
Abstract
Introduction
Mental health problems are the leading causes of disability and contribute to the global disease burden. 1 The most common mental health problems include depression, anxiety, and post-traumatic stress disorder. 1 Despite contributing significantly to the global disease burden, mental illness receives little attention, especially in low-and middle-income countries (LMIC), where more than 80% of people have mental health disorders. 2 Depression, the most common mental health problem, is ranked the leading cause of global disability and contributor to the overall global burden of disease. 1 However, in sub-Saharan Africa (SSA), depression often is undiagnosed and underreported. 3 Poor mental health outcomes in people living with HIV (PLHIV), have been linked to poor engagement in care, non-adherence to antiretroviral therapy (ART), and other risk behaviors, leading to poorer physical outcomes and a higher risk of HIV transmission.4–6 Thus, it is crucial to understand the determinants of mental health problems such as depression specifically in PLHIV.
Mental health problems arise from complex intersecting social determinants of health, including food insecurity. Food insecurity is a social determinant of health that occurs when a person lacks consistent access to enough food for a healthy life. 7 Food insecurity disproportionately impacts PLHIV and is associated with poor health outcomes in this group.7,8 A recent systematic review and meta-analysis demonstrated that food insecurity is significantly linked to an increased risk of depression in PLHIV. 9 In SSA, food insecurity has also been linked to depressive symptoms among PLHIV, including in pregnant women.8,10,11 For example, a study conducted in Kenya showed an association between food insecurity and depressive symptoms in perinatal women. 8 These studies show a high prevalence of food insecurity in this region, with more than 50% of the population experiencing severe food insecurity.7,12 Severe food insecurity among people living with HIV may lead to missed clinic appointments, non-adherence to HIV medication, and HIV treatment interruptions, which are strong determinants of worse HIV health outcomes. 9 Food insecurity has also been shown to impact HIV treatment outcomes through biological mechanisms. For example, in a study that was conducted in people living with HIV who also use drugs, severe food insecurity was associated with HIV wasting, which is linked to poor virological responses. 13
In sub-Saharan Africa, limited studies have examined the association of severe food insecurity and depressive symptoms among young people living with HIV (YPLH). Given the role of depression and HIV treatment, it is important to investigate the risk factors for depressive symptoms among PLHIV. Therefore, this paper assessed the association between severe food insecurity and depressive symptoms among YPLH.
Methods
Study design and sample
We analyzed cross-sectional (baseline) data collected from YPLH who participated in a feasibility study of an asset-based intervention to improve antiretroviral treatment adherence. Eligibility criteria included: age between 18 and 21 years old, male or female, awareness of HIV positive status, and receiving outpatient HIV treatment and care at either one of two hospitals (see research setting below). Participants were eligible if they could provide written informed consent (refer to the ethical consideration section below), and the age group was also based on the HIV prevalence in the region. Youths aged between 15 and 24 had high positivity rates compared to the national numbers. The two hospitals were selected due to their comparability based on accessibility for participants, access to antiretroviral therapy (ART), and availability of support services for youth living with HIV and their families. The ART enrollment list was used to select and recruit 60 participants per hospital. Project staff met with prospective participants at the participating hospitals to explain the study and to discuss and obtain consent. Each prospective participant was asked if they would like to consider further participating in the study to minimize coercion. In such cases, project staff sought oral consent to contact the youth no sooner than 3 days after the first consent discussion.
Discussions with prospective participants and informed consent procedures were conducted in private. Informed consent was obtained from all study participants. Study materials, including the participant information sheet and consent form, were in English, Tumbuka and Chewa. The project staff was also fluent in Tumbuka to accommodate participants who preferred to speak in Tumbuka.
Setting
The study was conducted in Chipata and Lundazi districts in Eastern Province. Eastern Province is predominantly rural, with 87% of the population living in rural areas Chipata and Lundazi districts were selected as they were within the service area of the Rising Fountains Development Program, the project’s community-based organization partner with offices in Chipata and Lundazi. Chipata District, the provincial capital, had an estimated population of 566,157 in 2020. 14 Lundazi District, adjacent to Chipata District, had an estimated population of 442,300 in 2020. 14 An equal proportion of each district’s population was male and female. Additionally, an estimated 20% of each district’s population was young people aged 15 to 24 years old.
