
Abstract
Background
Sex workers are disproportionately affected by HIV and sexually transmitted infections (STI) in the Republic of Congo. We conducted a one-group pre-post test participatory mapping (PM) intervention to increase HIV/STI testing uptake with female sex professionals (FSP) in Pointe Noire, Congo.
Methods
We engaged a peer-driven sample of FSP in Pointe Noire in a 2-day PM intervention. Voluntary HIV and STI testing and treatment was offered at Time 2 (T2) (directly post-intervention) until Time 3 (T3) (8-week post intervention). To measure HIV/STI testing changes between Time 1 (T1) (baseline, lifetime HIV/STI testing), T2, and T3, we used a generalized estimating equation model with robust standard errors, using an unstructured correlation matrix to account for within-subject correlations.
Results
Among n = 99 participants (mean age: 25.5, standard deviation = 6.5), in analyses adjusted for age and sex work duration, there were significant increases at T2 in uptake of HIV testing (adjusted Odds Ratio [aOR] = 2.42; 95% CI = 1.31–4.48) and STI testing (aOR = 2.40; 95% CI = 1.27–4.54), as well as at T3 (HIV testing: aOR = 7.37; 95% CI = 2.82–19.23, STI testing: aOR = 5.88; 95% CI = 2.82–12.24), compared to baseline.
Conclusions
Findings signal the promise of community-based approaches such as participatory mapping for increasing HIV/STI testing uptake with FSP in Pointe Noire.
Introduction
Female sex workers (FSW) are disproportionately affected by adverse health outcomes, stigmatization, and human rights violations. 1 Notably, compared to non sex working women, women engaged in sex work have an 8-fold higher HIV prevalence in Sub-Saharan Africa. 2 This disproportionate impact of HIV is even more pronounced in Western and Central Africa, where FSW have a 19.9 fold higher HIV incidence than non sex working counterparts. 2 As recent estimates indicate that there are approximately 2.5 million FSW aged 15 to 49 in Sub-Saharan Africa, 3 meeting the HIV prevention needs of this population is an urgent priority. This is particularly true in the Central African context of the Republic of Congo, where FSW are a priority for HIV prevention.
UNAIDS estimated the Republic of Congo adult HIV prevalence in 2023 is 3.2%, with only 33% of people living with HIV knowing their status. 4 This is far below the UNAIDS goal of 95% of people living with HIV aware of their status, 95% on treatment, and 95% virally suppressed to end the HIV pandemic by 2030. 5 In a multi-site study in the Republic of Congo, the HIV prevalence among FSW was estimated at 7.5%--more than double the national HIV prevalance, with additional high rates of sexually transmitted infections (STI) including syphilis (2.2%), Hepatitis B Virus (HBV) (4.2%), and Hepatitis C Virus (HCV) (0.7%). 6 Pointe Noire had the highest syphilis (5.2%) and HBV (4.2%) rates in this study. 6 This city thus is a strategic site for developing targeted FSP HIV/STI prevention interventions.
Despite this disproportionate impact of HIV and STIs on FSW in the Republic of Congo, little is known of effective strategies to engage this population in HIV testing and prevention services at large. Yet across Sub-Saharan Africa, criminalizing contexts 1 and sex work stigma present significant barriers to accessing HIV testing.7–9 Strategies to engage FSW in HIV and STI testing should therefore ensure programs can advance their dignity, health, and rights. 10
The HIV prevention cascade offers a conceptual framework to inform such interventions, and focuses on dimensions of motivation (e.g., knowledge), access (e.g. availability, acceptability, affordability), and effective use (e.g. self-efficacy, empowerment). 11 Addressing these complex dimensions across the cascade requires not only biomedical interventions but also participatory, community-engaged methods that can reduce structural, social, and spatial barriers to care such as costs and stigma. 12 Thus, comprehensive approaches based on local realities may offer promising solutions. While participatory approaches hold promise for increasing HIV prevention engagement with FSW, 13 they are understudied in the Republic of Congo.
Participatory mapping is one such method that also aligns with community empowerment-based approaches to HIV prevention with FSW. 10 This method remains understudied in the Republic of Congo, yet participatory mapping methods have been implemented across various contexts in Africa for health research, including HIV.14,15 Participatory mapping engages community members in identifying places in their community that they wish to create social change within, sharing lived experiences, and co-developing goals and problem-solving solutions. 16 For instance, participatory mapping has been used to identify community structures that could be used as healthcare facilities, to characterize social barriers that prevent individuals from addressing healthcare needs, to understand socio-environmental health risks, and to foster collaboration between researchers and local communities.15,17–19 In an example from Nigeria, participatory mapping was used to develop strategies for mass administration of neglected tropical disease medication; this approach identified both new community structures (e.g. football field, mechanic shops) for medicine distribution and access, and also documented potential logistic and socio-cultural challenges in using such structures. 17 Participant community mapping approaches were used in rural South Africa to co-develop peer-led HIV prevention strategies grounded in the community’s real-world mobility patterns, trusted networks, and safe spaces. 20 Participatory mapping can also guide community-informed interventions to develop health enabling environments for HIV prevention with marginalized communities.19–21 While limited studies have examined participatory mapping in HIV/STI prevention and/or testing interventions, or for stigma reduction, existing literature reveals its potential to be implemented across various contexts in health care and HIV research.14,15,20,21 These findings signal that participatory mapping can be adapted to various public health contexts in Africa, including HIV and STI testing, and may enable the emergence of local solutions and community empowerment.
