
Abstract
Background
Injection of opioids has contributed to growing HIV epidemics in Tajikistan and Afghanistan. This qualitative study explored determinants of access to primary prevention and screening for HIV among people who inject drugs (PWID) residing in border communities of Gorno-Badakhshan, Tajikistan and Badakhshan, Afghanistan.
Methods
Semi-structured interviews were conducted with PWID, community leaders, and healthcare workers. The social-ecological model was used to inform a thematic analysis of determinants of access.
Results
There were no preventive or screening services for HIV in the border districts of Afghanistan. Barriers to accessing HIV-related services in Tajikistan, and to accessing general health services in Afghanistan, included: lack of knowledge about HIV, inaccessible communities with poor infrastructure, discrimination and violence against women, and stigmatization of PWID and people living with HIV. Access to HIV-related and other health services by PWID was facilitated by community leader support, family support, outreach services, and linkage of harm reduction services with HIV testing and care.
Conclusion
Urgent interventions are needed to stem the escalating HIV epidemic in Afghanistan and enhance existing services in Tajik border communities. This qualitative study offers insights into barriers and facilitators for accessing HIV prevention and screening services among PWID, suggesting potential interventions.
Introduction
The growing HIV epidemics in Afghanistan and Tajikistan are a significant public health problem, especially among people who inject drugs (PWID). 1 Afghanistan is the world’s largest producer of opium and Tajikistan is a major transit hub of Afghan opium moving into Europe and Russia.1,2 Badakhshan in Afghanistan and Gorno-Badakhshan in Tajikistan are remote, hard-to-reach provinces located along the border in the Pamir Mountains, where cross-border shipments of opium have led to widespread drug addiction and a surge in parenterally transmitted HIV. 3
According to UNAIDS, there were approximately 15,000 people living with HIV (PLHIV) in Tajikistan in 2022 - 72% of whom knew their positive status. 1 Of all at-risk populations, PWID had the highest estimated HIV prevalence (8.9%). 1 In Afghanistan, there were an estimated 12,000 PLHIV in 2022, which reflected a 50% increase since 2010. 1 Of the PLHIV, only 27% knew their positive status, suggesting a significant gap in testing. Available data from Afghanistan estimated an HIV prevalence of 4.4% among PWID. 4
The great majority of the population in these border provinces of both countries live in poverty.5,6 In Afghanistan in particular, given the history of low economic productivity and political instability due to the ongoing civil conflict, the healthcare system is seriously underdeveloped. 7 As PWID constitute the highest-risk group for HIV in both countries, facilitating utilization of preventive HIV services for this population is crucial.4,8 Limited number of publications indicate significant barriers for PWID in accessing HIV preventive services in both countries.9,10 However, there are no published studies of the barriers to testing and preventive care among PWID in these border provinces. 11 The aim of this qualitative study was to identify barriers and facilitators to HIV testing and preventive services among PWID living in the border provinces of Gorno-Badakhshan in Tajikistan and Badakhshan in Afghanistan.
Methods
Sampling and data collection
Participants were recruited from six administrative districts — three in each of Gorno-Badakhshan and Badakhshan— which share the same names on either side of the Afghan-Tajik border: Ishkashim, Shugnan, and Rushan. In 2015, a non-random respondent-driven sampling (RDS) method was used to recruit 30 PWID (five per district) from drug rehabilitation centers in Tajikistan and Aga Khan Health Services (AKHS) in Afghanistan. Inclusion criteria were: (1) study district residents, (2) ≥18 years of age, and (3) injection drug use in the past year. The investigators were not able to recruit female PWID in Afghanistan. Instead, 16 Afghan women who used non-injection drugs were recruited to capture the perspectives of women who used drugs.
In-depth semi-structured interviews were conducted from May-December 2015. In Tajikistan, interviewers were research assistants from PRISMA Research Center who were familiar with the Gorno-Badakhshan region. In Afghanistan, interviewers were Afghan outreach healthcare workers from AKHS in Badakhshan. Both groups received the same 3-days training in qualitative research, and hands-on interviewing practice. The study design and analysis were guided by the social-ecological model. 12 Open-ended questions and probes were used to construct a phenomenological picture of the social-ecological context of HIV infection and drug-related risk behaviors in these communities. Interviews, conducted in Tajik or Dari, were audio-recorded, transcribed verbatim, and translated into English. Participants completed a brief questionnaire about their sociodemographic characteristics, and HIV-related risk behaviors.
