
Abstract
Stress can lead to depression, in part because of activation of inflammatory mechanisms. It is therefore critical to identify resilience factors that can buffer against these effects, but no research to date has evaluated whether psychosocial resilience mitigates the effects of stress on inflammation-associated depressive symptoms. We therefore examined psychosocial resources known to buffer against stress in a longitudinal study of women with breast cancer (N = 187). Depressive symptoms and inflammation were measured over a 2-year period extending from after diagnosis into survivorship. Cancer-related stress and psychosocial resources—social support, optimism, positive affect, mastery, self-esteem, and mindfulness—were measured after diagnosis. As hypothesized, women who reported having more psychosocial resources showed weaker associations between stress and depressive symptoms and weaker associations between stress and inflammation-related depressive symptoms. Results highlight the importance of psychosocial resilience by demonstrating a relationship between psychosocial resources and sensitivity to inflammation-associated depressive symptoms.
Psychological stress is ubiquitous, and its associations with human health are now well established (Cohen et al., 2007). Life stressors (e.g., a cancer diagnosis) and the responses they elicit increase risk for a variety of disorders, including depression—a leading cause of worldwide disability (James et al., 2018). Major life stressors often precede depression (Mazure, 1998; Monroe et al., 2009), and extant theories propose that stress-induced depression vulnerability can be attributed to both cognitive (Beck, 2008) and biological (Slavich & Irwin, 2014) consequences of stress exposure. In particular, psychosocial stressors often produce inflammation (Marsland et al., 2017), and inflammation reliably elicits sickness behaviors that include depressive symptoms (Dooley et al., 2018; Miller, 2009). Moreover, emerging research has now found that stress moderates the link between inflammation and depression such that stressed individuals exhibit more depressive symptoms following inflammatory stimulation (Irwin et al., 2019; Kuhlman et al., 2020). Stress is thus a significant risk factor for depression, and this is in part because stressors can enhance the link between inflammation and depressive symptoms.
Fortunately, although major life stressors commonly precede depression, most individuals do not develop depression after a major stressor (Bonanno et al., 2011; Masten, 2001). Instead, they exhibit resilience, or the ability to maintain healthy levels of psychological and physical functioning following adversity (Bonanno, 2004). Numerous psychosocial resources have been shown to buffer psychological or physiological responses to stress and are consequently hypothesized to promote resilience (Schetter & Dolbier, 2011; Taylor & Stanton, 2007). Indeed, a large literature supports the stress-buffering role of key resources, including social support (Ozbay et al., 2008), optimism (Segovia et al., 2012), mastery (Gallagher et al., 2019), positive affect (Pressman & Cohen, 2005), self-esteem (Buhrmester et al., 2011), and mindfulness (Creswell & Lindsay, 2014). These resilience factors have typically been considered in isolation (e.g., Wiley et al., 2017) or integrated in composite scores that conceptualize resilience factors as intercorrelated effect indicators of a latent resilience construct (e.g., Taylor et al., 2008). This is despite the relatively small amount of variance in outcomes explained by each factor in isolation (Bonanno et al., 2011; Southwick et al., 2014) and the reliable observation that individuals deemed resilient do not endorse a homogeneous set of resources and abilities (Bonanno et al., 2011, 2015). Another approach is to combine psychosocial resources without assuming intercorrelation—similar to allostatic load (Juster et al., 2011). This approach acknowledges that relatively independent psychosocial resources may contribute to resilience and could thereby characterize synergistic effects of psychosocial resources more effectively.
In the present study, we aimed to determine whether key psychosocial resources (social support, optimism, mastery, positive affect, self-esteem, and mindfulness) buffer the interactive effect of stress and inflammation on depressive symptoms. To this end, we analyzed data from a longitudinal study of women with breast cancer (Bower et al., 2020). Examining resilience and depression in this population has high relevance because women with breast cancer face intense stressors in the aftermath of diagnosis and treatment and are at increased risk for depression (Linden et al., 2012). Women recently diagnosed with early-stage breast cancer completed measures of depressive symptoms and inflammation before (Time 1) and after (Time 2) treatment and at three posttreatment follow-ups (Times 3–5). Cancer-related stress and resilience factors (i.e., social support, optimism, mastery, self-esteem, positive affect, and mindfulness) were measured before treatment (Time 1). In a previous study with this sample (Manigault et al., 2021), we found that stress was associated with depression and also moderated the association between inflammation and depression, such that women who reported higher levels of cancer-related stress were more depressed and more susceptible to inflammation-associated depressive symptoms. The goal of the current study was to determine whether a composite measure of resilience would buffer these effects. We hypothesized that women who scored higher on the composite index of psychosocial resilience would exhibit (a) reduced associations between stress and depressive symptoms and (b) a weakened interactive effect of stress and inflammation on depressive symptoms.
Statement of Relevance
Our understanding of the etiology of depression has evolved to consider how inflammation and stress can interact to increase depression risk. This progress has been largely driven by preclinical studies demonstrating that stressed animals show enhanced effects of peripheral inflammation on the brain. Building on this literature, psychologists are in a unique position to address how psychological and social factors that are distinctly human may protect against these stress-related effects. The present study examined psychosocial resources known to buffer against stress—social support, optimism, mastery, positive affect, self-esteem, and mindfulness—in a sample of women facing the stress of breast-cancer diagnosis, treatment, and recovery. We found that women who had more of these resources were less susceptible to stress-related depression; even when inflammation was elevated, they did not report higher levels of depression. Results highlight the importance of psychosocial resilience by demonstrating a relationship between psychosocial resources and sensitivity to inflammation-associated depressive symptoms.