Our study aimed to address these knowledge gaps regarding participatory mapping approaches to increase HIV and STI testing with FSW in the Republic of Congo. As sex professionals is the preferred term in the Republic of Congo, we hereafter refer to female sex professionals (FSP) regarding our study. The Republic of Congo is an important context to identify strategies to engage FSP in HIV and STI testing due to the high HIV/STI prevalence as well as the larger socio-legal context where sex work is not decriminalized and FSP are therefore exposed to police and client violence as well as marginalization. 22 Specifically, this study aimed to evaluate the effectiveness of a participatory mapping intervention among FSP in Pointe-Noire, Republic of Congo in increasing HIV and STI testing uptake.
Methods
Study design
We conducted a single group pre/post-test community-based research (CBR) study in 2023–2024 to examine the potential of participatory mapping in increasing HIV and STI testing uptake with FSP in Pointe Noire, Congo. This CBR study was a collaboration with a FSP community-based organization (CBO) in Pointe Noire who conducted non-random purposive sampling, using word-of-mouth, peer recruitment with six peer navigators (FSP identified) with support from a Research Assistant hired and trained to work on the study, and venue-based recruitment at the CBO. Participant eligibility included being: aged 18 and older, self-identifying as a women sex professional, living in Pointe Noire, and able to provide informed consent.
We conducted a series of five 2-day participatory mapping workshops at the FSP CBO, each with 20 participating FSP (described below). We collaborated with a local polyclinic to offer voluntary point-of-care HIV and STI (gonorrhea, syphilis, HBV, HCV) testing with clinic-based validation and free treatment. Free and voluntary HIV/STI testing was offered directly following the workshop at the FSP CBO in a private room, and for 8 subsequent weeks at the collaborating polyclinic. Blood samples were collected according to routine clinical protocols, and a rapid diagnostic test was used as the primary diagnostic tool, and for positive results, a PCR test was used for confirmation. We worked with the FSP CBO to provide a 1-day stigma reduction training and sex work sensitivity training for the participating polyclinic staff prior to study implementation.
Quantitative survey data were collected at three time points: at enrollment before the intervention (Time 1), immediately after the 2-day participatory mapping intervention (Time 2), and at 8 week post-intervention follow-up (Time 3). Paper-based standardized questionnaires were administered by trained peer navigators. To ensure confidentiality, each participant was assigned a unique case ID, and no personally identifying information was recorded or stored in the database. Participants were provided coupons with their study ID if they chose to engage with HIV and STI testing, and our study provided free HIV and STI testing and treatment. HIV testing and treatment costs are regularly covered by national health programs in the Republic of Congo so participants testing HIV positive were referred to local care, however STI testing and treatment costs are not covered therefore we provided this free of charge to participants during the study. The polyclinic collected the ID coupons in order to facilitate matching HIV/STI testing uptake and results with the survey data.
This study received ethics approval from The University of Toronto Research Ethics Board (Protocol Number: 41845) and Comité d’Éthique pour la Recherche en Santé (CERS) de la Fondation Marie Madeleine GOMBES (Research Ethics Committee in Health of the Marie Madeleine Gombes Foundation). Individual written informed consent was obtained prior to data collection. All HIV/STI testing methods and study procedures were performed in accordance with the principles of the Declaration of Helsinki.
Intervention description
The study design involved: a) a formative qualitative phase to understand lived experiences of FSP in Pointe Noire (data not presented); b) co-developing a participatory mapping intervention with FSP, academic, and clinic-based team members, including planning implementation of HIV/STI testing, and training the collaborating polyclinic staff on sex professional stigma reduction; and c) participatory mapping workshops delivered by a researcher, a community-based coordinator, and trained FSP peer navigators through a 2 day workshop with four sessions with 100 FSP, organized into five groups of 20, directly followed by on-site HIV/STI testing with coupons with study ID information to access polyclinic-based testing for an additional 8-weeks post-intervention.
