
Abstract
Background
Sexually transmitted infections (STIs) cause adverse health outcomes, including increasing HIV acquisition/transmission risk. We analyzed data from an HIV biomarker and behavioral survey to estimate STI prevalence, and explore associated factors in the setting of a generalized HIV epidemic in Siaya County, western Kenya.
Methods
Data were collected in March–September 2022 through face-to-face interviews using structured questionnaires; records from 9643 sexually active participants aged 13+ years were included in the analysis. We calculated weighted self-reported STI prevalence, by sex, age, and HIV status and explored associated factors using multivariable logistic regression.
Results
Median age was 37 years and 59.9% were female; HIV prevalence was 18.0%. Overall STI prevalence was 1.8%; 1.5-fold higher among males vs. females, and 2.6-fold higher among participants living with HIV vs. those without. HIV status and multiple sexual partners were independently associated with STI in both sexes. Mind-altering substance use and being circumcised were associated with STI among males.
Conclusions
This study estimates STI prevalence in the setting of high HIV prevalence. Findings underscore the importance of: effective STI screening in HIV clinics and HIV testing and counseling in STI clinics; screening and counseling on substance use, and HIV pre-exposure prophylaxis; and intensive sexual health counseling in male circumcision programmes.
Introduction
The World Health Organization (WHO) estimates 357 million new cases annually with one of four curable sexually transmitted infections (STIs) (Chlamydia trachomatis, Neisseria gonorrhoeae, Syphilis, Trichomonas vaginalis) worldwide, including 63 million in sub-Saharan Africa (SSA).1,2 STIs increase the risk of acquiring or transmitting HIV; cause human cell changes that may lead to some cancers; result in pregnancy complications, including fetal and neonatal deaths and infertility; and result in other detrimental physical and psycho-social consequences in affected individuals.3–6
Published studies on STIs in SSA2,5–7 have found that the burden of STIs in this region is high6–8 and increasing.3,7–10 A temporal trend analysis of STIs from 2010–2019 by geographical region and age-group found that southern SSA had the greatest increase in age-standardized incidence rates for trichomoniasis (estimated annual percentage change, 0.88) and greater growth in incident cases of syphilis, chlamydia, gonorrhoea, trichomoniasis, and genital herpes than was observed in western and central SSA. 8 A systematic review and meta-analysis of studies published between 1999–2019 on curable STIs among SSA women showed a pooled prevalence of 3.5, 4, 15.6, and 10.2% for gonorrhea, chlamydia, trichomoniasis and M.genitalium, respectively. An analysis of HIV/STI epidemiology, management, and control in SSA found that, in 2011, adult prevalence of herpes simplex virus type 2 (HSV-2) was 30–80% in women and 10–50% in men. 10 The same analysis found that new cases of gonorrhea, chlamydia, trichomoniasis and syphilis increased by 59.1% between 1999 and 2005. 10 Another meta-analysis of 18 HIV prevention studies conducted among women in SSA indicated a high prevalence of chlamydia, gonorrhea, trichomoniasis, syphilis, and HSV-2 and further observed that prevalence varied by age, region, and specific sub-populations. 9 Studies have shown some general correlates of STIs including being female, living with HIV, having had unprotected sex and having multiple sexual partners.11–15 WHO guidelines highlight the critical need for age- and sex-disaggregated data on the occurrence of STIs to estimate the burden of disease, target prevention strategies, and monitor program impact.2,4,16
Individuals living with HIV have a disproportionally high burden of STIs. A systematic review of STI/HIV co-infection among HIV-positive adults from 37 studies across low, middle and upper-income countries found an overall STI prevalence of 16.3%. 17 The meta-analysis of 1999-2019 studies found that the four curable STIs were more prevalent among women with than without HIV (relative risks ranging 1.54–1.89). 7 Furthermore, the rates of STIs are increasing in some HIV-positive and key populations. 18 This trend has been attributed, in part, to increases in behaviors associated with STI, including condomless last sex among people taking pre-exposure prophylaxis (PrEP) and people living with HIV on antiretroviral (ARV) medications, owing to reduced fear of acquiring/transmitting HIV, respectively. 18
Kenya is among the countries in SSA with the highest burden of HIV, with an estimated 1.4 million people living with HIV, 33,000 new infections, and 1.2 million people living with HIV on antiretroviral therapy (ART) in 2020. 19 Studies in Kenya have shown that people living with HIV,15,20–25 adolescents,26,27 female sex workers,23,28 and fisherfolk populations around Lake Victoria in western Kenya 24 are disproportionately affected by STIs; however, studies on STI prevalence and risk factors in the general population are limited. We analyzed data from an HIV bio-behavioral survey conducted in western Kenya to estimate the prevalence of self-reported STIs in the population, and to identify sociodemographic factors and behaviors associated with STIs.