Method
Participants
Women recently diagnosed with early-stage breast cancer were recruited from oncology practices in the Los Angeles, California, area as part of a larger study (the Research on Inflammation, Stress, and Energy [RISE] study) examining cancer-related fatigue (Bower et al., 2019, 2020). Recruitment occurred between January 2013 and July 2015. Eligibility criteria included (a) being newly diagnosed with early stage (I–IIIA) breast cancer, (b) having yet to begin adjuvant or neoadjuvant treatment regiments (including chemotherapy, radiation therapy, or endocrine therapy), and (c) English proficiency. A total of 270 women provided written consent and were enrolled in the study. Sample size was determined on the basis of the recruitment objectives of the parent study (Bower et al., 2019, 2020). All procedures were approved by the University of California, Los Angeles (UCLA) Institutional Review Board.
Procedure
Participants completed up to five assessments over the study period, which extended from after diagnosis into survivorship. At each assessment, participants provided blood samples (used for immune assessment) and completed online questionnaires. All participants completed a postdiagnosis assessment (Time 1), which took place before the start of adjuvant or neoadjuvant treatment; of note, 91% of enrolled women had already undergone surgery (lumpectomy or mastectomy) before the postdiagnosis assessment. Women who received chemotherapy and/or radiation therapy were invited to complete a posttreatment assessment (Time 2), and all participants were invited to complete follow-up assessments at 6, 12, and 18 months after treatment (Times 3–5, respectively). The RISE study achieved high retention, with 254 completing the Time 3 assessment, 246 completing the Time 4 assessment, and 244 completing the Time 5 assessment (Bower et al., 2020). The analytical sample for the current study included participants who provided at least two valid blood samples (a necessary condition for analyses described below) and thus comprised 187 women.
Measures
Depressive symptoms and inflammation were measured during each visit (Time 1–Time 5); cancer-related stress and all resilience factors were measured after diagnosis (Time 1).
Depressive symptoms
Depressive symptoms were measured using the 20-item Center for Epidemiologic Studies-Depression (CES-D) scale (Radloff, 1977). This scale examines cognitive, affective, and somatic symptoms of depression by asking participants to rate how often they experienced each scale item (e.g., “I felt sad”) over the past week on a 4-point scale ranging from 0 to 3. Scores were summed; higher CES-D scores indicate greater self-reported depression. The CES-D scale has demonstrated good internal consistency and test-retest reliability in cancer samples (Hann et al., 1999).
C-reactive protein
Blood samples were collected for assessment of C-reactive protein (CRP). The collection of blood samples typically took place before noon and was scheduled to coincide with clinic visits. CRP was chosen to index inflammation because it is an established marker of systemic inflammation that is reliably elevated in depressed samples (Osimo et al., 2020), longitudinally associated with depressive symptoms (Valkanova et al., 2013), and associated with risk for de novo depression (Pasco et al., 2010). CRP also exhibits higher temporal stability than proinflammatory cytokines, such as interleukin-6 (Pepys & Hirschfield, 2003; Whiteside, 1994). Blood samples were collected by venipuncture, processed, and then stored at −80 °C in the Inflammatory Biology Core Laboratory at the Cousins Center for Psychoneuroimmunology (UCLA) until assayed. Circulating plasma levels of CRP were quantified using Human Quantikine enzyme-linked immunosorbent assays (R&D Systems, Minneapolis, MN); the assay lower limit was 0.2 mg/L. Samples were assayed in duplicate and averaged. Interassay and intraassay coefficients of variation were low (4.6% and 1.8%, respectively).
Cancer-related stress
The seven-item intrusion subscale of the Impact of Event Scale (IES; Horowitz et al., 1979) was used as a measure of cancer-related stress. The IES is a measure of subjective distress caused by a specific traumatic event and has been used to measure cancer-related stress (Dupont et al., 2014; Salsman et al., 2015). Participants were presented with statements (e.g., “I thought about it when I didn’t mean to”) and asked to indicate (using a scale ranging from 0 to 5) “how frequently these comments were true for you during the past seven days with regard to your breast cancer.” We chose to focus on this stress measure because it was found to be the strongest moderator of the association between inflammation and depressive symptoms in this sample (Manigault et al., 2021).
Resilience factors
Social support
Social support was assessed using the attachment subscale of the Social Provisions Scale (Cutrona et al., 1986). The four items included in this subscale query participants’ perception of having close relationships with other people (e.g., “I do not have a feeling of closeness with anyone”). Participants indicated how much they agreed with each item on a 4-point scale; scores were summed. Greater scores indicate higher levels of social support.
Optimism
The revised Life Orientation Test (LOT-R) was used to measure optimism (Scheier et al., 1994). The LOT-R prompts participants to rate the degree to which they agree with six statements pertaining to expecting positive outcomes (e.g., “In uncertain times, I usually expect the best”). Responses were made on a 5-point scale. LOT-R scores were summed; greater scores indicate higher levels of optimism.
Mastery
The Pearlin-Schooler Mastery Scale was used to measure mastery (Pearlin & Schooler, 1978). This scale is composed of seven items pertaining to perceptions of control over life events (e.g., “What happens to me in the future mostly depends on me”). Each item is rated on a 4-point scale. Scores were summed; greater PSMS scores indicate higher levels of mastery.
Self-esteem
Self-esteem was measured using the 10-item Rosenberg Self-Esteem Scale (Rosenberg, 1965). Participants rated statements pertaining to self-perceptions (e.g., “I feel that I have a number of good qualities”) on a 4-point scale. Scores were summed; greater scores indicate higher self-esteem.
Positive affect
Positive affect was assessed using the 10-item Positive Affect subscale of the Positive and Negative Affect Schedule (PANAS; Watson et al., 1988). Participants were presented with 10 words describing positive emotions (e.g., “inspired”) and rated the degree to which they “felt this way over the past week” on a 5-point scale. Scores on this scale were summed; greater scores indicate more positive affect.
Trait mindfulness
Trait mindfulness was measured using the Mindful Attention Awareness Scale (Brown & Ryan, 2003). This scale measures trait mindfulness with 15 items pertaining to receptive awareness and attention to present-moment experiences (e.g., “I find myself doing things without paying attention”). Participants rated the frequency of experiencing each scale item on a 6-point scale. Scores were averaged; higher scores indicate greater trait mindfulness.