To better understand the community and health system perspectives, in-depth interviews were conducted with 12 service providers (2 per district) and 24 community leaders (4 per district). In Tajikistan, service providers worked within organizations offering harm reduction services, the regional AIDS Center or other healthcare facilities. In Afghanistan, service providers worked with AKHS. Community leaders included teachers, coaches, policemen, commanders, local council chairs, and clergymen.
Data analysis
Qualitative thematic analysis was conducted using QSR NVivo (version 12). Interviews were analyzed using both deductive and inductive approaches, with key domains identified a priori, complemented with emerging domains. Key domains included determinants of drug use, drug-related risk behaviors, and utilization of harm reduction and healthcare services among PWID. Four researchers read the interviews and independently generated an initial list of codes to capture relevant themes and sub-themes. This list was refined through an iterative process of multiple transcript readings and discussions.
This was followed by a second round of coding by three other researchers to further explore themes and sub-themes related to the domain of access to HIV preventive services. This analysis focused on barriers and facilitators of access to HIV primary prevention services (use of condoms and clean injection materials) and HIV testing among PWID.
Ethics approval
The research protocol was approved by Columbia University’s institutional review board (IRB) (number AAAO5009) on December 18, 2014, and the PRISMA Research Center’s IRB in Tajikistan. Informed consent (verbal) was obtained from all study participants prior to each part of data collection. All interviews were conducted in confidential spaces. All personal identifiers were removed from the data for confidentiality. Approval for data analysis was also obtained from the IRB (number A09-E53-21B) at McGill University on September 24, 2021.
Results
Characteristics of participants who used drugs
Summary of socio-demographic characteristics and HIV risk behaviours of participants who used drugs.
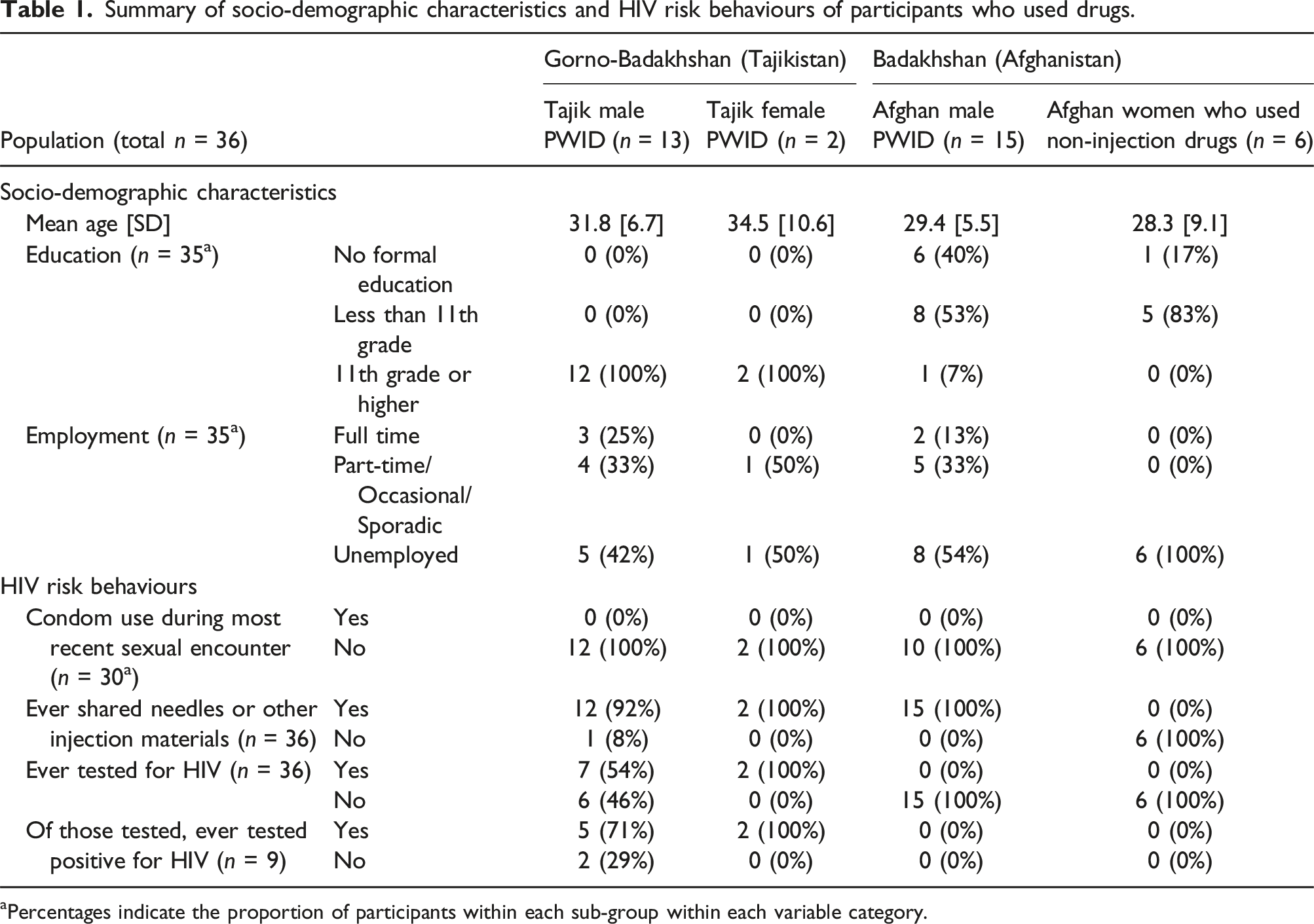
aPercentages indicate the proportion of participants within each sub-group within each variable category.
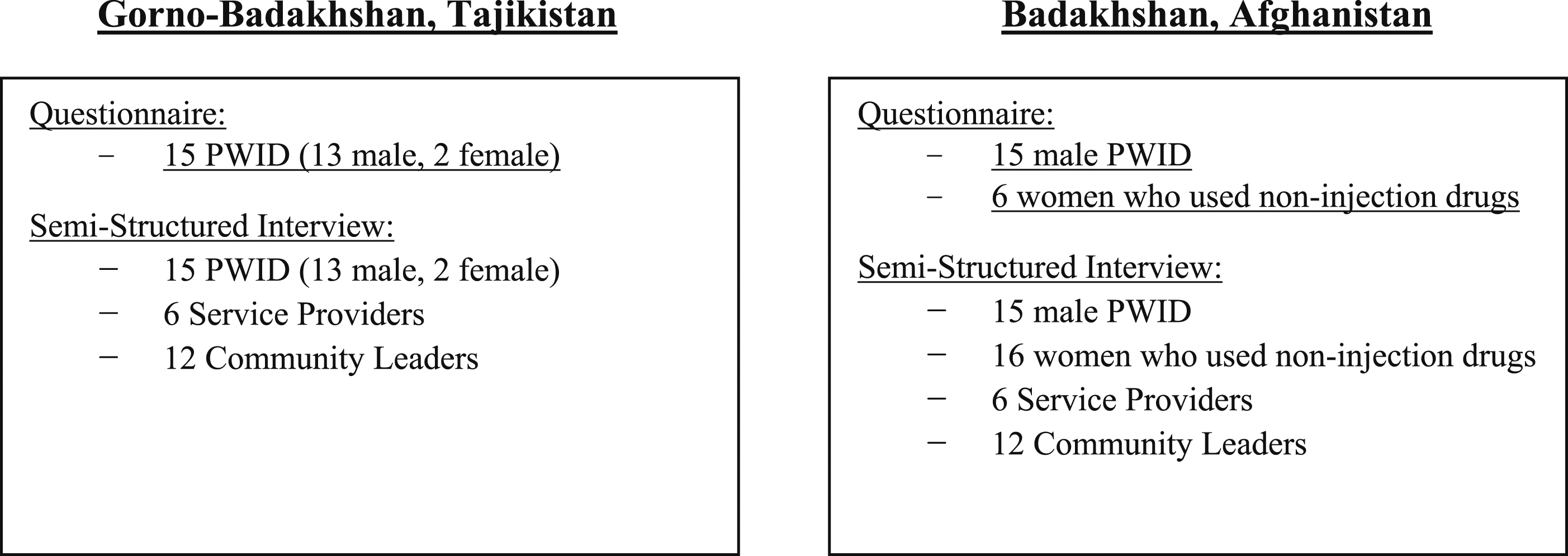
Number of individuals who participated in the sociodemographic questionnaire and semi-structured interview.
