
Abstract
Background
Pre-exposure prophylaxis (PrEP) may favor sexual satisfaction by reducing the fear of HIV and promoting less restrictive sexual practices. These benefits may be even higher among PrEP users with mental health issues.
Methods
We invited adult PrEP users to answer a questionnaire including demographics, questions on the sexual experience compared to the period before PrEP use, and the Hospital Anxiety and Depression Scale. Factors associated with improvements in the sexual experience were investigated using modified Poisson models.
Results
We included 221 participants; most were white males. A large percentage of participants reported improvements in quality of sex after PrEP initiation; the composite outcome “PrEP-associated improvement in the quality of sex” was observed in 92 (42%), whereas the outcome “PrEP-associated improvement in the fear of HIV acquisition” was observed in 120 participants (54%). Demographics and depression/anxiety were not significantly associated with the outcomes.
Conclusion
PrEP has positive effects beyond HIV prevention, improving several aspects of sexual quality of life. These benefits are valid incentives for PrEP use and prescription.
Introduction
Human immunodeficiency virus (HIV) incidence is still unacceptably high, despite a slow reduction in the frequency of estimated yearly new infections in the past decades. The most recent UNAIDS report estimated that approximately 1,500,000 new HIV infections occurred worldwide in 2021, 1 notwithstanding the existence of effective prevention methods. The occurrence of incident cases is particularly concerning among key populations including men who have sex with men, sex workers, transgender persons, and people who use drugs in most countries outside Sub-Saharan Africa, whereas several Sub-Saharan African countries present a more generalized pattern of HIV prevalence and incidence. 1
Studies demonstrate that prevention methods that rely on the use of antiretrovirals are underused in most settings. 2 HIV pre-exposure prophylaxis (PrEP) rollout has been slow, even in settings with broad implementation of PrEP in healthcare units. 3 For instance, the Ministry of Health of Brazil has implemented free-of-charge PrEP in the public healthcare system since early 2018, 4 yet by March 2022 only 33,000 people were accessing PrEP in the country. 5
Although PrEP is currently more broadly known and available, 6 a few barriers still discourage PrEP prescription. For instance, studies have shown that risk compensation, defined as the increase in sexual risk practices following a reduction in the perceived risk of HIV acquisition among PrEP users, is a commonly cited concern among healthcare providers, and could be a barrier to PrEP prescription. 7 Risk compensation could potentially result in a higher incidence of other sexually transmitted infections (STI), 8 although some studies also suggest that PrEP users may actually enhance prevention attitudes after PrEP initiation, influenced by the routine of testing, counseling and engagement in self-care.9–11 In addition, PrEP users undergoing frequent STI testing and early treatment may in fact have a lower risk of progression and transmission of bacterial STI. 12
From a different point of view, risk compensation may also reflect that PrEP users become less restrictive regarding their sexual practices, favoring sexual satisfaction. 13 Indeed, several studies demonstrate that the fear of acquiring HIV may hinder a more fulfilling sexual experience, particularly among key populations. 14 Scarce studies exploring potential benefits of PrEP use for the sexual quality of life suggest a positive effect associated with a reduced fear of HIV infection. 15 It is plausible to assume that these benefits could be even higher among PrEP users facing mental health issues such as anxiety and depression – particularly when such issues result from stigma associated with sexual practices - compared to PrEP users with no mental health conditions. Characterizing the effects of PrEP on sexual quality of life, in addition to its HIV preventive effects, could decrease the skepticism surronding PrEP use and increase PrEP uptake. 16 In this study, we invited Brazilian PrEP users to participate in a survey-based investigation of the effects of PrEP use on quality of sex and fear of HIV acquisition. We explored if demographics, depression, and anxiety were associated with improvements in the quality of sex and fear of HIV acquisition following PrEP initiation using univariable and multivariable models.
Methods
In this cross-sectional study, we included PrEP users aged 18 years old and older under follow-up at the HIV and PrEP outpatient clinic, Hospital das Clinicas, in Sao Paulo, Brazil. Participants answered a self-completion questionnaire including demographics, questions on the sexual experience following PrEP initiation using a modified version of the Arizona Sexual Experience Scale (ASEX), 17 and the Hospital Anxiety and Depression Scale (HADS). 18 Depression and anxiety were defined as present when scores in the HADS scale were ≥ 9 points.