Methods
Study design and population
Our study was an analysis of cross-sectional data collected in March–September 2022 as part of a longitudinal HIV bio-behavioral survey (LBBS) conducted in Siaya County, Kenya, where HIV prevalence (15.3%) is substantially higher than the national estimate (4.9%). 29 The LBBS started in 2010 and is nested within a well-established health and demographic surveillance system (HDSS), which covers approximately 240,000 residents across three administrative areas (Gem, Karemo, and Asembo). In this mostly rural region, fishing and agriculture are primary sources of subsistence/income. 30 Each LBBS round covers the 6890 residential compounds selected using simple random sampling in 2010, as well as compounds within Gem HDSS in which a participant from an earlier round resided. Residents aged 13 years and above who either lived, or spent the night preceding the survey, in a study compound were eligible to participate. Data analysis included all participants who reported ever having sex and responded “yes” or “no” to the study question about having an STI in the past 12 months.
Study procedures and ethical considerations
Informed consent was done based on participant’s preferred language (Dholuo, English or Swahili). Adults aged 18 years and above and emancipated minors gave written consent. Minors aged 13–17 years provided written assent in addition to written consent obtained from the parent/guardian. Parental consent was obtained first, after which, the rest of the procedures were conducted in the absence of the parent/guardian. Face-to-face interviews, using a structured questionnaire collected information on demographic characteristics, and sexual and behavioral HIV risks, including history of STI diagnosis in the past 12 months. Questionnaires were programmed in the three languages in CommCare mobile app, an advanced Open Data Kit application and participants chose their preferred language. Home-based HIV testing and counseling was offered to all participants who did not have a valid documented previous HIV diagnosis, according to Kenya Ministry of Health (MOH) guidelines.31,32 Interviews and HIV testing were conducted in private and safe venues of participants’ choice. All data were entered into CommCare in the field using tablets, auto-synchronized to the study server, and downloaded for cleaning, analysis, and archiving. An anonymized analytic dataset was generated by removing participants’ personal identifying information and retaining only the unique study identifier.
The study protocol was reviewed and approved by Kenya Medical Research Institute Scientific and Ethics Review Unit (KEMRI/SERU) (#1801) and United States Centers for Disease Control and Prevention (CDC) institutional review board (#3308).
Outcome variable
New STI
Participants were asked: “Have you had a new sexually transmitted infection in the last 12 months?” to which response options were “yes,”, “no,”,” “don’t know,” or “refuse to answer.” The interviewer explained STI using a standard explanation and gave examples: “By STI, I mean having an infection in your genital parts and being informed by a health care provider that you had a sexually transmitted infection. Examples of STIs include gonorrhoea, syphilis, chlamydia, etc.”. We calculated the weighted self-reported STI prevalence as a proportion of those who reported having had an STI out of all study participants. Other variables of interest are defined in Supplemental Table 1.
Statistical methods
Statistical analysis was performed using Stata version 17 (StataCorp. 2021. Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC.). We present weighted STI prevalence and 95% confidence intervals (CI) by age, sex, and HIV status. Individual-level weights were applied based on the inverse product of the probability of a compound being selected out of all the compounds in the study area and the number of people interviewed per compound out of the total number of the compound residents at the time of the interview. Associations between self-reported STI and other variables were explored using univariable and multivariable logistic regression, calculating unadjusted and adjusted odds ratios (OR) and 95% CI. Variables selected for the univariable analysis were those that have been associated with STI in the literature and/or are particularly relevant to the western Kenya context. Variables in the univariable analysis that had a p-value <0.2 were tested in the multivariable model. In the final multivariable model, we used the backward stepwise elimination while retaining significant predictors at p < 0.05.