Demographic and medical characteristics
Demographic statistics (age and race), physical condition (body mass index [BMI]), cancer (disease stage), and treatment characteristics (chemotherapy, radiation therapy, and endocrine therapy) were used as covariates because of their potential to influence depressive symptoms and inflammation (O’Connor et al., 2009). Endocrine therapies included aromatase inhibitors, selective estrogen receptor modulators (e.g., tamoxifen), and gonadal-suppression therapy. Age and race were self-reported. Clinic staff measured height and weight for determination of BMI. Medical records were used to determine cancer and treatment characteristics.
Analytic plan
Computation of the index of psychosocial resilience
Few studies have evaluated joint effects of psychosocial resources (Schetter & Dolbier, 2011), and best practices for combining psychosocial-resilience measures into a composite index are not yet established. We considered multiple methods and ultimately chose to dichotomize psychosocial-resource measures and sum the resulting binary values such that scores could range from 0 to 6, reflecting greater perceived availability of psychosocial resources. This choice produced an index of psychosocial resilience that made no assumptions about the underlying distribution of psychosocial resources or their degree of intercorrelation.
We generated binary variables using cutoffs intended to separate the lower tail of a given distribution from its upper bulk (i.e., similar to using the 25th percentile). This is because raw-score distributions were typically negatively skewed (with most participants endorsing high levels of each resource), consistent with the observation that resilience is relatively common (Masten, 2001). More specifically, cutoffs were empirically derived using an R function that locates the largest positive increase in raw-score density and returns the integer immediately preceding this increase (for a reproducible example of this method applied to random data, see the R script in the Supplemental Material available online). This approach has the advantage of producing a unique cutoff for each measure that is empirically derived (rather than relying on a single arbitrary cutoff). Figure S1 in the Supplemental Material illustrates how the function-derived cutoffs performed relative to cutoffs corresponding to the 25th percentile; resilience indices computed using each approach (function derived vs. 25th-percentile cutoff) were highly correlated (r = .84).
Modeling
Repeated measurements of depressive symptoms were modeled using robust multilevel models via the robustlmm package (Version 2.3; Koller, 2016) in R (Version 4.0.3; R Core Team, 2020). Repeated study assessments (Level 1) were nested within individuals (Level 2) to yield two-level models. Cancer-related stress, levels of the index of psychosocial resilience, and their interaction were entered as Level 2 fixed effects. These predictors were used to examine whether resilience buffered associations between stress and depression. To examine whether resilience buffered associations between stress, depression, and inflammation, we entered person-centered CRP as a Level 1 fixed effect and allowed it to interact with Level 2 fixed effects. CRP values were natural log transformed and centered relative to Level 2 units (i.e., persons; Enders & Tofighi, 2007), which required at least two valid CRP values. Accordingly, positive person-centered CRP values indicate that CRP levels (at a given assessment) exceeded average levels across assessments (for a given person). Significant higher order interactions were followed up with tests of nested interactions and simple slopes in which recentering was carried out—that is, contrasting low (−1 SD), average (mean), and high (+1 SD) levels of predictors.
In secondary analyses, the same analytic strategy was repeated to test the moderating effects of each individual’s resilience factors (i.e., social support, trait mindfulness, optimism, mastery, self-esteem, and positive affect). Holm’s procedure (Holm, 1979) was used to limit familywise Type I error rates to 5%, but its application did not influence the results. Effect-size estimates (βs) were obtained by standardizing continuous predictor and criterion variables prior to analyses (Lorah, 2018). Plots were created using sjPlot (Version 2.1; Lüdecke, 2018). Reported analyses include covariate measures (i.e., age, race, BMI, cancer stage, receipt of chemotherapy, receipt of radiation therapy, receipt of endocrine therapy) as Level 2 fixed effects (mean centered or centered on the most frequently endorsed category). Excluding covariate measures from final models did not influence the results. Furthermore, controlling for comorbidities (as indexed by the Charlson Comorbidity Index; Charlson et al., 1987) and antidepressant-medication use did not influence the results.
Secondary analyses
Inclusion of behavioral factors in the index of psychosocial resilience
Our primary aim in the present study was to evaluate how psychological and social factors may buffer associations between stress, inflammation, and depressive symptoms. Accordingly, our primary measure of resilience did not include behavioral factors such as physical activity, sleep, and nutrition, despite the potential impact of these factors on resilience (Laird et al., 2019; Schetter & Dolbier, 2011). Secondary analyses were conducted to broaden the scope of the index of psychosocial resilience to include behavioral factors relevant for depression and neuroimmune interactions (Bower et al., 2019), specifically physical activity and sleep disturbance (fully reported in the Supplemental Material).
Alternate methods for computing the index of psychosocial resilience
We interpret the extant literature to indicate that relatively independent psychosocial resources may contribute to resilience (Bonanno et al., 2011, 2015), and this guided our approach to computing the index of psychosocial resilience in primary analyses. However, psychosocial resources have also been conceptualized as intercorrelated effect indicators of a latent resilience construct (e.g., Taylor et al., 2008), which would suggest a different analytic approach. Thus, we also used principal components analysis (PCA) to compute the index of psychosocial resilience and conducted additional analyses to determine whether this approach altered the primary results of the study (fully reported in the Supplemental Material). Of note, computing the index using PCA methods also involves making notable assumptions regarding the distribution (i.e., normality) and synergistic effects of psychosocial measures (i.e., low scores in a given resource can be averaged out by high scores on other resources).
Results
Sample characteristics
Demographic and clinical characteristics of the final analytical sample are presented in Table 1. Women in the present sample were primarily middle aged, college educated, White, and married and most reported annual household incomes above $100,000. These women most often presented with Stage 0 or I breast cancer that was treated with lumpectomy and radiation therapy, and most also received endocrine therapy. Over the study period, women reported depressive symptoms that were below the clinical threshold of 16 but elevated relative to community-dwelling older adults (Lewinsohn et al., 1997). Finally, the majority of women indicated on our composite index that they had at least four resilience resources.