Barriers and facilitators to accessing primary and secondary HIV prevention services
Tajikistan
Intrapersonal barriers
Lack of knowledge about HIV transmission
Participants had limited knowledge about HIV and the role of condoms in prevention of HIV transmission. None of the PWID reported using condoms consistently (Table 1). Several male PWID said that their approach for HIV prevention was to avoid sex with women perceived to be at high risk of sexually transmitted infections (STIs). Women were often blamed for the transmission of HIV/STIs in the community. “… [sexually transmitted] disease is inside women [...] I just try not [to] have sex with the girls who are infected.” (25-year-old, HIV-positive male PWID, Tajikistan)
Several PWID perceived sharing needles among friends to be safe and indicated that they shared needles with peers. “I have heard that somehow HIV could be transmitted through needles [...] Most likely this is just to frighten [PWID] to stop using drugs, but in reality, there isn’t any connection between HIV and drug use, because HIV is a sexually transmitted disease.” (23-year-old male PWID, Tajikistan)
Afghanistan
Intrapersonal barriers
Lack of knowledge about HIV and prevention
The majority of participants who used drugs had no knowledge of HIV. Participants were also largely unaware of condoms, with some adding that condoms were not available or sold in the region. “I don’t know what you are talking about. Nobody uses anything when [they] have sex. These things are for “kuffor” (infidels). Muslims shouldn’t use these things [...]” (35-year-old male PWID, Afghanistan)
None were aware of the risk of HIV transmission through needle sharing. All Afghan PWID indicated that they shared needles and other injection materials (Table 1).
Tajikistan
Institutional barriers
Reduced availability of needle-exchange services in remote villages
While several PWID stated that they could obtain clean injection materials for free from drug harm reduction organizations in larger towns, those from remote villages indicated more difficult access.
Institutional facilitators
Linking HIV counseling and testing with harm reduction services
Organizations offering drug-treatment and harm reduction services also provided PWID with HIV counseling and referred them to health facilities for HIV screening and care. “I got treatment for drug addiction and then got tested for HIV. Then I learnt about [positive status] for the first time.” (42-year-old male PWID, Tajikistan)
All pregnant women, including those who used injection drugs, were routinely screened (obligatory) for HIV.
Outreach services
Certain organizations offering harm reduction services also offered outreach services to improve PWID access to clean injection materials. “We have volunteers in each of the villages in our jamoat [sub-district]… They could provide [health information], [and] have [clean] syringes and needles to distribute among clients who couldn’t visit our exchange points… We help [them] get tested for HIV, STI, and other conditions in primary care. Our volunteers also accompany clients to the AIDS Center [for HIV testing and care] or to [clinics] for any health problems.” (NGO Service Provider, Tajikistan)
Providers from a district hospital indicated that they offered outreach services to improve access to healthcare. These outreach services were particularly important for female PWID who were not at ease visiting service points.
Afghanistan
Institutional barriers
Physical inaccessibility of health services
Participants indicated that the border communities were among the most remote and inaccessible in Afghanistan. Due to treacherous highland routes, and lack of vehicles, physical access to existing health centers for basic services was challenging. Several remote villages were completely blocked during winter months.
Unavailability of HIV preventive services
Needle exchange services were unavailable in border communities. Several PWID and service providers reported these were available in larger cities, but were inaccessible to PWID due to the distance, and the financial inability of PWID to afford the cost of travel and health services in other jurisdictions.
Healthcare providers also indicated that HIV screening and care were generally unavailable, and that general health services in Badakhshan communities had only recently become available through the establishment of AKHS clinics.
Institutional facilitators
Outreach services
Several health providers stated that people in remote villages became aware of their services through clinic outreach workers. Health providers highlighted that deploying female outreach workers with an accompanying male chaperon could help to overcome cultural barriers and improve access to services for women and their children in remote communities.
