHT scores at ages 11 and 70, and covariates are shown in Table S2 in the Supplemental Material. For brevity, we show only correlations with performance level reached; however, given this variable’s strong correlation with the other indicators of experience of playing a musical instrument (see Table 2), it is likely that similar correlation effects would be observed for all indicator variables. A higher performance level was significantly correlated with a more affluent childhood environment (r =
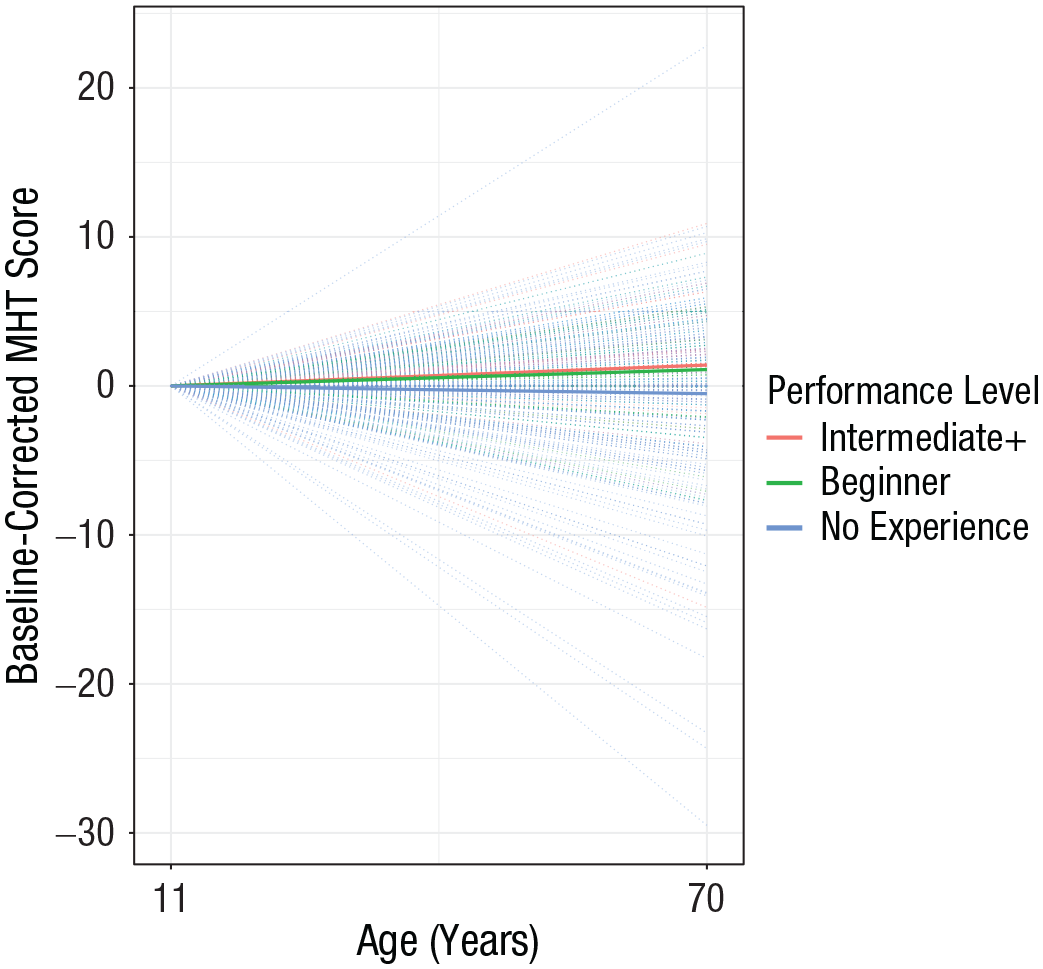
Distribution of baseline-corrected (residualized) Moray House Test No. 12 (MHT) scores at age 70 and mean trajectories of participants at different performance levels. Performance level reached was one of the five indicators of the latent variable used in the main analysis: experience of playing a musical instrument. Dotted lines show individual trajectories for all participants; the three bold lines show mean trajectories of participants grouped into three levels of musical-performance ability. “Intermediate+” includes advanced, semiprofessional, and professional.