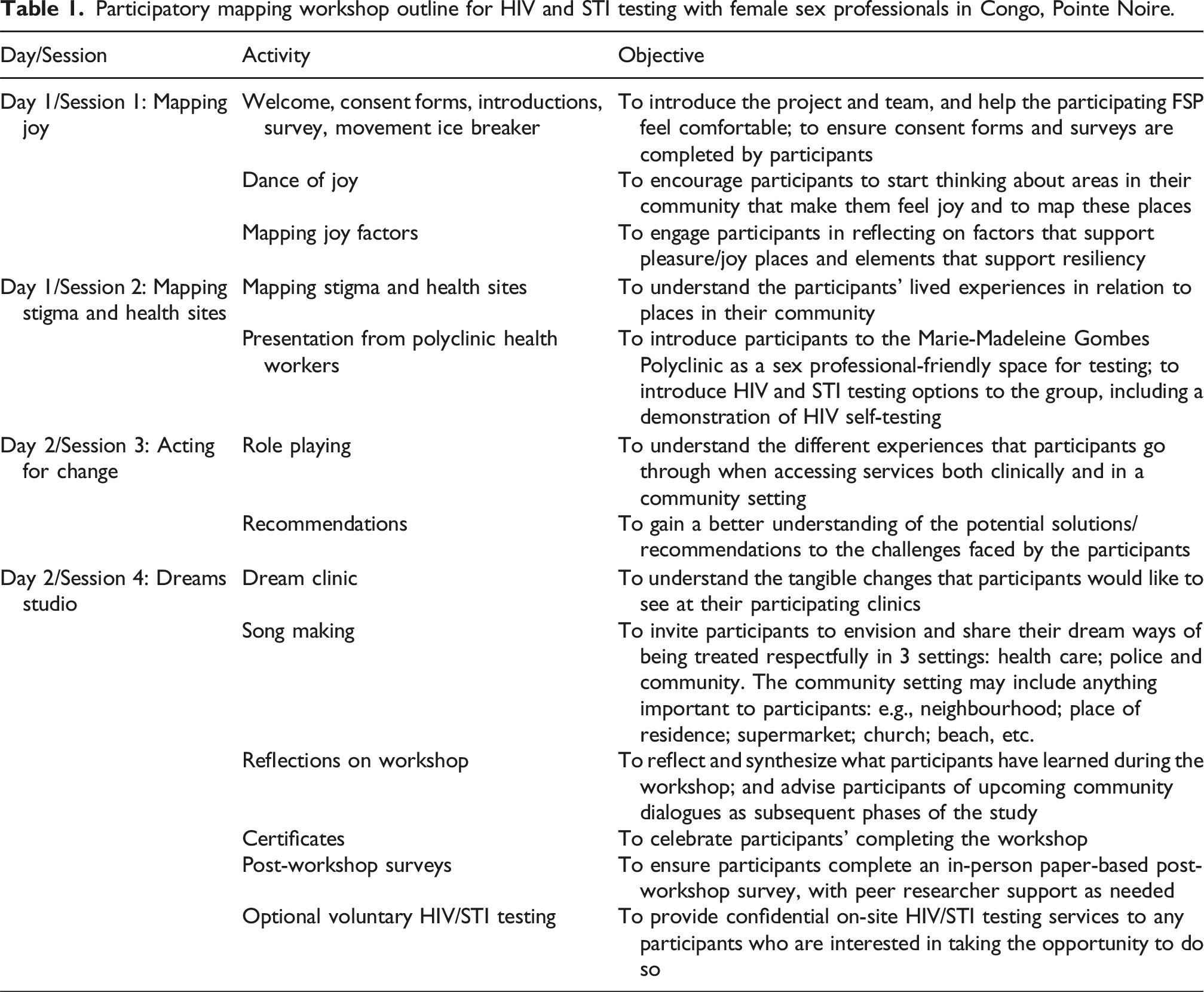
The participatory mapping workshops aimed to increase HIV and STI testing access and uptake by addressing the key domains of the HIV prevention cascade: 1) increasing motivation through providing peer-based education, addressing social norms regarding stigma toward FSP, stigma and HIV, and providing knowledge of HIV/STI testing and treatment; 2) addressing access through increasing testing availability and acceptable provision with voluntary and free HIV/STI testing and treatment offered at a CBO and polyclinic trained in reducing sex work stigma; and 3) increasing effective use through leveraging FSP empowerment through small group sessions that included sharing lived experiences of stigma, social cohesion building with arts-based methods (e.g., mapping, dream clinic activities), and generating recommendations for social change.10,11,13
Participatory mapping workshop outline for HIV and STI testing with female sex professionals in Congo, Pointe Noire.