Two health facilities were selected as study sites – Chipata Central Hospital (CCH) and Lundazi District Hospital (LDH). CCH is a third-level or specialty hospital. It serves the entire Eastern Province, with a catchment population of 1.96 million people, including 455,000 residents of Chipata District. CCH offers the most comprehensive medical services in the Eastern Province. LDH is a first-level hospital serving Lundazi District, with an estimated population of 324.000. Both hospitals are government-run and offer HIV counseling and testing, prevention of vertical transmission, and HIV treatment and care. CCH and LDH are 180 km apart.
Consistent with the national trend, HIV prevalence in Eastern Province was higher for females than males among youth aged 15–19 and 20–24. In 2019, HIV positivity rates for females aged 15–19 and 20–24 were 1.7 and 3.2%, respectively. Males from the same age groups had HIV positivity rates of 0.8 and 1.9%. HIV positivity rates among youth in Eastern Province remained lower than the national averages. 14 An estimated 91% of people (aged ≥15 years old) living with HIV in Eastern Province knew their status and were on antiretroviral therapy in 2019. Further, 80% were virally suppressed. The most recent available data indicated that 81,000 residents of Eastern Province were living with HIV. 15
Data collection
Data was collected between August 2018 and May 2019 using an interviewer-administered survey questionnaire. The questionnaire gathered data on participants’ demographics, household economic status, food security and dietary diversity, health behaviors and treatment adherence, social support, social and emotional skills, and experiences of stigma and discrimination. All interviewers trained to administer the survey questionnaire were community members who have worked with YPLH. All interviewers were fluent in English, Chewa, and Tumbuka.
Measures
Dependent variable: Depressive symptoms
Depressive symptoms were measured using the short form of the Children’s Depression Inventory (CDI-S). The CDI-S comprises 10 items adapted from the original 27-item CDI. 16 The CDI-S asks youth to rate the severity of different symptoms of depression. Each symptom is presented as a series of three phrases, and youth are asked to select the phrase that best represents how they feel (e.g., “I have plenty of friends”/“I have some friends but wish I had more”/“I do not have any friends”). Higher scores indicated more depressive symptomatology (α = 0.74). Research has identified the similarity of CDI-S to the original CDI concerning sensitivity and specificity to detect depression. 17 Additionally, validation studies have supported the reliability and validity of the CDI-S for use in young people with chronic health conditions.18,19 CDI-S has been used in research studies with young people between 18 and 21 years old in southern Africa.4,20
Independent variable: Food insecurity
Food insecurity was the primary exposure of interest and was measured using an adaptation of the Household Food Insecurity Access Scale. 21 This scale has previously been validated in similar settings as the current study. For example, it has been validated in Tanzania 22 and Ghana. 23 Validation studies have demonstrated that the HFIAS is able to distinguish food secure from insecure households across different cultural contexts. The questions cover three domains of experience of food insecurity: (1) anxiety and uncertainty about food supply, (2) insufficient quality (includes the variety and preferences of the type of food), and (3) insufficient food intake and its physical consequences. HFIAS consists of nine items that asks respondents the frequency of experiencing different conditions and degrees of food insecurity within the past 30 days. HFIAS guidelines ranks access to food using four categories: food secure, mildly food insecure, moderately food insecure, and severely food insecure. 21 Since we hypothesized that the effects of food insecurity on depressive symptoms would be most notable for severely food insecure persons, food security was dichotomized as severely food insecure versus all other categories.
