
Abstract
Background
The study aimed to explore the sociodemographic factors associated with the acceptance of index case testing (ICT) among newly diagnosed people living with HIV (PLHIV) in Southern Borno, Nigeria.
Methods
The study involved four healthcare facilities providing antiretroviral therapy (ART) services in Southern Borno, Nigeria. Secondary data from the index case testing register were collected between April 2022 and April 2023. Categorical variables were analyzed using descriptive statistics, while bivariate and multiple logistic regression analyses was used to determine the factors associated with ICT acceptance, using a 95% confidence interval and significance level of p ≤ .05.
Results
Among the 302 index cases offered ICT, the acceptance rate was 69.5%. Individuals aged 25–49 years (AOR: 0.294, 95% CI: 0.098–0.775) and 50 years and above (AOR: 0.210, 95% CI: 0.046–0.862) were less likely to accept ICT compared to those aged 18–24 years. Married individuals were 38.86 times more likely to accept ICT than those who were single and never married (AOR: 38.856, 95% CI: 12.620–171.674).
Conclusion
The study shows high ICT acceptance among newly diagnosed PLHIV in Southern Borno, with age and marital status as significant factors. These findings can guide targeted interventions to enhance ICT acceptance and enhance HIV care and prevention strategies in the region.
Introduction
Globally, HIV continues to be a significant public health challenge, approximately affecting 38.4 million people and resulting in an estimated 650,000 deaths in 2021. 1 Nigeria shoulders a substantial HIV burden, responsible for approximately one-third of all new HIV cases in West and Central Africa, with a notably high prevalence rate of 1.4%. 2 To combat the epidemic, UNAIDS has set ambitious targets for epidemic control, known as the 95:95:95 fast track targets, which aim to make 95% of people living with HIV (PLHIV) aware of their status, 95% of people who know their status to have access to treatment, and 95% of people on treatment to have suppressed viral loads by 2030. 3 Achieving these targets is crucial for reducing new infections and ending the HIV epidemic. However, efficient HIV testing services are essential for identifying individuals who are living with HIV and linking them to treatment, care, and support services. 4 The identification of high-risk groups for HIV infection, including partners of PLHIV along with individuals living with HIV yet to be undiagnosed, is therefore a matter of utmost importance. 4 This is because such individuals have the potential to initiate new infections by transmitting the virus, making it imperative to identify and address these individuals and groups. An effective approach to accomplish this objective is by implementing index case testing (ICT), as it focuses on testing only those who are at higher risk of living with HIV.
Index testing, also referred to as partner testing or partner notification services (PNS), is a voluntary procedure that involves offering HIV testing services to the sexual partners, biological children, and individuals who have shared needles with a person who is diagnosed as living with HIV, known as the index client. 5
ICT is highly recommended to individuals who have been newly diagnosed with HIV and those living with HIV and who have not yet achieved viral suppression. This is because these two groups of people are at the greatest risk of transmitting the virus to others. Offering HIV index case testing for new clients is critical to both individual and public health. When someone is newly diagnosed with HIV, it is important to determine who their sexual partners or injection drug use partners may have been during the period of possible transmission. These individuals can be identified as “index cases” and offered HIV testing, counseling, and prevention services. By identifying and testing the sexual or injection drug use partners of newly diagnosed individuals, it is possible to identify and treat other individuals who may be living with undiagnosed HIV. This helps to prevent further transmission of the virus and can ultimately lead to a reduction in new HIV infections. 6
Studies have shown that index testing has one of the highest positivity rates among other HIV testing modalities including voluntary counseling and testing (VCT) and provider-initiated testing and counseling (PITC). Studies conducted in Cameroon and Nigeria found that the positivity rates for index testing were high, with significant differences between genders. In Cameroon for instance, the study reported a positivity rate of 37.2% when testing the partners of index clients, with females having a higher positivity rate (42.9%) than males (31.6%). 7 In Nigeria however, the positivity rate was lower at 20%, but male partners had a higher positivity rate (26.9%) than female partners (15.5%). 8 These findings further highlight the importance of index testing to identify and link individuals to care and treatment. The high positivity rates observed in these studies underscore the urgent need for increased HIV testing and prevention efforts, particularly among populations with higher risk of HIV transmission.
