
Abstract
Background
Despite the availability of PrEP, 2023 data have demonstrated an increase in new HIV diagnoses. LGBTQ + individuals are disproportionately affected by HIV. PrEP access is crucial but limited due to high demand on sexual health services. Additional modalities of PrEP access may help to address this unmet need. LVNDR Health, a digital solution for LGBTQ + care, sought to evaluate its PrEP pathway.
Methods
We conducted a retrospective cross-sectional service evaluation of users accessing the LVNDR digital PrEP pathway between December 2022-April 2023. Operational data (e.g., appointment attendance) were derived from the clinical dashboard. Service-user feedback (e.g., service experience) was sought using a bespoke questionnaire. Descriptive statistics are reported for socio-demographic information. Non-parametric between-group analyses are reported.
Results
In total, 90 users completed the end-to-end pathway and received PrEP. Average time for pathway completion was 2.7 weeks. A survey response rate of 71.0% was achieved. Users reported significantly higher service satisfaction, inclusivity, and accessibility, compared to their most recent experience accessing PrEP (p < .01). Up to 89% of users strongly agreed they would switch to a digital PrEP service if made available.
Conclusion
Digital PrEP shows acceptability among LGBTQ + populations. More research is needed to assess scalability, digital equity, and cost-effectiveness.
Introduction
Pre-Exposure Prophylaxis (PrEP) is an intervention that can significantly reduce the risk of HIV transmission. In 2020, PrEP became free at the point of access in England from NHS sexual health clinics (known as Level 3 services) following the success of the IMPACT trial, which demonstrated a 87% risk reduction in HIV infection (HIV incidence per 100 person-years 0.13, 95% Confidence Interval (95% CI) 0.08, 0.19) among Gay, Bisexual and other Men who have Sex with Men (GBMSM) on PrEP when compared to non-PrEP users. 1 Prior to 2022, the UK Health Security Agency (UKHSA) had reported a continued and steady decline in new HIV diagnoses. 2 However, more recent figures indicate a significant rise between 2022–2023 in new diagnoses in England (n = 2451 vs n = 2810), while late diagnoses increased by 3% (n = 896 vs n = 923). Notably, the COVID-19 pandemic has had a considerable impact on HIV testing since 2020 that has made subsequent analyses on testing uptake and transmission more complex to interpret. 3 Nevertheless, current national targets are set with a view to reduce new HIV transmissions to 0 by 2030. 4
UK model estimates for future and current lifetime care costs of managing people living with HIV (PLWHIV) range from ∼£73,000-£404,000. 5 For GBMSM diagnosed in 2023 alone (n = 811), this represents a healthcare system cost of approximately £59-328Mn. 2 While the recent Office for National Statistics data suggest that LGB + individuals make up only 3.2% of the population in England and Wales, sex between men accounted for 29% (n = 811/2810) of new diagnoses compared to 49% (n = 1836) for women and men exposed through heterosexual contact in 2023.2,6 Preventative models of HIV care therefore have the capacity to benefit a range of populations, including both LGBTQ+ and heterosexual individuals, as well as reduce healthcare utilisation associated with HIV-related morbidity and mortality. 7
The efficacy of combined tenofovir disoproxil and emtricitabine (TDF/FTC) PrEP has been established in cisgender men and women taking four tablets and six tablets per week, respectively.8,9 There is a growing evidence base among other populations, including transgender women, serodifferent couples where one member of the couple is living with HIV and the other one is not, people who inject drugs, and groups affected by high HIV prevalence, such as sex workers. 10 This evidence has facilitated the recommendation of PrEP for these groups as outlined in recent national guidelines provided by organisations such as the National Institute for Health and Care Excellence (NICE), British Association for Sexual Health and HIV (BASHH), and the British HIV Association (BHIVA).11,12 However, despite these recommendations, a 2022 joint statement from BASHH and related organisations highlighted a concerning reduction in PrEP access by up to 90% for some UK regions due to the challenges associated with the recent MPox outbreak and increasing demands on sexual health services. 13 These unmet demands and fall in activity are reflected in the 2022 “Not PrEPared” report. 14 The report highlighted that almost half (n = 37/79, 47.0%) of all clinicians surveyed felt that they did not have sufficient capacity to deliver PrEP, over half (n = 638/1120, 57.0%) of community respondents on waiting lists had waited more than 12 weeks for a call-back, and that at the time of the report, only 35.0% (n = 392) of respondents had successfully accessed PrEP.