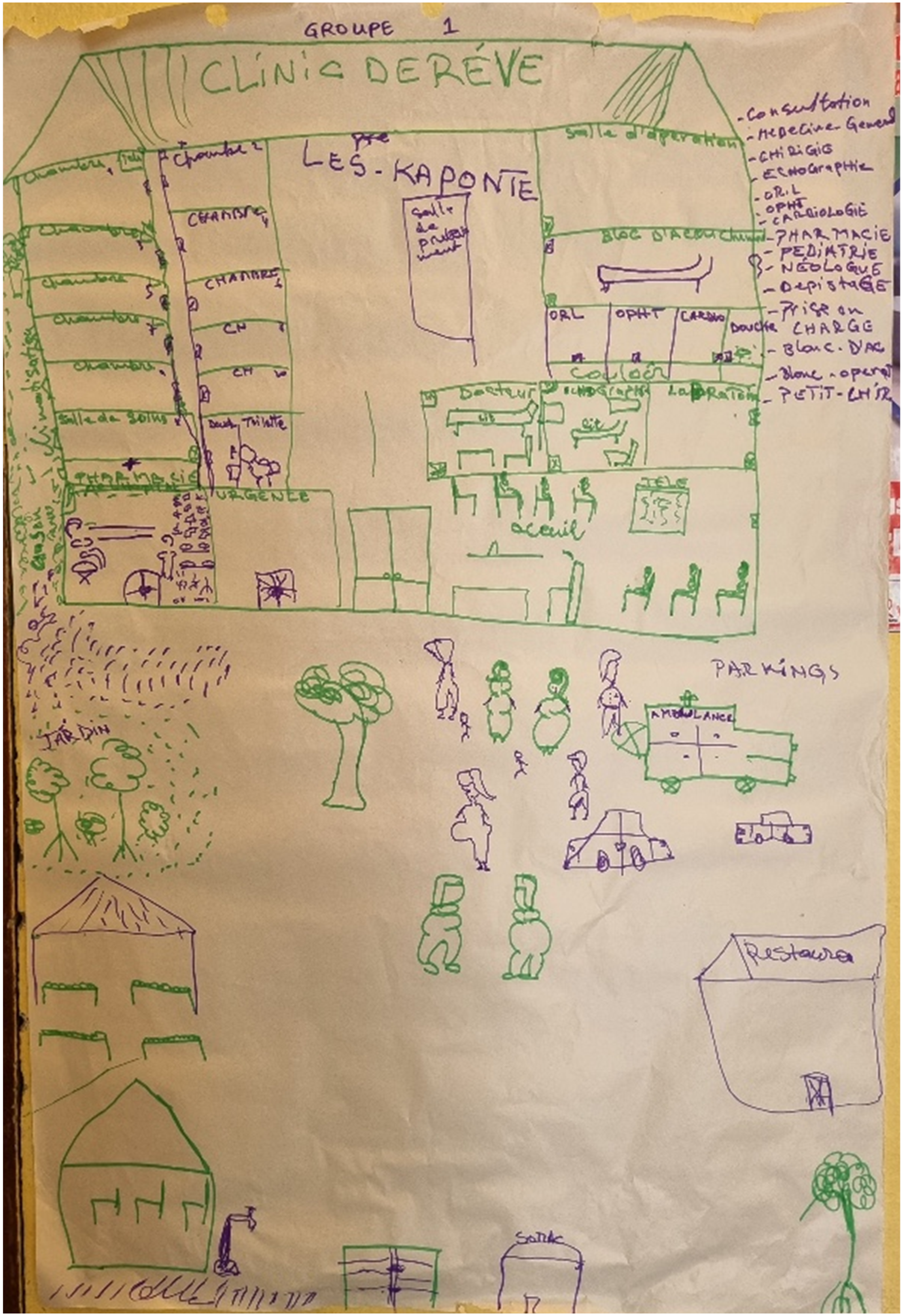
Dream clinic drawing by female sex professional participants in the participatory mapping workshop in Pointe Noire, Congo.
Measurement and analysis
Socio-demographic variables
Data was collected on sociodemographic characteristics including age, duration of sex work, relationship status, highest level of education, sources of income other than sex work, and dependents.
Outcome variables
The two primary outcomes of HIV and STI testing were treated as binary variables. At baseline, we asked lifetime HIV and STI testing uptake, as well as results for those who reported ever testing for HIV/STI. We provided study coupons with participant identification (ID) numbers for HIV and STI testing at each site (CBO, collaborating polyclinic) that participants provided the clinic staff with in order to link each participants’ survey to their testing uptake and results.
We conducted descriptive statistics to characterize the study population at baseline using frequencies and proportions for categorical variables and means (with standard deviation [SD]) for continuous variables. To measure changes in outcomes across the three time points, we used a generalized estimating equation (GEE) model with robust standard errors, using an unstructured correlation matrix to account for within-subject correlations. 24 Logistic GEE models were conducted for the categorical outcomes (HIV testing, STI testing) with time as the primary exposure.