Acceptance of index case testing and partner elicitation is crucial in achieving the goal of the Joint United Nations Programme on HIV/AIDS (UNAIDS) of ending the HIV epidemic by 2030. Partner elicitation involves identifying and testing the sexual partners of HIV-positive individuals, which is vital for reducing the spread of HIV. It is an essential component of HIV prevention and control efforts, as it allows for early detection and treatment of HIV infection among sexual partners. 9
However, the success of partner elicitation depends on the willingness of people with diagnosed HIV to disclose their status and encourage their partners to get tested. Acceptance of ICT is a critical factor in partner elicitation, as it enables PLHIV individuals to understand the importance of partner testing and provides an opportunity for testing and treatment of their sexual partners.
Therefore, understanding the sociodemographic factors associated with acceptance of index case testing is essential for developing targeted interventions to improve HIV testing. Therefore, the objective of this study is to ascertain the sociodemographic factors linked with the acceptance of index case testing among newly diagnosed PLHIV in Southern Borno. Additionally, the study encompasses an analysis of the ICT cascade for these individuals
Methodology
Study design and setting
The research involved a retrospective study of four healthcare facilities, focusing on the secondary data found in ICT registers for people newly diagnosed with HIV from April 2022 to April 2023. The register included information about PLHIV index clients who received PNS as well as their identified sexual partners. The study was conducted in May 2023 at four healthcare facilities in southern Borno state, Nigeria. These facilities, which are supported by the United States President’s Emergency Plan for AIDS Relief (PEPFAR), include Askira General Hospital, Biu General Hospital, Briyel General Hospital, and Lassa General Hospital. As of March 2023, the total number of PLHIV receiving treatment at these facilities were 398, 1514, 380, and 241 respectively. Tier 1 facilities were defined as those having 1000 or more clients receiving ART, whereas Tier 2 encompassed sites with fewer than 1000 clients.
Sampling
The sampling method utilized in this study is total sample enumeration, whereby all newly diagnosed PLHIV index clients who were offered ICT within the specified time period were included in the study population. However, enrollment of clients was restricted to those with complete data in the ICT registers from the four health facilities that met the inclusion criteria. The inclusion criteria included newly diagnosed individuals with HIV from April 2022 to April 2023, aged 18 years and older and being offered PNS, and appropriately documented in the ICT register. Any record in the ICT registers that lacked any of the key analytical variables, including all the sociodemographic variables of the study (age, sex, marital status, education, occupation, and address) and records of ICT was excluded from the study. The study employed a total sample size of 302 individuals.
Data collection
Data regarding the socio-demographic traits of the index cases was obtained from their respective folders, whereas data related to ICT such as ICT acceptance, partner elicitation, contact’s testing and the HIV test outcome of the contacts was gathered from the ICT registers in a structured format.
Variables of the study
Dependent Variable: The dependent variable measured in this study was the acceptance of ICT.
Independent Variable: This included socio-demographic variables such as age, sex, marital status, education, residential distance from the ART center, and facility category.
ICT-related variables, including ICT acceptance, number of contacts elicited, number of contacts tested for HIV, and testing outcome were used in the ICT cascade analysis.
Data analysis
The research data was cleaned using Microsoft Excel 2016 before it was loaded into R studio statistical software version 1.0.143. The categorical variables of the study, which encompassed all the sociodemographic characteristics, were described using frequencies and percentages.
To analyze the relationship between the dependent and independent variables of the study, bivariable analysis was conducted using Chi-squared test. Independent variables with a p-value below 0.2 were selected for multivariate analysis. Finally, multivariable binary logistic regression analysis was carried out to determine the association between each independent variable and the acceptance of index case HIV testing.