Correlation Matrix of Indicators of Experience of Playing a Musical Instrument, Moray House Test No. 12 (MHT) Scores at Ages 11 and 70, and Residualized and Raw Change in MHT Scores
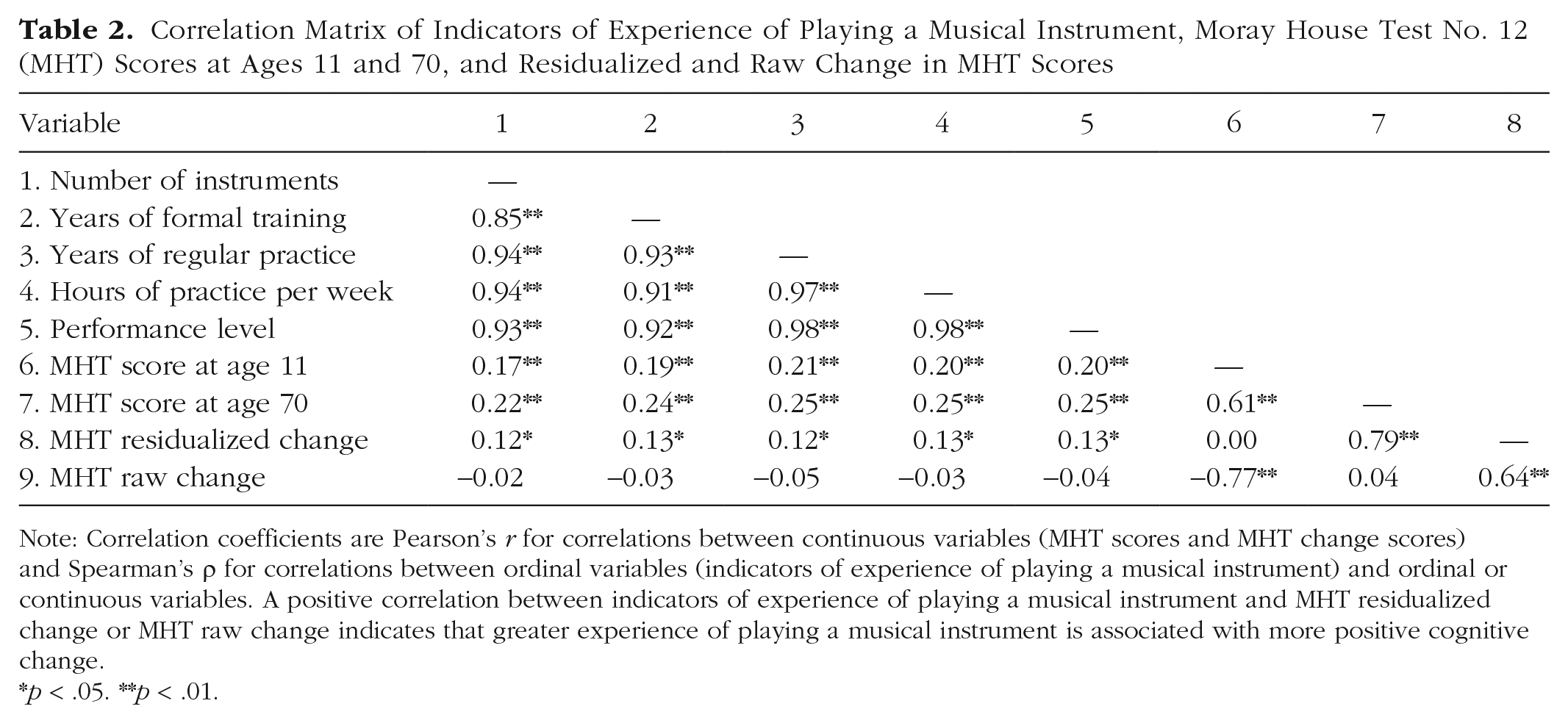
Note: Correlation coefficients are Pearson’s r for correlations between continuous variables (MHT scores and MHT change scores) and Spearman’s ρ for correlations between ordinal variables (indicators of experience of playing a musical instrument) and ordinal or continuous variables. A positive correlation between indicators of experience of playing a musical instrument and MHT residualized change or MHT raw change indicates that greater experience of playing a musical instrument is associated with more positive cognitive change.