Results
A total of 12,801 participants aged 13 years or older were enrolled in the study. Overall, 75.5% (9671) of participants reported ever having sex, of whom 99.7% (9643) responded to the question about having an STI in the past 12 months: 169 (1.7%) responded “yes,” 9474 (98.3%) responded “no” (Figure 1). Participant records from 2022 Siaya County LBBS included in STI analysis — Siaya County, Kenya.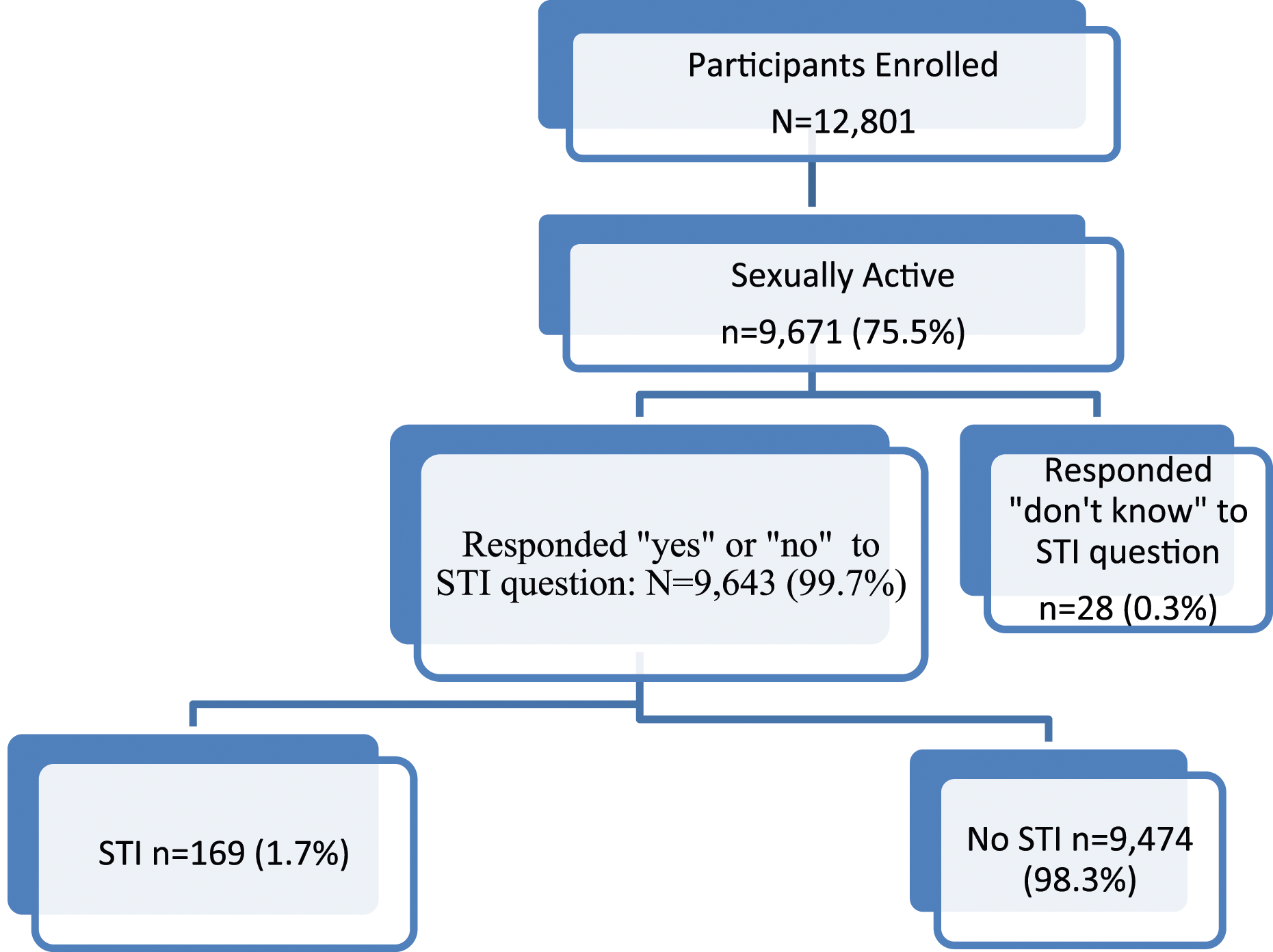
Study participant characteristics, weighted prevalence of self-reported STI by HIV status, age and sex, and the results of the regression analysis are presented below.