Demographics and Clinical Characteristics of the Final Sample (N = 187)
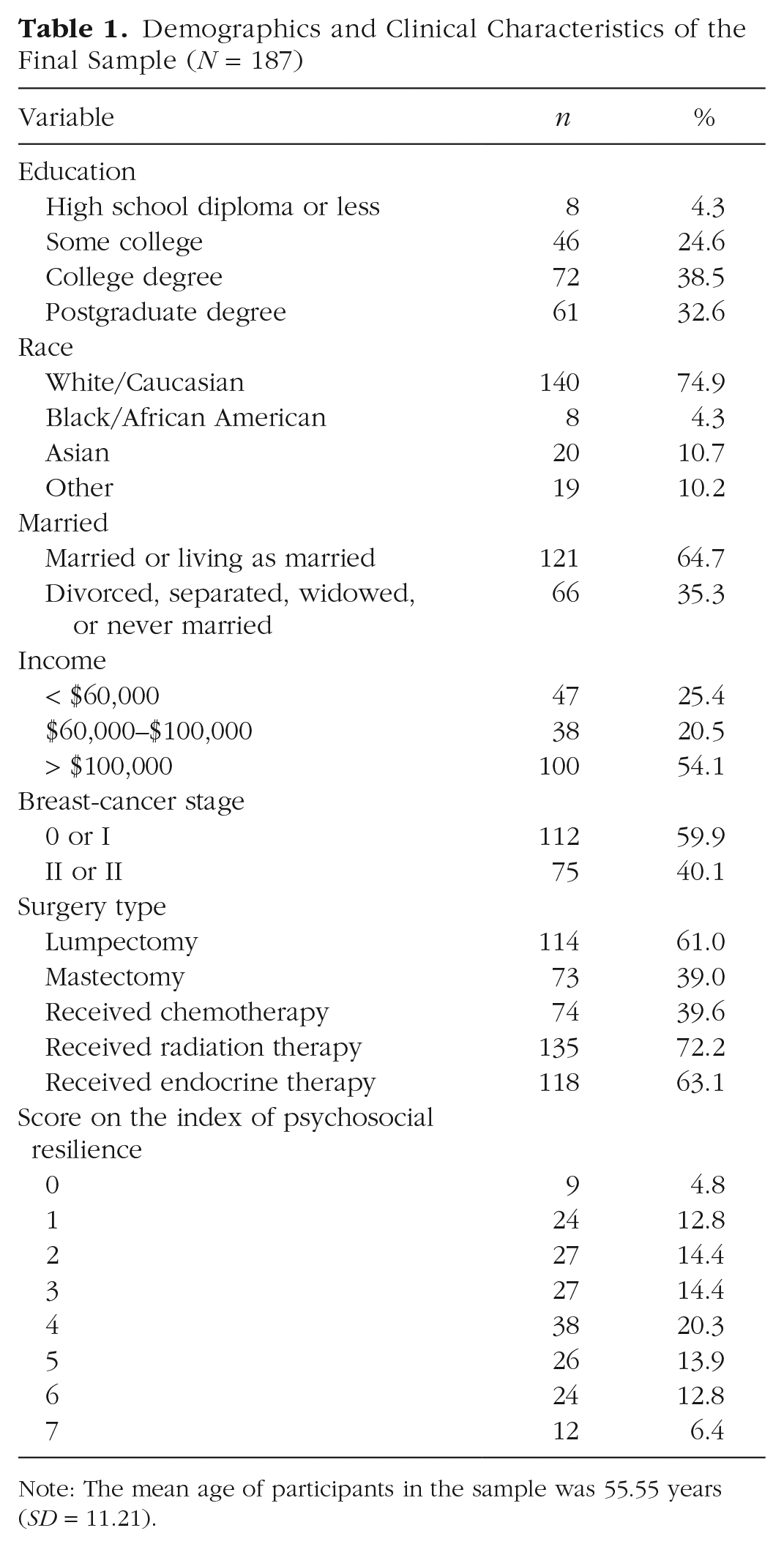
Note: The mean age of participants in the sample was 55.55 years (SD = 11.21).
Associations between initial levels of depression, CRP, stress, and resilience factors
Descriptive statistics and zero-order correlations of depressive symptoms, CRP, cancer-related stress and resilience measures at the initial assessment (Time 1) are presented in Table 2. Consistent with a prior publication of these data (Manigault et al., 2021), our results showed that Time 1 depressive symptoms were negatively correlated with Time 1 optimism, mastery, self-esteem, and mindfulness. Furthermore, Time 1 depressive symptoms were positively correlated with cancer-related stress and negatively correlated with the index of psychosocial resilience as well as Time 1 social support and positive affect. Resilience factors were all positively correlated with the index of psychosocial resilience (rs = .47–.79) and one another (rs = .15–.66).