Covariates
Characteristics that have previously been found to be associated with depressive symptoms and food insecurity were assessed as potential confounders. Covariates included gender (male/female), age (in years), currently in school (yes/no), worked in the last 30 days (yes/no), attitudes toward living at home. Attitudes toward living at home were measured using a 6-item, 4-point Likert scale (Amato, 1988). Youth were asked about their level of agreement or disagreement (strongly disagree/disagree/agree/strongly agree) with positive or negative evaluations of one’s family and home environment. Item scores were summed to create an attitudes-toward-living-at-home scale score, with higher scores indicating positive views about living at home (α = 0.79). Research has identified that these covariates affect mental health outcomes. 24 Engagement in sex for money was assessed by the item, ‘have you ever given or received sexual intercourse or sexual acts in exchange for money, food gifts or other resources?’ Response options included “yes’, ‘no’, and ‘don’t know”. To assess childhood sexual abuse, participants were asked whether they have ever had sex with someone 10 or more years older and responses were ‘yes’, ‘no’, and ‘don’t know’. Lastly, livestock ownership was as operationalized as the number of livestock owned by the household. Livestock consisted of chickens, pigs, goats, cattle, donkeys, and sheep. Livestock ownership by households is important for food security because they can be sold to smooth consumption during times of need, as such, they are a good proxy for household income levels. 25 Participants reported the number of livestock owned in the household.
Ethical considerations
Study procedures were submitted to and approved by the University of Zambia Biomedical Research Ethics Committee, the University of North Carolina at Chapel Hill Institutional Review Board, and the National Health Research Authority of Zambia. All participants provided written informed consent at enrollment
Data analysis
Descriptive statistics were conducted to characterize the sociodemographic characteristics of the study sample. In the descriptive analysis, mean and standard deviations were done for continuous variables. Proportions were used for categorical variables. In bivariate analysis, we examined the association between the independent variable (food insecurity) and potential covariates on depression. Variables that were significantly associated with the outcome at p < 0.02 and other potential confounders were included in the final multivariable linear regression model.
Before estimation, we performed multiple imputation to address missing data issues. First, missing data patterns were described. Study variables with missing values included food security (10%), depression (20%), home environment (7%), engagement in sex for money (11%), and childhood sexual abuse (13%). We explored the differences between youth with complete and incomplete data to examine the validity of the missing-at-random (MAR) assumption. Youth with complete and incomplete data did not differ significantly on all independent and dependent variables in our models. Second, diagnostic tests were conducted to compare the distributions of the observed, imputed, and completed values.26,27 The distributions obtained using midiagplots did not differ considerably, indicating that our imputation model was appropriate (Eddings & Marchenko, 2012). Third, we built an imputation model based on best practices suggested in the literature.28,29 For example, all variables in the MI model were minimally associated with the variables containing the missing values. We also created a more general imputation model than a specific analytical model to capture more associations between the variables. 30 Our imputation model comprised all variables in our analytic models, including the dependent, independent, control, and auxiliary variables, such as social and emotional skills. These auxiliary variables were not included in our analytic models but were added to the imputation model to increase statistical power and plausibility of the MAR assumption. 31 We determined auxiliary variables based on our review of the literature. Fourth, MI datasets were created by imputation using the chained equations approach (White et al., 2011). We also used regression with augmented data to avoid problems associated with perfect prediction in multiple imputations of categorical variables.29,32 Continuous variables with nonnormal distributions were imputed by predictive mean matching. 33 Last, we created our primary MI model with 100 imputed data sets to yield accurate statistical results and improve power. 34 All analyses were conducted using Stata 16.0.
Results
Sociodemographic characteristics
Overall characteristics of the study sample by severity food insecurity.