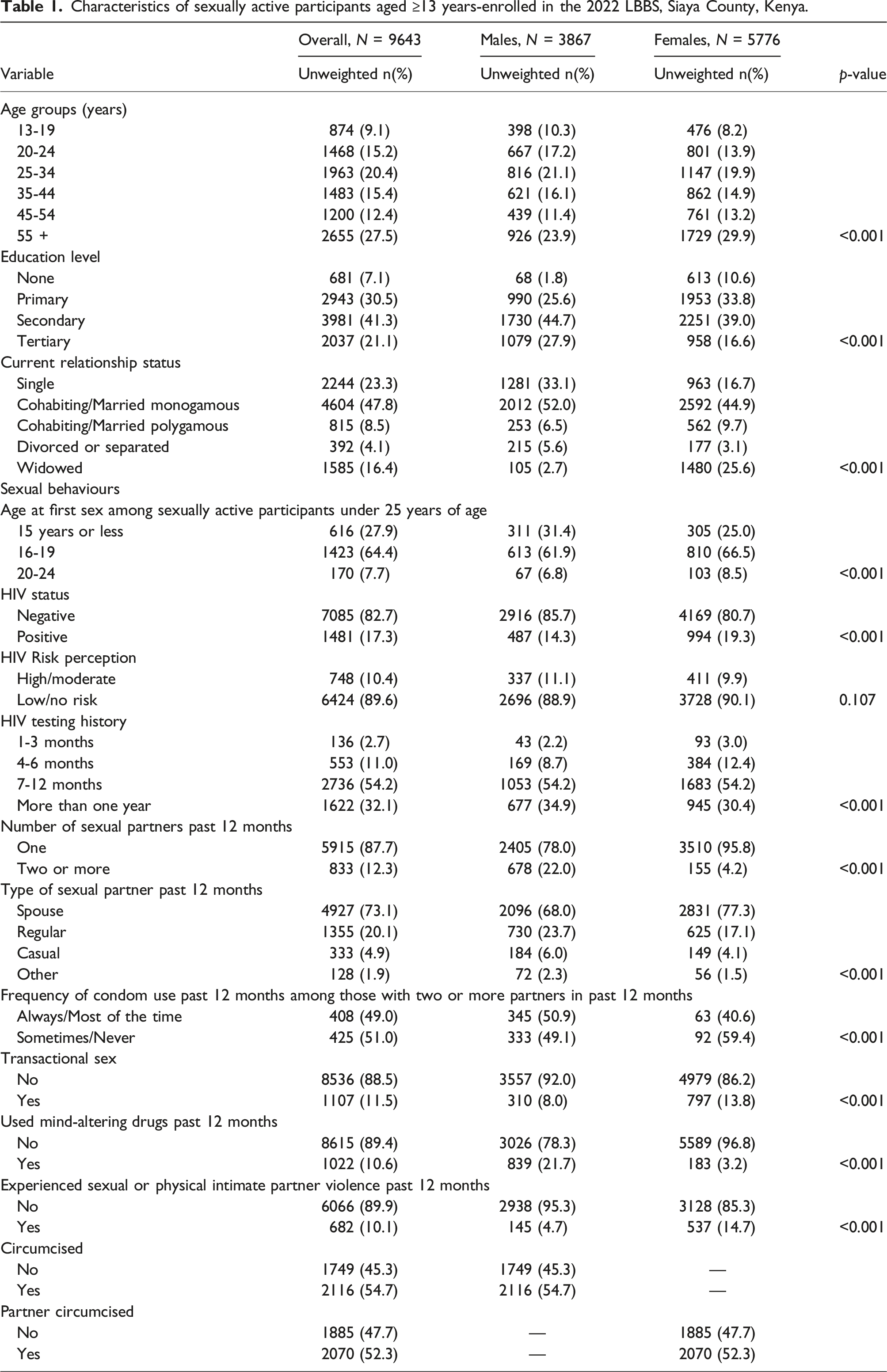
Participant characteristics
Characteristics of sexually active participants aged ≥13 years-enrolled in the 2022 LBBS, Siaya County, Kenya.