Each model was first conducted without adjustment, followed by adjustment for pre-specified covariates (age and duration of sex work). We selected these covariates based on prior evidence that these factors are consistently associated with HIV/STI testing uptake among FSP in Sub-Saharan Africa.25–28 Other sociodemographic variables were not included due to limited sample size in each category. Intervention effects are presented as crude and adjusted ORs (aORs) for binary categorical outcomes with 95% confidence intervals (CI). All regression analyses were performed using a complete-case analysis, those who were lost to follow-up were not included in outcome analyses. All analyses were two-sided with a significance level of p ≤ 0.05, and were conducted in Stata 14.2 (StataCorp, College Station, TX, USA).
Results
Socio-demographic characteristics
Sociodemographic characteristics and HIV and STI testing among female sex professionals in Pointe Noire, Congo.
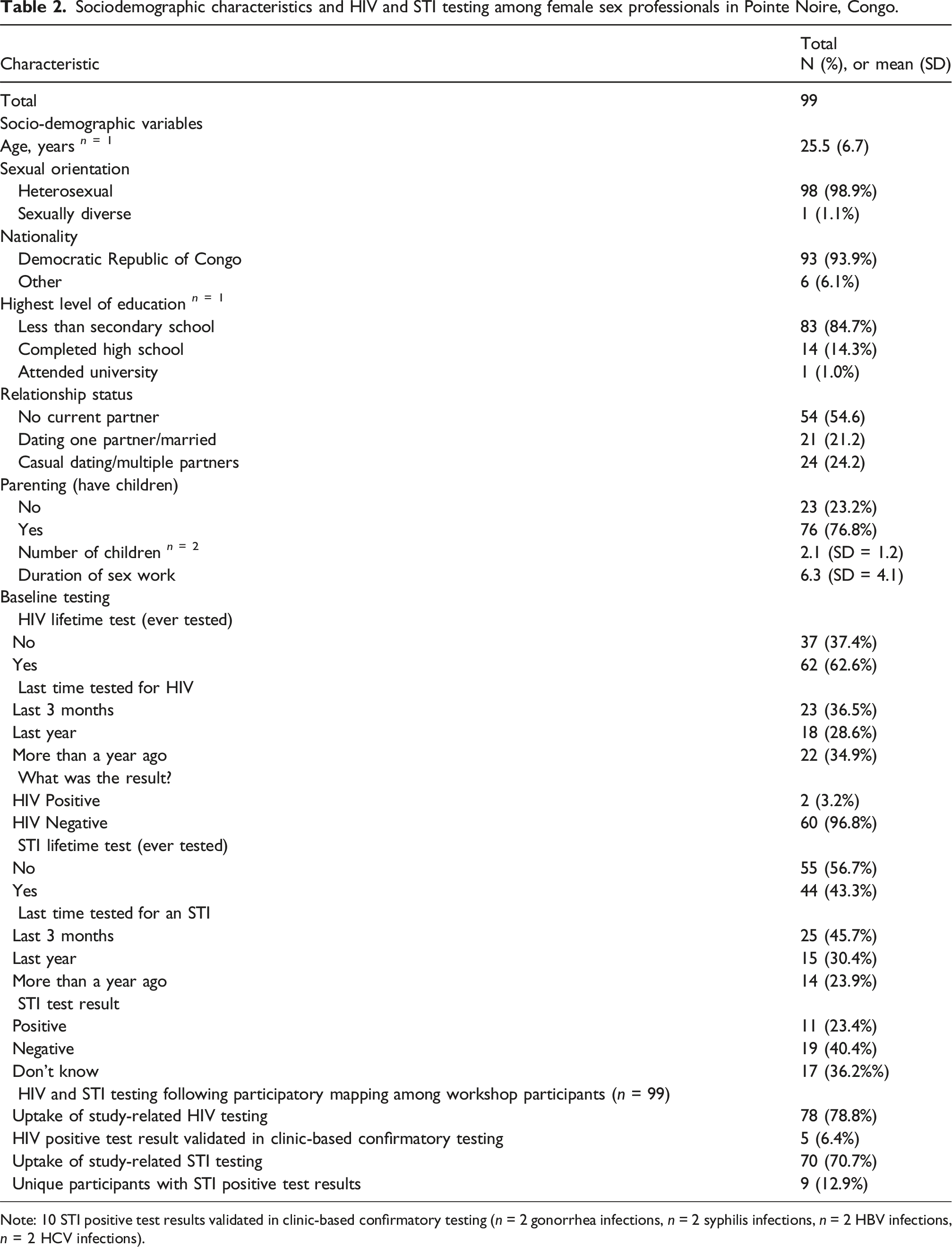
Note: 10 STI positive test results validated in clinic-based confirmatory testing (n = 2 gonorrhea infections, n = 2 syphilis infections, n = 2 HBV infections, n = 2 HCV infections).