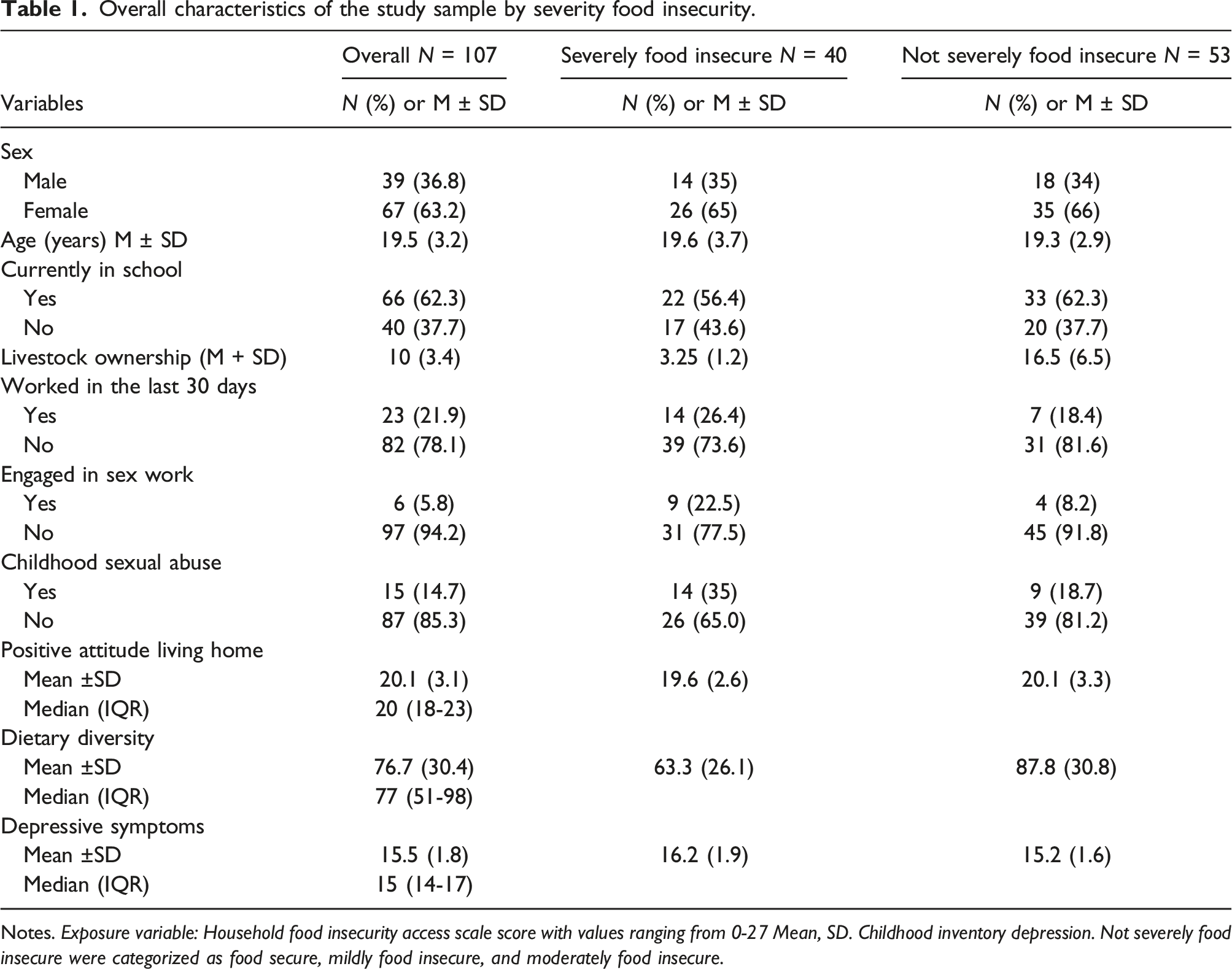
Notes. Exposure variable: Household food insecurity access scale score with values ranging from 0-27 Mean, SD. Childhood inventory depression. Not severely food insecure were categorized as food secure, mildly food insecure, and moderately food insecure.
Relationship between food insecurity and depressive symptoms
Bivariable model showing association between variables and depressive symptoms.