We modified questions from the original ASEX to address perceptions after PrEP initiation for each of the 5 components of the scale and for time spent to reach an orgasm compared to the period before PrEP use, as follows: (1) Compared to the period before PrEP use, how strong is your sex drive? (2) Compared to the period before PrEP use, how easily do you get sexually aroused? (3) Compared to the period before PrEP use, how easily do you get and keep an erection? (4) Compared to the period before PrEP use, how easily can you reach an orgasm? (5) Compared to the period before PrEP use, how satisfied do you feel with your orgasms? (6) Compared to the period before PrEP use, how do you perceive the time spent to reach an orgasm?
In addition, we included questions on the reported frequency of thinking about HIV during or after a sexual intercourse; anxiety and concerns regarding HIV acquisition; and how often the risk of HIV acquisition impairs the quality of sexual relationships compared to the period before PrEP use. Responses concerning sexual experience were collected using close-ended, single choice ordinal answers.
We defined two composite outcomes for the study. The outcome “PrEP-associated improvement in the quality of sex” was defined as present for all participants with improvements in at least one of the questions concerning sex drive, arousal, capacity to get and keep an erection, to reach orgasm, and the level of satisfaction with the orgasm. The second composite outcome was named as “PrEP-associated improvement in the fear of HIV acquisition”. This outcome was considered present for participants reporting improvements in all three questions concerning subjective aspects of the influence of fearing HIV on the quality of sex (thinking of HIV during or after the sexual intercourse; concerns/anxiety regarding the risk of acquiring HIV sexually; and the risk of HIV infection hampering the quality of sex).