The PrEP Access and Equity Task and Finish Group, a subgroup of the HIV Action Plan Implementation Steering Group, was established in 2022 to support implementation of the national HIV Action Plan. Recommendations made by the group include the adoption of locally commissioned pilots to provide PrEP outside of sexual health services, such as making PrEP (TDF/FTC) accessible via pharmacies, GP surgeries, and digital services. 15 Edwards 16 provides an important commentary on the potential role of digital PrEP services in the future. This includes the need for co-development with populations that may face barriers to PrEP access, including trans and cisgender women, individuals from minority ethnic communities, as well as people who inject drugs.17,18 Conversely, while early evidence of acceptability for digital PrEP (or ePrEP) services continues to grow, it is critical to address concerns raised in relation to novel modalities for PrEP access. 19 . For example, Girometti et al. 20 identified that almost 1 in 5 individuals diagnosed with HIV between 2016–2020 at a clinic in London had been recent users of PrEP, with 63.5% (n = 33/52) those newly diagnosed accessing PrEP from a non-clinical setting. This may suggest poor uptake of prerequisite testing for PrEP, which includes screening for bloodborne viruses, such as HIV and hepatitis, as outlined in national BASHH/BHIVA guidance. PrEP efficacy is highly dependent on adherence, hence this is also an important consideration given that a significant difference in the presence of drug-resistant HIV was observed among PrEP users newly diagnosed in this cohort (p < .01). This may be addressed in future with the introduction of alternative PrEP interventions that are less suitable for a digital model but can help to address unmet demand and support those with complex PrEP needs, particularly related to non-adherence. These interventions may include long-acting injectable cabotegravir (CAB-LA), with a NICE decision on approval in England expected by December 2024, or twice-yearly subcutaneous lenacapavir, which recently demonstrated no new HIV infections among a cohort of cisgender women (n = 2134) in South Africa and Uganda.21–23
LVNDR Health is a Care Quality Commission (CQC) registered digital clinic for LGBTQ + sexual health and wellbeing. Over the course of 2022, LVNDR Health developed a novel patient-facing mobile application (App) and clinician dashboard to deliver an end-to-end digital PrEP pathway. The pathway has been informed by national guidance for the use of PrEP and co-developed following extensive research with NHS Trusts, Public Health (PH), clinicians, commissioners, and LGBTQ + community members (n = ≥800).
The LVNDR App could be downloaded by Service Users (SUs) to either an Apple or Android device after receiving a specific link for that individual user. SUs could access a homepage where they would be directed to their profile section to record their socio-demographic details and a selection of self-reported population health metrics for example, smoking status, substance use, family history of hypertension or kidney disease, vaccination status etc. The homepage also provided options to navigate to “Test Kit” and “Prescription” tabs. Via the Test Kit tab, SUs were able to order discreet packages comprising capillary blood tests for HIV, hepatitis B, and creatinine, in addition to a urine sample to determine a urinary protein creatinine ratio (uPCR). Test kits were returned via post to a third-party accredited lab. provider who reported results directly to LVNDR via an integration to the clinician dashboard, a bespoke electronic health record (EHR) developed for the service. SU data, including their age, self-reported weight, and sex assigned at birth, were shared directly with the lab provider via the integration to calculate an estimated Glomerular Filtration Rate (eGFR). Once results were reviewed, SUs were invited to attend an online video consultation via the App. The video call functionality was integrated within the dashboard for clinicians to conduct the consultation while providing simultaneous access to the SU results, history taking, and digital prescribing capabilities. Where clinically appropriate, PrEP (TDF/FTC) was prescribed and delivered to a SU’s address of choice. Tracking details were made available for each prescription for both the SU and clinical team.