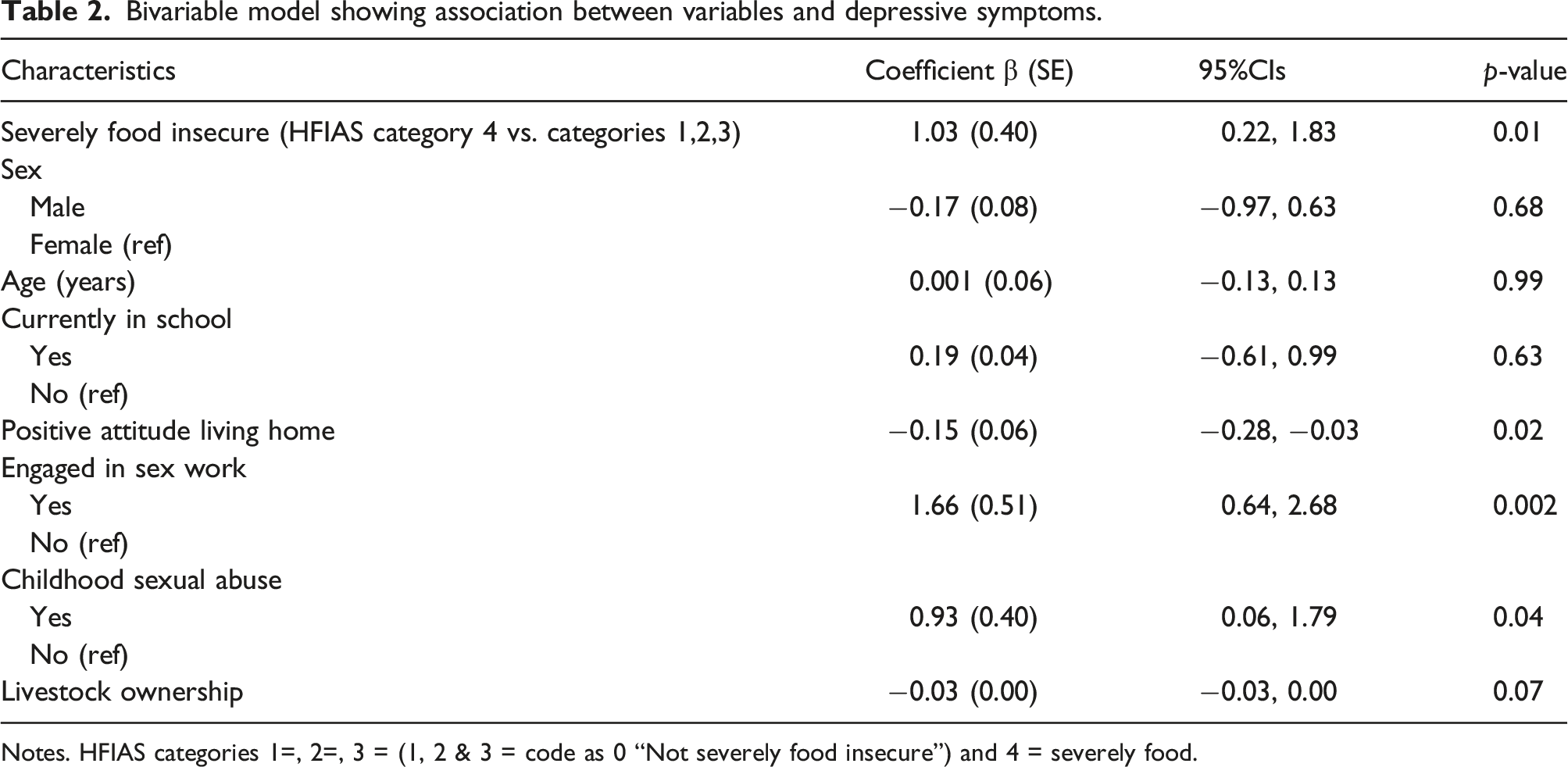
Notes. HFIAS categories 1=, 2=, 3 = (1, 2 & 3 = code as 0 “Not severely food insecure”) and 4 = severely food.
Multivariable model showing association between food insecurity and depressive symptoms adjusting for covariates.
