
Abstract
Background
Increasingly, young women living with perinatally acquired HIV (YWLPaHIV) have transitioned from paediatric to adult services. There remains a paucity of data on the sexual and reproductive health (SRH) needs of YWLPaHIV and their access to youth-friendly care. Amidst healthcare changes due to COVID-19 pandemic restrictions, we explored SRH needs of a cohort of YWLPaHIV.
Methods
Evaluation of SRH needs of YWLPaHIV attending a UK NHS-youth HIV service with data collected from patient records and self-reported questionnaires amongst women attending between July and November 2020 following easing of the first lockdown and reintroduction of in-person appointments.
Results
71 of 112 YWLPaHIV registered at the clinic completed questionnaires during the study period and were included in the analysis. Median age was 23 y (IQR 21–27, range 18–36). 51/71(72%) reported coitarche, average age 17.6 y (IQR 16–18, range 14–24). 24 women reported 47 pregnancies resulting in 16 (34%) HIV-negative live-births, 19 (40%) terminations, 9(19%) miscarriages, with 3 pregnancies ongoing. 31/48(65%) sexually active women reported current contraception: 10 (32%) condoms, 19 (62%) long-acting, and 3(10%) oral contraceptive pill. 18/51(35%) reported a previous sexually transmitted infection; human papillomavirus (HPV) (11), Chlamydia trachomatis (9) and herpes simplex (2). 27/71(38%) women had undergone cervical cytology including 20/28(71%) women aged ≥25 y with abnormalities documented in 29%. HPV vaccination was reported in 83%, with protective hepatitis B titres in 71%.
Conclusion
High rates of unplanned pregnancy, STIs and cervical abnormalities highlight the continuing SRH needs of YWLPaHIV and requirement for open access to integrated HIV/SRH services despite pandemic restrictions.
Introduction
Increasing numbers of young women living with perinatally acquired HIV (YWLPaHIV) are surviving into adulthood, owing to advances in anti-retroviral therapy (ART). They face unique clinical and psychological challenges surrounding their sexual and reproductive health (SRH) including HIV-related stigma, concerns around onward transmission, and the impact of lifelong immune dysregulation.
Previous studies from highly-resourced, low-prevalence settings have begun to document the SRH vulnerabilities for YWLPaHIV including; low rates of cervical smear uptake with high incidences of cervical abnormalities compared to age-matched HIV negative controls, and higher rates of unplanned conceptions and adverse pregnancy outcomes when compared to their behaviourally infected peers.1,2
Following the SARS-CoV-2 global pandemic, national UK lockdown was imposed on 23rd March 2020. NHS services were reconfigured with cancellation of non-urgent appointments leading to disruptions in screening, contraceptive and sexual health services, with HIV care moving to remote consultations. Poor SRH service uptake carries the potential for unwanted pregnancies, undiagnosed sexually transmitted infections (STI) and cervical cancers. Global barriers to SRH care for adolescents are both internal-lack of knowledge, fear of stigma and shame; and external-including difficulties in access, poor provider attitudes and lack of integration within HIV services. 3
An evaluation was carried out to assess the SRH needs of YWLPaHIV as they exited the first lockdown describing past SRH experiences and identifying the ongoing SRH needs of this unique population.
Methods
A single centre cohort review of the SRH of YWLPaHIV attending a specialist NHS HIV service termed the “900 Clinic” for young adults living in London, with care provided by a multidisciplinary team with integrated HIV/SRH services. Data were collected through electronic case records and a self-reported questionnaire of women ≥18 y during face-to-face (F2F) consultations between 01.07.2020 to 05.11.2020, following the easing of the first lockdown in the UK, and reintroduction of F2F consultations.
Data captured included demographics, HIV viral load (VL), CD4 count, age of menarche/coitarche, Human papillomavirus (HPV) and Hepatitis B virus (HBV) vaccination, serological response to HBV, contraception, past STIs, obstetric history, and cervical cytology. British HIV Association (BHIVA) guidelines recommend annual cervical screening in those living with HIV from 25 y as per the general population.
Data were anonymised with median and interquartile ranges (IQR) summarising non-normally distributed continuous variables, and numbers and percentages summarising categorical variables. The crude incidence rate (CIR) per 1000 person-years at risk (13th birthday to date of questionnaire completion) was calculated for pregnancy.
The survey was categorised as a service evaluation of routinely collected clinical data by the local research committee and research ethics not required, in line with the NHS REC tool.
Public and patient involvement
As this was a service evaluation, there was no involvement nor recruitment of patients or the public in the study design, however identifying their sexual and reproductive health needs was the priority for outcome measures.