p < .05. **p < .01.
Main results
Results from the main analysis (Models 1–3) are displayed in Figure 5 and in Tables S3, S4, and S5 in the Supplemental Material. First, we tested for an association between experience of playing a musical instrument and lifetime change in MHT score without controlling for covariates. This minimally adjusted model (Model 1; controlling only for age at time of testing) fitted the data well (CFI = .999, TLI = .999, RMSEA = .046). Standardized factor loadings for experience of playing a musical instrument ranged between 0.908 and 0.980. In this model, greater experience of playing a musical instrument was significantly associated with more positive lifetime change in MHT score (β = 0.200, 95% CI = [0.111, 0.289], p < .001). Age-11 MHT score was positively correlated with experience of playing a musical instrument (r = .207, p < .001) and negatively associated with lifetime change in MHT score (β = −0.781, 95% CI = [−0.825, −0.737], p < .001). That is, in line with a ceiling-effect interpretation, results showed that participants with a higher MHT score at age 11 experienced less positive change in MHT score (between ages 11 and 70). See Table S3 for the remaining estimates from this model.
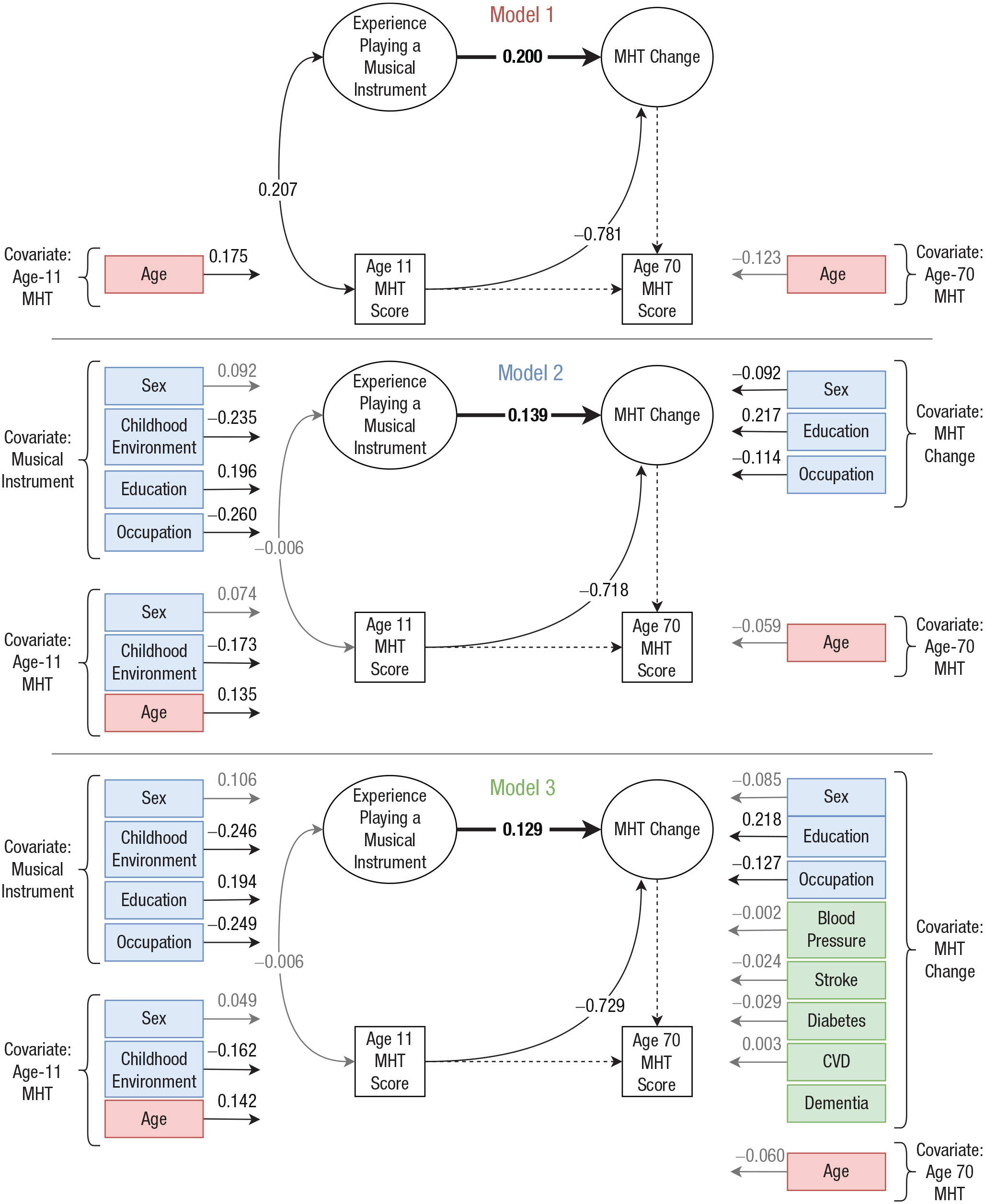
Results from Models 1, 2, and 3, which tested for an association between experience of playing a musical instrument and lifetime change in Moray House Test No. 12 (MHT) score. Ellipses represent latent variables, rectangles represent observed variables, single-headed arrows represent standardized regression paths, and double-headed arrows represent correlations. Dashed arrows are fixed at 1 for identification purposes. Estimates in black are significant (p < .05). The red, blue, and green shading indicates variables that were added in Models 1, 2, and 3, respectively. The estimate in boldface is the association of interest between experience of playing a musical instrument and lifetime change in MHT score. Sex was coded 0 (male) or 1 (female), occupation (i.e., occupational class) shows contrast between 0 (professional) and 1 (skilled manual), higher childhood-environment score indicates greater deprivation, and disease history was coded 0 (no) and 1 (yes). Participants with possible dementia were excluded from the sample in Model 3. CVD = cardiovascular disease.
Next, we controlled the model for covariates that could potentially confound the association between experience of playing a musical instrument and lifetime change in MHT score. Model 2 (additionally adjusting for sex, years of education, adult occupational class, and childhood environment) provided a good fit to the data according to CFI (.992) and TLI (.989) values but had slightly poorer fit according to the RMSEA (.071). The positive association between experience of playing a musical instrument and lifetime change in MHT score was reduced but remained statistically significant (β = 0.139, 95% CI = [0.062, 0.215], p < .001). The correlation between age-11 MHT score and experience of playing a musical instrument was nonsignificant in Model 2 (r = −.006, p = .881). See Table S4 for the remaining parameter estimates from this model.
Finally, in Model 3, we controlled for chronic diseases known to impact cognitive decline to see whether experience of playing a musical instrument was associated with lifetime change in MHT score independently of these established risk factors. This final model additionally controlled lifetime change in MHT score for disease history (high blood pressure, diabetes, cardiovascular disease, and stroke) and excluded participants with possible dementia from the analytical sample (remaining n = 364). In this fully adjusted model, which provided a good fit to the data (CFI = .997, TLI = .996, RMSEA = .035), experience of playing a musical instrument remained significantly associated with lifetime change in MHT score (β = 0.129, 95% CI = [0.049, 0.208], p = .002). See Table S5 for the remaining parameter estimates from this final model.