Descriptive Statistics and Zero-Order Correlations at the Initial (Time 1) Assessment
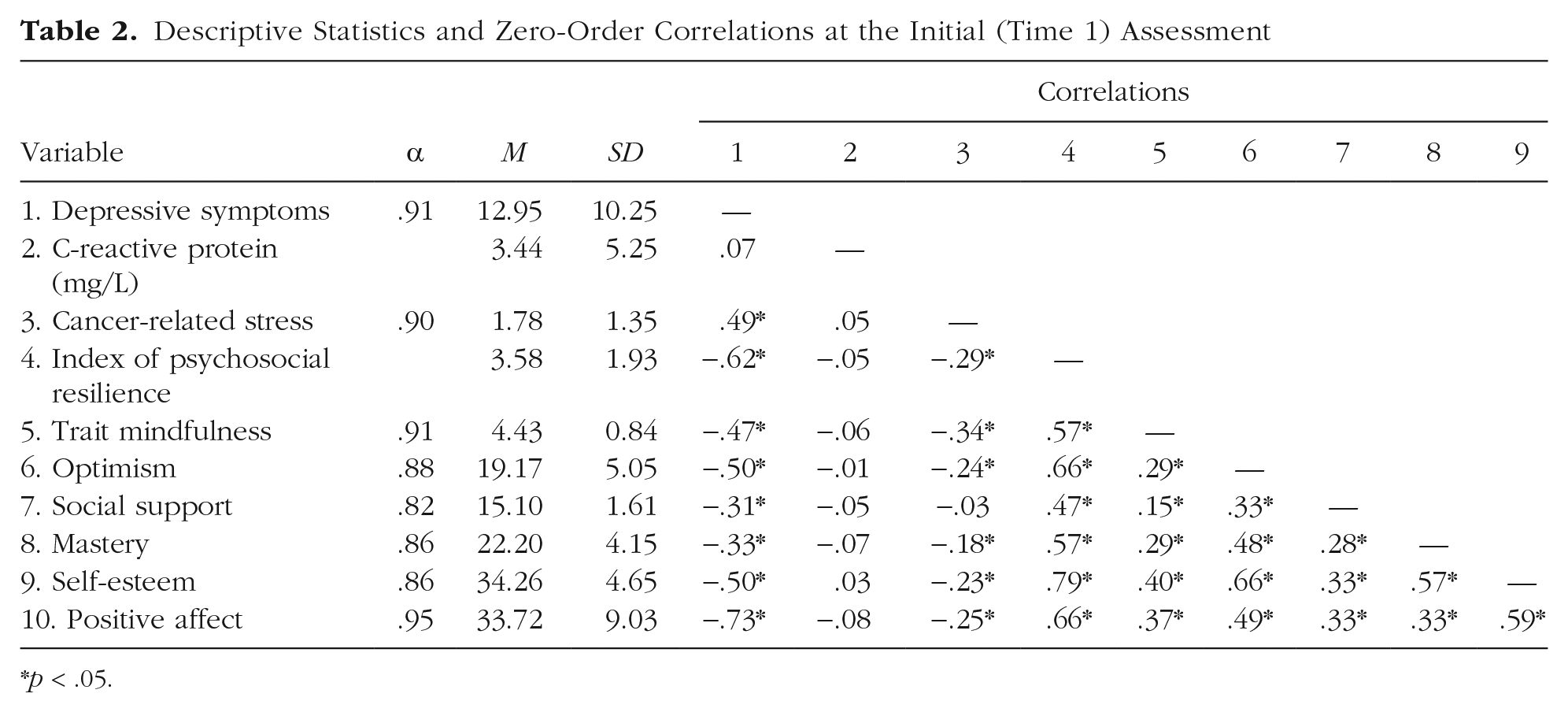
p < .05.
Resilience buffers the link between stress and depressive symptoms
Postdiagnosis cancer-related stress was positively associated with depressive symptoms across the study period, b = 1.90, SE = 0.42, β = 0.23, t(172) = 4.56, p < .001. In the present study, we aimed to test the hypothesis that resilience would buffer this association. As hypothesized, a two-way interaction between cancer-related stress and index of psychosocial resilience was found, b = −0.42, SE = 0.17, β = −0.092, t(222) = 2.48, p = .014, showing that resilience buffered the association between cancer-related stress and depressive symptoms. More specifically, cancer-related stress was positively associated with depressive symptoms at low and average levels of the index of psychosocial resilience, b = 1.75, SE = 0.42, β = 0.217, t(186) = 4.19, p < .001, and b = 1.01, SE = 0.34, β = 0.124, t(170) = 2.99, p = .003, respectively. By contrast, cancer-related stress and depressive symptoms showed no significant associations among individuals who scored high on the index of psychosocial resilience (p > .05). See Figure 1 for a graphical representation of this interaction.
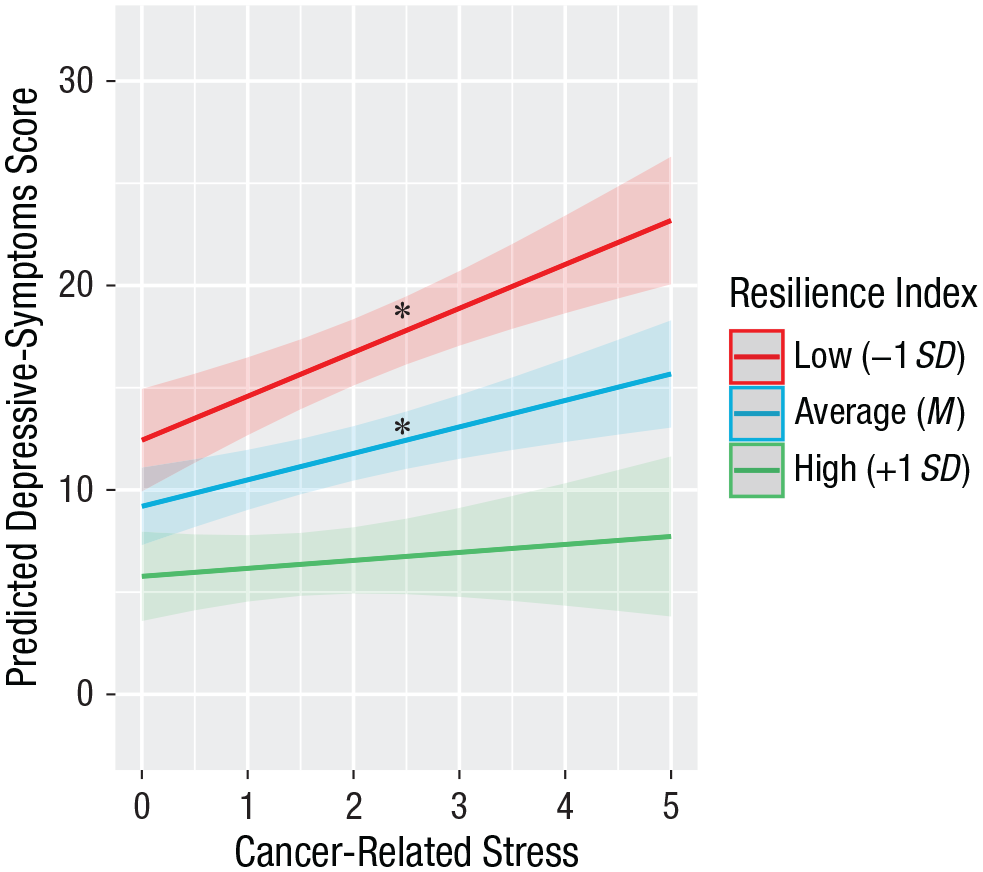
Predicted depressive-symptoms score as a function of cancer-related stress and score on the index of psychosocial resilience. Simple slopes depicted were obtained by recentering the index of psychosocial resilience on low (−1 SD), average (mean), and high (+1 SD) values. Predicted depressive-symptom scores were adjusted for age, body mass index, race, surgery, cancer stage, and treatment characteristics (chemotherapy, radiation therapy, and endocrine therapy). Shaded areas depict confidence intervals. Asterisks indicate statistically significant slopes (p < .05).