This project sought to evaluate a pilot digital PrEP service and usability of the LVNDR App.
Methods
The project was conducted as a retrospective cross-sectional service evaluation of the LVNDR Health PrEP pathway, which was conducted between December 2022 and April 2023.
Sample size
Average PrEP activity data for 2021–22 were provided by a Southeast London Trust to help determine a suitable sample size. Figures indicated a typical monthly load of 120–240 PrEP patients. A standard pilot calculation (∼10%) was applied to the mean monthly load (n = 180) over a 4-month period to determine a minimum sample size of 72.
Recruitment & sample characteristics
The initial pilot implemented a convenience and snowball sampling method, such that local support/advocacy groups in Southeast London known to LVNDR were approached to share information about the pilot. Potential participants could disseminate/recommend the pilot by sharing the digital sign-up link. SUs were predominantly recruited via social media channels e.g., Instagram/Twitter, following exposure to a LVNDR social media campaign containing a registration link for the pilot. Social media campaigns were designed to attract potential LGBTQ + SUs, however neither any specific sexual orientation nor gender identity were a precluding factor to participate in the pilot. Individual SUs were assessed by the clinical team to determine service ineligibility based on a brief onboarding survey. Exclusion criteria were: SUs <18 years of age, individuals living with HIV, and a history of severe renal disease. Other excluding factors e.g., self-reported history of liver disease or pregnancy/breast feeding, were assessed during the video consultation. Included SUs received an email with instructions to download the App and order a test kit. Although delivered as a digital service and therefore not limited geographically, the initial online recruitment focused on distribution to social media channels and organisations to support the recruitment of LGBTQ + individuals based in Southeast London given the high prevalence of HIV in this region.
Data collection
Data were divided into two main categories: operational metrics and SU feedback. Operational data were derived from the LVNDR clinical dashboard to evaluate the overall delivery of the pathway in terms of service uptake and end-to-end completion (e.g., socio-demographics of participants), usage (e.g., remote testing, appointment attendance), and efficiencies (e.g., test kit return rate, time taken to complete the pathway). SU feedback was collected using a bespoke online questionnaire developed using Typeform. Post-pilot, SUs were provided with an information sheet that outlined the intent of the service evaluation. Written informed consent was obtained prior to completion of the self-administered questionnaire. Five major domains of user experience (defined as the period between downloading the App and receiving a prescription/follow-up care) were examined using Likert-scale items including time taken to access the service, service inclusivity (defined as the SU’s perception of their identity, values, and needs being respected), accessibility (defined as the SU’s perception that the service was designed around their availability/requirements e.g.,. Time/date of appointments, routes/timeliness of communication with LVNDR team), experience with the clinician, and overall satisfaction. The same questions were posed to SUs that had previously accessed PrEP who were asked to rate their most recent experience from a different service. Furthermore, the System Usability Scale (SUS), a Patient-Reported Outcome Measure (PROM), was implemented to explore the usability of the LVNDR App. To gauge overall satisfaction and determine the likelihood that users would recommend the service, a Net Promoter Score (NPS) was calculated. NPS is assessed by firstly asking “On a scale of 0–10, how likely are you to recommend this [product/service] to a friend or colleague?”. Individuals are then stratified by response into Promoters,9,10 Passives,7,8 and Detractors (0–6). The final NPS score is calculated as a probabilistic percentage measure by detracting the percentage proportion of Detractors from the percentage proportion of Promoters.
Data analysis
Given the sample size, non-normal distribution was assumed, hence non-parametric analyses were applied where relevant with p < .05 considered significant. Wilcoxon signed-rank tests were used to compare means scores for service user feedback for LVNDR vs a previous PrEP experience. Data were reported at a 95% CI in addition to Cohen’s d for effect size estimation. Between-group differences in SUS score were evaluated using a Kruskal-Wallis H test by stratifying group responses by socio-demographic and PrEP behavioural factors with >3 categories (e.g., age, ethnicity, previous PrEP use, sexual orientation, gender identity). A Wilcoxon rank-sum test was applied for binary variables (e.g., Born in UK). Cronbach’s alpha (α) was calculated as an internal consistency estimate of reliability for the SUS with α ≥ 0.7 considered to be acceptable.