Figure 5 additionally shows standardized estimates for the associations between the covariates, added in Models 2 and 3, and experience of playing a musical instrument and MHT score (these estimates, together with their respective 95% CIs and p values are also displayed in Tables S4 and S5). Table S6 in the Supplemental Material shows the total effect and the total indirect effect of the covariates on lifetime change in MHT score, estimated in Model 3.
Subsidiary analyses
We carried out nonpreregistered subsidiary analyses to further examine the association between experience of playing a musical instrument and lifetime change in MHT score. Details regarding these analyses and the results are reported in the Subsidiary Analyses section of the Supplemental Material as well as in Table S7. Briefly, to aid our interpretation of the main findings, we reran the analysis (a) removing participants with experience of playing a musical instrument in mid or later adulthood; (b) excluding participants without any experience of playing a musical instrument; (c) replacing the latent variable experience of playing a musical instrument with a binary observed variable indicating whether or not participants had any experience of playing a musical instrument; (d) applying two alternative methods of controlling for covariates; (e) rerunning the main analysis using maximum likelihood estimation with robust standard errors (MLR), which is robust to nonnormality; and (f) rerunning the main analysis including the 45 participants who had continued playing a musical instrument between the ages of 70 and 82. Results from these analyses suggest that the association between experience of playing a musical instrument and lifetime change in MHT score was potentially driven by (a) musical-instrument experience in childhood (not mid or later adulthood) and (b) the contrast between participants with and without any experience of playing a musical instrument (rather than differences between participants with varying levels of musical experience). The association between experience of playing a musical instrument and lifetime change in MHT score, observed in the main analysis, remained statistically significant when we applied alternative methods of controlling for covariates and, separately, the MLR estimator. Results were also similar when we included the 45 participants who reported playing a musical instrument between the ages of 70 and 82.
Discussion
Our results show that experience of playing a musical instrument is positively associated with lifetime change in general cognitive ability (minimally adjusted β = 0.200). The effect size of this association was small but remained statistically significant following adjustment for sex, indicators of childhood and adulthood socioeconomic status, years of education, and disease history (fully adjusted β = 0.129).
The association between experience of playing a musical instrument and positive change in general cognitive ability could, at least partly, represent a causal effect. As described in the introduction, results from intervention studies with children indicate that participation in musical training can result in improved cognitive performance over the short term (e.g., Barbaroux et al., 2019; Moreno et al., 2011; Schellenberg, 2004). Evidence from intervention studies revealing that cognitive advantages resulting from musical training endure over the longer term is currently lacking (Costa-Giomi, 2015). However, findings from cross-sectional observational studies indicate that musical training in childhood is positively associated with cognitive performance in adulthood (Schellenberg, 2006). Results from the present observational longitudinal study provide further support for a long-term positive association between musical training and general cognitive ability.
Cognitive advantages associated with learning to play a musical instrument could also reflect the preexisting characteristics of individuals who engage in this type of training. Importantly, and unusually, we were able to test for potential confounding by childhood cognitive ability, indicators of childhood and adulthood socioeconomic status (namely, childhood environment and adult occupational class), years of education, and disease history. As documented previously with this cohort (Okely et al., 2021), years of education and measures of socioeconomic status were positively associated with experience of playing a musical instrument. Results from models including these demographic variables (Models 2 and 3) suggest that they partly accounted for the association between experience of playing a musical instrument and positive change in general cognitive ability. However, experience of playing a musical instrument continued to make a small unique contribution to predicting change in general cognitive ability in these models (β = 0.129).
Considering the predominance of childhood musical training in our participant sample, it is perhaps most plausible that our findings reflect an association between experience of playing a musical instrument and more positive cognitive development during the childhood years. However, experience of playing a musical instrument might be associated with cognitive change at other life stages, too. There is growing interest in the potential contribution of musical training (earlier in life or during older age) to healthier cognitive aging. In this context, it has been suggested that musical training might contribute to cognitive reserve, potentially slowing rates of cognitive decline in older age (Schneider et al., 2018). Evidence for such an effect is still limited (Schneider et al., 2018); however, our results could, at least potentially, reflect a combined association between experience of playing a musical instrument and (a) more positive cognitive development during childhood and (b) less severe cognitive decline during older age. Further research would be needed to investigate this possibility.