Examining resilience factors individually revealed an identical pattern of results for social support and mastery, b = −0.58, SE = 0.21, β = −0.121, t(182) = 2.73, p = .007, and b = −0.27, SE = 0.09, β = −0.150, t(170) = 3.18, p = .002, respectively. Cancer-related stress was positively associated with depressive symptoms only when social support and mastery were low, b = 2.87, SE = 0.52, β = 0.357, t(178) = 5.59, p < .001, and b = 2.50, SE = 0.51, β = 0.309, t(168) = 4.92, p < .001, respectively, or when social support and mastery were average, b = 1.91, SE = 0.39, β = 0.236, t(171) = 4.91, p < .001, and b = 1.28, SE = 0.39, β = 0.159, t(170) = 3.30, p = .001, respectively. By contrast, the association between cancer-related stress and depression was not moderated by trait mindfulness, optimism, self-esteem, or positive affect (all ps > .05).
Resilience buffers the link between stress, inflammation, and depressive symptoms
The present study also tested the hypothesis that the index of psychosocial resilience would buffer the association between stress, inflammation, and depressive symptoms. We have previously shown that CRP was positively associated with depressive symptoms only among women who reported high levels of cancer-related stress in this sample (Manigault et al., 2021). As hypothesized, greater resilience buffered against stress effects on the association between inflammation and depressive symptoms (see Fig. 2). More specifically, a three-way interaction among CRP, cancer-related stress, and the index of psychosocial resilience was found, b = −0.27, SE = 0.13, β = −0.038, t(611) = 2.19, p = .029. The two-way interaction between CRP and cancer-related stress was significant among women who scored low or average on the index of psychosocial resilience, b = 1.22, SE = 0.27, β = 0.096, t(611) = 4.53, p < .001, and b = 0.74, SE = 0.22, β = 0.059, t(610) = 3.32, p = .001, respectively, but not among women who scored high on the index of psychosocial resilience, b = 0.26, SE = 0.35, β = 0.020, t(610) = 0.74, p = .46. Tests of simple slopes revealed that CRP was positively associated with depressive symptoms when cancer-related stress levels were high and scores on the index of psychosocial resilience were low, b = 2.21, SE = 0.49, β = 0.138, t(611) = 4.56, p < .001, or when cancer-related stress levels were high and scores on the index of psychosocial resilience were average, b = 1.26, SE = 0.42, β = 0.078, t(610) = 3.00, p = .003. All other tests of simple slopes were nonsignificant (all ps > .05). Examining resilience factors individually revealed no significant three-way interactions (all βs between −0.027 and 0.004; all ps > .05).
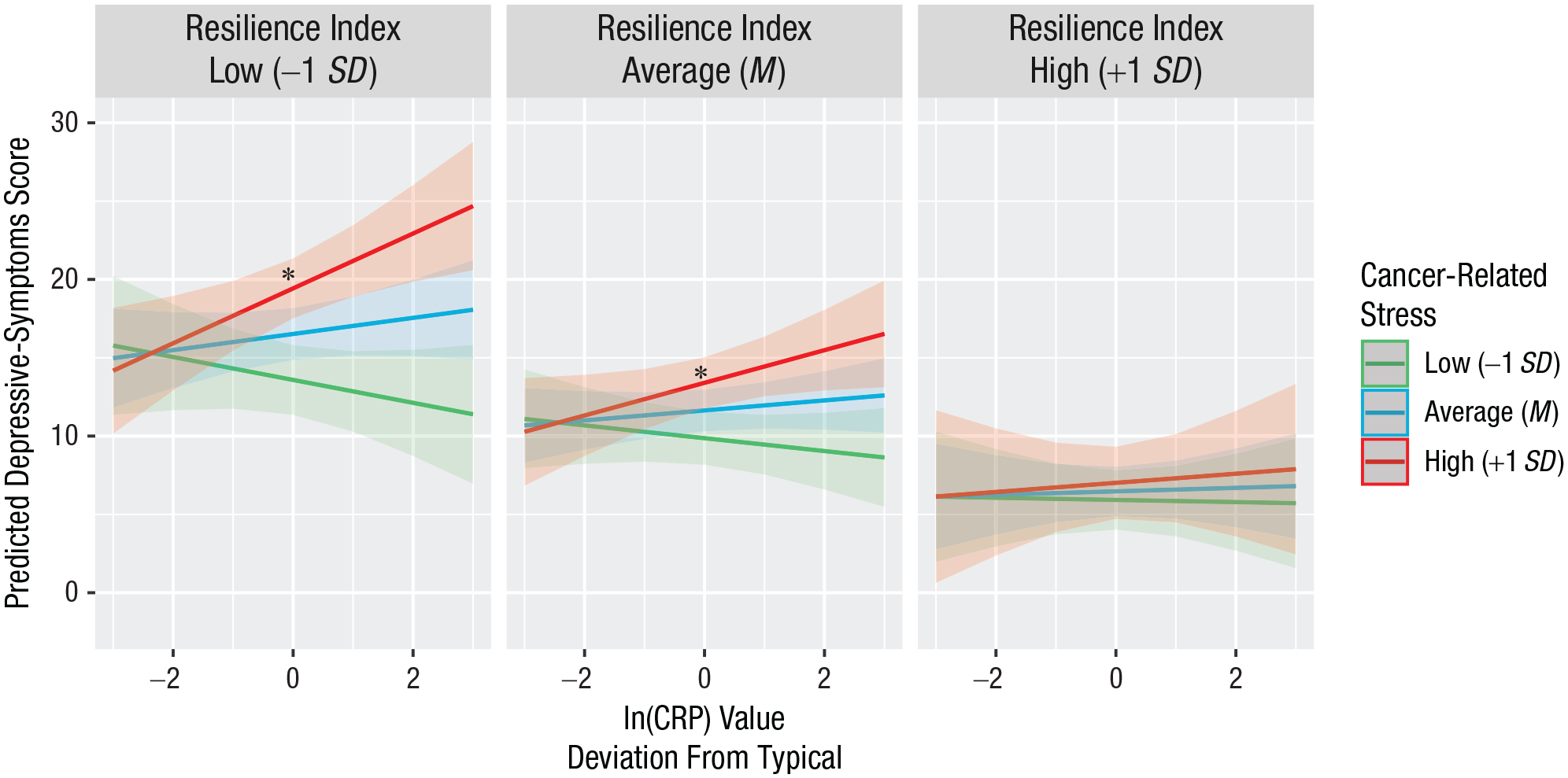
Predicted depressive-symptoms score as a function of person-centered C-reactive protein (CRP), and cancer-related stress, separately for participants with low, average, and high scores on the index of psychosocial resilience. Simple slopes depicted were obtained by recentering the index of psychosocial resilience and cancer-related stress on low (−1 SD), average (mean), and high (+1 SD) values. Predicted depressive-symptom scores were adjusted for age, body mass index, race, surgery, cancer stage, and treatment characteristics (chemotherapy, radiation therapy and endocrine therapy). Shaded areas depict confidence intervals. Asterisks indicate statistically significant slopes (p < .05).
Secondary analyses
Secondary analyses (fully reported in the Supplemental Material) revealed that including a measure of physical activity and sleep in the index of psychosocial resilience showed the same pattern of results as primary analyses and that both physical activity and sleep predicted susceptibility to inflammation-associated depressive symptoms on their own. Furthermore, tests of primary hypotheses were not supported when the index of psychosocial resilience was computed using a PCA approach.
Discussion