As shown in Table 2, at baseline, 62.6% (n = 62) and 43.3% (n = 42) of the participants had ever tested for HIV and STI respectively. Participant retention rate was high in this study, with 92% (n = 91) surveyed at post-intervention (Time-2), and 90% (n = 89) at 8-week follow-up (Time-3). More than three-quarters (79%) of participants (78/99) agreed to have an HIV test following the participatory mapping workshop; of these, n = 5 (6.4%) had an HIV positive test result validated in clinic-based confirmatory testing. Among participants, n = 70 (70.7%) received an STI test following the workshop. There were n = 10 STI positive test results validated in clinic-based confirmatory testing among nine unique participants (one person was coinfected with syphilis and HCV): n = 2 gonorrhea infections, n = 2 syphilis infections, n = 2 HBV infections, and n = 2 HCV infections. One other participant was co-infected with HIV and HCV.
HIV and STI testing uptake following the intervention
Pre and post-test differences in HIV/STI testing uptake among female sex professional participants in a participatory mapping workshop in Pointe Noire, Congo.
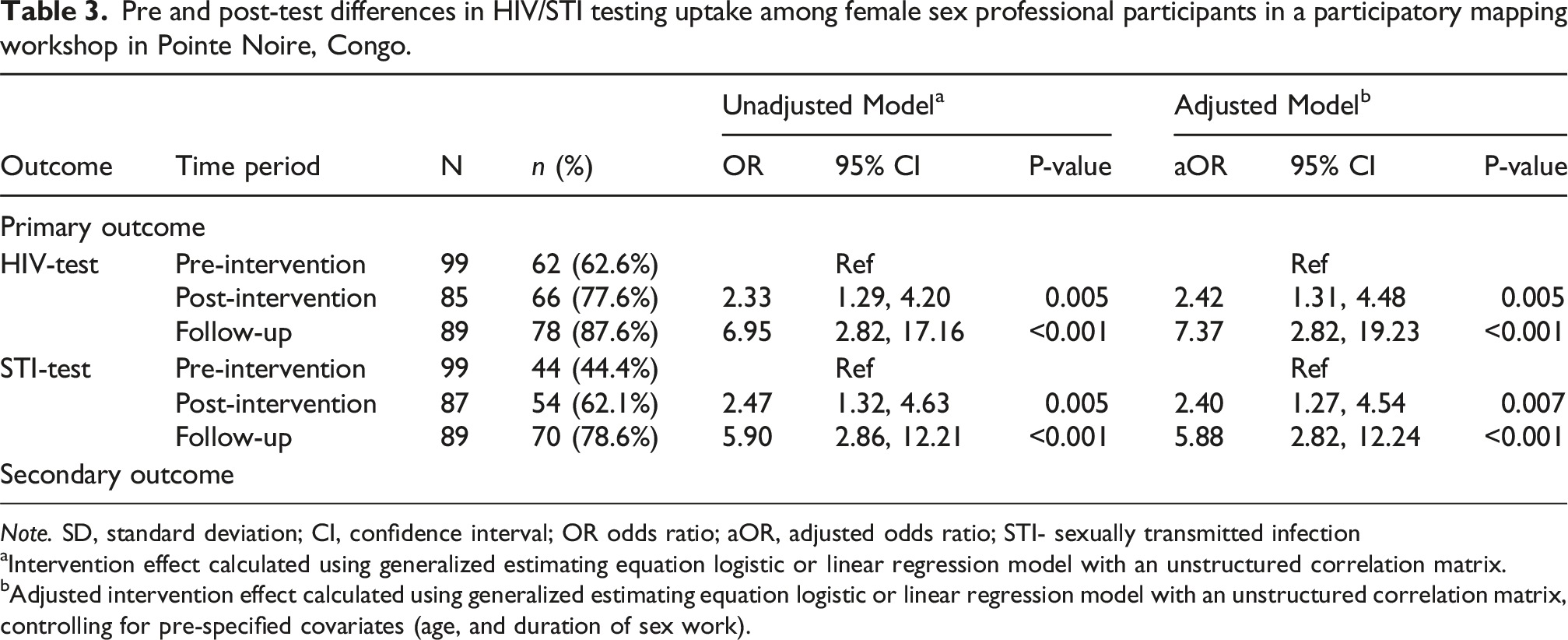
Note. SD, standard deviation; CI, confidence interval; OR odds ratio; aOR, adjusted odds ratio; STI- sexually transmitted infection
aIntervention effect calculated using generalized estimating equation logistic or linear regression model with an unstructured correlation matrix.
bAdjusted intervention effect calculated using generalized estimating equation logistic or linear regression model with an unstructured correlation matrix, controlling for pre-specified covariates (age, and duration of sex work).