Tajikistan
Societal barriers
Stigma towards PWID and PLHIV
Tajik community leaders expressed a negative attitude towards PWID, with some suggesting that they should either be sent to Russia or incarcerated. Moreover, lack of knowledge about HIV, HIV transmission, and the effectiveness of ART contributed to strong community-based fear of and discrimination against people living with HIV. “Because [people] do not know what HIV is, they heard that it is incurable [...] most [people] think that it could be transmitted even through the air and kill [everyone] in our village. Therefore, nobody [reveals their] positive HIV status to [others]… I’m afraid that if somebody in my community [finds out] that I’m HIV infected, they will kill me.” (37-year-old male PWID, Tajikistan)
A service provider also explained that due to fear of double stigma (towards injection drug use and HIV), PWID were not forthcoming to be screened for HIV. Consequently, many PWID were diagnosed with HIV at later stages, upon presentation to clinics due to AIDS-related health problems. Participants also indicated that drug overdose suicides were common among PWID upon learning their HIV status.
Discrimination against women
Participants expressed that women had lower social status than men in Gorno-Badakhshan. Several male and female PWID mentioned that women were expected to be submissive to their husbands (or other household patriarchs) or face violent consequences. Female PWID indicated that they were afraid and unable to ask their male partners to use condoms during sex. Male PWID blamed women who had extramarital sex for HIV and STI transmission in their community. “We never use condoms. I have a spiral. [If I ask my husband to use a condom] most likely he would become jealous and beat me.” (27-year-old, HIV-positive female PWID, Tajikistan)
Notably, community leaders and PWID suggested that injection drug use and positive HIV status were more stigmatizing for women than for men. Service providers highlighted that this led to much greater difficulty for women to openly access harm reduction services. “It is too shameful to be a drug user for women. Therefore, they leave their home and their region after people find out about their drug use[...] If [they have] brothers, then I think they would force [them] to stop using drugs or would just kill [them].” (Hospital Physician, Tajikistan)
Societal facilitators
Community leaders’ support for harm reduction services
Most community leader participants expressed favorable views towards HIV harm reduction services to reduce HIV risk in their communities. Despite their negative attitude towards PWID, most community leaders endorsed the efforts of organizations offering free access to clean needles and syringes for PWID. Healthcare providers, including physicians and organization leaders who were influential public figures, also prioritized addressing HIV prevention among PWID. “[The major health issue among PWID] is HIV, because most HIV-infected people in Tajikistan are [PWID] and most [PWID] are HIV-infected.” (Hospital Physician, Tajikistan)
Family support
Several PWID indicated that their families supported them financially and facilitated their access to food, housing, and medication. This was especially instrumental for female PWID who were less comfortable with openly accessing harm reduction services by themselves.
Afghanistan
Societal barriers
Lack of prioritization of HIV
All participants, including people who used drugs, community leaders and healthcare workers, expressed that HIV was rare or non-existent in the region. “We don’t have HIV. Most of our people never heard [of] HIV. I have very close contacts with the doctors in our district clinic and I’m sure they would inform me about any cases of HIV… Fortunately till today, I [have] never heard about any HIV infected people in our district.” (Community Leader, Afghanistan)
Most healthcare providers also suggested that because HIV was rare, HIV prevention and care were not considered priorities in the region. Also, although all participants indicated that opioid use was prevalent, healthcare providers and community leaders suggested that injection of opioids was uncommon. “In big cities people have some access to HIV services, but not here. Fortunately, we don’t have HIV infected people here yet. The number of PWID is very low, people do not practice chaotic [sex], and we don’t have sex work here.” (Healthcare Provider, Basic Health Center, Afghanistan)
Discrimination against women
Interviews with all participants in Badakhshan highlighted prevailing discrimination against women. Participants expressed that women were considered “property” of men, and they had no autonomy over any aspect of their lives, including sexuality and access to health services. Women were obliged to obtain their husband’s permission to leave the house to access health services for themselves or their children. Male PWID participants expressed that if their wives left home without their permission, they would be punished through “beating”. All female participants using drugs described having experienced violence by men. “My husband does not let me [go out of the house]. When I need to go to the clinic, then my husband’s brother [has to] accompany me.” (30-year-old female using non-injection drugs, Afghanistan)
Discussion
Although needle exchange services and HIV testing were generally available in Gorno-Badakhshan in Tajikistan, barriers across multiple levels of the social-ecological model complicated PWID access to these services. Societal and institutional barriers contributed to the lack of availability of HIV preventive services in border communities of Badakhshan, Afghanistan. At the intrapersonal level, PWID from both countries had little knowledge about HIV and reported high-risk behavior for HIV transmission, including needle sharing and condomless sex.