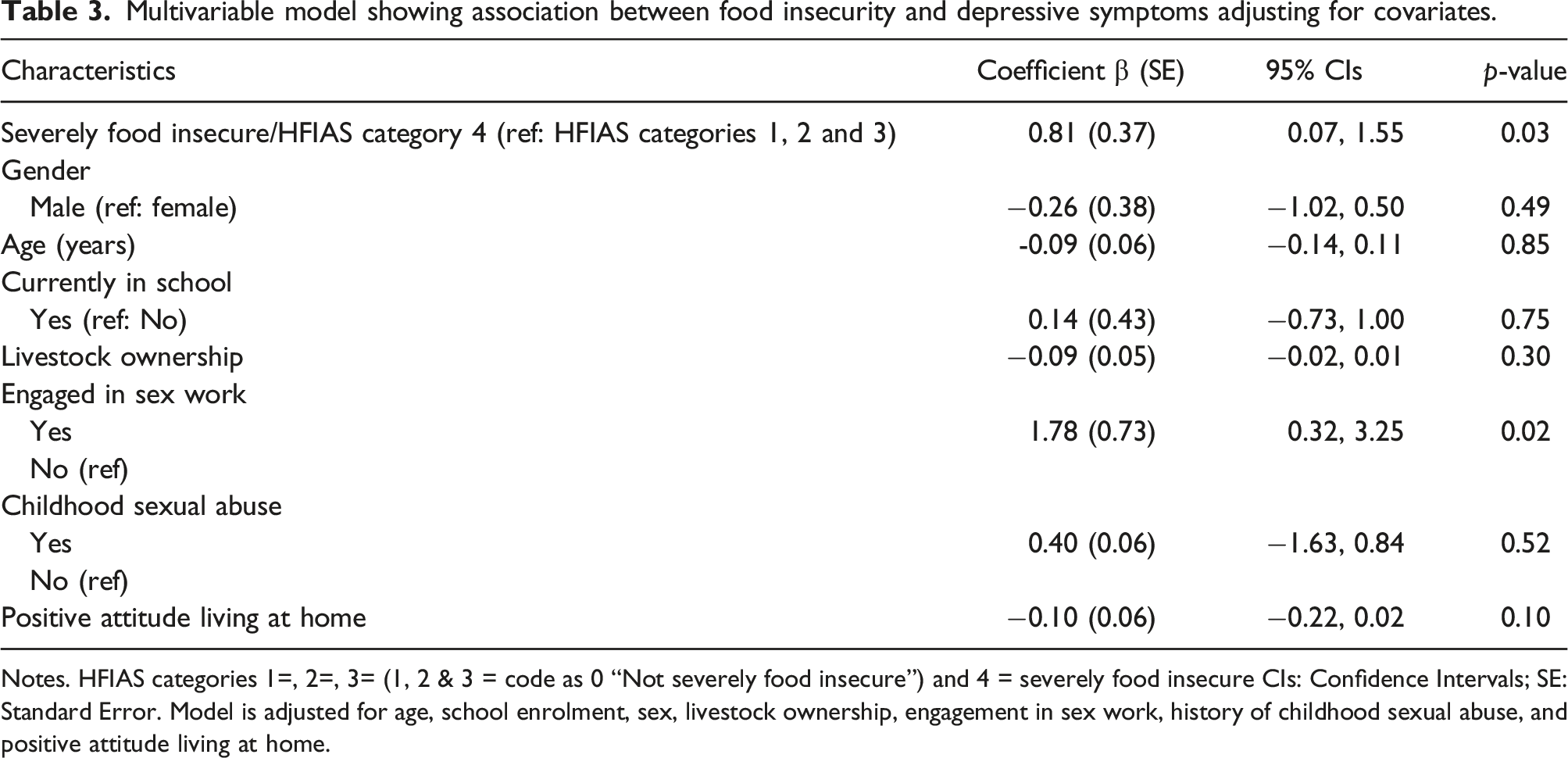
Notes. HFIAS categories 1=, 2=, 3= (1, 2 & 3 = code as 0 “Not severely food insecure”) and 4 = severely food insecure CIs: Confidence Intervals; SE: Standard Error. Model is adjusted for age, school enrolment, sex, livestock ownership, engagement in sex work, history of childhood sexual abuse, and positive attitude living at home.