Results
Cohort sample size & characteristics
Sociodemographic characteristics.

aEthnicity data were collected as a mix of drop-down and self-reported data leading to >18 ethnicities being coded for this variable. Data were therefore aggregated in line with the harmonised Standards for Ethnicity Data (2023) to support reporting and data analysis due to the limited sample size 24 .
Operational metrics (usage)
Remote testing summary
Of the 113 users, 81.4% (n = 92/113) received results from their first set of samples within the normal range and were invited to a consultation. Overall, 21 users had samples that were not deemed appropriate to proceed directly to a consultation. Those with an abnormal eGFR (<90 mL/min), uPCR (>50 mg/mmol), haemolysed or insufficient sample were given the option to retest via the LVNDR pathway. SUs with a reactive HIV or Hepatitis B results were referred to a local NHS service for confirmatory testing after a telephone consultation with the LVNDR clinical team to discuss their initial results and appropriate follow-up care. Of these 21 samples, 7 (n = 7/21, 33.3%) were identified with abnormal results providing an overall successful first test rate of approximately 88% (n = 99/113). After a follow-up with a LVNDR clinician, six of these users successfully retested via the LVNDR pathway and proceeded to be invited to book a consultation, whilst 12 opted to not return their second set of samples. Those with an abnormal eGFR or uPCR result that decided not to retest were included in a telephone or email follow-up, based on their communication preference, within 1–2 weeks of receiving the initial results. Advice was provided on further testing (if not with LVNDR) via their GP or sexual health service. Only one user presented with an eGFR <60 mL/min during initial testing, which resolved during follow-up with advice on completion of testing around physical activity, creatine/protein supplementation, and fluid intake. One transgender male SU presented with an initial borderline eGFR <90 mL/min. A further medical history was conducted via a telephone consultation prior to retesting, which confirmed the use of Gender-Affirming Hormone Therapy (GAHT) for an extended period (>5 years). In consultation with the SU and previous advice from their endocrinologist, the eGFR was retested using their affirmed gender, which provided an eGFR >90 mL/min. Further testing as part of the NHS referrals confirmed that those with reactive HIV and Hepatitis B samples were negative. The most common reasons for failed tests or abnormal results were as follows: • Abnormal eGFR and uPCR (4 users) • Haemolysed Blood Sample (8 users) • Insufficient Blood Sample (6 users) • Reactive HIV result (1 user) • Reactive Hepatitis B result (2 users)
Haemolysis was typically identified in users who reported previous difficulties with capillary blood testing for example, via similar remote testing service, or who did not follow the test kit instructions. Furthermore, 50% (n = 4) were received in the lab. after the typically accepted cut-off time range for samples (72 h), which may have been a contributing factor.