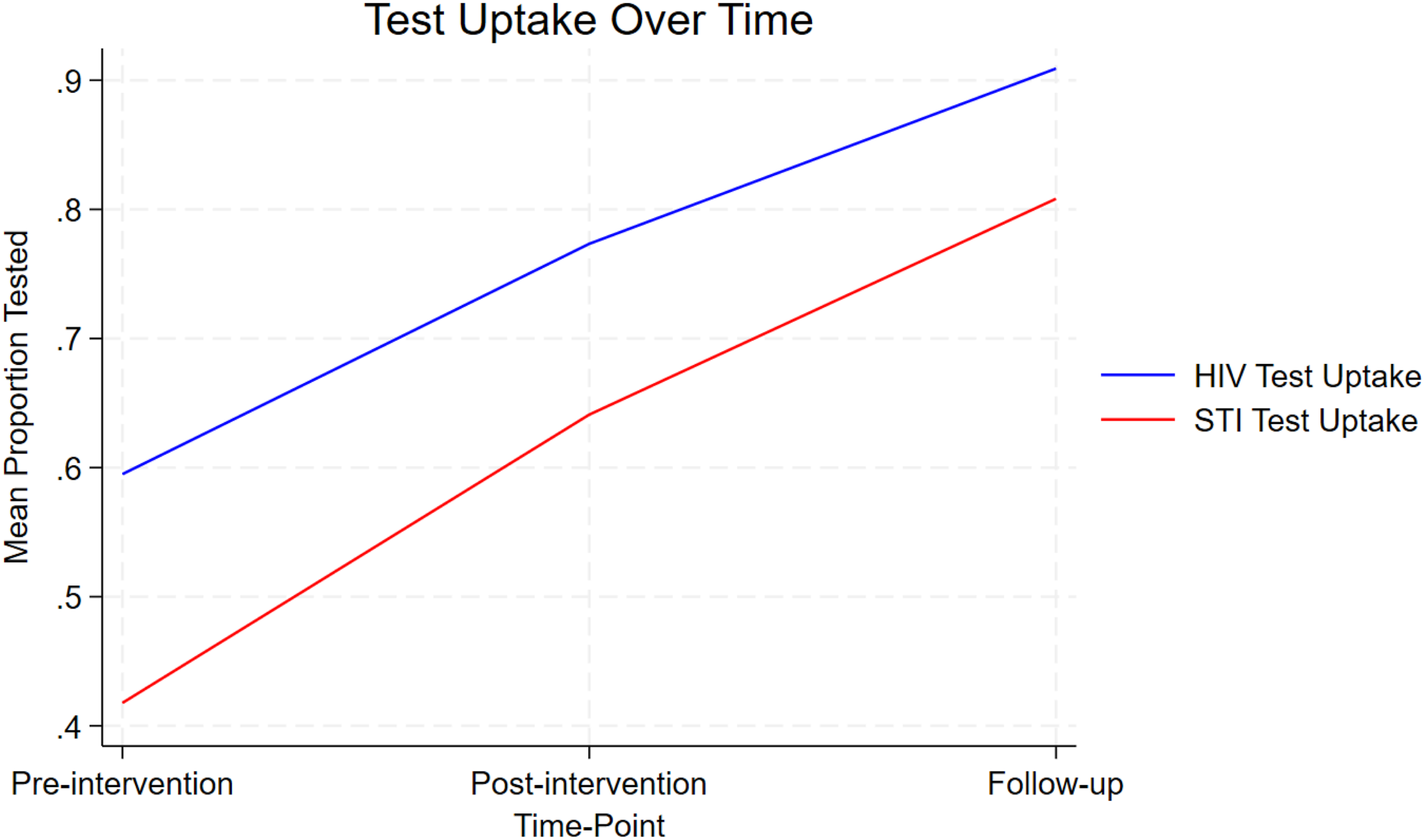
Pre and post-test differences in HIV and STI testing following a participatory mapping workshop with female sex professionals in Pointe Noire, Congo.
Discussion
This study explored the impact of a participatory mapping workshop on increasing HIV and STI testing uptake among FSP in Pointe Noire, Republic of Congo. Our findings demonstrate that participatory mapping accompanied by HIV/STI testing is a feasible and potentially impactful community-based strategy with FSP associated with increased HIV and STI testing uptake immediately following the intervention with sustained improvements at 8 weeks post-intervention. These results suggest that participatory mapping may be an effective method to strengthen the HIV prevention cascade domains of motivation, access, and effective use 11 for HIV testing among FSP in this context.