Self-reported STI prevalence
Self-reported STI prevalence by age, sex, and HIV status among sexually active persons aged ≥13 years enrolled in the 2022 LBBS, Siaya County, Kenya.
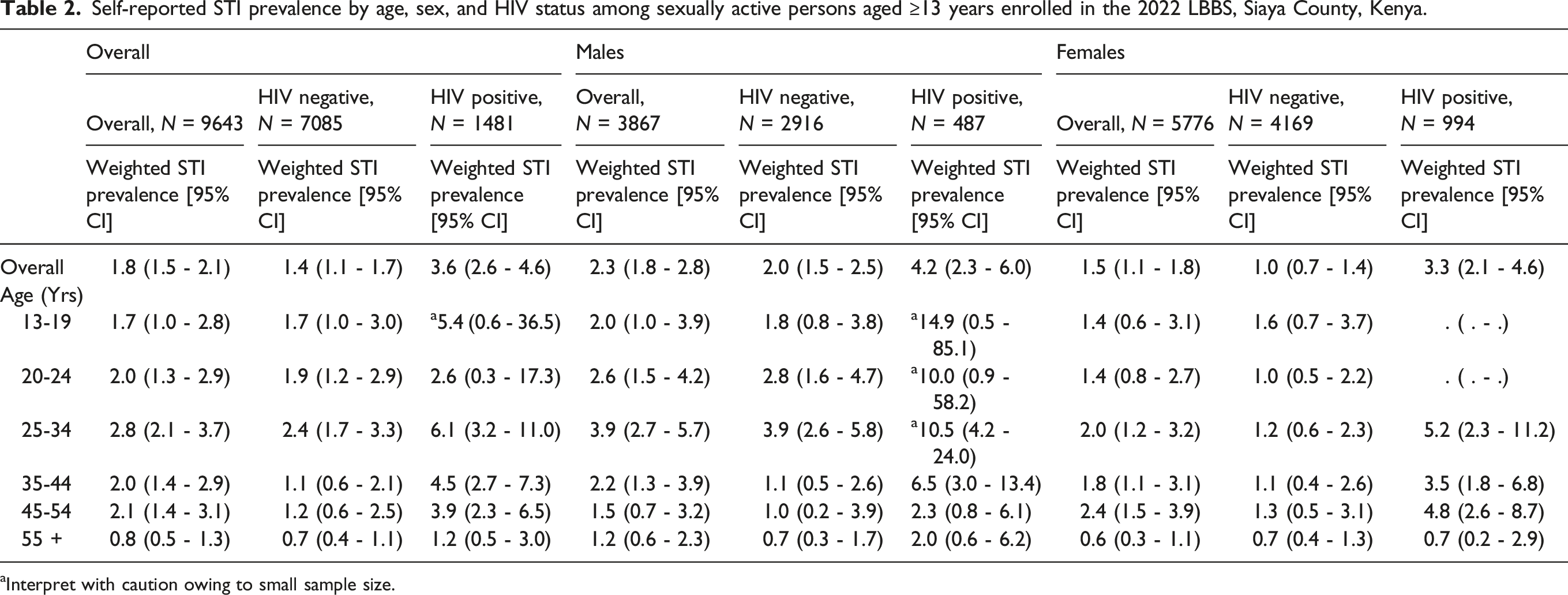
aInterpret with caution owing to small sample size.
Factors associated with reporting an STI in the past 12 months
Factors associated with self-reported STI among males and females aged ≥13 years enrolled in the 2022 LBBS, Siaya County, Kenya.