Appointment summary
In total, 101 users received an invite to book an appointment. Of those invited, four users (n = 4/101, 4%) did not book an appointment, therefore a total of 97 appointments were booked during the pilot. The SUs referred to the NHS (n = 3) returned to the LVNDR service for a follow-up telephone consultation but had already received PrEP during their NHS referrals and therefore were excluded from the “Attended” group for PrEP consultations as part of the LVNDR service. The breakdown of appointments is described below: • Attended (n = 90/97, 92.8%) • Referred to NHS for confirmatory testing (n = 3, 3.1%) • Cancellations that did not rebook (n = 2, 2.1%) • Did Not Attend (DNA) (n = 2, 2.1%)
Operational metrics (efficiency)
On average, SUs took 2.7 weeks (range = 0.8–5.4) to complete the end-to-end pathway with a mean appointment duration of 24 min (range = 11–57). Approximately 94% (n = 85/90) of SUs received PrEP medication by post within 48 h of their consultation. Of those five cases that exceeded the 48h cut-off, one instance related to a change of SU address, while the remaining cases related to issues with the mail service provider, for example, lost package. In all instances of a failure with the mail service provider, all SUs received a follow-up delivery so that 100.0% of SUs received their PrEP prescription during the pilot. While the pilot was orientated around SUs based in Southeast London, care was delivered digitally across a wide geographical area in the UK (Figure 1). Care Delivered by Borough/County. Notes: Purple sections denote a county/Borough in which a SU took part in the pilot and received a PrEP prescription.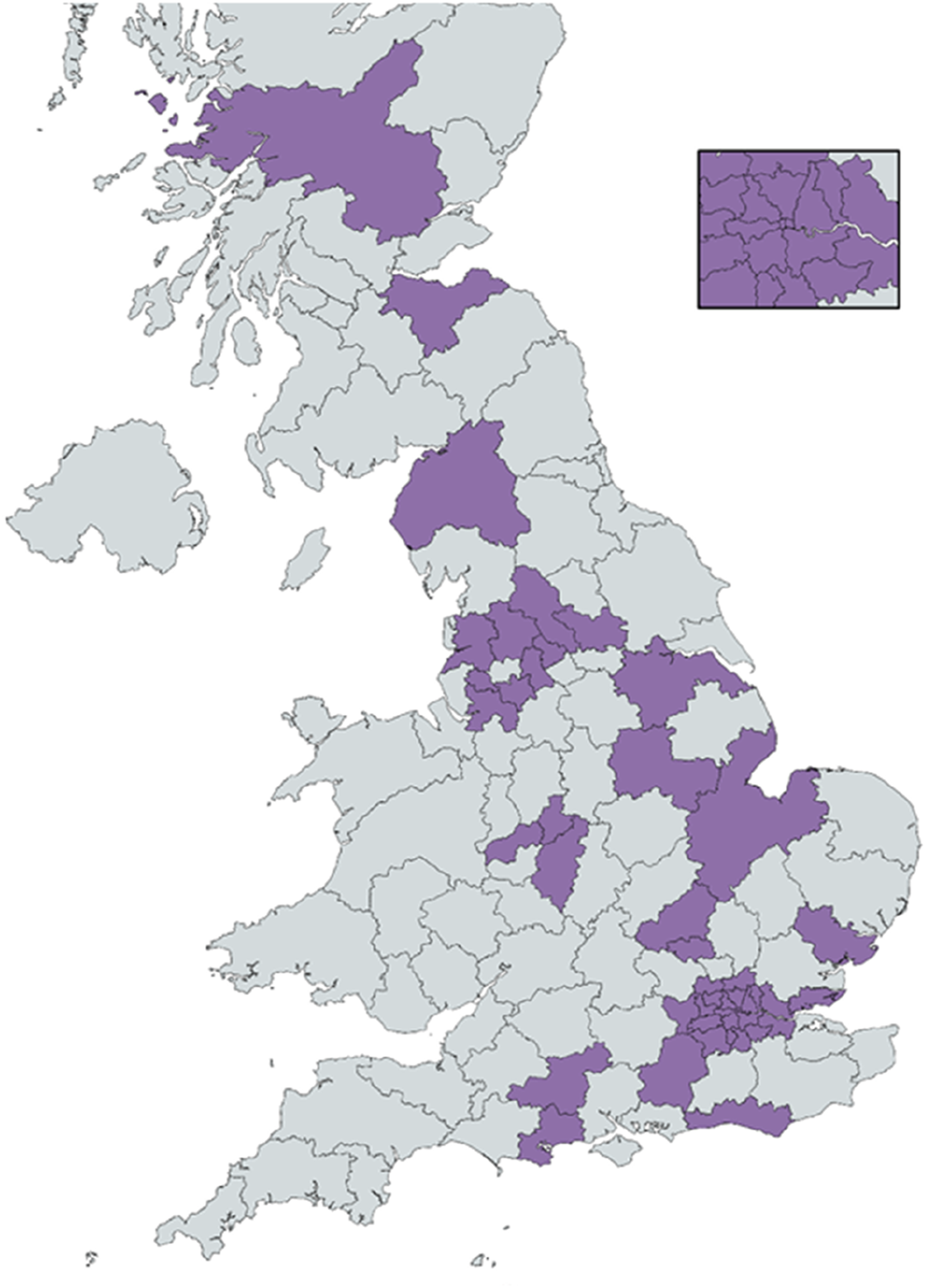
Service user feedback
Comparative analysis
Comparative Analysis of LVNDR vs Previous PrEP Service.