Key societal barriers to accessing services included stigma against PWID and PLHIV in Gorno-Badakhshan (Tajikistan), and discrimination against women in both countries—particularly in Afghanistan—as shown in other studies.10,13,14 Interviews with participants in both countries indicated that enhancing outreach health services at the institutional level could help improve access to basic and HIV-related services, especially for women and PWID facing discrimination; this strategy is supported by the WHO. 15 Also, health providers in both countries highlighted that other evidence-based strategies at the institutional level, including training and deploying more female healthcare workers, along with provision of incentives to families, could be instrumental for improving access and utilization of health services for women.16–18 Tajik interviews underscored the importance of linking drug harm reduction services with HIV counseling and testing, to improve PWID’s knowledge of HIV transmission, and to streamline their access to preventive care, as shown in other studies.19–21
In Badakhshan (Afghanistan), in addition to the lack of HIV knowledge among PWID, healthcare providers and community leaders believed that HIV and injection drug use were uncommon. Consequently, HIV-related and harm reduction services were not prioritized at the institutional and societal levels. However, based on UNAIDS estimates, the number of new HIV infections has steadily increased in Afghanistan, including from 2015 to 2022. 1 Studies also reveal that the number of PWID has increased, and sharing contaminated needles is one of the most common risk factors for HIV transmission in Afghanistan.22–24 On the contrary, in Tajikistan, health stakeholders and, notably, community leaders were cognizant of the HIV burden, particularly among PWID. The leaders comprehended and endorsed the importance of HIV harm reduction strategies and screening, serving as influential societal facilitators. According to the UNAIDS estimates from 2015 to 2022, HIV incidence has stabilized and appears to have declined in Tajikistan. 1 While this study focused on border communities in Gorno-Badakhshan, we believe that these societal facilitators were likely widespread across Tajikistan and could also be applicable to curb the HIV epidemic in Afghanistan.
A limitation of this study is the small sample size of PWID, which can limit the generalizability of the findings. The stigma of injection drug use may have affected participation. Also, especially in Afghanistan, participants who used drugs skipped certain questions. It is possible that they skipped or may not have reliably answered questions, for example, those regarding sexual experiences, due to cultural sensitivity or a lack of understanding of the questions. The respondent-driven sampling method of recruitment may have introduced selection bias, such as favoring participants with similar characteristics and behaviours. For example, younger PWID (aged <25) and female PWID were underrepresented in this study. Moreover, in Afghanistan, investigators were not able to reach women who used injection drugs. Finally, the data for this study was collected in 2015. However, based on more recent available information, the health services, political system, and civil infrastructure have not shown significant improvement in Tajikistan,25–27 while the situation in Afghanistan appears to have deteriorated.28–30
Our study offers insights into multi-level barriers and facilitators for accessing HIV prevention and screening services among PWID in border communities of Tajikistan and Afghanistan. The findings from this study can fill a current data gap regarding the intersecting epidemics of intravenous drug use and HIV in these border communities, and may inform current and future public health interventions.
Footnotes
Acknowledgements
We acknowledge: all participants in this study in Tajikistan and Afghanistan; the researchers who executed the study, including Dr. Nabila El-Bassel (Columbia University, U.S.A.); and the healthcare workers at Aga Khan Health Services in Afghanistan and Tajikistan.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Alissa Davis received support from the U.S. National Institute on Drug Abuse (NIDA) (K01DA044853) and the National Institute of Mental Health (T32MH019139, P30MH043520). Dr. Phillip Marotta and Dr. Anindita Dasgupta received support from the NIDA (T32DA037801). Harsimren Sidhu and Frezghi Gebreweldi received financial support from McGill University. This study was supported by internal funds from Columbia University.