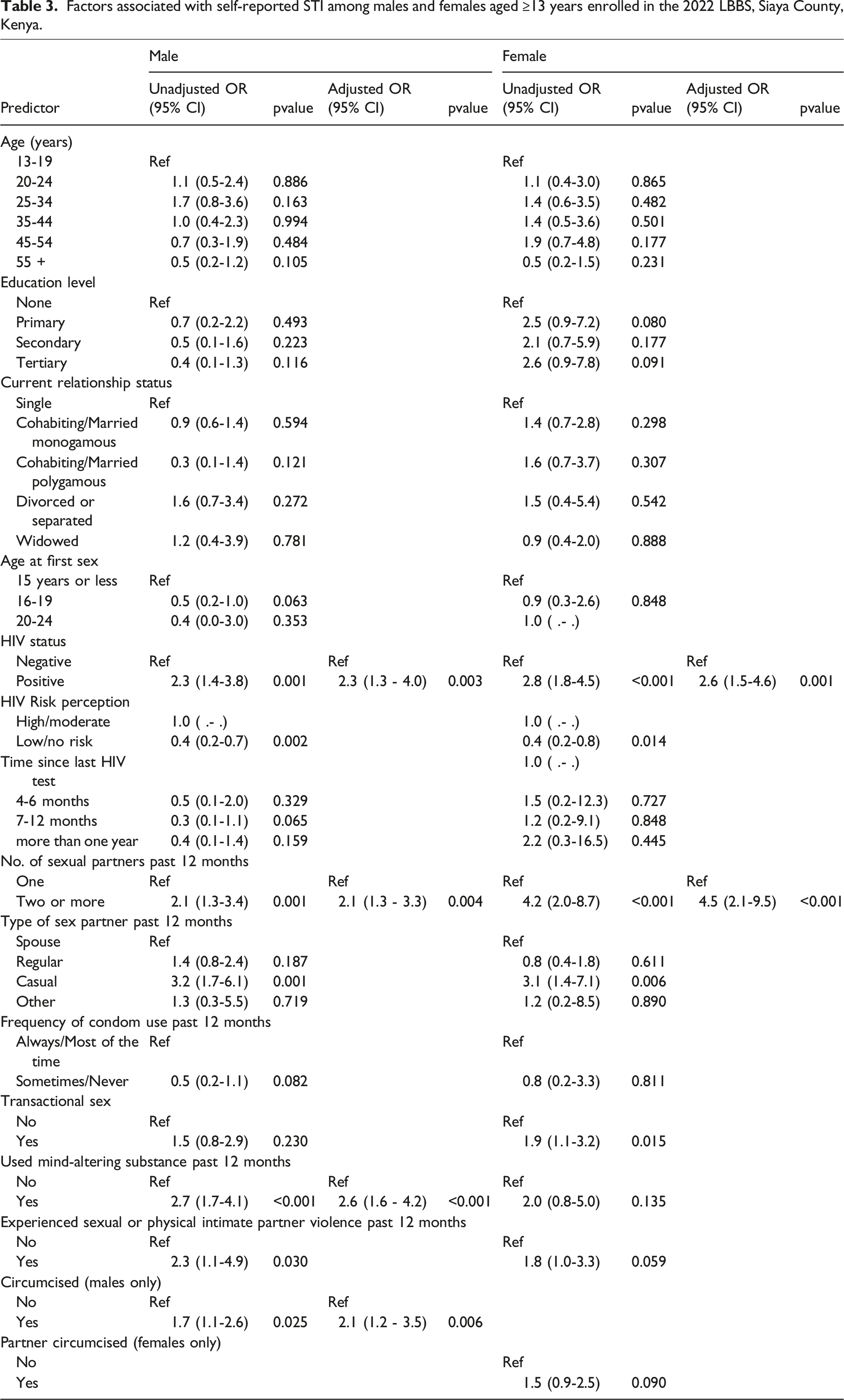
In the multivariable analysis, HIV-positive status (aOR 2.3; 95% CI 1.3–4.0), multiple sexual partners (aOR 2.1; 95% CI 1.3–3.3), having used mind-altering substances (aOR 2.6; 95% CI 1.6–4.2), and being circumcised (aOR 2.1; 95% CI 1.2–3.5) were all independently associated with self-reported STI among males. Among females, HIV-positive status (aOR 2.6; 95% CI 1.5–4.6) and multiple sexual partners (aOR 4.5; 95% CI 2.1-9.5) were independently associated with self-reported STI.