Because of the observational design of the present study, our findings should be interpreted cautiously, and other noncausal explanations should be given careful consideration. For instance, individual genetic variation could potentially play a role. A study with 2,568 twin pairs found that a positive association between music practice and general cognitive ability was largely driven by shared genetic influences (Mosing et al., 2016). Because most LBC1936 participants learned and practiced a musical instrument during childhood, it is also possible that parent characteristics, such as personality or cognitive ability, influenced both participants’ musical engagement (Corrigall & Schellenberg, 2015) and their cognitive development.
Strengths of the present study include the large sample size, the narrow age range of the participant sample, the exceptionally long study period (from age 11 to age 70), and the data available regarding participants’ lifetime musical experience as well as childhood environment, years of education, adult occupational class, and disease history. Limitations of the study should also be considered. As a self-selecting group, LBC1936 participants, on average, have higher cognitive ability and socioeconomic status and are physically healthier than the general population of older people in Scotland (Taylor et al., 2018). The effect of bias related to the composition of the sample is likely to result in some small attenuation of true associations. Furthermore, only six participants in this sample reported reaching an advanced musical-performance level; most participants reported just a few years of beginner-level musical training in their teenage years. This limited our capacity to test whether more advanced experience of playing a musical instrument was associated with increased positive change in general cognitive ability. Nevertheless, this highlights an interesting finding—that in a sample of individuals with mostly high socioeconomic status, even a limited amount of musical training was associated with more positive change in general cognitive ability. In addition, the available data allowed us to test for changes in general cognitive ability rather than specific cognitive-ability domains. The skewed distribution of experience of playing a musical instrument might have biased our results; however, subsidiary analysis with the robust MLR estimator (which provides standard errors that are robust to nonnormality) yielded similar, albeit slightly reduced, estimates (see Subsidiary Analysis (e) in the Supplemental Material). We indexed childhood environment by self-reported household overcrowding and access to toilet facilities, measures that are commonly used to assess socioeconomic status (Galobardes et al., 2006). However, data regarding other potentially confounding variables in childhood, including participation in other nonmusical extracurricular activities and parents’ characteristics (e.g., personality or cognitive ability; Corrigall & Schellenberg, 2015), were not assessed as part of the LBC1936 study and therefore could not be controlled for. In addition, our analysis could not account for the potential influence of genetic variables (Mosing et al., 2016).
To conclude, our findings suggest that experience of playing a musical instrument is associated with a small, long-term cognitive advantage. Further longitudinal studies, including randomized controlled trials, will be needed to establish whether this long-term association is causal and whether the effect is driven predominantly by enhanced cognitive development or by reduced cognitive decline.
Supplemental Material
sj-docx-1-pss-10.1177_09567976221092726 – Supplemental material for Experience of Playing a Musical Instrument and Lifetime Change in General Cognitive Ability: Evidence From the Lothian Birth Cohort 1936
Supplemental material, sj-docx-1-pss-10.1177_09567976221092726 for Experience of Playing a Musical Instrument and Lifetime Change in General Cognitive Ability: Evidence From the Lothian Birth Cohort 1936 by Judith A. Okely, Katie Overy and Ian J. Deary in Psychological Science
Footnotes
Acknowledgements
We thank Barbara Tillmann for her comments on an earlier version of this article.
Transparency
Action Editor: M. Natasha Rajah
Editor: Patricia J. Bauer
Author Contributions
All the authors developed the study concept and design. J. A. Okely analyzed the data and drafted the manuscript. K. Overy and I. J. Deary provided critical revisions. All authors approved the final manuscript for submission.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.