Independent variables with p-values less than 0.05 on multivariable logistic regressions were regarded as having statistically significant associations. The results of the multivariable analysis were interpreted using adjusted odds ratios (AOR) accompanied by a 95% confidence interval.
Ethical approval
Ethical clearance was sought and obtained from Borno State Ministry of Health’s Ethical clearance committee (number 38/2023). The research relied on secondary data that was extracted from registers used in the healthcare facilities, containing anonymous client identification details.
Results
Sociodemographic characteristics of newly diagnosed PLHIV in Southern Borno.
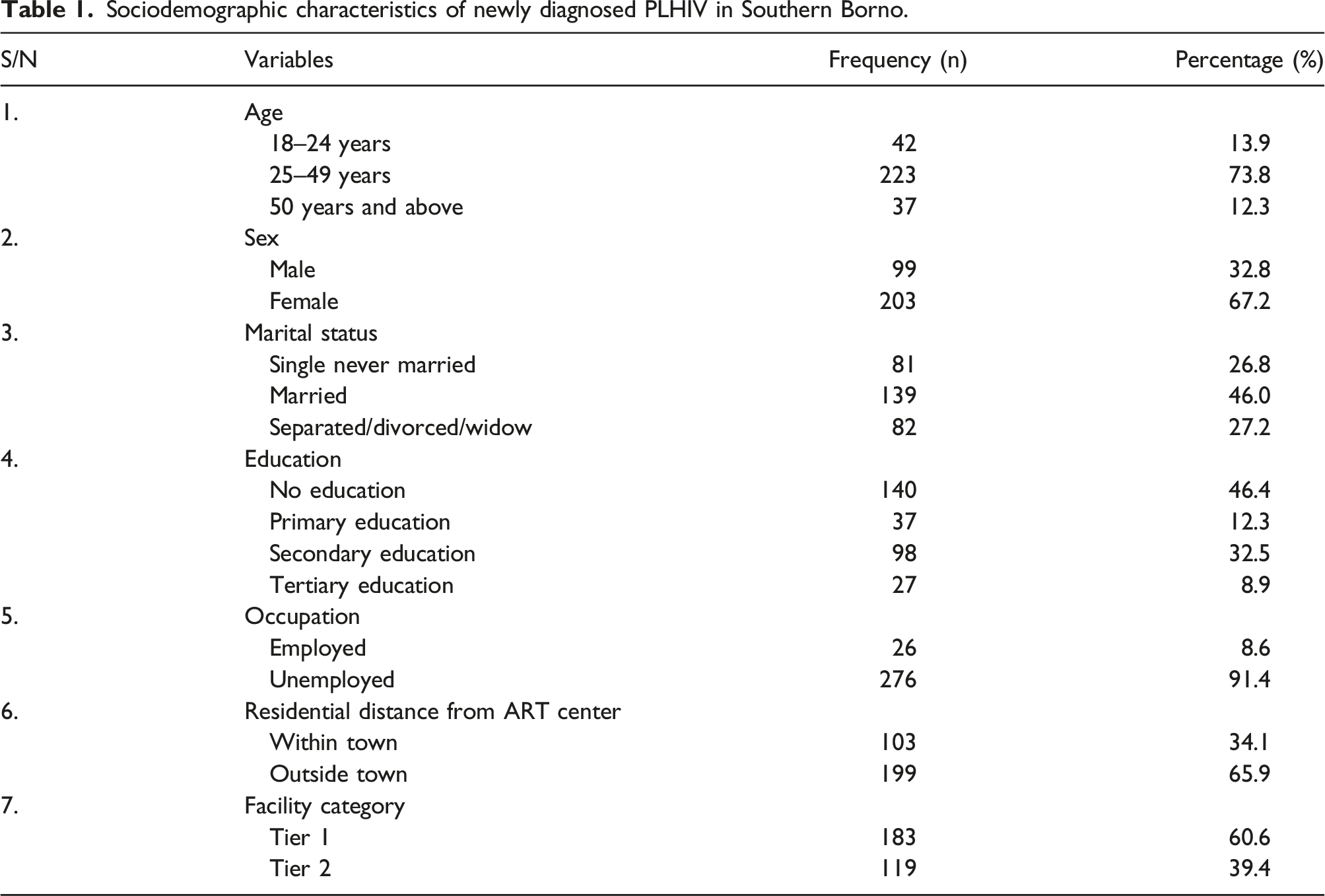
The study analyzed ICT records of 302 newly diagnosed PLHIV in Southern Borno. A large proportion of these individuals fell within the age group of 25–49 years, comprising 223 individuals and accounting for 73.8% of the total sample. Among the participants, the majority were females, with 203 individuals (67.2%), while the remaining 99 individuals (32.8%) were males. Regarding marital status, the highest percentage was observed among married individuals, at 139 individuals (46.0%). In terms of education, most of the participants had no formal education, with 140 individuals (46.4%). The occupational status of the participants revealed that the vast majority were unemployed, comprising 276 individuals (91.4%). In terms of residential distance from the ART center, most of the participants, 199 (65.9%) lived outside the town where the ART center was located and regarding facility category, the majority of the participants received their diagnosis at Tier 1 facilities, with 183 individuals (60.6%).