Questionnaire responses were collected either in-person by a study investigator or remotely using self-completion electronic forms.
Participants’ demographics and answers to the study questionnaire were presented using frequencies and percentages. Factors associated with improvements in the sexual experience following PrEP initiation were investigated using modified univariable and multivariable Poisson models to estimate prevalence ratios, with a significance level of 0.05. The multivariable models included age categories, race/ethnicity, marital status, religion, income, and the presence of anxiety or depression. Variables included in the multivariable model were defined according to a theoretical rationale for causal inference using acyclic diagrams. We also fit multivariable models including the sociodemographic variables and excluding depression/anxiety as sensitivity analyses. We used Stata 15.1 (StataCorp College Station, TX: StataCorp LP) for all analyses.
The institutional ethics review board revised and approved the study. All participants provided written informed consent prior to inclusion. We kept all participants’ identifiable information confidential throughout the study.
Results
Sociodemographic characteristics of study participants.
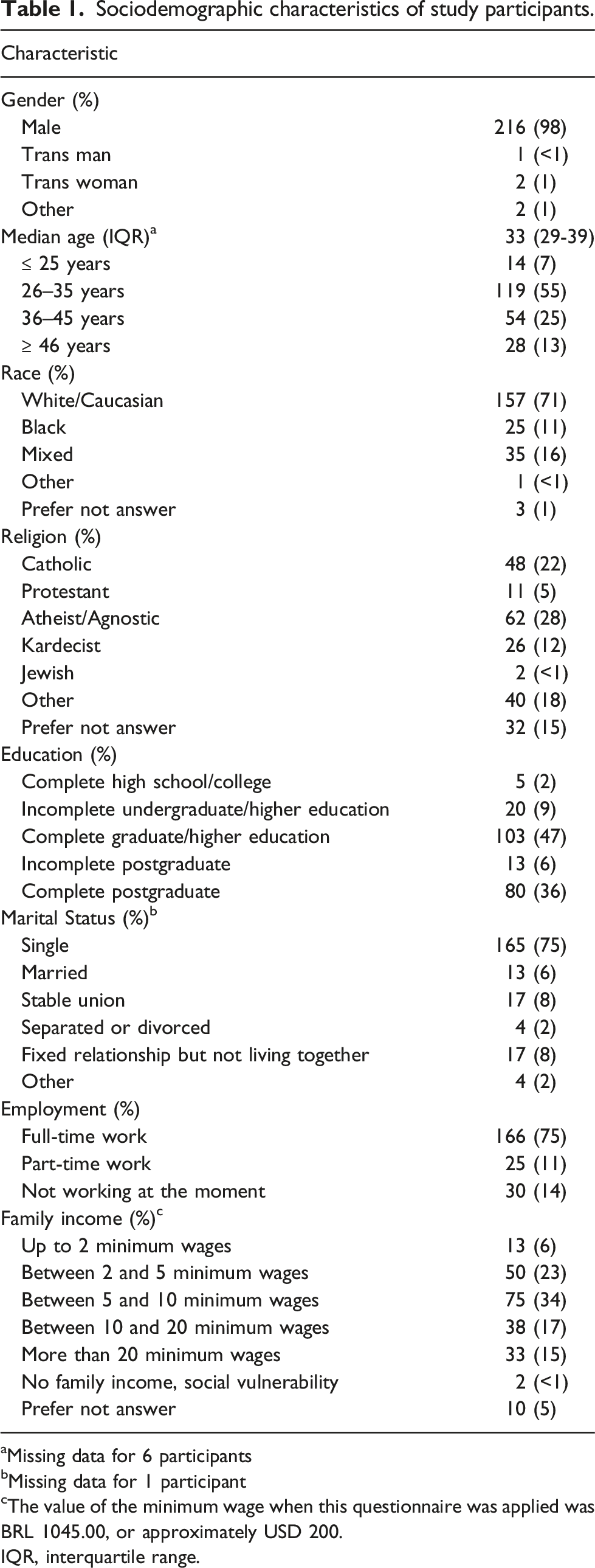
aMissing data for 6 participants
bMissing data for 1 participant
cThe value of the minimum wage when this questionnaire was applied was BRL 1045.00, or approximately USD 200.
IQR, interquartile range.
Questionnaire responses concerning the sexual experience and the effect of PrEP use on the quality of sex life and sexual satisfaction.
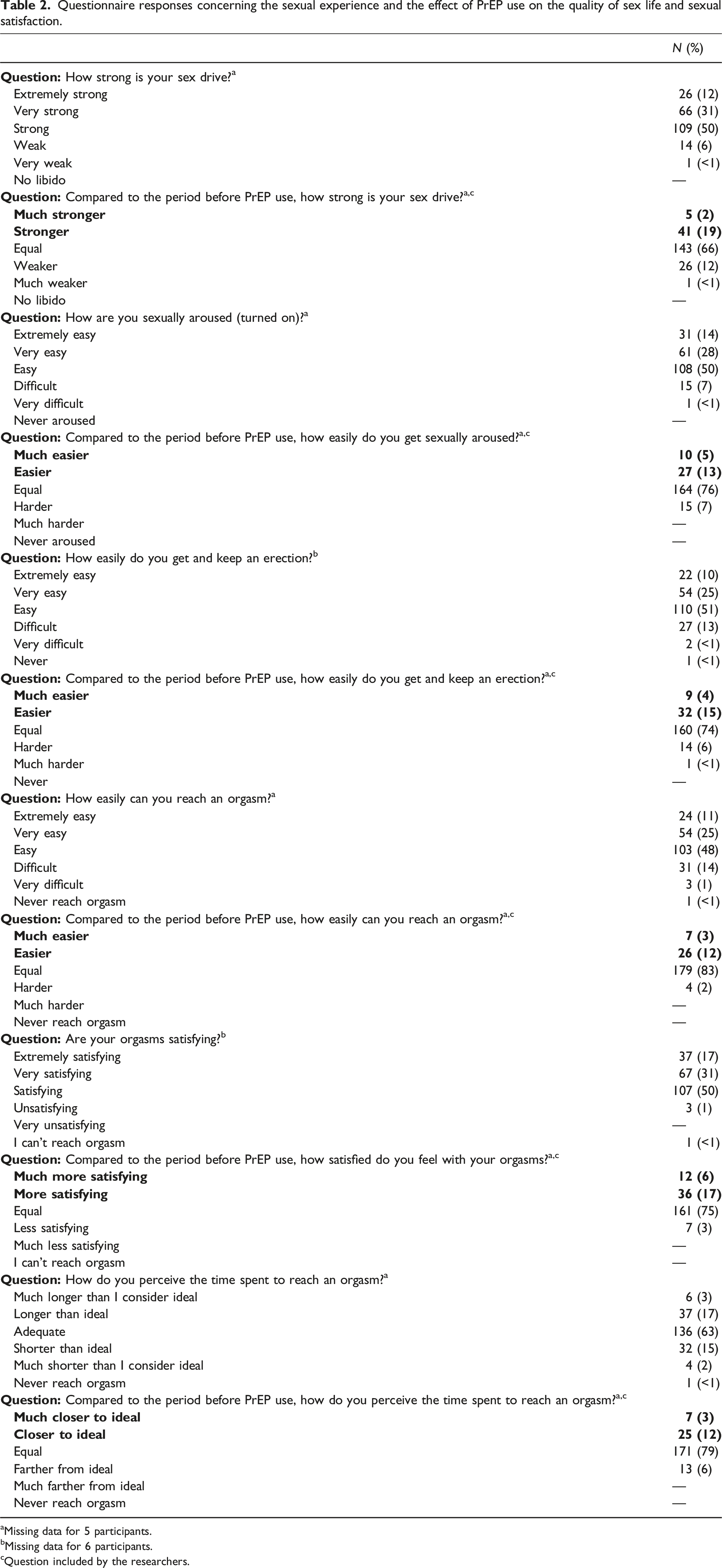
aMissing data for 5 participants.
