
Abstract
Human papillomavirus (HPV) is a common sexually transmitted infection with wide-ranging clinical manifestations. High-risk anogenital HPV genotypes have also been reported to cause extragenital disease. We describe the case of a 69-year-old male patient living with HIV who was diagnosed with HPV-16 associated Bowen’s Disease (BD) of the right middle finger nailbed, despite good virologic control and immune reconstitution. The lesion was managed surgically with adjunctive post-exposure HPV vaccination. This case adds to the growing body of evidence of extra-genital HPV disease attributable to anogenital genotypes in people living with HIV.
Keywords
Introduction
Human papillomavirus (HPV) is the most common sexually transmitted infection globally, and can cause a wide spectrum of clinical manifestations; ranging from benign to pre-malignant and malignant lesions.1–3 High-risk (HR) HPV genotypes 16 and 18 are among the most common HPVs detected and are a significant risk factor for malignant disease, typically at anogenital sites.1,2,4 People living with HIV are at greater risk of HPV-related disease.2,5 Despite the advent of antiretroviral treatment (ART), a lower nadir CD4 count has been associated with severe HPV-related disease, even after successful HIV viral suppression and CD4 count recovery.2,3,5 Bowen’s Disease (BD) is a pre-malignant lesion of the skin associated with ultraviolet (UV) light at sun exposed sites, and with HR-HPV and lichen sclerosus at genital sites.6–8 Cases of extra-genital cutaneous disease caused by genital HPV genotypes have been reported, including HPV-16 associated BD of the nailbed and fingers.9–14
Case report
A 69-year-old male with well-controlled HIV was referred to Dermatology with a 2-years history of pain, swelling, and nail dystrophy of the right middle finger. He had a past medical history of hyperlipidaemia, transient ischaemia attack, and hiatus hernia. He was diagnosed with HIV in 2010 with baseline HIV viral load of 140,000 copies/ml and nadir CD4 count of 60 cells/mm3. After initiation of ART with tenofovir-disoproxil (TDF), emtricitabine, darunavir, and ritonavir, viral suppression was achieved within 5 months and had been maintained since. The CD4 count had reconstituted to 620 cells/mm3 within 12 months of ART initiation.
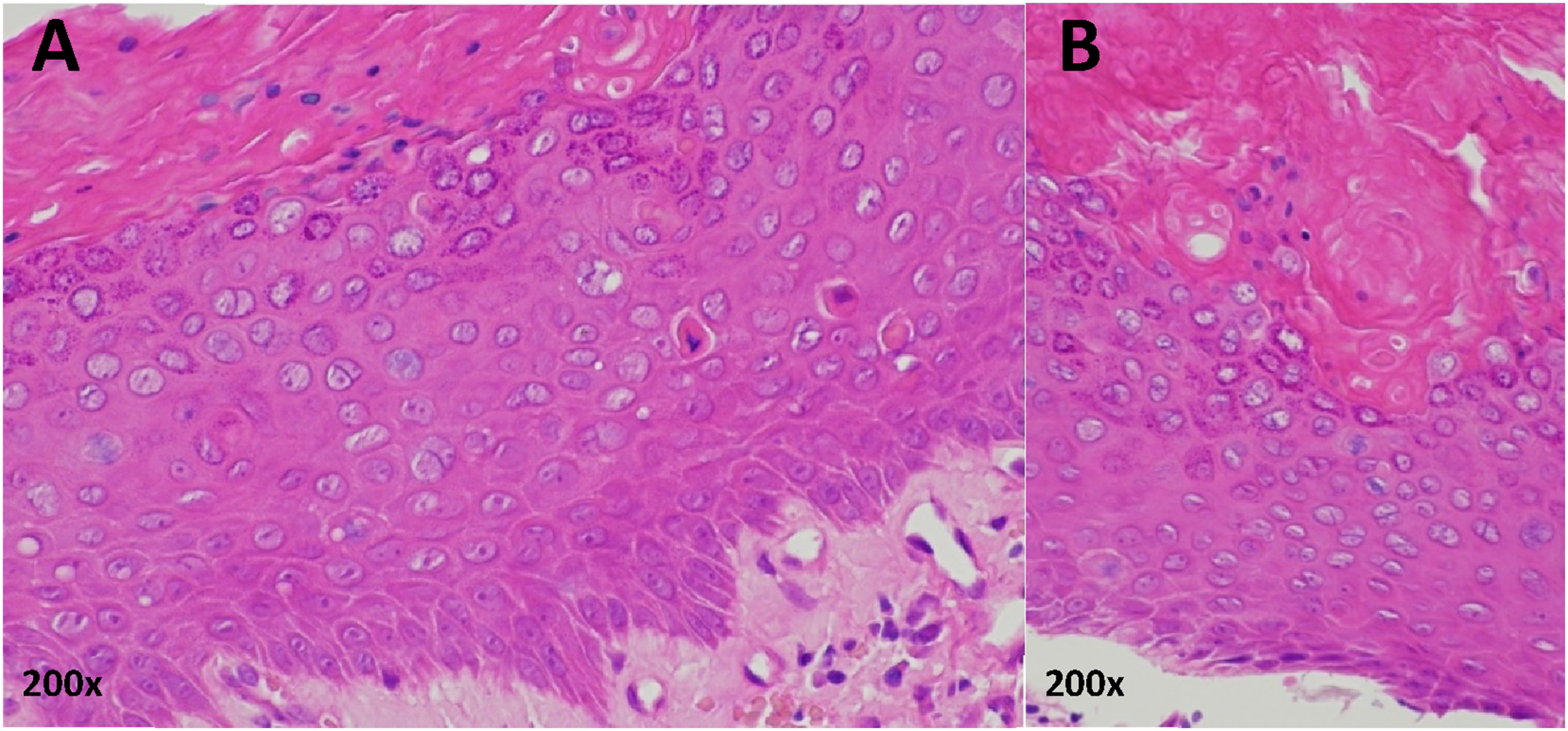
In June 2016, the patient was seen in the Dermatology clinic with changes to the right middle fingernail and was diagnosed with chronic paronychia. At the time, his CD4 count was 980 cells/mm3. He was a smoker with a 10-pack year history. He was prescribed Dermovate® (clobetasol propionate 0.05%), Trimovate® (clobetasone butyrate 0.05%, oxytetracycline 3%, nystatin 100,000units/g), and acetic acid soaks, and was discharged from the service. In July 2019, he was re-referred to Dermatology with a suspected right middle finger nailbed viral wart. He continued to smoke cigarettes. On examination, the right middle fingernail was found to be dystrophic laterally with erythema and swelling of the proximal nail fold (Figure 1). No other fingernails were affected. A biopsy was undertaken, and the histological findings were in keeping with BD of the nailbed (Figure 2). HPV genotyping confirmed the presence of HPV-16. Clinical photographs showing the appearance of the patient’s right middle finger over time: (a) at the time of the