Bivariate association between sociodemographic characteristics and acceptance of ICT among newly diagnosed PLHIV in Southern Borno.
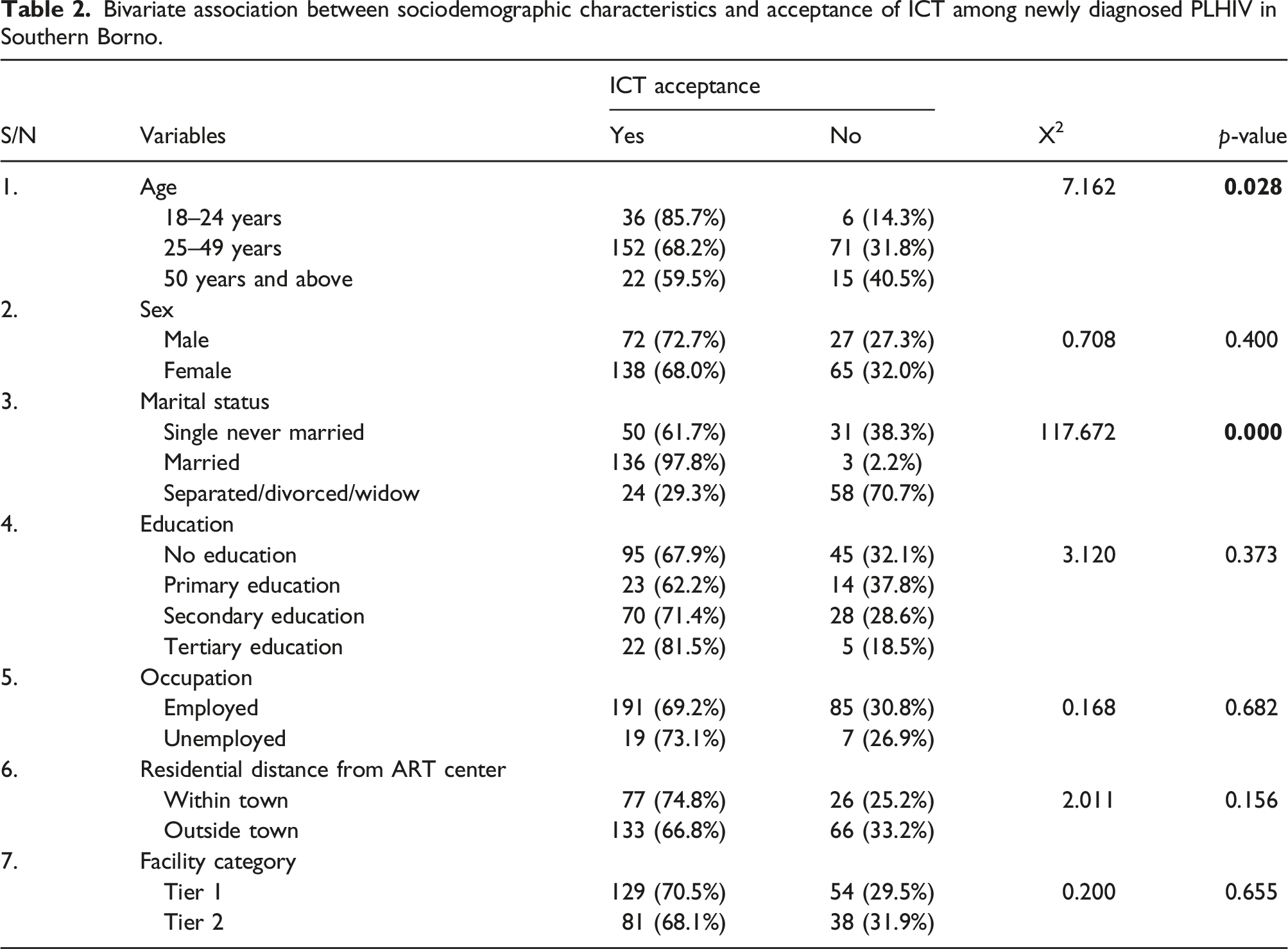
Regarding age, the results revealed a significant association (X2 = 7.162, p = .028) with ICT acceptance, with higher proportions of acceptance observed among individuals aged 18–24 years (85.7%), 25–49 years (68.2%), and 50 years and above (59.5%). However, the association between sex and ICT acceptance was found to be insignificant (X2 = 0.708, p = .400), with similar acceptance rates among males (72.7%) and females (68.0%).
Marital status showed a strong association with ICT acceptance (X2 = 117.672, p = .000), highlighting substantial differences among the categories. Specifically, a high acceptance rate was observed among married individuals (97.8%), while those who were single and never married exhibited a relatively lower acceptance rate (61.7%). Conversely, individuals who were separated, divorced, or widowed demonstrated the lowest acceptance rate (29.3%).
Regarding education level, although no significant association was found (X2 = 3.120, p = .373), the results suggest that individuals with tertiary education exhibited the highest ICT acceptance rate (81.5%), followed by those with secondary education (71.4%) and primary education (62.2%). Similarly, occupation did not demonstrate a significant association (X2 = 0.168, p = .682) with ICT acceptance, with employed individuals showing a slightly higher acceptance rate (69.2%) compared to the unemployed (73.1%).
The analysis of residential distance from the ART center indicated no significant association (X2 = 2.011, p = .156) with ICT acceptance. However, PLHIV residing within the town demonstrated a relatively higher acceptance rate (74.8%) compared to those living outside the town where the ART centre is located (66.8%). Finally, the facility category displayed no significant association (X2 = 0.200, p = .655) with ICT acceptance, with comparable acceptance rates observed between Tier 1 (70.5%) and Tier 2 facilities (68.1%).
Independent variables with a p-value below 0.2, including age (p = .028), marital status (p = .000) and residential distance from the ART center (0.156) were further selected for multivariate analysis.
Multivariate logistic regression for sociodemographic characteristics associated with acceptance of ICT among newly diagnosed PLHIV in Southern Borno.