bMissing data for 6 participants.
cQuestion included by the researchers.
Questionnaire responses concerning the effect of PrEP on fear of HIV and the quality of sexual relationships.
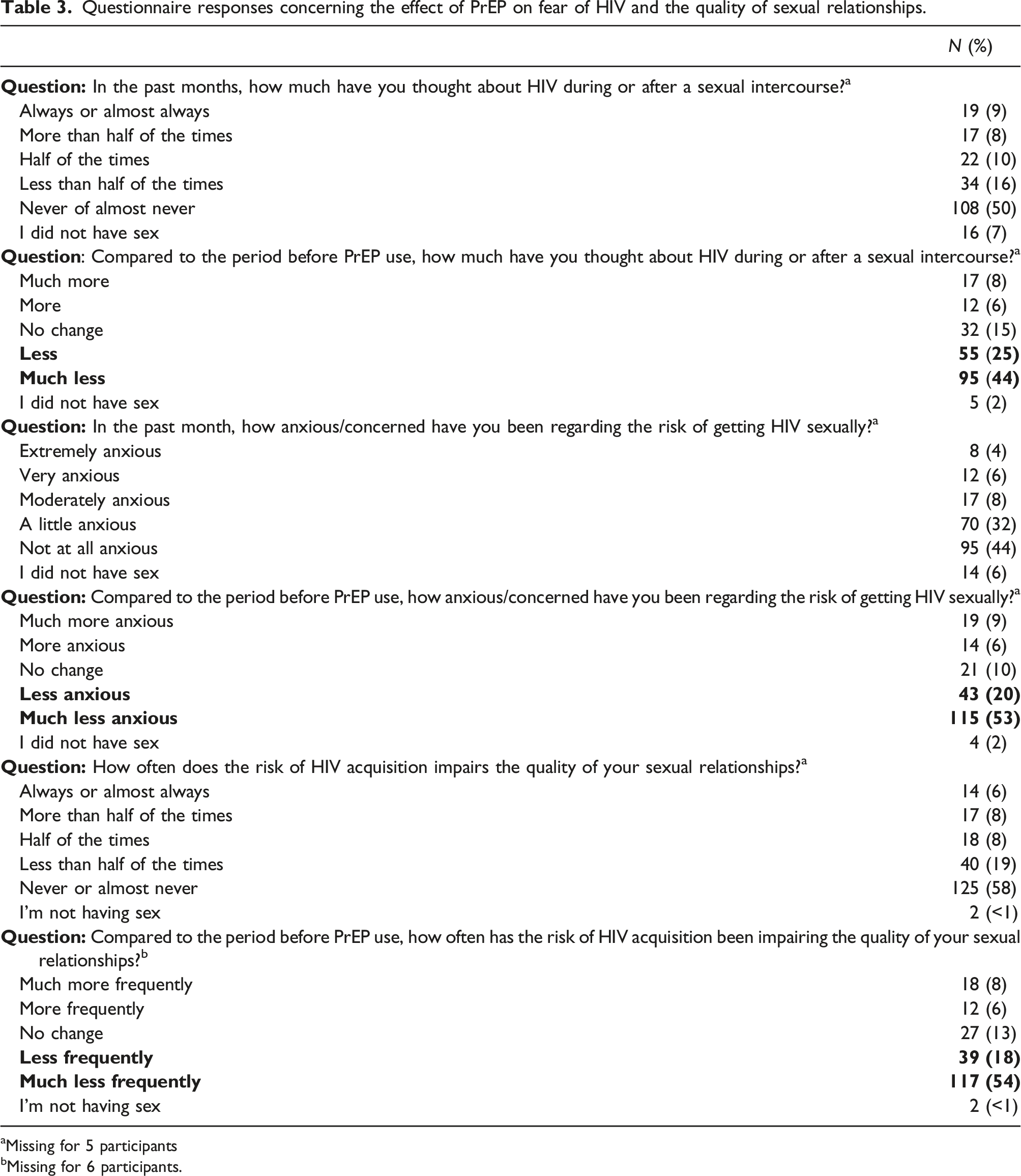
aMissing for 5 participants
bMissing for 6 participants.