Results
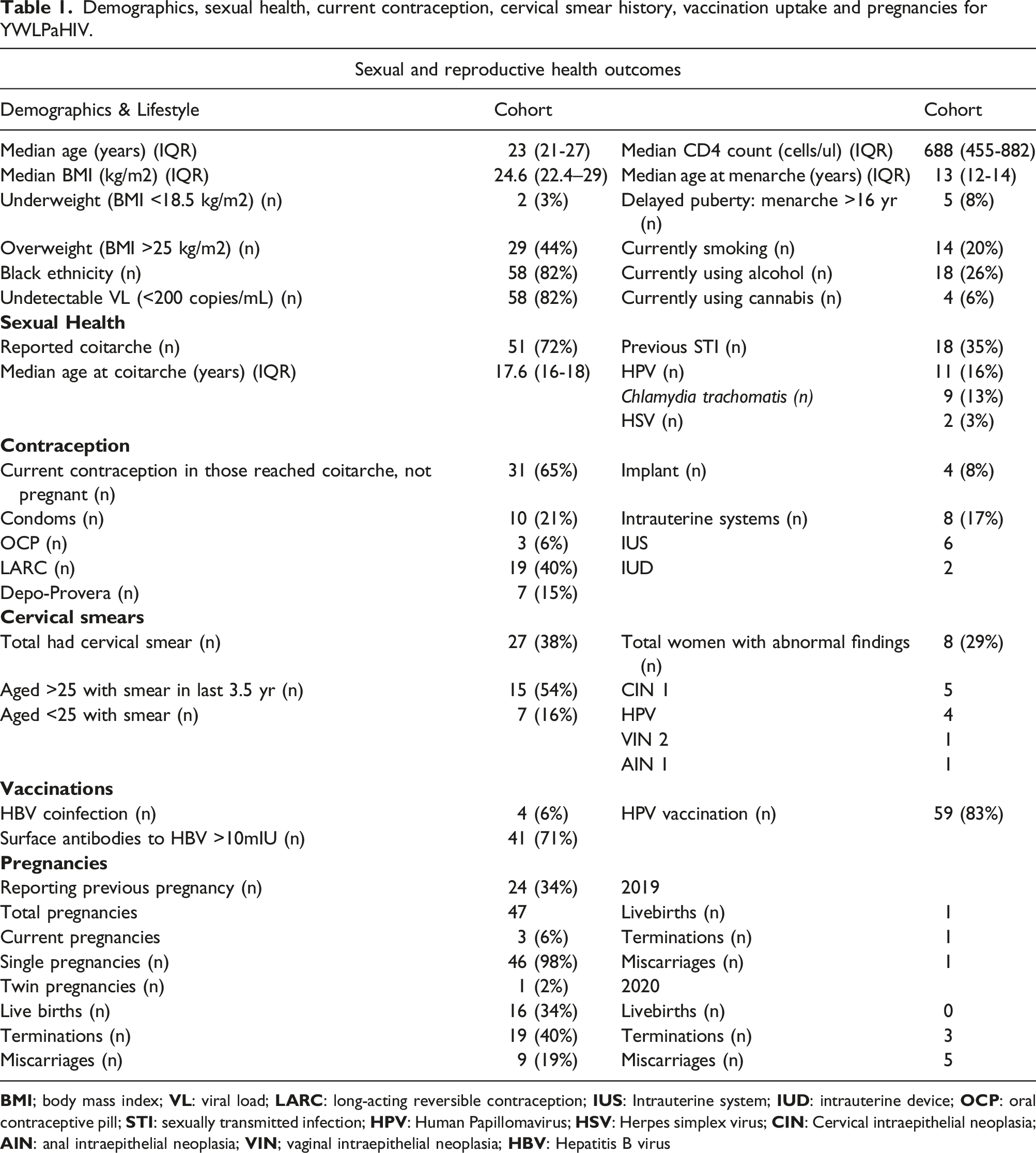
Demographics, sexual health, current contraception, cervical smear history, vaccination uptake and pregnancies for YWLPaHIV.
Sexual Health and Contraception
51/71 (72%) reported coitarche, median age 18 y (IQR 16-18, range 14–24). 18 (35%) reported a previous STI (Table 1). Excluding three pregnant women, 31/48 (65%) of sexually active women reported current contraception, 19 (62%) with current long-acting reversible contraception (LARC). LARC was defined as contraception requiring administration less than once a month and use of contraceptive measures was asked during routine clinical conversations about primary contraception and prevention of STI transmission.
Obstetric History
24 women reported 47 pregnancies, median age first pregnancy 23 y, resulting in 16 (34%) live births, 19 (40%) terminations, 9 (19%) miscarriages with 3 (6%) pregnancies ongoing. All 16 infants were HIV-negative. The pregnancy incidence was 57 per 1000 y of follow up. There were 3 terminations and 5 miscarriages reported by 6 women in 2020. Two terminations were elective first trimester, with one emergency termination at 22 weeks’ gestation for life threatening maternal eclampsia. Of the miscarriages, four were first trimester, with one second trimester (23/40) due to placental insufficiency and intrauterine growth restriction.