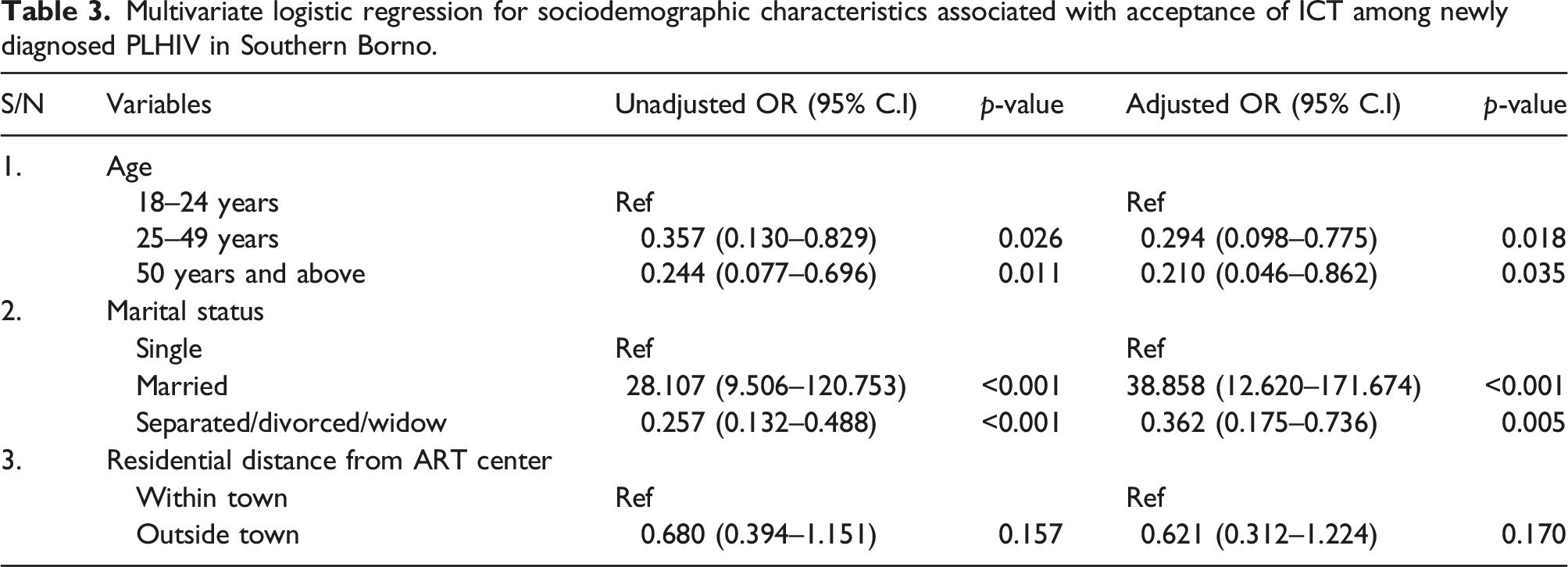
Figure 1 below shows the ICT cascade of newly diagnosed PLHIV in Southern Borno. The data elements and their respective frequencies provide an in-depth overview of the cascade's performance. From the figure, a total of 302 index cases were offered ICT, of which 210 accepted the offer. This reflects a 69.5% acceptance rate for ICT among the index cases. ICT cascade of newly diagnosed PLHIV in Southern Borno.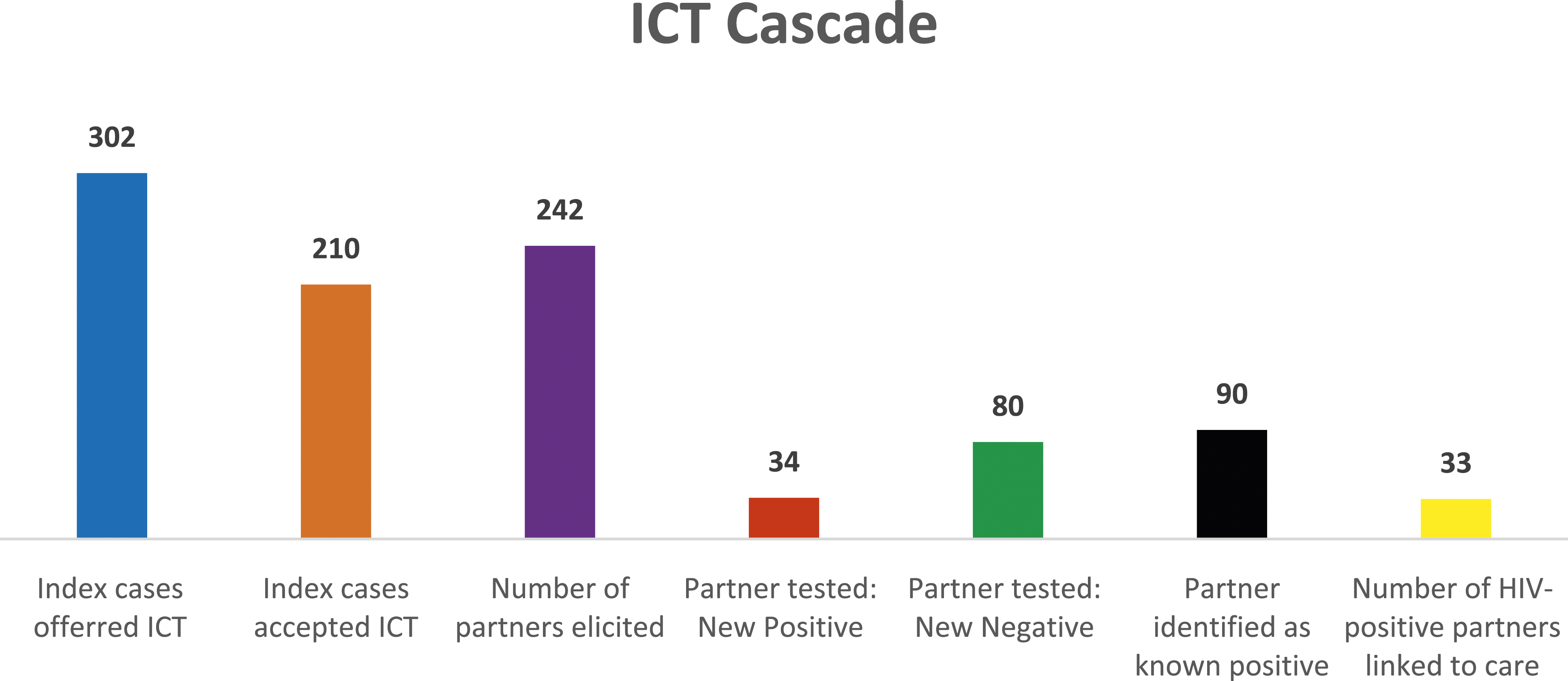
The second data element pertains to partner elicitation and indicates that 242 sexual partners of the index cases were elicited, thus yielding an elicitation ratio of approximately 1 to 1. Of the total 114 partners tested, 34 were found to be living with HIV, while 80 were HIV-negative, thus giving a yield of 29.8%. Furthermore, 90 partners already knew their HIV status and are all linked to care. The identification of these newly diagnosed partners is vital in terms of linking them to appropriate care and treatment to prevent HIV transmission and improve their health outcomes.
Finally, the last data element refers to the number of partners living with HIV who were linked to care. Out of 34 partners who were newly identified as living with HIV, 33 were successfully linked to care, thus giving a linkage rate of 97%. This highlights the importance of linkage to care in the HIV cascade, which ensures that individuals receive timely and appropriate treatment to improve health outcomes and prevent HIV transmission.
Discussion
The findings of this study provide valuable insights into sociodemographic characteristics and their association with the acceptance of ICT among newly diagnosed PLHIV in Southern Borno. The results revealed several noteworthy patterns and associations that contribute to our understanding of the factors influencing ICT acceptance in this population.
Regarding acceptance rate, the study found a 69.5% acceptance rate for ICT among the index cases. This rate is higher than that of previous studies conducted in Tanzania which reported an acceptance rate of 55.5% 10 but lower than that of a study conducted in Nigeria and Ethiopia that reported an acceptance rate of 84.9% and 85.2% respectively.11,12 The differences in the acceptance rate among these studies might be due to factors such as effective partner elicitation strategies, the level of awareness about HIV testing and its benefits, stigma and discrimination, fear of being identified as living with HIV and the availability of convenient and confidential HIV testing services. 10 However, it's essential to recognize that further research is warranted to confirm these claims.