Univariable and multivariable analyses of factors associated with “PrEP-associated improvement in the fear of HIV acquisition.”
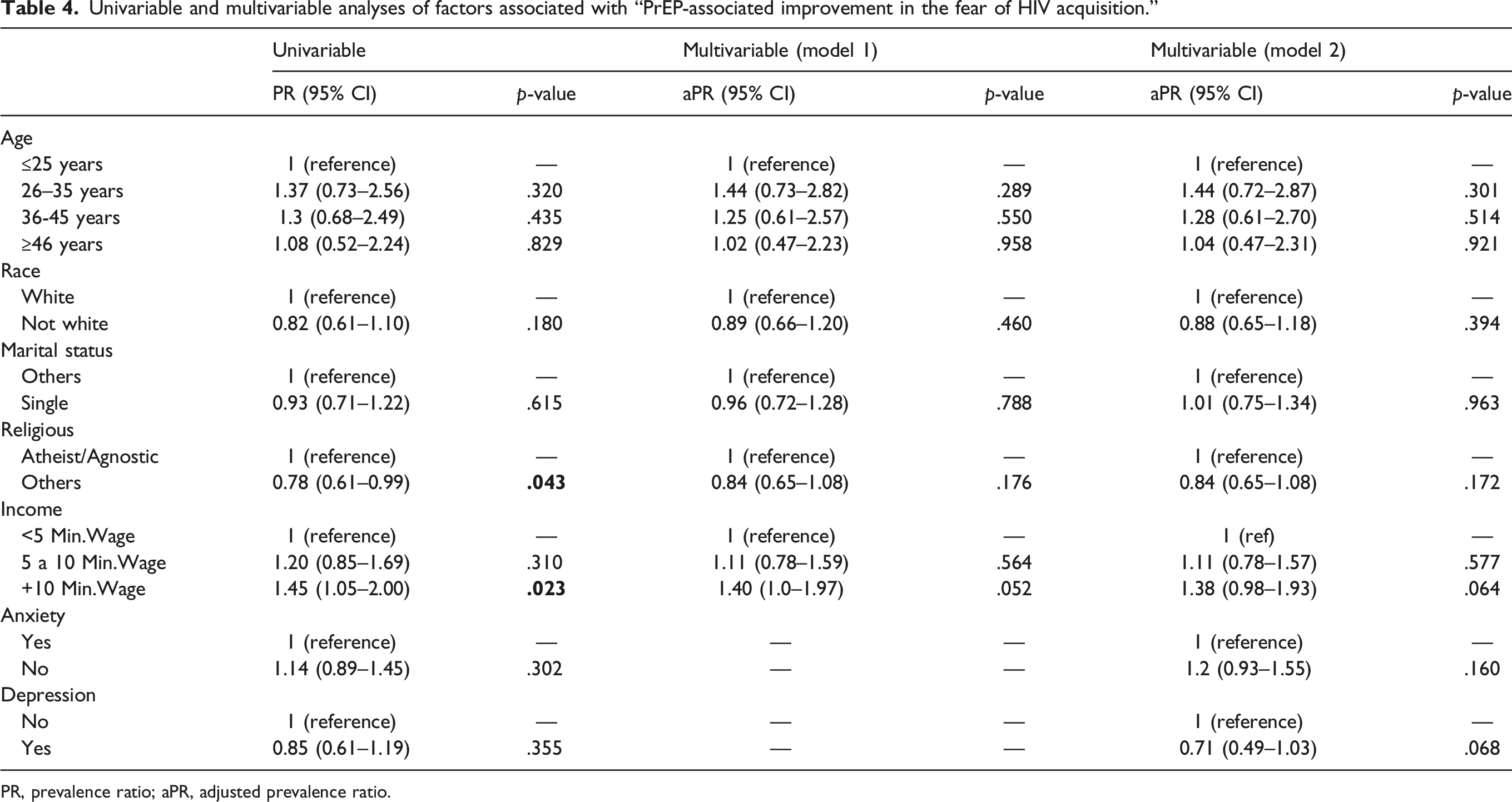
PR, prevalence ratio; aPR, adjusted prevalence ratio.