Consistent with previous studies in Sub-Saharan Africa,25–29 baseline data from our sample of FSP revealed levels of HIV testing were far below the UNAIDS goals of 95% of people living with HIV knowing their status. 30 Despite a documented high prevalence of HIV and STIs among FSP in the Republic of Congo,2,6 nearly 40% of our participants had never tested for HIV, and more than half had never tested for STIs, even when HIV testing is available free of charge. Structural and social barriers—such as stigma, criminalization, and limited access to sex worker-sensitive services—likely contribute to these low testing levels.6,8,9,31–35 Across Africa, evidence shows that biomedical services alone do not ensure testing uptake among sex workers; interventions that combine access with community empowerment, peer navigation, and stigma-reduction have proven far more effective in increasing HIV testing9,10,20 Our workshops focused on community empowerment, peer support, tailored education, and accessible HIV/STI testing—important for FSP’s wellbeing—10,13 and participation was associated with a 2.4-fold and 7.4-fold increase in HIV testing at Time 2 and Time 3 respectively, and similarly strong increases in STI testing uptake. Our study therefore may have increased testing uptake through fostering an enabling environment for HIV prevention engagement. Dimensions of such an enabling environment targeted by our intervention include both technical communication (offering testing services, sharing HIV information) as well as transformative communication (whereby participants were provided the opportunity to both communicate about their needs and have a social environment, comprised of peers, researchers and clinicians, who were interested and receptive to their needs and priorities). 36 Our approach also aligns wth research on the effectiveness of community empowerment-based approaches on advancing HIV and STI prevention with sex workers. 10
These results also support the broader applicability of the HIV prevention cascade dimensions of motivation, access, and effective use 11 in guiding community-based interventions. Prior participatory arts-based research aligned with these HIV prevention cascade domains in Uganda also noted improved HIV testing engagement.12,37 While there is a growing body of evidence supporting participatory mapping HIV-related research in Sub-Saharan Africa,19–21 there is limited evidence on participatory mapping specifically for HIV/STI testing with FSP—or other populations. Our study extends existing research by providing empirical evidence that participatory mapping can be effectively adapted to the local context of Pointe Noire. Prior research in Nigeria, 17 Benin, 18 Kenya, 19 and South Africa 20 has found that participatory mapping can foster dialogue and insight regarding spatial and social determinants of health, and our findings build on this to highlight the potential for integrating HIV and STI testing into this method. Our intervention’s sustained impact on testing uptake over time supports the integrating HIV prevention cascade-informed community empowerment strategies with accessible testing services for FSP.
The relatively high number of clinically confirmed HIV (6%) and STI (13%) cases detected in this sample of FSP in Pointe Noire further emphasizes the importance of scaling up accessible testing for FSP as well as the promotion of biomedical HIV prevention such as pre-exposure prophylaxis (PrEP) and bacterial STI prevention with doxycycline post-exposure prophylaxis (DoxyPEP). Our finding suggest there may be an important undiagnosed burden in this population, reflecting the suboptimal HIV testing uptake with FSW in other Sub-Saharan African contexts.6,8,9,31–35 These data reinforce the call for differentiated HIV services and tailored outreach strategies for FSP. 5
Our study has several limitations. First, as we used a single-group pre/post-test design without a control group this limits causal inference. However, the consistency of significant testing improvements across two time points and the high retention rate strengthen confidence in the observed effects. Second, our non-random sample means findings cannot be generalized to all FSP in Pointe Noire, and self-selection bias may have occurred, as individuals engaged with the sex worker CBO may have been more aware of and motivated to access HIV services. Third, we were not able to assess within the study duration any long-term engagement and adherence to HIV/STI treatment and linkage to other health services. Fourth, as we offered workshops and HIV/STI testing to all participants, we were not able to disentangle the effect of PMW alone vs. combination of PMW with HIV and STI testing services. Future studies could conduct a factorial trial to evaluate the HIV/STI testing and participatory mapping intervention components separately as well as combined to understand the interaction between these components. 38 Finally, while participatory mapping demonstrated promise, the scalability and sustainability of these approaches warrant further evaluation in both urban and rural Congolese settings using a rigorous randomized controlled group design.
Conclusion
This study contributes novel evidence that participatory mapping is a feasible, acceptable, and effective approach to engage FSP in HIV and STI testing services in Pointe Noire. Future programs with FSP can consider integrating participatory mapping with low-barrier HIV and STI testing and treatment. Participatory and visual methods, combined with tailored services, can contribute to HIV prevention strategies that are rights-based and centered on the needs of FSP.
Footnotes
Acknowledgements
We acknowledge all participants and peer researchers for their contributions.
Ethical approval
This study received approval from The University of Toronto Research Ethics Board (Protocol Number: 41845) and Comité d’Éthique pour la Recherche en Santé (CERS) de la Fondation Marie Madeleine Gombes (Research Ethics Committee in Health of the Marie Madeleine Gombes Foundation).
Informed consent
Informed consent was obtained from all participants involved in the study.
Author Contributions
Design of study: CHL, SBV, BM, LMAC, LSGL, HL. Acquisition, analysis, interpretation of data: CHL, ZA, SVB, DP, FM, BM, LMAB, LSGL, HL. Drafting and reviewing work: CHL, ZA, SVB, DP, FM, BM, LMAB, LSGL. Approval of final version: CHL, ZA, SVB, DP, FM, BM, LMAB, LSGL, HL.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by Grand Challenges Canada; R-ST-POC-2205-52021 and the Canada Research Chairs Program (Tier 2, Logie: Canada Research Chair in Global Health Equity & Social Justice with Marginalized Populations).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.