Stress can lead to depression, in part because stressors can enhance mechanisms via which peripheral inflammation produces depressive symptoms (Slavich & Irwin, 2014). Resilience factors may protect against these stress-related effects, but no research to date has evaluated whether psychologically resilient individuals are less sensitive to the interactive effects of stress and inflammation on depressive symptoms. The present study tested this hypothesis in women who face the psychological and physical stress of breast-cancer diagnosis and treatment. As hypothesized, women who reported having numerous psychosocial resources known to buffer against stress (i.e., who scored higher on the composite index of psychosocial resilience) exhibited weakened associations between stress and depressive symptoms. Moreover, women who scored higher on the composite index of psychosocial resilience exhibited weaker associations between stress and inflammation-associated depressive symptoms. The present study thus demonstrates the relevance of psychosocial resilience factors for understanding stress- and inflammation-associated depression risk. In addition, the present study adds to a growing literature illustrating how varied psychosocial resources may synergistically contribute to psychosocial resilience.
Novel pathways linking stress to depression are being discovered, but the potentially protective role of psychosocial resilience within such pathways remains understudied. In particular, recent work has found that stress could increase depression risk by enhancing the effects of peripheral inflammation on the brain (Slavich & Irwin, 2014). This mechanism is supported by preclinical work suggesting that multiple neuroimmune communication routes are enhanced in stressed animals (Dudek et al., 2020; Menard et al., 2017; Wohleb et al., 2016) and illustrated by recent experiments in which stressed adults exhibited greater depressed mood in response to inflammatory stimulation (Irwin et al., 2019; Kuhlman et al., 2020). Yet relatively little research to date has evaluated how these stress-related effects may be buffered among resilient individuals. Notable preclinical work has investigated biological mechanisms of resilience (Cathomas et al., 2019; Russo et al., 2012), but this work has not addressed how psychosocial factors that are unique to humans could be protective. Contributing to this literature, the present study found that among individuals who have more numerous psychosocial resources known to act as stress buffers, cancer-related stress no longer enhanced the association between inflammation and depressive symptoms. Psychosocial resilience factors may therefore play an important role in protecting individuals from inflammation-associated depressive symptoms under conditions of high stress.
Results also suggest that identifying individuals who are most likely to exhibit resilience to stress-related depression is complex. Tests of primary hypotheses were supported using a resilience-index measure based on six established psychosocial-stress buffers. However, no single psychosocial resource significantly interacted with cancer-related stress and inflammation to predict depressive symptoms. Secondary analyses revealed that tests of primary hypotheses were still supported when behavioral factors (i.e., physical activity and sleep disturbance) were added to the index of psychosocial resilience. Moreover, physical activity and sleep disturbance each interacted with cancer-related stress and inflammation to predict depressive symptoms such that the link between cancer-related stress and inflammation-related depressive symptoms was buffered when physical activity was high or when sleep disturbance was low. Examining individual effects of behavioral stress-buffering resources was therefore more successful than examining individual effects of psychosocial stress-buffering resources, but combining resources was most reliable.