Univariable and multivariable analyses of factors associated with “PrEP-associated improvement in the quality of sex”.
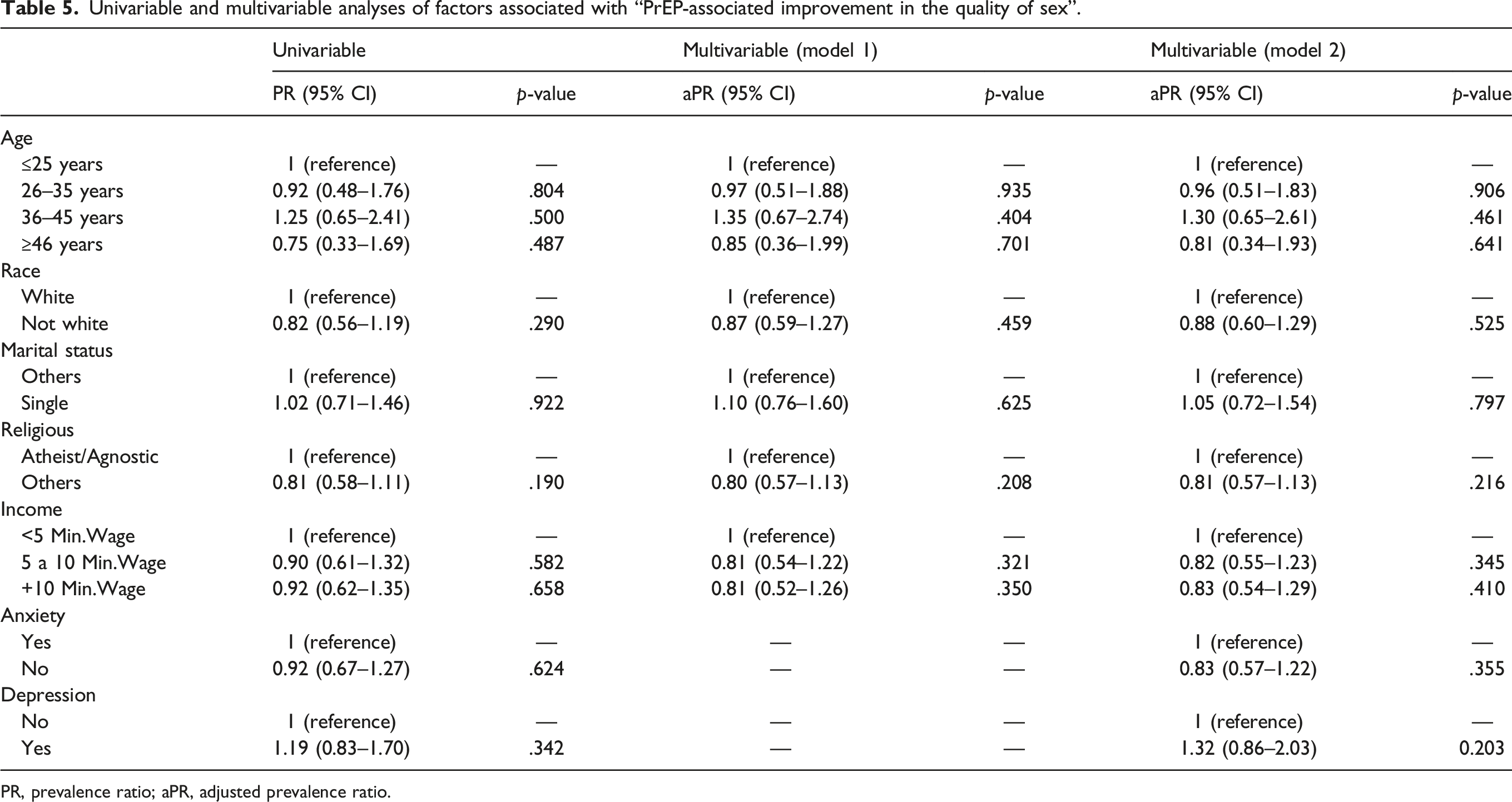
PR, prevalence ratio; aPR, adjusted prevalence ratio.