Discussion
The study findings indicate that YPLH who reported severe food insecurity were more likely to have depressive symptoms. This association was independent of characteristics such as gender, age, education, and assets. These findings align with previous studies in the same study settings that found an association between food insecurity and poor mental health outcomes.10,35 For example, Tsai and team surveyed people living with HIV in Uganda and found food insecurity was associated with depressive symptom severity among women but not men. 35
Our findings add to the existing literature by showing the negative psychosocial impacts of severe food insecurity in YPLH. Other studies assessing food insecurity among PLHIV in SSA have demonstrated the relationship between food insecurity and poor mental health outcomes.8,35 However, these studies were mostly among adults living with HIV. 11 The few studies that focused on this topic were mostly conducted in Ethiopia and Uganda and also focused on adults living with HIV not YPLH.11,36,37 For example, Yeneatbat et al. (2017) found that PLWHA in Ethiopia who were food insecure were about four times more likely to have symptoms of depression than food-secure individuals. 37 Also, Kinyanda and colleagues who studied people living with HIV in Uganda found that adults who experience food insecurity were almost three times more likely to report major depressive symptoms than food-secure people living with HIV. 36 We complement these findings by showing that the association between severe food insecurity and depressive symptoms affects YPLH. The effects of severe food insecurity are cumulative across the lifespan and have intergenerational effects. Therefore, understanding how food insecurity impacts young people can help prevent long-term impacts on mental health.
Given that more than 40% of our sample reported severe food insecurity and greater scores of depressive symptoms, the implications for long-term outcomes are substantial for YPLH. For example, due to the reported associations between depression and medication adherence (Gonzalez et al., 2011), food insecurity can have implications for HIV clinical outcomes such as viral load. 38 Also, our study found that close to 15% engaged in sex work for money and resources. Engaging in sex work negatively impacts mental health outcomes due to the many stressors related to sex work, such as the risk for violence, stigma, and HIV transmission. 39 We also found that those YPLH who engaged in sex work reported significantly higher symptoms of depressive symptoms. Although, this finding was not part of our study objectives, it complements other studies conducted in low- and middle-income settings that have found that engaging in sex work negatively impacts psychological wellbeing among young people.40–42 Poverty and food insecurity have been shown to be key drivers for adolescent girls' and young women's engagement in transactional sex. 42
This study adds to the literature the association between severe food insecurity and mental health outcomes among YPLH, an area that has not been adequately addressed. However, we note some of the study limitations. Depressive symptoms and food insecurity assessments relied on self-reports which may be subject to social desirability and recall bias, particularly under-reporting due to the stigmatization of mental health problems in these settings. However, we minimized this by training the research staff on administering the questionnaires with consistency and without judgment. The HFIAS scale was designed to measure the severity of household food insecurity. Using the HFIAS scale to assess individual experiences may not be represent the perceptions of all other household members. Also, due to the cross-sectional study design, statistical associations may not be indicative of causal relationships between exposure and outcome variables. Longitudinal research is needed to determine the temporal relationship between food insecurity and mental disorders and to identify potential pathways through which food insecurity may elevate the risk of common mental disorders among YPLH. Another limitation is the potential role of the covariates not included in our study, such as a prior history of depression and social support. Also, this study was conducted in rural Zambia and thus the findings may not be generalizable to urban Zambia. The sample consisted of YPLH willing to participate in the study, representing a convenience sample. Thus, we cannot determine how representative they were of the population of YPLH in Eastern Zambia. In addition, although the sample size is appropriate for most of the analyses performed, it was too low to conduct additional analysis such as sensitivity analysis with all the categories of food insecurity (no, mild, moderate, and severe food insecurity) or assess the associations by sex to determine moderating effect of sex on the associations between food insecurity and depressive symptoms. Thus, future research with large samples of YPLH would be useful to determine the generalizability of our findings and assess other possible influences and mechanisms in the associations between food insecurity and depressive symptoms. Missing data was another limitation in this study and was addressed through multiple imputations discussed in the methods section above.
Despite these limitations, we show that severe food insecurity is significantly linked to depressive symptoms in YPLH. More research is needed to understand the effects of severe food insecurity on other health outcomes and disparities in low- and middle- income countries. Research in this area will facilitate public health efforts to address food insecurity as a social determinant of health and inform targeted interventions in households of YPLH in SSA, which in the long run may improve HIV-related outcomes in this setting.
Footnotes
Acknowledgements
We thank the study team, study participants, and collaboration from the University of Zambia, the University of North Carolina at Chapel Hill, and the National Health Research Authority of Zambia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Boston/Providence Center for AIDS Research: P30AI042853. The funder had no role in the study design, data collection and analysis, and manuscript preparation.