Discussion
To our knowledge, this is the first study to generate estimates of self-reported STI by sex, age, and HIV status among the general population in western Kenya, a setting with a generalized HIV epidemic, and a region with high HIV prevalence. We also identified risk factors independently associated with self-reported STI, which for both sexes included HIV infection and having multiple sexual partners; and among males, included the use of mind-altering substances, and being circumcised. Our findings are consistent with groups considered to be vulnerable to STIs by WHO 4 and with studies conducted in western Kenya focusing on STIs in adolescents 26 young men 15 and women 25 and fishermen. 24
Self-reported prevalence of recent STI in the study population (1.8%) was 2-fold higher than earlier national estimates (0.9%) 20 and similar to estimates among persons aged 15–49 years in the former Nyanza region, which includes Siaya County. 33 Our findings are also consistent with more recent national estimates of self-reported STI diagnosed by a healthcare provider in the past 12 months among HIV-positive males (3.5%) and females (3.1%) and HIV-negative males (1.5%) and females (2.5%). 29 Overall, 19.3% of females and 14.3% of males in the study population were living with HIV, which is significantly higher than the national estimate (4.9%) and similar to the estimate for Siaya County (15.3%) observed in the most recent national HIV survey. 29 Furthermore, self-reported STI prevalence was higher among persons living with HIV across all age categories, consistent with national surveys 20 and other studies.7,17,18,21,22 HIV was independently associated with STI in the multivariable model for both sexes. This may result from more frequent access to healthcare for routine HIV services, which include STI screening, and awareness of STIs among the HIV-positive population, and ongoing behavioral risks for sexually acquired infections, including unprotected sex.34–37 ARVs substantially reduce HIV transmission;38–42 however, with over 20% of people living with HIV on ART in Siaya having viral load non-suppression (>1000 virus copies/mL of blood), 29 the high prevalence of unprotected sex and other behavioral risks in this population point to continued risk of HIV transmission, and acquisition/transmission of other STIs.
The relatively high prevalence of self-reported STIs among HIV-negative men 20–34 years (2.8%–3.9%) is concerning as an indicator of unprotected sex and a risk factor for HIV acquisition. We did not evaluate care-seeking behaviors for STIs; however, in a national survey, an estimated 25% of women and 14% of men who reported having an STI in the past 12 months did not seek treatment from a healthcare provider. 33 This underscores the potential for persistent STIs and associated adverse health outcomes, including HIV infection, and further transmission of STIs to sexual partners. Collectively, these findings highlight the importance of routine HIV testing among clients accessing STI clinics, and routine STI screening and treatment among people living with HIV at each clinic encounter per Kenya MOH guidelines.43,44 Findings also point to the value of targeted prevention counseling for STIs and HIV in key populations, including counseling on HIV PrEP and voluntary medical male circumcision (VMMC). 4
In our study, 22% of males and 4.2% of females had multiple sexual partners in the past 12 months. Consistent with the literature from Kenya,14,20,37 other countries in SSA, 13 and other regions, 45 having multiple sexual partnerships was also associated with STI. In Kenya, a national survey found that STI prevalence in people with multiple sexual partners was higher than among those reporting zero or one sexual partner. 20 Another study conducted in Kisumu, an urban center adjacent to Siaya County, found that among young, sexually active men, having multiple sexual partners was associated with sexual partner concurrency and a high number of lifetime sexual partners, 14 all of which may further compound the risk of STI (including HIV) transmission and acquisition. Aggressive scale-up of PrEP is a key priority for Kenya’s National HIV Program. Kenya’s national PrEP implementation framework targets key populations, including persons with multiple sexual partners.43,46–48 Our study identifies a large proportion of the population who meet this criterion, and may benefit from PrEP for HIV prevention.
Use of mind-altering substances in the past 12 months was highly prevalent in the male population (22.4%) and independently associated with self-reported STI among males. The use of alcohol, and other mind-altering substances before or during sex, has been associated with various adverse health outcomes, including the acquisition of HIV and other STIs.45,49 Therefore, when appropriate, WHO recommends programs focused on alcohol and drug use be incorporated into comprehensive services for STI prevention among men as these factors can impair judgment and exacerbate sexual behaviors associated with STIs and HIV. 4 Kenya’s ART and STI/HIV prevention guidelines recommend screening all adult and adolescent HIV-positive persons for alcohol and drug use at the initial visit, and regularly during follow-up visits. Our findings point to the importance of implementing these guidelines effectively. Additionally, strengthening both facility and community-based outreach, counseling and treatment services for alcohol and drug use in western Kenya could be a critical component of comprehensive STI/HIV prevention programs in this region.