Cervical smears and vaccination
27/71 (38%) women reported ever having a cervical smear including 20/28 (71%) women aged ≥25; six (21%) with the last year and 15 (54%) within 3.5 y. Abnormal findings reported in 8/27 (30%) (Table 1). One woman is under specialist gynaecological care with concomitant VIN2 and AIN1 lesions, 3 were referred back to general practice, 4 have not attended recalls; 3 since 2017, one since 2015. One of three patients turning 25 during the review period reported having her first smear.
59/71 (83%) recalled prior HPV vaccination. 24 women were ≥14 y when the national HPV vaccination programme was introduced in 2008. Excluding four YWLPaHIV with HBV coinfection, 41/63 (71%) demonstrated HBV surface antibodies >10mIU.
Discussion
This service evaluation of the SRH needs of YWLPaHIV demonstrated low smear uptake with high rates of abnormalities, as well as high rates of pregnancy termination, highlighting the need for improved uptake of contraception and cervical screening.
Young women living with perinatally acquired HIV have unique SRH needs from childhood; growing up, negotiating puberty, and sexuality with a sexually transmissible disease before ever having had sex themselves. For those who struggle with adherence to ART (18% of this cohort) there is the potential for transmission to partners and infants. Sexual debut occurred at a similar age to their HIV-unaffected peers, median 17.6 y, UK median 16–17 y, and is consistent with previously published data.1,2,4 One third of the cohort had experienced pregnancy; 40% resulting in termination. This reflects higher rates than the UK population although terminations are highest in: 18–24-y-olds, those living in social deprivation, London compared to the rest of the country, with recurrent abortions more common in women of black ethnicity. All of these factors are overly represented within this cohort. 19% of pregnancies resulted in miscarriage with similar rates of spontaneous foetal loss reported in a US cohort of women living with HIV (median age 29). 5 Reassuringly all 16 infants born to YWLPaHIV were HIV unaffected, despite UK data to suggest that women with PaHIV are more likely to have lower CD4 counts and detectable viral loads nearer to conception and delivery than their age-matched behaviourally infected peers. 2
Access to adequate contraception is essential in reducing unwanted pregnancies. Only 65% of sexually active women in this group reported current contraception; 40% with LARC, a rate comparable to 2013. 1 Whilst some women reporting no current contraception may be explained by reduced sexual activity in lockdown and planning pregnancy, it suggests lack of uptake of contraception despite engagement in HIV care with integrated SRH services, although pandemic restrictions may have enhanced barriers to recent care.
54% of women aged ≥25 had a smear in the last 3.5 y, compared with the national average of 69% in women aged 25–49. Almost one third previously had cervical abnormalities which, although lower than 48% reported in a US PaHIV cohort, is significantly higher than the UK rate of 5%. 6 Embarrassment, cultural barriers, and fear prevent women attending smear appointments, heightened in the pandemic for women of ethnic minority backgrounds due to fear of contracting COVID-19 whilst attending screening. 7 Delays in screening due to COVID-19 project an estimated additional cervical cancer diagnosis in 4.3 per 100,000. 7 To address low smear uptake, a UK trial is assessing HPV home-testing kits for women ≥15 months overdue their smear test. Within the clinic, a study is enrolling comparing cervical smears and rapid point of care HPV testing, including those aged 18–24 y who are currently excluded from the national screening program, due to concerns of early CIN changes reported in perinatal cohorts under 25 y.1,6
HPV vaccine uptake in this group is good, with 83% reporting previous vaccination. However, national reports of HPV vaccine uptake amongst year 9 females demonstrate a significant decline from 83.9% to 64.7% between 2019 and 2020 and reflects the impact of lockdown on vaccine programs delivered in schools. A significant improvement in HBV uptake within this cohort can be assumed from the improved serological markers; in 2013 only 26% had HBV surface antibody titres >10 mlU, rising to 71% of the current cohort. 1
Whilst the limitations of the review include a relatively small cohort with retrospective nature open to recall bias, this is likely to under rather than over report past events such as terminations of pregnancy and STIs. Screening for cervical abnormalities must be prioritised in those overdue.
COVID-19 has presented many challenges to continuum of healthcare, however maintaining open access to integrated SRH services for vulnerable populations must remain a priority. We suggest future research focuses on elucidating the sexual and reproductive health disparities that YWLPaHIV experience, including the impact of HPV vaccination.
Footnotes
Acknowledgements
The preliminary findings of this analysis were presented at the BHIVA/BASHH 2021 5th Joint Conference.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.