In both the unadjusted and adjusted models of the logistic regression analysis, age and marital status emerged as statistically significant factors associated with ICT acceptance. The finding that age is associated with ICT acceptance does not corroborate with previous studies conducted in Tanzania 10 and Ethiopia, 12 which found no association between age and ICT acceptance. The variation observed in these studies could be attributed to cultural differences, sample characteristics, and contextual factors such as environmental or social factors. However, the finding that marital status is associated with ICT acceptance aligns with a previous study conducted in Tanzania. 10
Regarding age, the results indicated that individuals aged 25–49 years are 70.6% less likely to accept ICT compared to individuals aged 18–24 years. Similarly, individuals aged 50 years and above are 79% less likely to accept ICT than those aged 18–24 years. One possible reason for this association is that younger individuals, who might have grown up in an era with more HIV awareness campaigns and reduced stigma, may be more open and comfortable discussing and disclosing their sexual partners during the process of partner elicitation than older individuals, who may have experienced the peak of the HIV epidemic with higher levels of stigma, and hence, exhibiting greater hesitancy towards partner elicitation. This finding underscores the importance of considering age-specific needs and preferences when designing ICT interventions for PLHIV.
Moreover, being married was strongly associated with a higher likelihood of accepting ICT compared to being single. One possible reason for this is the fact that marriage signifies commitment and a sense of responsibility towards a spouse's health, increasing the likelihood of accepting ICT as a responsible step for partner safety. In contrast, unmarried individuals may lack the same level of commitment, leading to hesitancy towards accepting ICT.
While no significant association was found between education level and ICT acceptance, it is worth noting the trend suggesting higher acceptance rates among individuals with higher education levels. Higher acceptance rates of ICT among individuals with higher education levels could be due to better access to information, improved health literacy, and reduced stigma and discrimination. 13
Regarding positivity yield among partners that were tested, the study found a yield of 29.8%. This yield is higher than the yield reported in a previous study conducted in Ondo State, Nigeria, where the positivity yield among the partners of index cases tested was 20%. 8 The higher yield reported in this study may be due to the effective partner elicitation and testing strategies used, high prevalence of HIV in the population as well as willingness of partners to undergo testing. Considering the scarcity of HIV test kits in Nigeria, it is crucial to emphasize the importance of Index case testing as the way forward due to its significantly high yield of up to 29.8% as found by this study.
In terms of linkage to care, the study found a linkage rate of 97% among partners identified. Although the linkage rate is relatively higher than the UNAIDS second 95 threshold, it is still lower than that of other studies conducted in Nigeria 8 and Cameroon. 7
Although, the results presented in the ICT cascade of newly diagnosed PLHIV in Southern Borno indicate that the cascade is performing relatively well, particularly in terms of acceptance rate and positivity yield, there is room for improvement in certain areas, such as increasing partner elicitation and ensuring that all partners living with HIV are linked to care.
The study is however limited by its retrospective design, which relies on secondary data from registers and may have missing or incomplete data that could affect the accuracy of the study findings. Furthermore, while the study controls for confounding variables, it is possible that other factors such as cultural or social factors not measured in the study could affect the acceptance of ICT among newly diagnosed PLHIV in Southern Borno. Despite these limitations, to our knowledge, this study is the first to assess the factors associated with acceptance of ICT among newly diagnosed PLHIV in Northeastern Nigeria, which could be an important contribution to the literature, inform policy and practice in the region. In addition, the study is multicentered, including data from multiple health facilities in Southern Borno, which could increase the generalizability of the study findings and enhance the external validity of the study.
Conclusion
This study provides valuable insights into the acceptance of HIV index case testing among newly diagnosed PLHIV in Southern Borno. The findings highlight a relatively high acceptance rate and positivity yield, but also identify areas for improvement, particularly in partner elicitation and ensuring linkage to care for affected partners. Age and marital status emerged as significant factors associated with acceptance of index case testing. The findings emphasize the need for tailored strategies that address age-specific needs and promote partner safety within different marital statuses. By addressing these factors, we can enhance acceptance rates and the effectiveness of HIV index case testing among newly diagnosed PLHIV in Southern Borno.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.