ap < .0001.
The reported likelihood of switching to the LVNDR service if publicly available was assessed using Likert-scale responses.1–5 A mean score of 4.8/5 was observed for the cohort, with 88.9% (n = 45/54) of users rating that they strongly agree that they would opt for an ePrEP service with LVNDR over their current modality of PrEP access.
Satisfaction & usability analysis
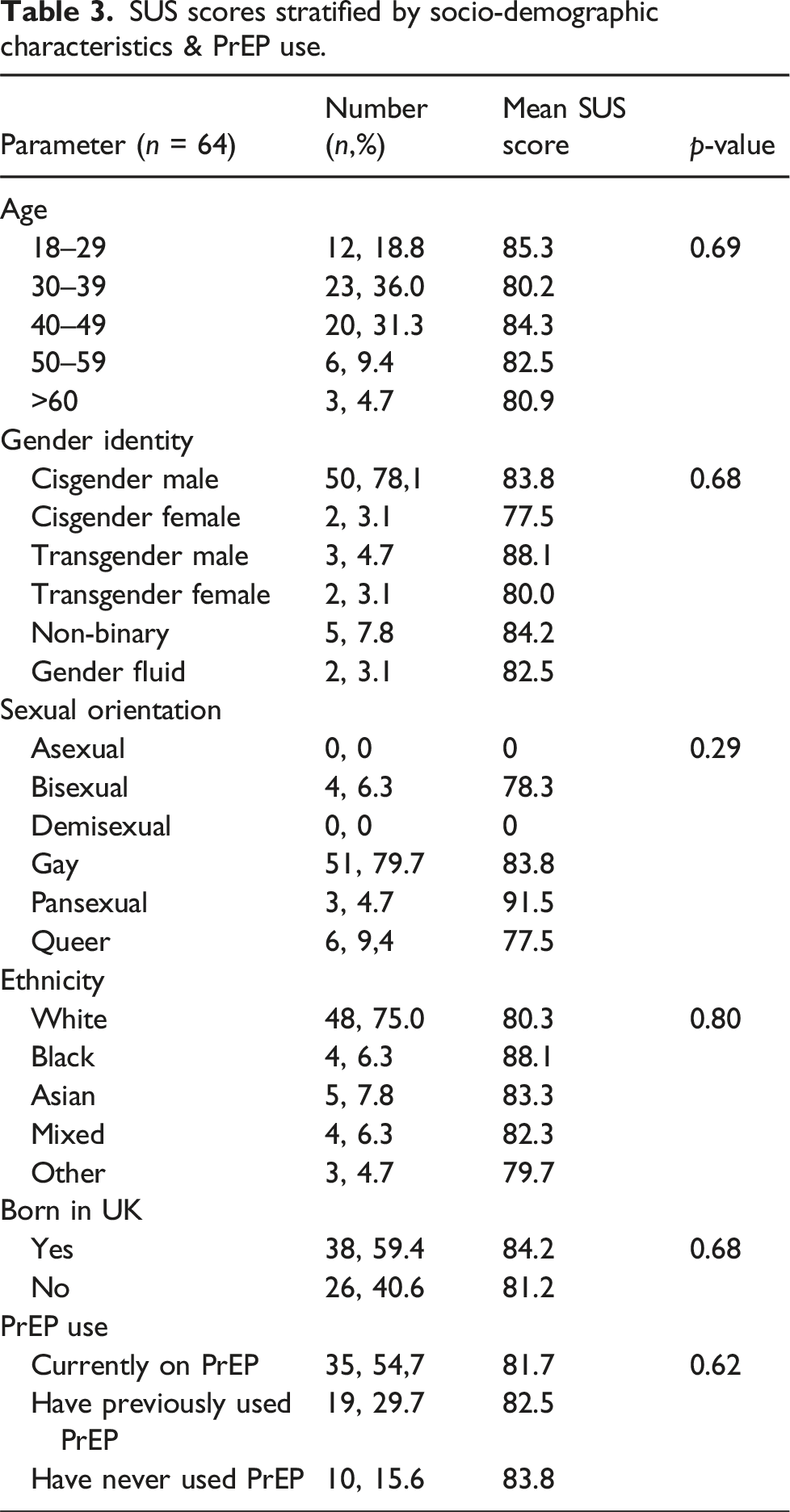
SUS scores stratified by socio-demographic characteristics & PrEP use.