It is important to acknowledge that the primary conclusions of the study were dependent on the method used to combine resilience resources into an index. More specifically, tests of primary hypotheses were not supported when the index of psychosocial resilience was computed using a PCA approach. This is despite the high correlation (r = .88) observed between the index of psychosocial resilience computed without PCA (i.e., as reported in the primary analyses) and the index of psychosocial resilience computed using PCA. One potential explanation for these results is that these two computation methods are capturing fundamentally different assumptions regarding how psychosocial resources synergize to promote resilience. More specifically, PCA produces an index that is a linear combination (determined by factor loadings) of standardized psychosocial-resource measures. Accordingly, a PCA-based index of psychosocial-resilience computation can average out deficits in psychosocial resources such that the same score can be obtained from an individual who scored at an average level across psychosocial measures and an individual who scored far below average on some resources and far above average on others. In other words, a PCA-based index of psychosocial-resilience computation is based on the implicit assumption that a given deficit in a psychosocial resource (e.g., scoring low in social support) can be compensated for by a surplus in other psychosocial resources (e.g., scoring high in mindfulness and optimism).
By contrast, the index of psychosocial resilience presented in the primary analyses was based on the opposite assumption—a given deficit in a psychosocial resource cannot be compensated for by a surplus in another psychosocial resource. This is because summing binary variables indicating the perceived presence or absence of psychosocial resources does not capture the degree to which any one resource is endorsed and thus does not allow for a high score on one resource to compensate for a low score on another. Instead, deficits in any one resource are clearly reflected in the final score. Another potential limitation of PCA is that it combines standardized (i.e., z-scored) resources, and this approach is questionable when raw scores are not normally distributed.
In summary, using a PCA approach to compute the index of psychosocial resilience produced nonsignificant effects, and additional work is needed to determine whether this reflects differences in the assumptions inherent to each approach or Type I error.
Finally, future work may benefit from considering the degree of independence exhibited by psychosocial resources. The psychosocial resources included in our study were not reliably highly intercorrelated; we observed correlations (rs) as low as .15. This is important because there may be an advantage to relying on independent resources (and/or perceiving that independent resources can be drawn on). Seminal work on cognitive complexity has suggested that individuals who perceive aspects of their self-concept as both more numerous and more independent are protected against negative effects of stressful life events, particularly depression (Linville, 1985). This is because events that threaten a single self-aspect influence a smaller proportion of the self when self-aspects are more numerous and more independent. Similarly, it is possible that perceiving the loss of a psychosocial resource contaminates perceived availability of closely related resources. Of course, more work is necessary to address this possibility, but a potentially fruitful avenue for future work is examining how composite indices of resilience perform when they include weakly versus highly correlated measures.
Strengths and limitations of the present study should be noted. Examining cancer-related stress in a sample of breast-cancer survivors followed over a 2-year period provided a valuable opportunity to examine stress and resilience effects. Moreover, examining multiple psychosocial factors previously shown to buffer against stress was a strength of the present study. However, resilience factors exist across more varied domains than those presently tested (Ungar, 2021), and future work in this area could include multisystemic resilience factors (e.g., community and environmental factors, biological factors). Relatedly, because resilience is considered a multifaceted construct, the present findings may be subject to omitted-variable bias, although secondary analyses including behavioral factors supported the primary results. Furthermore, this sample was more educated than the general population, and generalizability to other populations should be evaluated in future work. We found that the index-computation method impacted the primary conclusions of the study. Accordingly, future work should evaluate whether this reflects a meaningful distinction between computation methods evaluated presently or Type I error. The present measure of physical activity relied purely on self-report; replication using more objective measures of physical activity (e.g., step trackers) are therefore warranted. Finally, the present study benefited from measuring stress related to a specific and ongoing life event (i.e., breast cancer), but replication will be necessary to evaluate generalizability to other major stressors.
Conclusion
The present study examined whether psychosocial resilience factors can protect individuals from inflammation-associated depressive symptoms under conditions of high stress. We found that breast-cancer survivors who endorsed more numerous psychosocial resources known to buffer against stress showed weaker associations between stress and depressive symptoms and weaker associations between stress and inflammation-associated depressive symptoms. To date, the extant body of knowledge on resilience to inflammation-associated depressive symptoms was generated from preclinical studies and thus focused on biological resilience factors. The present study extends this literature by showing protective associations of psychosocial resilience factors. Finally, the present study adds to a growing literature focused on clarifying the synergistic effects of psychosocial resources hypothesized to promote resilience.
Supplemental Material
sj-docx-2-pss-10.1177_09567976221079633 – Supplemental material for Psychosocial Resilience to Inflammation-Associated Depression: A Prospective Study of Breast-Cancer Survivors
Supplemental material, sj-docx-2-pss-10.1177_09567976221079633 for Psychosocial Resilience to Inflammation-Associated Depression: A Prospective Study of Breast-Cancer Survivors by Andrew W. Manigault, Kate R. Kuhlman, Michael R. Irwin, Steve W. Cole, Patricia A. Ganz, Catherine M. Crespi and Julienne E. Bower in Psychological Science
Supplemental Material
sj-R-1-pss-10.1177_09567976221079633 – Supplemental material for Psychosocial Resilience to Inflammation-Associated Depression: A Prospective Study of Breast-Cancer Survivors
Supplemental material, sj-R-1-pss-10.1177_09567976221079633 for Psychosocial Resilience to Inflammation-Associated Depression: A Prospective Study of Breast-Cancer Survivors by Andrew W. Manigault, Kate R. Kuhlman, Michael R. Irwin, Steve W. Cole, Patricia A. Ganz, Catherine M. Crespi and Julienne E. Bower in Psychological Science
Footnotes
Transparency
Action Editor: Paul Jose
Editor: Patricia J. Bauer
Author Contributions
A. W. Manigault, K. R. Kuhlman, J. E. Bower, and M. R. Irwin developed the study concept and design. J. E. Bower, P. A. Ganz, M. R. Irwin, S. W. Cole, and C. M. Crespi performed testing and data collection. A. W. Manigault analyzed the data; all the authors interpreted the data. A. W. Manigault and J. E. Bower drafted the manuscript. All authors provided critical revisions and approved the final manuscript for submission.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.