Discussion
In this cross-sectional study, most of the 221 study participants were white cisgender males with high educational attainment, reflecting the demographic profile of PrEP users in Brazil. 5 We addressed the effect of PrEP on subjective aspects associated with the fear of HIV acquisition using a composite outcome named “PrEP-associated improvement in the fear of HIV acquisition” and assessed the effect of PrEP on more objective aspects associated with the sexual experience using a composite outcome named “PrEP-associated improvement in the quality of sex”. Most participants reported improvements in individual questions related to the fear of HIV acquisition, and 54% reported improvement in all three items. Regarding the specific aspects of sex drive, arousal, erection, and orgasm, although a lower number of participants reported improvements in individual aspects following PrEP use, 42% had improvements in at least one aspect. Taken together, our findings suggest that PrEP has potential benefits to the sexual experience of users, including subjective aspects related to a relief from the fear of HIV, and more objective aspects of the sexual intercourse.
A few previous studies explored the possible benefits of PrEP for the sexual quality of life and other social and mental health aspects. In a study addressing PrEP adoption intentions, the desire for intimacy in condomless sex was an independent predictor of PrEP adoption intentions. 19 Indeed, condoms are seen as physical and symbolical barriers often associated with lesser intimacy, 15 and are less likely to be used when closeness and affection are prioritized. 20
As seen in our results, other studies showed that PrEP is associated with lower levels of anxiety about HIV transmission 21 and improvements in sexual pleasure and quality of sex life. 15 A recent longitudinal study conducted in the Netherlands showed positive effects of PrEP on the quality of sex life related to reduced fear of HIV; moreover, this study suggested increased interest in experimenting with sex in the first months of PrEP use. 22 The positive impact of PrEP on sexual satisfaction, pleasure, intimacy, and sexual anxiety and fears has been highlighted in a systematic review including 16 studies conducted in 7 countries. 23 Finally, studies also suggest that PrEP may contribute to empowerment, giving people autonomy about their decisions regarding sexual practice and risk management. 15 Nevertheless, these benefits may be hindered by moral constraints that stigmatize pleasure, particularly in sexually diverse communities already facing judgment and discrimination. Such moral constraints are sometimes disguised as concerns with risk compensation, 13 ultimately leading to missed opportunities of prevention. 7
Our study had several limitations. We included current PrEP users using a cross-sectional approach, and therefore could not address the experience of former PrEP users; in addition, we asked participants to report on sexual perceptions compared to the period before PrEP use, which could be subject to recall bias. We selected participants from a single public health facility, limiting generalizability of our findings. We also used different strategies to collect questionnaire responses, which could produce differences in results that were not controlled for in this analysis. The questionnaire included adapted instruments with no prior validation assessment, and the main study outcomes were defined using composite responses, not necessarily inferring the intended phenomena. Importantly, the question concerning erection from the ASEX instrument was not applicable for our study participant who was a transgender man; instruments to assess sexual function and quality of sex life in non-cisgender populations are lacking. Finally, another limitation was the implementation of the study questionnaire during the COVID-19 pandemic, which likely had a negative impact on the sexual experience of study participants and could have contributed to an underestimation of the benefits of PrEP for the sexual quality of life.
Despite these limitations, we included a sample of participants that reflects the demographic profile of PrEP users in Brazil and other countries, and our results reinforce the data from existing literature showing that PrEP has positive effects beyond HIV prevention, improving several aspects of the sexual quality of life. Our findings suggest that the potential impact of PrEP on sexual quality of life should be emphasized as a significant incentive for PrEP prescription among healthcare providers, and meaningful encouragement for PrEP adoption among potential users.
Footnotes
Acknowledgements
We thank Maria Amelia Veras, Aluisio Segurado and Ines Dourado for their useful suggestions in study design and data interpretation.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RV received support from Gilead Sciences, Janssen, and GSK ViiV to participate in medical conferences and advisory boards. VIAS received support from Gilead Sciences for registration in a medical conference.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.