Discussion
To our knowledge, this is the first service evaluation that provides early evidence from both an operational and user-feedback perspective to support an end-to-end digital PrEP service as an adjunct clinical pathway to current Level 3 PrEP services for LGBTQ + populations. The pilot looked to address some previously cited concerns regarding digital PrEP, namely co-development, inclusion of underrepresented populations (e.g., cisgender women), and the provision of suitable screening for all users prior to receiving a PrEP prescription.12–15 While these early results are encouraging, there are several limitations. Notably, while the minimum sample size target was exceeded, patients accessing the pilot were more likely to be ‘activated’ as well as previous users of PrEP. Hence, even participants from underrepresented groups that took part in the pilot may not reflect members of their wider communities that may be affected by additional factors such as digital exclusion, language barriers, or needs that may hinder access to a digital PrEP service, such as a learning disability. This may have also been influenced by selection bias, namely the recruitment process that was designed around the LGBTQ + community, those accessing/engaging with similar content, as well as individuals that had a smart device and used social media. Moreover, while between-group analyses were conducted and found to be non-significant, the sample size remains particularly small and is broadly comprised of white cisgender MSM; results should therefore be interpreted cautiously. Conversely, effect sizes and internal consistency estimates were evaluated to strengthen the results and supported the positive feedback outcomes associated with the digital PrEP pathway, particularly around usability with the implementation of the validated SUS. It is also relevant to consider that every patient, irrespective of their previous experience with PrEP, was treated as a “new” LVNDR patient. Hence, operational efficiencies (e.g., appointment duration, time taken to complete pathway) and the perceived usability of the App/service have the potential to improve significantly during repeat appointments with clinicians having access to a previous medical/drug history and patients’ increased familiarity with testing, consultation, and prescription procedures within the LVNDR App. Finally, broader STI screening was not conducted as part of the pilot. This limits the comparability to in-person services where a more comprehensive screening assessment may be conducted, increasing the overall time of the consultation. Any future digital PrEP service should therefore also look to include a broader STI screening process.
Conclusion
An end-to-end digital PrEP service may offer a suitable adjunct pathway to improve PrEP access and uptake among LGBTQ+ and other populations at risk of HIV transmission. Further work is required to determine feasibility at scale, needs of digitally excluded populations, and the potential health-economic impact for NHS organisations providing PrEP services.
Footnotes
Acknowledgements
The authors would like to thank all pilot participants, as well as the many users, clinicians, academics, and digital health subject matter experts that contributed to the initial co-development of the service, particularly those identifying as LGBTQ + who shared their own personal experiences to shape the LVNDR service and App. The authors would also like to extend their thanks to the wider LVNDR team of engineers, designers, researchers and many more that supported this project.
Author contributors
JW and JC conducted the data analysis and devised this project. JW and JC wrote the manuscript. AB and CB supported conceptualisation, reviewed the draft manuscript, and provided editorial input.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors are, or were, employees and/or shareholders of LVNDR Health Ltd. The funder designed the application setting in which the data was collected and was responsible for the study design.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by Funding for this paper was provided by LVNDR Health.