patient’s second presentation to dermatology (July 2019), (b) 10 months later and after a diagnostic biopsy had taken place confirming Bowen’s disease due to high-risk HPV (May 2020), (c) following further deterioration of the nail (January 2021), (d) following excision and skin grafting (February 2022). Histology of right middle finger nailbed biopsy (haematoxylin and eosin, October 2019). Two high power views (200x magnification) from a single histologic sample (a) and (b). Sections from the nail biopsy show parakeratosis and irregular acanthosis. There is full-thickness dysplasia of the epidermal keratinocytes and suprabasal mitotic activity amounting to Bowen’s disease.
Following progression of the nailbed disease (Figure 1), in January of 2020 the patient was advised to have the area excised. The patient initially declined excision, and in May of 2021 started a 3-dose schedule of Gardasil-4® post-exposure HPV vaccination. In June of 2021 the patient agreed to proceed with surgery. Excision with full-thickness skin grafting was undertaken; the histology revealed dysplasia extending to the peripheral margins of the sample. A repeat excision was thus undertaken with further histology showing no residual BD. Gardasil-4® HPV vaccination (covering HPV-6, HPV-11, HPV-16, and HPV-18) was completed in December 2021 and at follow-up in February 2022 no residual lesion could be detected (Figure 1). In June 2022, the patient underwent high resolution anoscopy with anal cytology and biopsies, and no evidence of anal intraepithelial neoplasia (AIN) was found. HPV detection was not performed on these samples.
Discussion
This case adds to a growing body of reported cases on extra-genital manifestations of genital HPV disease. Nailbed HR-HPV disease, particularly in people living with HIV, is an emerging entity in the literature.9–14 Any site involved in sexual activity is at risk of infection with ‘anogenital’ HR-HPV strains and may bear the consequences of that. People living with HIV remain at increased risk of HR-HPV associated disease, despite good virological control and immune reconstitution. When assessing atypical cutaneous lesions in people living with HIV, the nadir CD4 count should be considered a potential risk factor for pre-malignancy or malignancy.3,5 Alongside historic immunosuppression, smoking was an additional risk factor for HR-HPV disease in this patient, and smoking cessation advice should form part of management for all HPV disease. 6
Prophylactic HPV vaccination, primarily for girls, was first introduced in 2006 leading to marked reductions in cervical cancer and cervical intraepithelial neoplasia (CIN). 4 There is also growing evidence and ongoing research on the utility of post-exposure vaccination for HR-HPV disease.4,6,15 A meta-analysis of 11 studies found that post-exposure HPV vaccination significantly reduced CIN2/3 recurrences (n = 19,909; risk ratio 0.43; 95% confidence interval 0.30-0.60), with recurrences of HPV-16 and HPV-18 associated CIN reduced even further (n = 1879; RR 0.26; 95% CI 0.16-0.43). 15 Whilst prophylactic HPV vaccination is now recommended for all children in the UK, this is not the case in all countries and many adults remain unvaccinated. 16 Post-exposure HPV vaccination should be considered for all those diagnosed with HR-HPV-related disease. 15
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.