The odds of STI were 2-fold higher among circumcised vs. uncircumcised males, and over 50% of male participants were circumcised. The study area includes traditionally non-circumcising communities, 50 which since 2008, have been targeted by Kenya’s National HIV Program for aggressive programmatic scale-up of VMMC to reduce HIV transmission risk among heterosexual men.51–53 The protective effects of male circumcision may be partially offset by increased sexual risk behaviour as a result of lower perception of HIV infection risk after circumcision. 54 The literature on risk compensation is mixed, with earlier studies finding evidence of sexual risk compensation after male circumcision55–58 and more recent studies finding contrary59–61,61–65 or inconclusive56,66,67 evidence. Our findings suggest that ongoing risk of both HIV and other STIs among HIV-negative men in western Kenya may be compounded by behavioral risk compensation after circumcision. These findings further underscore the importance of intensive sexual health counselling, including eligibility screening for PrEP for HIV, as a key component of VMMC programmes in the region.
Limitations
The outcome of having STI was based on self-report, which may be subject to recall and social desirability biases. Additionally, the survey focused on STIs confirmed by a healthcare provider and did not ask about specific signs/symptoms of STIs. These factors may have resulted in an underestimation of the burden of STIs. 33 We, nevertheless, documented a high self-reported STI prevalence in the population. Finally, our study took place in a primarily rural region of Siaya County and may not be fully generalizable to other parts of Kenya. However, consistency between the HIV and STI prevalence estimates presented, and the published literature on western Kenya20,29,33 suggest this analysis may reflect the broader western Kenya region.
Conclusions
Our study provides granular-level data on self-reported STI prevalence by age, sex, and HIV status in the general population of Siaya County, an area with a generalized HIV epidemic in western Kenya. STI burden was exceptionally high among men and women living with HIV, and HIV-negative men of all ages. We found that several highly prevalent (>10%) risk factors were independently associated with STIs in this population, including, among both sexes, HIV infection, multiple sex partners, and among men, circumcision and use of mind-altering substances. These findings are relevant for both STI and HIV prevention and control in this region. Our study underscores the importance of evaluating the degree to which relevant Kenya MOH guidelines are being fully implemented in this area, including STI screening in HIV clinics, and HIV testing and counseling in STI clinics; and substance use and PrEP eligibility screening and counseling. Findings also highlight the importance of intensive sexual health and PrEP counselling in VMMC programmes in the region.
Supplemental Material
Supplemental Material - Prevalence and risk factors of sexually transmitted infections in the setting of a generalized HIV epidemic—a population-based study, western Kenya
Supplemental Material for Prevalence and risk factors of sexually transmitted infections in the setting of a generalized HIV epidemic—a population-based study, western Kenya by Hellen C Awuoche, Rachael H Joseph, Faith Magut, Sammy Khagayi, Fredrick S Odongo, Moses Otieno, Aoko Appolonia, Elijah Odoyo-June, and Daniel O Kwaro in International Journal of STD & AIDS
Footnotes
Acknowledgements
We acknowledge, with great appreciation, the study participants for their time and invaluable contributions to the existing knowledge base on HIV and the HIV epidemic in Kenya. We are grateful to the KEMRI study team for their dedication and contributions to this important work. Finally, we would like to thank the Director of the KEMRI Centre for Global Health Research for permission to publish the manuscript.
Authors contribution
HCA conceptualized and designed the study, analyzed, and interpreted the data and drafted the original manuscript. RHJ designed the study, edited, and rewrote the discussion and was a major contributor in writing the entire manuscript. FM analyzed and interpreted the data. SK analyzed and interpreted the data and reviewed the subsequent manuscript drafts. MO prepared data for analysis. FSO, EOJ and AA reviewed and edited the subsequent manuscript drafts. DOK conceived, designed, and implemented the study. The final version of the manuscript was read and approved by all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication has been supported by the President's Emergency Plan for AIDS Relief (PEPFAR) through the US Centers for Disease Control and Prevention (CDC) under the terms of GH001995.
Disclaimer
The findings and conclusions in this report are those of the author(s) and do not necessarily represent the official position of the funding agencies.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.